

Relationship between Nutrition, Lifestyle Habits and Laboratory Parameters in Hypertensive Patients with/without Cognitive Dysfunction
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Data Collection and Paraclinical Tests
2.3. Statistics
3. Results
3.1. Demographic Data Results
3.2. Laboratory Parameters Comparison in the Study Groups
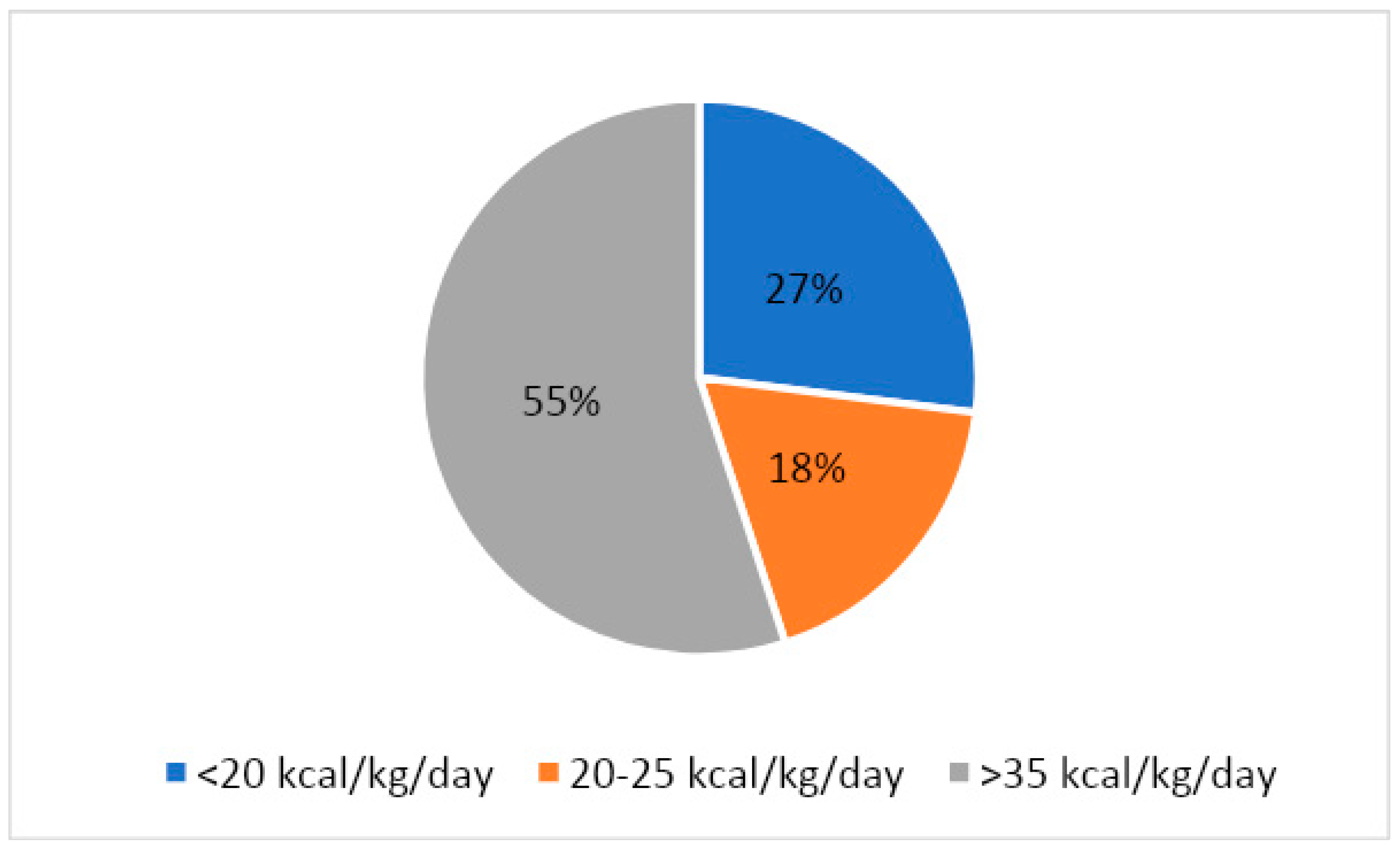
3.3. Dietary Intake and Nutritional Status of the Subjects
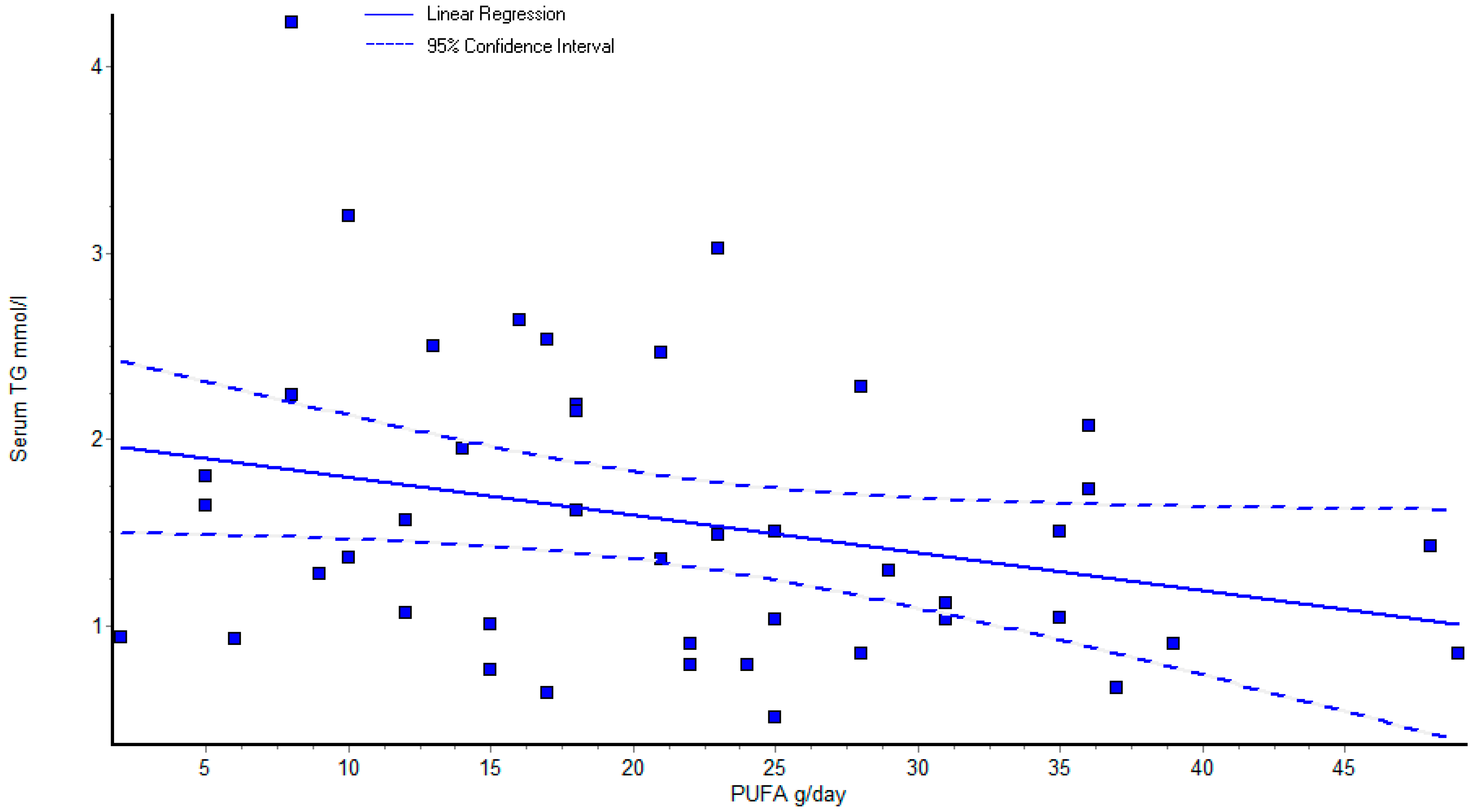
3.4. Correlations of Laboratory Parameters and Diet
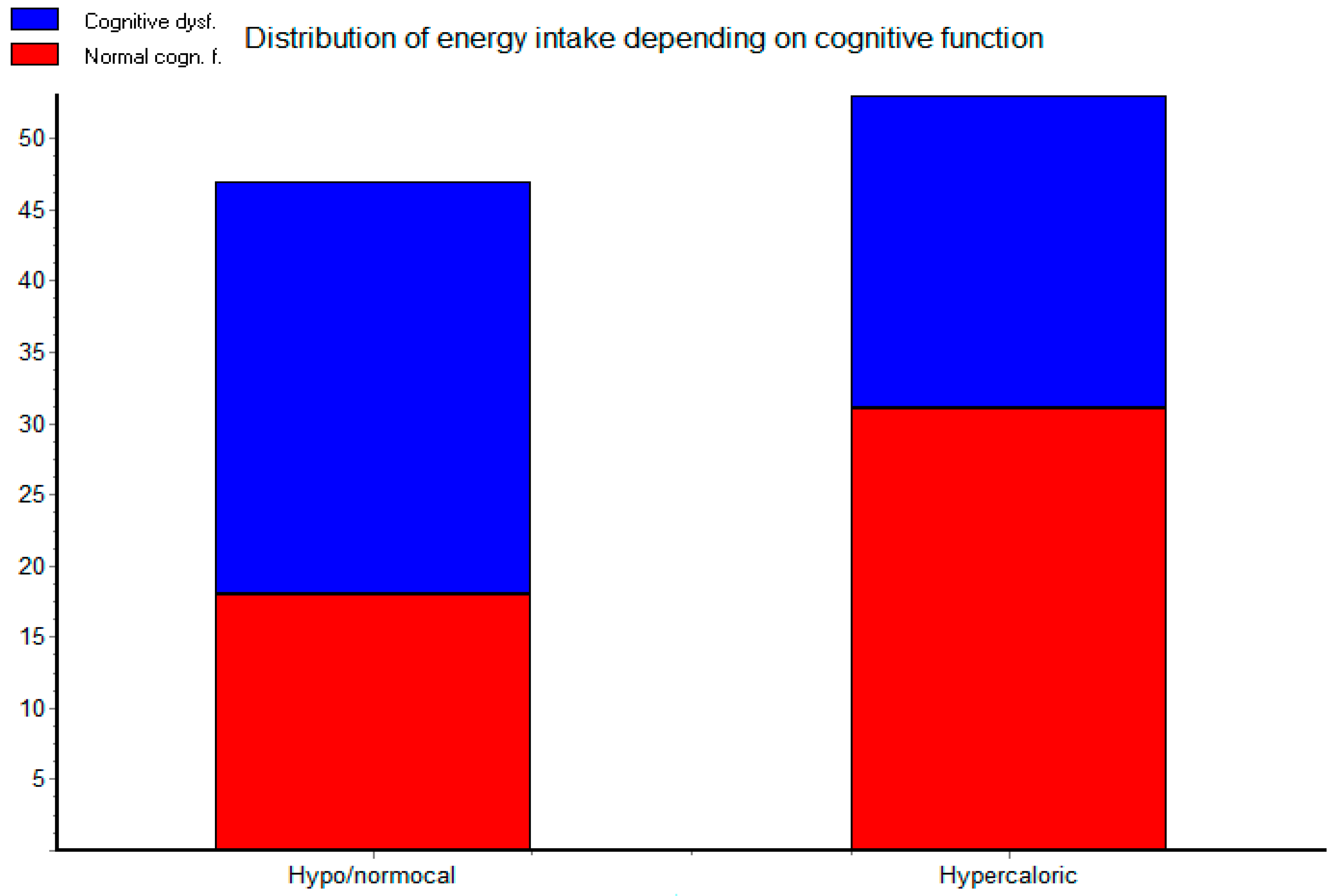
3.5. Distribution of Cognitive Dysfunction according to Diet
4. Discussion
Nutritional Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| DM | diabetes mellitus |
| ESR | erythrocyte sedimentation rate |
| HDL | high density lipoproteins |
| hsCRP | high sensitivity C reactive protein |
