

Ferulic Acid Treats Gastric Ulcer via Suppressing Oxidative Stress and Inflammation
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Ethical Consideration
2.3. Drugs and Other Chemicals
2.4. Indomethacin-Induced Gastric Ulcer
2.5. Experimental Design
2.6. Macroscopic Evaluation
2.7. Estimation of Biochemical Parameters in Gastric Tissue
2.7.1. Measurement of Gastric Oxidative Stress Markers Levels
2.7.2. Measurement of MPO Activity and Gastric Inflammatory Mediators’ Levels
2.8. Histological Evaluation
2.9. Scanning Electron Microscopy (SEM)
2.10. Statistical Analysis
3. Results
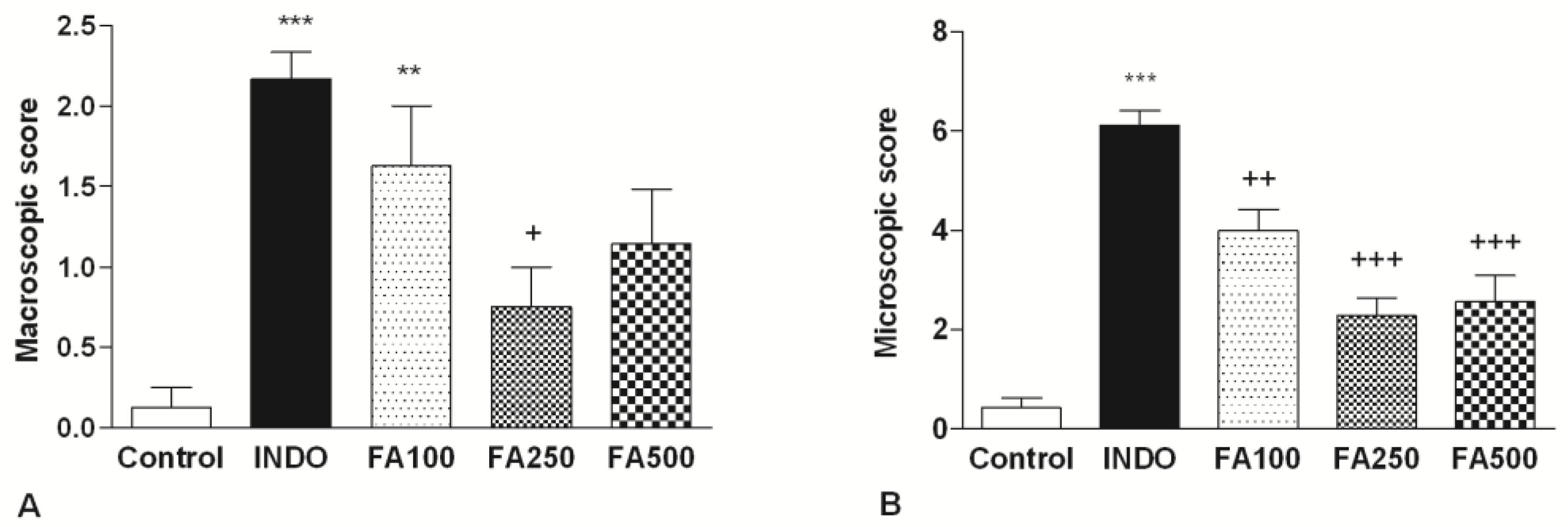
3.1. Macroscopic and Microscopic Scores
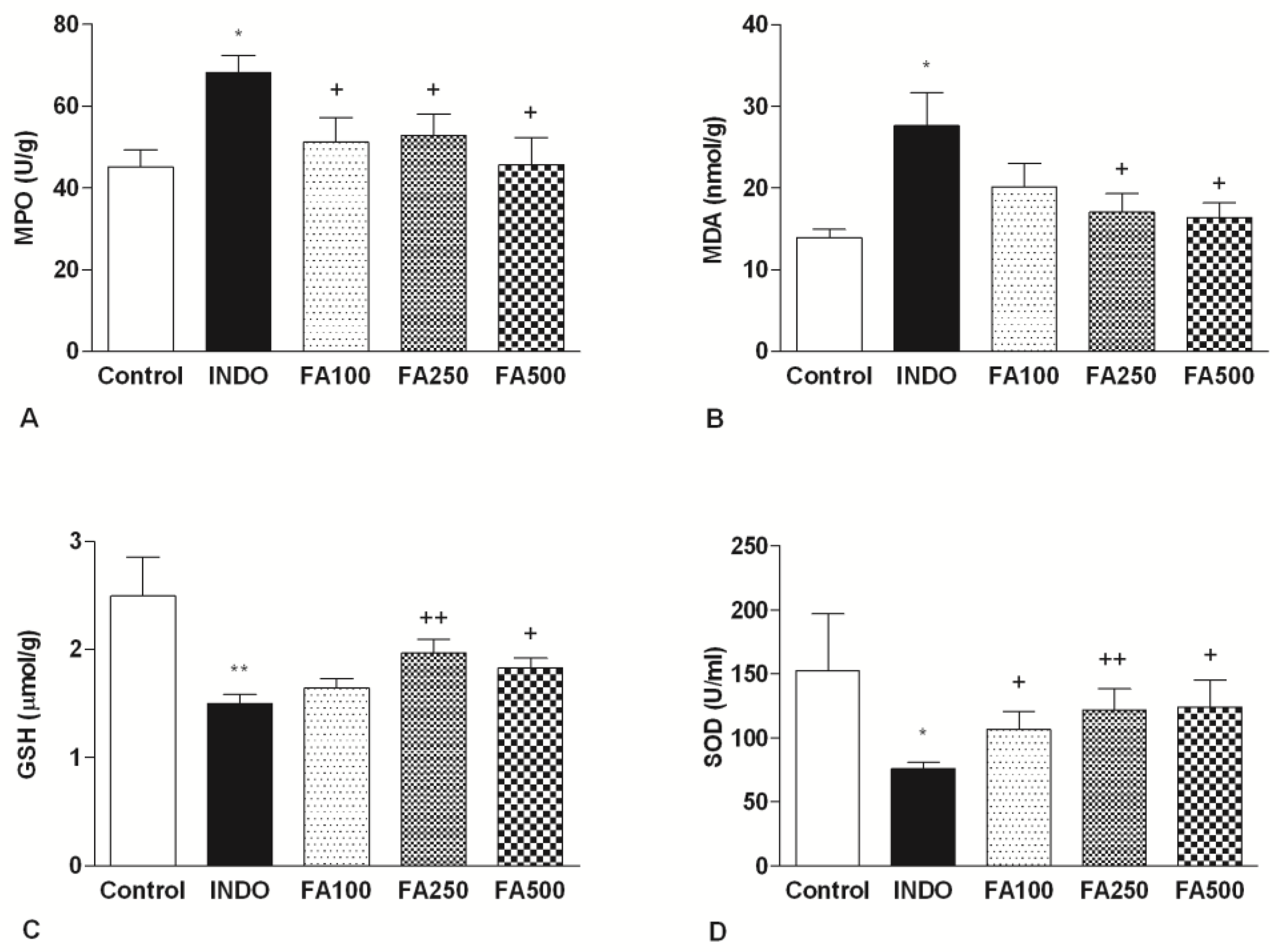
3.2. Effect of FA on MPO and Gastric Oxidative Stress Markers Levels
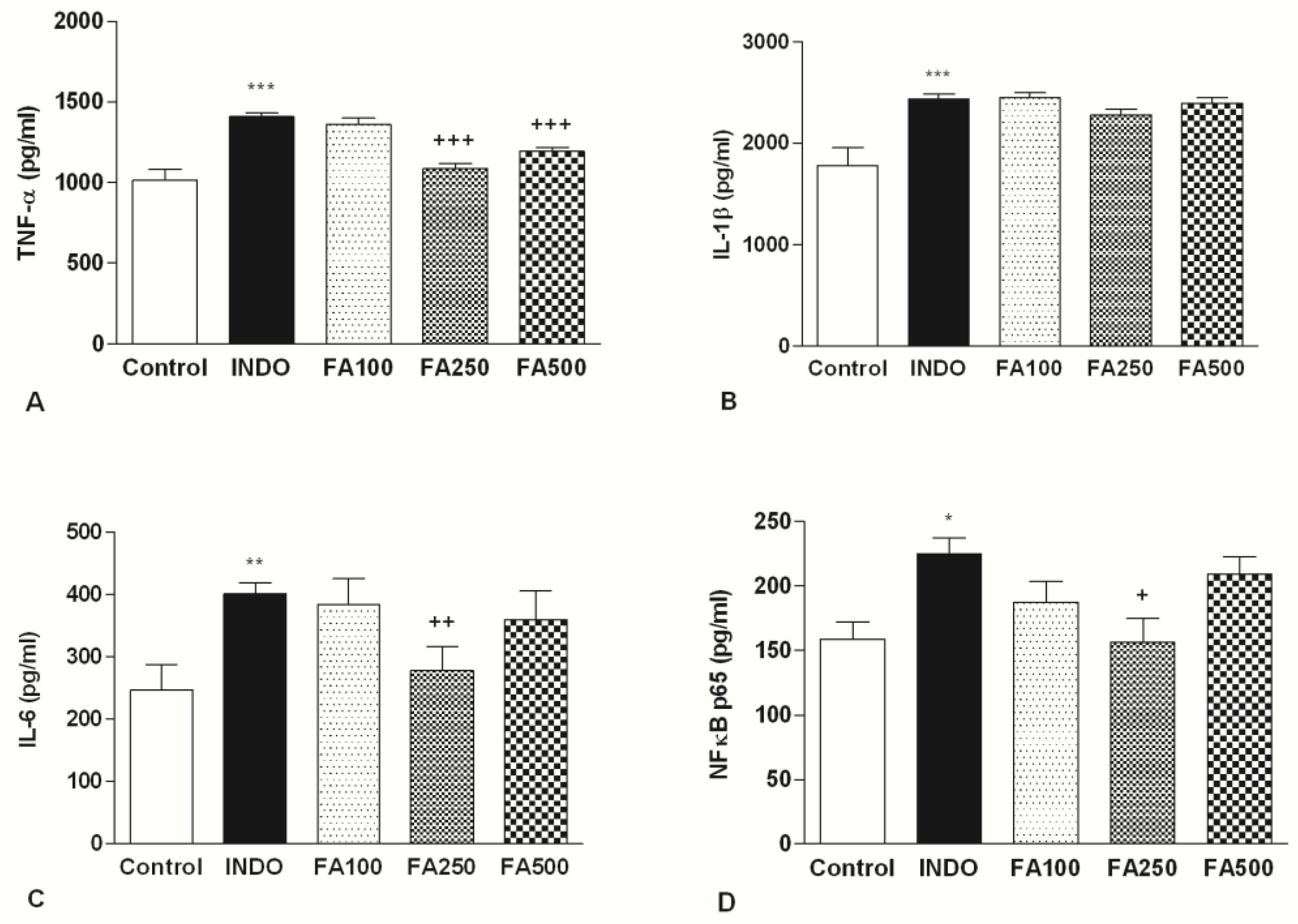
3.3. Effect of FA on Gastric Inflammatory Mediators’ Levels
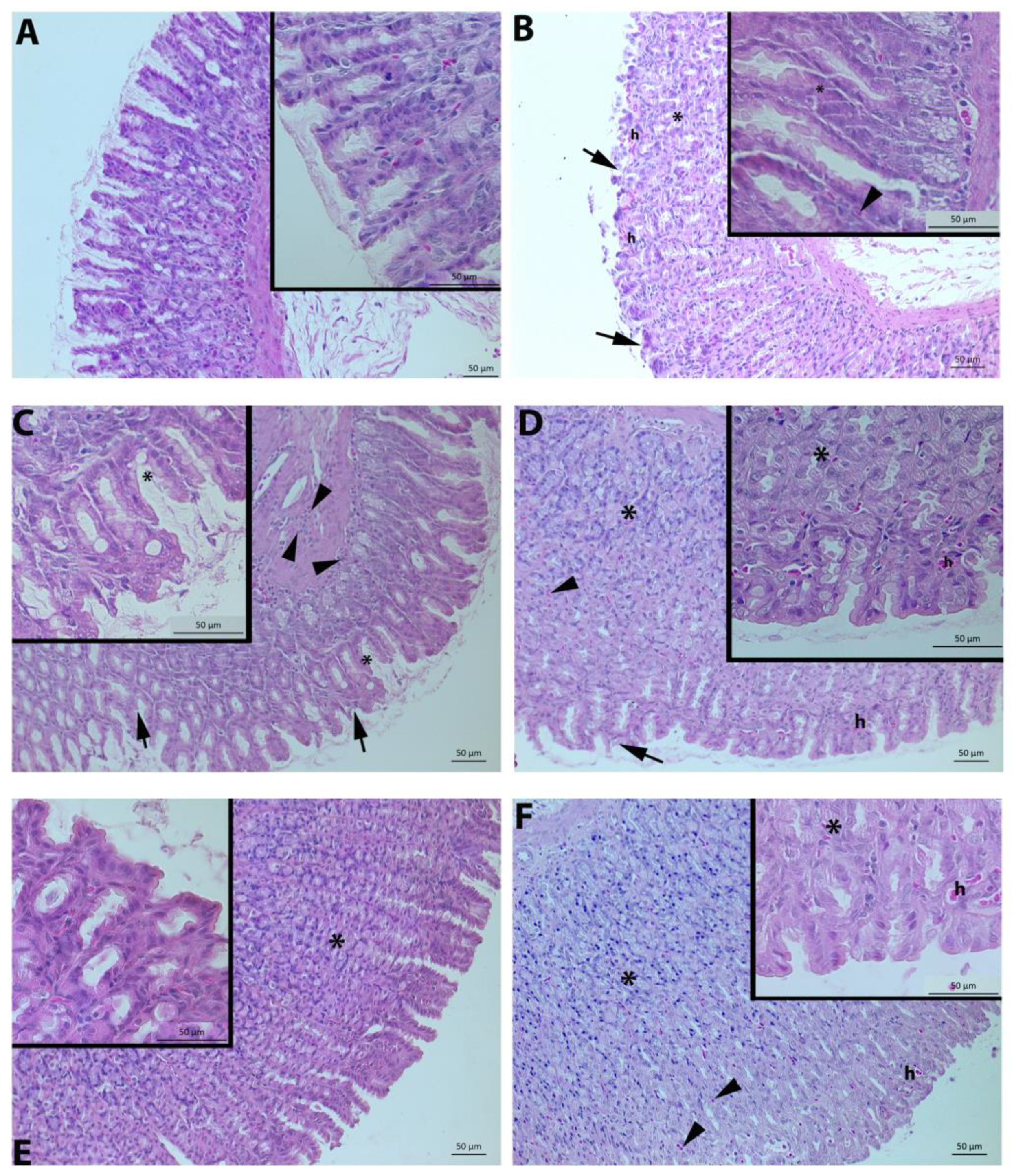
3.4. Histological Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lanas, A.; Chan, F.K. Peptic ulcer disease. Lancet 2017, 390, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Paradee, N.; Koonyosying, P.; Kusirisin, W.; Janthip, R.; Kanjanapothi, D.; Pattanapanyasat, K.; Srichairatanakool, S. Analgesic, anti-inflammatory and anti-ulcer properties of Thai perilla frutescence fruit oil in animals. Biosci. Rep. 2021, 41, BSR20203166. [Google Scholar] [CrossRef] [PubMed]
- Tkacs, N.; Herrmann, L.; Johnson, R. Advanced Physiology and Pathophysiology: Essentials for Clinical Practice; Springer Publishing Company: New York, NY, USA, 2020. [Google Scholar]
- Reshetnyak, V.I.; Burmistrov, A.I.; Maev, I.V. Helicobacter pylori: Commensal, symbiont or pathogen? World J. Gastroenterol. 2021, 27, 545. [Google Scholar] [CrossRef] [PubMed]
- Harirforoosh, S.; Asghar, W.; Jamali, F. Adverse effects of nonsteroidal antiinflammatory drugs: An update of gastrointestinal, cardiovascular and renal complications. J. Pharm. Pharm. Sci. 2013, 16, 821–847. [Google Scholar] [CrossRef] [Green Version]
- Melcarne, L.; García-Iglesias, P.; Calvet, X. Management of NSAID-associated peptic ulcer disease. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 723–733. [Google Scholar] [CrossRef]
- Aleid, I.S.; Alfheeaid, H.A.; Aljutaily, T.; Alhomaid, R.M.; Alharbi, H.F.; Althwab, S.A.; Abdel-Rahman, H.A.; AlGeffari, M.A.; Barakat, H. Gastroprotective effects of spirulina platensis, golden kiwifruit flesh, and golden kiwifruit peel extracts individually or in combination against indomethacin-induced gastric ulcer in rats. Nutrients 2021, 13, 3499. [Google Scholar] [CrossRef]
- AbdelAziz, E.Y.; Tadros, M.G.; Menze, E.T. The effect of metformin on indomethacin-induced gastric ulcer: Involvement of nitric oxide/Rho kinase pathway. Eur. J. Pharmacol. 2021, 892, 173812. [Google Scholar] [CrossRef]
- Karampour, N.S.; Arzi, A.; Rezaie, A.; Pashmforoosh, M.; Kordi, F. Gastroprotective effect of zingerone on ethanol-induced gastric ulcers in rats. Medicina 2019, 55, 64. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Xue, F.; Han, C.; Yang, H.; Han, L.; Li, K.; Li, J.; Xu, Q.; Li, Z.; Yuan, B. Ferulic acid ameliorated placental inflammation and apoptosis in rat with preeclampsia. Clin. Exp. Hypertens. 2019, 41, 524–530. [Google Scholar] [CrossRef]
- Kumar, N.; Pruthi, V. Potential applications of ferulic acid from natural sources. Biotechnol. Rep. 2014, 4, 86–93. [Google Scholar] [CrossRef]
- Chaudhary, A.; Jaswal, V.S.; Choudhary, S.; Sharma, A.; Beniwal, V.; Tuli, H.S.; Sharma, S. Ferulic acid: A promising therapeutic phytochemical and recent patents advances. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 115–123. [Google Scholar] [CrossRef]
- Ghosh, S.; Basak, P.; Dutta, S.; Chowdhury, S.; Sil, P.C. New insights into the ameliorative effects of ferulic acid in pathophysiological conditions. Food Chem. Toxicol. 2017, 103, 41–55. [Google Scholar] [CrossRef]