| LDL | low density lipoproteins |
| MOCA | Montreal Cognitive Assessment |
| NIH | National Institutes of Health |
| PUFA | polyunsaturated fatty acids |
References
- Dorobanţu, M.; Darabont, R.; Ghiorghe, S.; Georgescu, C.A.; Macarie, C.; Mitu, F.; Lighezan, D.; Musetescu, R.; Pop, C.; Ardeleanu, E.; et al. Hypertension prevalence and control in Romania at a seven-year interval. Comparison of SEPHAR I and II surveys. J. Hypertens. 2014, 32, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Tilea, I.; Petra, D.; Voidazan, S.; Ardeleanu, E.; Varga, A. Treatment adherence among adult hypertensive patients: A cross-sectional retrospective study in primary care in Romania. Patient Prefer. Adherence 2018, 12, 625–635. [Google Scholar] [CrossRef] [Green Version]
- Nepali, P.; Suresh, S.; Pikale, G.; Jhaveri, S.; Chaithanya, A.; Bansal, M.; Islam, R.; Chanpura, A. Hypertension and the Role of Dietary Fiber. Curr. Probl. Cardiol. 2022, 47, 101203. [Google Scholar] [CrossRef] [PubMed]
- Pop, C.; Gheorghe Fronea, O.F.; Branea, I.A.; Itu, L.M.; Darabont, R.; Parepa, I.; Benedek, T.; Dorobantu, M. Prevalence and Predictors of Renal Disease in a National Representative Sample of the Romanian Adult Population: Data from the SEPHAR IV Survey. Diagnostics 2022, 12, 3199. [Google Scholar] [CrossRef] [PubMed]
- Dorobantu, M.; Vijiiac, A.E.; Fronea, O.F.G. The SEPHAR-FUp 2020 Project (Study for the Evaluation of Prevalence of Hypertension and Cardiovascular Risk in Romania-Follow-up 2020). J. Hypertens. Res. 2021, 7, 29–33. [Google Scholar]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 36, 1953–2041. [Google Scholar]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 10 December 2022).