- De Paiva, L.B.; Goldbeck, R.; dos Santos, W.D.; Squina, F.M. Ferulic acid and derivatives: Molecules with potential application in the pharmaceutical field. Braz. J. Pharm. Sci. 2013, 49, 395–411. [Google Scholar] [CrossRef] [Green Version]
- De Barros, M.P.; Lemos, M.; Maistro, E.L.; Leite, M.F.; Sousa, J.P.B.; Bastos, J.K.; de Andrade, S.F. Evaluation of antiulcer activity of the main phenolic acids found in Brazilian green propolis. J. Ethnopharmacol. 2008, 120, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Kolgazi, M.; Cantali-Ozturk, C.; Deniz, R.; Ozdemir-Kumral, Z.N.; Yuksel, M.; Sirvanci, S.; Yeğen, B.C. Nesfatin-1 alleviates gastric damage via direct antioxidant mechanisms. J. Surg. Res. 2015, 193, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Yabe, T.; Hirahara, H.; Harada, N.; Ito, N.; Nagai, T.; Sanagi, T.; Yamada, H. Ferulic acid induces neural progenitor cell proliferation in vitro and in vivo. Neuroscience 2010, 165, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Cilingir, S.; Açıkel-Elmas, M.; Arbak, S.; Kolgazi, M. Ferulic acid attenuates panrceaticobiliary duct occlusion induced inflammation in both pancreas and liver. Inflammopharmacology, 2022; preprint. [Google Scholar]
- Marte, V.M.M.; Ateufack, G.; Mbiantcha, M.; Atsamo, A.D.; Adjouzem, C.F.; Nguemnang, S.F.D.; Tsafack, E.G.; Nana, W.Y.; Kouam, Y.K.M.; Azanze, E.N. Methanolic extract of distemonanthus benthamianus (caesalpiniaceae) stem bark suppresses ethanol/indomethacin-induced chronic gastric injury in rats. Gastroenterol. Res. Pract. 2020, 2020, 8180323. [Google Scholar] [CrossRef]
- Cevík, H.; Erkanli, G.; Ercan, F.; Işman, C.A.; Yeğen, B.C. Exposure to continuous darkness ameliorates gastric and colonic inflammation in the rat: Both receptor and non-receptor-mediated processes. J. Gastroenterol. Hepatol. 2005, 20, 294–303. [Google Scholar] [CrossRef]
- Abbas, A.M.; Sakr, H.F. Effect of selenium and grape seed extract on indomethacin-induced gastric ulcers in rats. J. Physiol. Biochem. 2013, 69, 527–537. [Google Scholar] [CrossRef]
- Katary, M.; Salahuddin, A. Gastroprotective effect of vanillin on indomethacin-induced gastric ulcer in rats: Protective pathways and anti-Secretory mechanism. Clin. Exp. Pharmacol. 2017, 7, 2161–1459. [Google Scholar]
- Pozzoli, C.; Menozzi, A.; Grandi, D.; Solenghi, E.; Ossiprandi, M.C.; Zullian, C.; Bertini, S.; Cavestro, G.M.; Coruzzi, G. Protective effects of proton pump inhibitors against indomethacin-induced lesions in the rat small intestine. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2007, 374, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Bami, E.; Ozakpınar, O.B.; Ozdemir-Kumral, Z.N.; Köroglu, K.; Ercan, F.; Cirakli, Z.; Sekerler, T.; Izzettin, F.V.; Sancar, M.; Okuyan, B. Protective effect of ferulic acid on cisplatin induced nephrotoxicity in rats. Environ. Toxicol. Pharmacol. 2017, 54, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Phaniendra, A.; Jestadi, D.B.; Periyasamy, L. Free radicals: Properties, sources, targets, and their implication in various diseases. Indian J. Clin. Biochem. 2015, 30, 11–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharyya, A.; Chattopadhyay, R.; Mitra, S.; Crowe, S.E. Oxidative stress: An essential factor in the pathogenesis of gastrointestinal mucosal diseases. Physiol. Rev. 2014, 94, 329–354. [Google Scholar] [CrossRef] [Green Version]
- Tsikas, D. Assessment of lipid peroxidation by measuring malondialdehyde (MDA) and relatives in biological samples: Analytical and biological challenges. Anal. Biochem. 2017, 524, 13–30. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.-W.; Kim, D.-J. Protective effects of BK-1202 on the indomethacin-induced gastric ulcer in rats. J. Korean Med. 2015, 36, 42–55. [Google Scholar] [CrossRef]
- Qi, M.-Y.; Wang, X.-T.; Xu, H.-L.; Yang, Z.-L.; Cheng, Y.; Zhou, B. Protective effect of ferulic acid on STZ-induced diabetic nephropathy in rats. Food Funct. 2020, 11, 3706–3718. [Google Scholar] [CrossRef]