- Sánchez-Nieto, J.M.; Rivera-Sánchez, U.D.; Mendoza-Núñez, V.M. Relationship between Arterial Hypertension with Cognitive Performance in Elderly. Syst. Rev. Meta-Analysis Brain Sci. 2021, 11, 1445. [Google Scholar]
- Ungvari, Z.; Toth, P.; Tarantini, S.; Prodan, C.I.; Sorond, F.; Merkely, B.; Csiszar, A. Hypertension-induced cognitive impairment: From pathophysiology to public health. Nat. Rev. Nephrol. 2021, 17, 639–654. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Hemmelgarn, B.; Alhaider, S.; Quan, H.; Campbell, N.; Rabi, D. Meta-Analysis of Adverse Cardiovascular Outcomes Associated With Antecedent Hypertension After Myocardial Infarction. Am. J. Cardiol. 2009, 104, 141–147. [Google Scholar] [CrossRef]
- Luo, D.; Cheng, Y.; Zhang, H.; Ba, M.; Chen, P.; Li, H.; Chen, K.; Sha, W.; Zhang, C.; Chen, H. Association between high blood pressure and long term cardiovascular events in young adults: Systematic review and meta-analysis. BMJ 2020, 370, m3222. [Google Scholar] [CrossRef]
- Wajngarten, M.; Silva, G. Hypertension and Stroke: Update on Treatment. Eur. Cardiol. 2019, 14, 111–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics 2017. Eur. Heart J. 2018, 39, 508–579. [Google Scholar]
- Muela, H.C.; Costa-Hong, V.A.; Yassuda, M.S.; Moraes, N.C.; Memória, C.M.; Machado, M.F.; Macedo, T.A.; Shu, E.B.; Massaro, A.R.; Nitrini, R.; et al. Hypertension Severity Is Associated With Impaired Cognitive Performance. J. Am. Heart Assoc. 2017, 6, e004579. [Google Scholar] [CrossRef] [Green Version]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Sierra, C.; Doménech, M.; Camafort-Babkowski, M.; Coca, A. Hypertension and Mild Cognitive Impairment. Curr. Hypertens Rep. 2012, 14, 548–555. [Google Scholar] [CrossRef]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults—Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2020, 323, 764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iadecola, C. The Pathobiology of Vascular Dementia. Neuron 2013, 80, 844–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mota, M.; Dinu, I.-R. The analysis of prevalence and incidence of diabetes mellitus in Romania. Rom. J. Diabetes Nutr. Metab. Dis. 2013, 20, 135–139. [Google Scholar] [CrossRef]
- Lyu, F.; Wu, D.; Wei, C.; Wu, A.; Dan, W. Vascular cognitive impairment and dementia in type 2 diabetes mellitus: An overview. Life Sci. 2020, 254, 117771. [Google Scholar] [CrossRef]
- Serafinceanu, C.; Elian, V.I.; Catrinoiu, D.; Guja, C.; Mihai, B.; Mota, M.; Roman, G.; Timar, R. Clinical and therapeutic characteristics of patients with type 2 diabetes mellitus in Romania—MENTOR study. Rom. J. Diabetes Nutr. Metab. Dis. 2018, 25, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Tilinca, M.C.; Barabas-Hajdu, E. Involvement of inflammatory cytokines in obesity and its complications. Rev. Rom. Med. Lab. 2018, 26, 359–371. [Google Scholar] [CrossRef] [Green Version]
- Bruda, I.; Cucuianu, M. Abnormal lipid metabolism in metabolic syndrome: An epigenetic perspective. Rev. Rom. Med. Lab. 2016, 24, 153–160. [Google Scholar]
- Roberts, R.O.; Geda, Y.E.; Knopman, D.S.; Christianson, T.J.H.; Pankratz, V.S.; Boeve, B.F.; Vella, A.; Rocca, W.A.; Petersen, R.C. Association of Duration and Severity of Diabetes Mellitus With Mild Cognitive Impairment. Arch. Neurol. 2008, 65, 1066–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saedi, E.; Gheini, M.R.; Faiz, F.; Arami, M.A. Diabetes mellitus and cognitive impairments. World J. Diabetes 2016, 7, 412–422. [Google Scholar] [CrossRef]