- de Barros, M.; Da Silva, L.M.; Boeing, T.; Somensi, L.B.; Cury, B.J.; de Moura Burci, L.; Santin, J.R.; de Andrade, S.F.; Monache, F.D.; Cechinel-Filho, V. Pharmacological reports about gastroprotective effects of methanolic extract from leaves of Solidago chilensis (Brazilian arnica) and its components quercitrin and afzelin in rodents. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2016, 389, 403–417. [Google Scholar] [CrossRef]
- Liu, Y.-H.; Zhang, Z.-B.; Zheng, Y.-F.; Chen, H.-M.; Yu, X.-T.; Chen, X.-Y.; Zhang, X.; Xie, J.-H.; Su, Z.-Q.; Feng, X.-X. Gastroprotective effect of andrographolide sodium bisulfite against indomethacin-induced gastric ulceration in rats. Int. Immunopharmacol. 2015, 26, 384–391. [Google Scholar] [CrossRef]
- Zaghlool, S.S.; Abo-Seif, A.A.; Rabeh, M.A.; Abdelmohsen, U.R.; Messiha, B.A. Gastro-protective and anti-oxidant potential of Althaea officinalis and solanum nigrum on pyloric ligation/indomethacin-induced ulceration in rats. Antioxidants 2019, 8, 512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roghani, M.; Kalantari, H.; Khodayar, M.J.; Khorsandi, L.; Kalantar, M.; Goudarzi, M.; Kalantar, H. Alleviation of liver dysfunction, oxidative stress and inflammation underlies the protective effect of ferulic acid in methotrexate-induced hepatotoxicity. Drug Des. Dev. Ther. 2020, 14, 1933. [Google Scholar] [CrossRef] [PubMed]
- Pérez, Y.; Oyárzabal, A.; Mas, R.; Molina, V.; Jiménez, S. Protective effect of D-002, a mixture of beeswax alcohols, against indomethacin-induced gastric ulcers and mechanism of action. J. Nat. Med. 2013, 67, 182–189. [Google Scholar] [CrossRef]
- Yuan, J.; Ge, K.; Mu, J.; Rong, J.; Zhang, L.; Wang, B.; Wan, J.; Xia, G. Ferulic acid attenuated acetaminophen-induced hepatotoxicity though down-regulating the cytochrome P 2E1 and inhibiting toll-like receptor 4 signaling-mediated inflammation in mice. Am. J. Transl. Res. 2016, 8, 4205. [Google Scholar] [PubMed]
- Kim, Y.-S.; Nam, Y.; Song, J.; Kim, H. Gastroprotective and healing effects of polygonum cuspidatum root on experimentally induced gastric ulcers in rats. Nutrients 2020, 12, 2241. [Google Scholar] [CrossRef]
- Mancuso, C.; Santangelo, R. Ferulic acid: Pharmacological and toxicological aspects. Food Chem. Toxicol. 2014, 65, 185–195. [Google Scholar] [CrossRef]
- Alam, M.A. Anti-hypertensive effect of cereal antioxidant ferulic acid and its mechanism of action. Front. Nutr. 2019, 6, 121. [Google Scholar] [CrossRef]
- Wu, X.; Huang, Q.; Xu, N.; Cai, J.; Luo, D.; Zhang, Q.; Su, Z.; Gao, C.; Liu, Y. Antioxidative and anti-inflammatory effects of water extract of Acrostichum aureum Linn. against ethanol-induced gastric ulcer in rats. Evid.-Based Complement. Altern. Med. 2018, 2018, 3585394. [Google Scholar] [CrossRef] [Green Version]
- Sallam, A.-A.M.; Darwish, S.F.; El-Dakroury, W.A.; Radwan, E. Olmesartan niosomes ameliorates the Indomethacin-induced gastric ulcer in rats: Insights on MAPK and Nrf2/HO-1 signaling pathway. Pharm. Res. 2021, 38, 1821–1838. [Google Scholar] [CrossRef]
- Salem, N.A.; Wahba, M.A.; Eisa, W.H.; El-Shamarka, M.; Khalil, W. Silver oxide nanoparticles alleviate indomethacin-induced gastric injury: A novel antiulcer agent. Inflammopharmacology 2018, 26, 1025–1035. [Google Scholar] [CrossRef]
- Antonisamy, P.; Arasu, M.V.; Dhanasekaran, M.; Choi, K.C.; Aravinthan, A.; Kim, N.S.; Kang, C.-W.; Kim, J.-H. Protective effects of trigonelline against indomethacin-induced gastric ulcer in rats and potential underlying mechanisms. Food Funct. 2016, 7, 398–408. [Google Scholar] [CrossRef]
- De Melo, T.; Lima, P.; Carvalho, K.; Fontenele, T.; Solon, F.; Tomé, A.; De Lemos, T.; da Cruz Fonseca, S.; Santos, F.; Rao, V. Ferulic acid lowers body weight and visceral fat accumulation via modulation of enzymatic, hormonal and inflammatory changes in a mouse model of high-fat diet-induced obesity. Braz. J. Med. Biol. Res. 2017, 50, e5630. [Google Scholar] [CrossRef]