- Pistollato, F.; Iglesias, R.C.; Ruiz, R.; Aparicio, S.; Crespo, J.; Lopez, L.D.; Manna, P.P.; Giampieri, F.; Battino, M. Nutritional patterns associated with the maintenance of neurocognitive functions and the risk of dementia and Alzheimer’s disease: A focus on human studies. Pharm. Res. 2018, 131, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.L.; Norhaizan, M.E. Effect of High-Fat Diets on Oxidative Stress, Cellular Inflammatory Response and Cognitive Function. Nutrients 2019, 11, 2579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubey, P.; Thakur, V.; Chattopadhyay, M. Role of Minerals and Trace Elements in Diabetes and Insulin Resistance. Nutrients 2020, 12, 1864. [Google Scholar] [CrossRef] [PubMed]
- Sluijs, I.; Cadier, E.; Beulens, J.; Spijkerman, A.; van der Schouw, Y. Dietary intake of carotenoids and risk of type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 376–381. [Google Scholar] [CrossRef]
- Yao, J.; Hu, P.; Zhang, D. Associations Between Copper and Zinc and Risk of Hypertension in US Adults. Biol. Trace Element Res. 2018, 186, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Refsum, H. Homocysteine, B Vitamins, and Cognitive Impairment. Annu. Rev. Nutr. 2016, 36, 211–239. [Google Scholar] [CrossRef]
- García-Sánchez, A.; Miranda-Díaz, A.G.; Cardona-Muñoz, E.G. The Role of Oxidative Stress in Physiopathology and Pharmacological Treatment with Pro- and Antioxidant Properties in Chronic Diseases. Oxid Med. Cell Longev. 2020, 2020, 2082145. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, D.; Hitomi, H.; Nishiyama, A. Hypertension with diabetes mellitus complications. Hypertens. Res. 2018, 41, 147–156. [Google Scholar] [CrossRef]
- Ohishi, M. Hypertension with diabetes mellitus: Physiology and pathology. Hypertens. Res. 2018, 41, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Villaverde, P.; Lajous, M.; Macdonald, C.-J.; Fagherazzi, G.; Bonnet, F.; Boutron-Ruault, M.-C. High dietary total antioxidant capacity is associated with a reduced risk of hypertension in French women. Nutr. J. 2019, 18, 31. [Google Scholar] [CrossRef] [PubMed]
- Sorriento, D.; De Luca, N.; Trimarco, B.; Iaccarino, G. The Antioxidant Therapy: New Insights in the Treatment of Hypertension. Front. Physiol. 2018, 9, 258. [Google Scholar] [CrossRef]
- Thakur, P.; Kumar, A. Targeting oxidative stress through antioxidants in diabetes mellitus. J. Drug Target 2018, 26, 766–776. [Google Scholar] [CrossRef]
- Ellulu, M.S. Obesity, cardiovascular disease, and role of vitamin C on inflammation: A review of facts and underlying mechanisms. Inflammopharmacology 2017, 25, 313–328. [Google Scholar] [CrossRef]
- Darroudi, S.; Saberi-Karimian, M.; Tayefi, M.; Tayefi, B.; Khashyarmanesh, Z.; Fereydouni, N.; Haghighi, H.M.; Mahmoudi, A.A.; Kharazmi-Khorassani, J.; Gonoodi, K.; et al. Association Between Hypertension in Healthy Participants and Zinc and Copper Status: A Population-Based Study. Biol. Trace Elem. Res. 2019, 190, 38–44. [Google Scholar] [CrossRef]
- Massaro, M.; Scoditti, E.; Carluccio, M.A.; De Caterina, R. Oxidative stress and vascular stiffness in hypertension: A renewed interest for antioxidant therapies? Vasc. Pharm. 2019, 116, 45–50. [Google Scholar] [CrossRef]
- Cammisotto, V.; Nocella, C.; Bartimoccia, S.; Sanguigni, V.; Francomano, D.; Sciarretta, S.; Pastori, D.; Peruzzi, M.; Cavarretta, E.; D’Amico, A.; et al. The Role of Antioxidants Supplementation in Clinical Practice: Focus on Cardiovascular Risk Factors. Antioxidants 2021, 10, 146. [Google Scholar] [CrossRef]
- National Institutes of Health, Office of Dietary Supplements. Available online: https://ods.od.nih.gov/factsheets/VitaminA-HealthProfessional (accessed on 13 December 2022).