- Gerin, F.; Erman, H.; Erboga, M.; Sener, U.; Yilmaz, A.; Seyhan, H.; Gurel, A. The effects of ferulic acid against oxidative stress and inflammation in formaldehyde-induced hepatotoxicity. Inflammation 2016, 39, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.F.; Nabil, M.; Abdo, W.; Abdelfattah, M.A.; El-Shazly, A.M.; El Kharrassi, Y.; Sobeh, M. Syzygium samarangense leaf extract mitigates indomethacin-induced gastropathy via the NF-κB signaling pathway in rats. Biomed. Pharmacother. 2021, 139, 111675. [Google Scholar] [CrossRef] [PubMed]
- Yin, P.; Zhang, Z.; Li, J.; Shi, Y.; Jin, N.; Zou, W.; Gao, Q.; Wang, W.; Liu, F. Ferulic acid inhibits bovine endometrial epithelial cells against LPS-induced inflammation via suppressing NK-κB and MAPK pathway. Res. Vet. Sci. 2019, 126, 164–169. [Google Scholar] [CrossRef]
- El Badawy, S.A.; Ogaly, H.A.; Abd-Elsalam, R.M.; Azouz, A.A. Benzyl isothiocyanates modulate inflammation, oxidative stress, and apoptosis via Nrf2/HO-1 and NF-κB signaling pathways on indomethacin-induced gastric injury in rats. Food Funct. 2021, 12, 6001–6013. [Google Scholar] [CrossRef] [PubMed]
- Akanda, M.R.; Park, B.-Y. Involvement of MAPK/NF-κB signal transduction pathways: Camellia japonica mitigates inflammation and gastric ulcer. Biomed. Pharmacother. 2017, 95, 1139–1146. [Google Scholar] [CrossRef]
- Mir, S.M.; Ravuri, H.G.; Pradhan, R.K.; Narra, S.; Kumar, J.M.; Kuncha, M.; Kanjilal, S.; Sistla, R. Ferulic acid protects lipopolysaccharide-induced acute kidney injury by suppressing inflammatory events and upregulating antioxidant defenses in Balb/c mice. Biomed. Pharmacother. 2018, 100, 304–315. [Google Scholar] [CrossRef]
- Garro, M.F.; Ibáñez, A.G.S.; Vega, A.E.; Sosa, A.C.A.; Pelzer, L.; Saad, J.R.; Maria, A.O. Gastroprotective effects and antimicrobial activity of Lithraea molleoides and isolated compounds against helicobacter pylori. J. Ethnopharmacol. 2015, 176, 469–474. [Google Scholar] [CrossRef]