- Nicolai, L.; Leunig, A.; Brambs, S.; Kaiser, R.; Weinberger, T.; Weigand, M.; Muenchhoff, M.; Hellmuth, J.C.; Ledderose, S.; Schulz, H.; et al. Immunothrombotic Dysregulation in COVID-19 Pneumonia Is Associated With Respiratory Failure and Coagulopathy. Circulation 2020, 142, 1176–1189. [Google Scholar] [CrossRef]
- Barbagallo, M.; Veronese, N.; Dominguez, L.J. Magnesium in Aging, Health and Diseases. Nutrients 2021, 13, 463. [Google Scholar] [CrossRef] [PubMed]
- Kostov, K.; Halacheva, L. Role of Magnesium Deficiency in Promoting Atherosclerosis, Endothelial Dysfunction, and Arterial Stiffening as Risk Factors for Hypertension. Int. J. Mol. Sci. 2018, 19, 1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Xun, P.; Tang, Q.; Cai, W.; He, K. Circulating magnesium levels and incidence of coronary heart diseases, hypertension, and type 2 diabetes mellitus: A meta-analysis of prospective cohort studies. Nutr. J. 2017, 16, 60. [Google Scholar] [CrossRef]
- Dueñas Ricaurte, J.; Ordoñez Araque, R.; Suarez Varela, M.M. Evaluation of zinc levels in biological samples of hypertensive patients in Valladolid, Spain. Nutr. Clín. Diet. Hosp. 2020, 40, 133–140. [Google Scholar]
- Freitas, E.P.S.; Cunha, A.T.O.; Aquino, S.L.S.; Pedrosa, L.F.C.; Lima, S.C.V.C.; Lima, J.G.; Almeida, M.G.; Sena-Evangelista, K.C.M. Zinc Status Biomarkers and Cardiometabolic Risk Factors in Metabolic Syndrome: A Case Control Study. Nutrients 2017, 9, 175. [Google Scholar] [CrossRef]
- Williams, C.R.; Mistry, M.; Cheriyan, A.M.; Williams, J.M.; Naraine, M.K.; Ellis, C.L.; Mallick, R.; Mistry, A.C.; Gooch, J.L.; Ko, B.; et al. Zinc deficiency induces hypertension by promoting renal Na + reabsorption. Am. J. Physiol. Renal Physiol. AM. J. Physiol-Renal 2019, 316, F646–F653. [Google Scholar] [CrossRef]
- Suliburska, J.; Skrypnik, K.; Szulińska, M.; Kupsz, J.; Bogdański, P. Effect of hypotensive therapy combined with modified diet or zinc supplementation on biochemical parameters and mineral status in hypertensive patients. J. Trace Elem. Med. Biol. 2018, 47, 140–148. [Google Scholar] [CrossRef]
- SKunutsor, K.; Laukkanen, J.A. Serum zinc concentrations and incident hypertension. J. Hypertens 2016, 34, 1055–1061. [Google Scholar] [CrossRef] [Green Version]
- Choi, S.; Liu, X.; Pan, Z. Zinc deficiency and cellular oxidative stress: Prognostic implications in cardiovascular diseases. Acta Pharmacol. Sin. 2018, 39, 1120–1132. [Google Scholar] [CrossRef] [Green Version]
- Marques, F.Z.; Nelson, E.; Chu, P.Y.; Horlock, D.; Fiedler, A.; Ziemann, M.; Tan, J.K.; Kuruppu, S.; Rajapakse, N.W.; El-Osta, A.; et al. High-Fiber Diet and Acetate Supplementation Change the Gut Microbiota and Prevent the Development of Hypertension and Heart Failure in Hypertensive Mice. Circulation 2017, 135, 964–977. [Google Scholar] [CrossRef] [PubMed]
- Woolf, K.J.; Bisognano, J.D. Nondrug Interventions for Treatment of Hypertension. J. Clin. Hypertens. 2011, 13, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Anstey, K.J.; Ashby-Mitchell, K.; Peters, R. Updating the Evidence on the Association between Serum Cholesterol and Risk of Late-Life Dementia: Review and Meta-Analysis. J. Alzheimer's Dis. 2017, 56, 215–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EKorcz; Kerényi, Z.; Varga, L. Dietary fibers, prebiotics, and exopolysaccharides produced by lactic acid bacteria: Potential health benefits with special regard to cholesterol-lowering effects. Food Funct. 2018, 9, 3057–3068. [Google Scholar] [CrossRef]
- Arsic, A.; Takic, M.; Kojadinovic, M.; Petrovic, S.; Paunovic, M.M.; Vucic, V.; Medic, D.R. Metabolically healthy obesity: Is there a link with polyunsaturated fatty acid intake and status? Can. J. Physiol. Pharmacol. 2021, 99, 64–71. [Google Scholar] [CrossRef]
- Huang, M.-C.; Chang, C.-I.; Chang, W.-T.; Liao, Y.-L.; Chung, H.-F.; Hsu, C.-C.; Shin, S.-J.; Lin, K.-D. Blood biomarkers of various dietary patterns correlated with metabolic indicators in Taiwanese type 2 diabetes. Food Nutr. Res. 2019, 63, 1. [Google Scholar] [CrossRef]
- Goligorsky, M.S. Vascular endothelium in diabetes. Am. J. Physiol. Renal Physiol. AM. J. Physiol.-Renal. 2017, 312, F266–F275. [Google Scholar] [CrossRef] [Green Version]
- Aronow, W.S. Association of obesity with hypertension. Ann. Transl. Med. 2017, 5, 350. [Google Scholar] [CrossRef]
- Lopez-Candales, A.; Burgos, P.H.; Hernandez-Suarez, D.; Harris, D. Linking Chronic Inflammation with Cardiovascular Disease: From Normal Aging to the Metabolic Syndrome. J. Nat. Sci. 2017, 3, 4. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Unit | Hypertensives with Cognitive Dysfunction | Hypertensives without Cognitive Dysfunction | Statistical Significance |
|---|---|---|---|---|
| Duration of hypertension | years | 19.08 ± 12.27 | 17.08 ± 12.19 | p = 0.574 |
| BMI | kg/m2 | 32.61 ± 7.43 | 27.82 ± 4.36 | p = 0.009 * |
| Glycemia | mmol/L | 5.99 ± 1.26 | 5.53 ± 1.02 | p = 0.159 |
| Cholesterol | mmol/L | 4.48 ± 1.03 | 5.06 ± 1.15 | p = 0.071 |
| Triglycerides | mmol/L | 1.53 ± 0.89 | 1.58 ± 0.68 | p = 0.813 |
| HDL | mg/dL | 44.76 ± 13.52 | 50.14 ± 12.60 | p = 0.152 |
| LDL | mmol/L | 2.61 ±1.11 | 3.05 ± 1.03 | p = 0.156 |
| Uric acid | µmol/L | 303.76 ± 78.85 | 278.84 ± 96.95 | p = 0.324 |
| Creatinine | mg/dL | 0.99 ±0.22 | 0.99 ± 0.26 | p = 0.940 |
| Cystatin C | mg/L | 1.11 ± 0.34 | 1.12 ± 0.24 | p = 0.955 |
| Zinc | µmol/L | 10.21 ± 1.58 | 9.99 ± 1.65 | p = 0.631 |
| HsCRP | mg/L | 2.94 ± 3.76 | 1.56 ± 1.82 | p = 0.107 |
| ESR | mm/h | 14.36 ± 8.89 | 10.76 ± 7.49 | p = 0.128 |
| Fibrinogen | g/dL | 3.92 ± 1.08 | 3.39 ± 0.74 | p = 0.066 |
| Dietary Intake/Day | Unit | Hypertensives with Cognitive Dysfunction | Hypertensives without Cognitive Dysfunction | Statistical Significance |
|---|---|---|---|---|
| Energy | kcal/day | 2157.39 ± 974.80 | 2296.41 ± 860.65 | p = 0.615 |
| Water | mL/day | 1423.00 ± 457.16 | 1620.59 ± 520.55 | p = 0.183 |
| Protein | g/day | 90.43 ± 39.63 | 96.18 ± 41.60 | p = 0.637 |
| Fat | g/day | 94.43 ± 46.83 | 103.45 ± 43.24 | p = 0.506 |
| Carbohydrates | g/day | 215.39 ± 82.88 | 232.09 ± 81.06 | p = 0.498 |
| Dietary fibers | g/day | 26.70 ± 9.53 | 31.45 ± 11.70 | p = 0.141 |
| PUFA | g/day | 19.43 ± 12.12 | 23.18 ± 10.35 | p = 0.272 |
| Cholesterol | mg/day | 288.61 ± 139.08 | 409.27 ± 198.69 | p = 0.022 * |
| Alcohol | g/day | 1.83 ± 5.01 | 3.05 ± 4.45 | p = 0.393 |
| Dietary Intake/Day | Unit | Hypertensives with Cognitive Dysfunction | Hypertensives without Cognitive Dysfunction | Statistical Significance |
|---|---|---|---|---|
| Vitamin A | µg/day | 1606.17 ± 617.77 | 1909.45 ± 796.24 | p = 0.160 |
| Carotene | mg/day | 6.09 ± 2.43 | 7.18 ± 3.07 | p = 0.190 |
| Vitamin E | mg/day | 22.74 ± 14.16 | 26.09 ± 12.03 | p = 0.398 |
| Vitamin B1 | mg/day | 1.17 ± 0.65 | 1.27 ± 0.77 | p = 0.643 |
| Vitamin B2 | mg/day | 1.74 ± 0.81 | 1.95 ± 0.79 | p = 0.370 |
| Vitamin B6 | mg/day | 1.78 ± 0.78 | 2.05 ± 0.79 | p = 0.271 |
| Folic acid | µg/day | 298.09 ± 141.77 | 362.68 ± 150.52 | p = 0.145 |
| Vitamin C | mg/day | 193.52 ± 98.64 | 209.68 ± 106.60 | p = 0.600 |
| Sodium | mg/day | 1767.57 ± 952.17 | 1797.18 ± 762.79 | p = 0.909 |
| Potassium | mg/day | 3389.65 ± 1266.35 | 3932.41 ± 1493.86 | p = 0.195 |
| Calcium | mg/day | 1399.96 ± 1188.14 | 1196.77 ± 555.03 | p = 0.470 |