- Costa, P.; Boeing, T.; Somensi, L.B.; Cury, B.J.; Espíndola, V.L.; França, T.C.S.; de Almeida, M.O.; Arruda, C.; Bastos, J.K.; da Silva, L.M. Hydroalcoholic extract from Baccharis dracunculifolia recovers the gastric ulcerated tissue, and p-coumaric acid is a pivotal bioactive compound to this action. Biofactors 2019, 45, 479–489. [Google Scholar] [CrossRef]
- El-Din, M.I.G.; Youssef, F.S.; Said, R.S.; Ashour, M.L.; Eldahshan, O.A.; Singab, A.N.B. Chemical constituents and gastro-protective potential of Pachira glabra leaves against ethanol-induced gastric ulcer in experimental rat model. Inflammopharmacology 2021, 29, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Thong-Ngam, D.; Choochuai, S.; Patumraj, S.; Chayanupatkul, M.; Klaikeaw, N. Curcumin prevents indomethacin-induced gastropathy in rats. World J. Gastroenterol. WJG 2012, 18, 1479. [Google Scholar] [CrossRef] [PubMed]
- Zaki, S.M.; Mohammed, E.A. Experimental study Effect of glucocorticoids on indomethacin-induced gastric ulcer in the adult male albino rat–histological, morphometric and electron microscopy study. Arch. Med. Sci. 2014, 10, 381–388. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ermis, A.; Aritici Colak, G.; Acikel-Elmas, M.; Arbak, S.; Kolgazi, M. Ferulic Acid Treats Gastric Ulcer via Suppressing Oxidative Stress and Inflammation. Life 2023, 13, 388. https://doi.org/10.3390/life13020388
Ermis A, Aritici Colak G, Acikel-Elmas M, Arbak S, Kolgazi M. Ferulic Acid Treats Gastric Ulcer via Suppressing Oxidative Stress and Inflammation. Life. 2023; 13(2):388. https://doi.org/10.3390/life13020388
Chicago/Turabian StyleErmis, Aleyna, Gozde Aritici Colak, Merve Acikel-Elmas, Serap Arbak, and Meltem Kolgazi. 2023. "Ferulic Acid Treats Gastric Ulcer via Suppressing Oxidative Stress and Inflammation" Life 13, no. 2: 388. https://doi.org/10.3390/life13020388