| Magnesium | mg/day | 323.65 ± 126.61 | 419.45 ± 159.56 | p = 0.032 * |
| Phosphorus | mg/day | 1376.17 ± 614.93 | 1615.09 ± 634.38 | p = 0.206 |
| Iron | mg/day | 13.35 ± 5.21 | 15.91 ± 6.06 | p = 0.135 |
| Zinc | mg/day | 13.52 ± 6.04 | 14.00 ± 6.10 | p = 0.793 |
| Parameter | Unit | Reference Range Male Patients | Reference Range Female Patients | Notes |
|---|---|---|---|---|
| Glycemia | mmol/L | 3.5–5.6 | 3.5–5.6 | For non-diabetics |
| Cholesterol | mmol/L | 3.9–5.2 | 3.9–5.2 | In high risk group < 4.6 |
| Triglycerides | mmol/L | 0.45–1.81 | 0.40–1.52 | |
| HDL | mg/dL | >40 | >50 | |
| LDL | mmol/L | <2.6 | <2.6 | |
| Uric acid | µmol/L | 240–510 | 160–430 | |
| Creatinine | mg/dL | 0.74–1.35 | 0.59–1.04 | |
| Cystatin C | mg/L | 0.7–1.10 | 0.57–1.03 | |
| Zinc | µmol/L | 10.4–16.4 | 10.4–16.4 | |
| HsCRP | mg/L | <1 | <1 | |
| ESR | mm/h | 5–15 | 5–17 | |
| Fibrinogen | g/dL | 2.0–4.0 | 2.0–4.0 | |
| Microalbuminuria | mg/24 h | <30 | <30 |
| Dietary Intake/Day | Units | Recommended/Acceptable for Healthy Subjects | Special Recommendations (Hypertension/Overweight) |
|---|---|---|---|
| Energy | kcal/day | 30–35 kcal/kg | 20–25 kcal/kg |
| Water | mL/day | 30–35 mL/kg | |
| Alcohol | g/day | acceptable moderate intake: 20–30 g/day in males 10–20 g/day in females | No alcohol intake |
| Protein | g/day | 12–20% of total calories (0.8–2.0 g/kg) 46–56 g/day | 15–18% of total calories (1.0–1.8 g/kg) |
| Fat | g/day | 20–35% of total calories (<10% saturated) 44–77 g/day | 20–30% of total calories (<6% saturated) |
| Carbohydrates | g/day | 45–65% of total calories 174–194 g/day | 45–55% of total calories |
| Dietary fibers | g/day | 30 g/day | |
| PUFA | g/day | 6–11% of total calories 1.1–1.6 g/day | |
| Cholesterol | mg/day | <300 mg/day | <150 mg/day |
| Dietary Intake/Day | Units | Recommended/Acceptable for Healthy Subjects | Special Recommendations (Hypertension/Overweight) |
|---|---|---|---|
| Vitamin A | µg/day | 900 µg/day in males 700 µg/day in females | |
| Carotene | mg/day | 12–15 mg/day | |
| Vitamin E | mg/day | 12–20 mg/day | |
| Vitamin B1 | mg/day | 1–2 mg/day | |
| Vitamin B2 | mg/day | 1.1–1.2 mg/day | |
| Vitamin B6 | mg/day | 2 mg/day | |
| Folic acid | µg/day | 400 µg/day | |
| Vitamin C | mg/day | >120 mg/day | |
| Sodium | mg/day | 5–6 g/day | 1.5–3 g/day |
| Potassium | mg/day | 4600–4800 mg/day | |
| Calcium | mg/day | 850–1500 mg/day | |
| Magnesium | mg/day | 400–500 mg/day | |
| Phosphorus | mg/day | 800–1000 mg/day | |
| Iron | mg/day | 10–18 mg/day | |
| Zinc | mg/day | 12–15 mg/day |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nyulas, K.-I.; Germán-Salló, M.; Fazakas, Z.; Preg, Z.; Pál, T.; Pál, S.; Tripon, R.G.; Cseh, M.J.; Simon-Szabó, Z.; Arbănași, E.M.; et al. Relationship between Nutrition, Lifestyle Habits and Laboratory Parameters in Hypertensive Patients with/without Cognitive Dysfunction. Life 2023, 13, 311. https://doi.org/10.3390/life13020311
Nyulas K-I, Germán-Salló M, Fazakas Z, Preg Z, Pál T, Pál S, Tripon RG, Cseh MJ, Simon-Szabó Z, Arbănași EM, et al. Relationship between Nutrition, Lifestyle Habits and Laboratory Parameters in Hypertensive Patients with/without Cognitive Dysfunction. Life. 2023; 13(2):311. https://doi.org/10.3390/life13020311
Chicago/Turabian StyleNyulas, Kinga-Ilona, Márta Germán-Salló, Zita Fazakas, Zoltán Preg, Tünde Pál, Sándor Pál, Robert Gabriel Tripon, Margit Judit Cseh, Zsuzsánna Simon-Szabó, Emil Marian Arbănași, and et al. 2023. "Relationship between Nutrition, Lifestyle Habits and Laboratory Parameters in Hypertensive Patients with/without Cognitive Dysfunction" Life 13, no. 2: 311. https://doi.org/10.3390/life13020311