
The Diagnostic Accuracy of SARS-CoV-2 Nasal Rapid Antigen Self-Test: A Systematic Review and Meta-Analysis
 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol and Guidelines
2.2. Eligibility Criteria
- Use of self-taken rapid antigen test as an index test;
- Use of rt-PCR as a reference standard;
- Presence of the sensitivity and specificity of rapid antigen test;
- Use of nasal specimen;
- English language.
- Duplicate articles;
- Original investigation;
- Reviews;
- Editorials;
- Letters;
- Comments;
- Meta-analysis articles.
2.3. Information Sources, Search Strategy and Selection Process
2.4. Data Collection Process and Data Items
2.5. Study Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
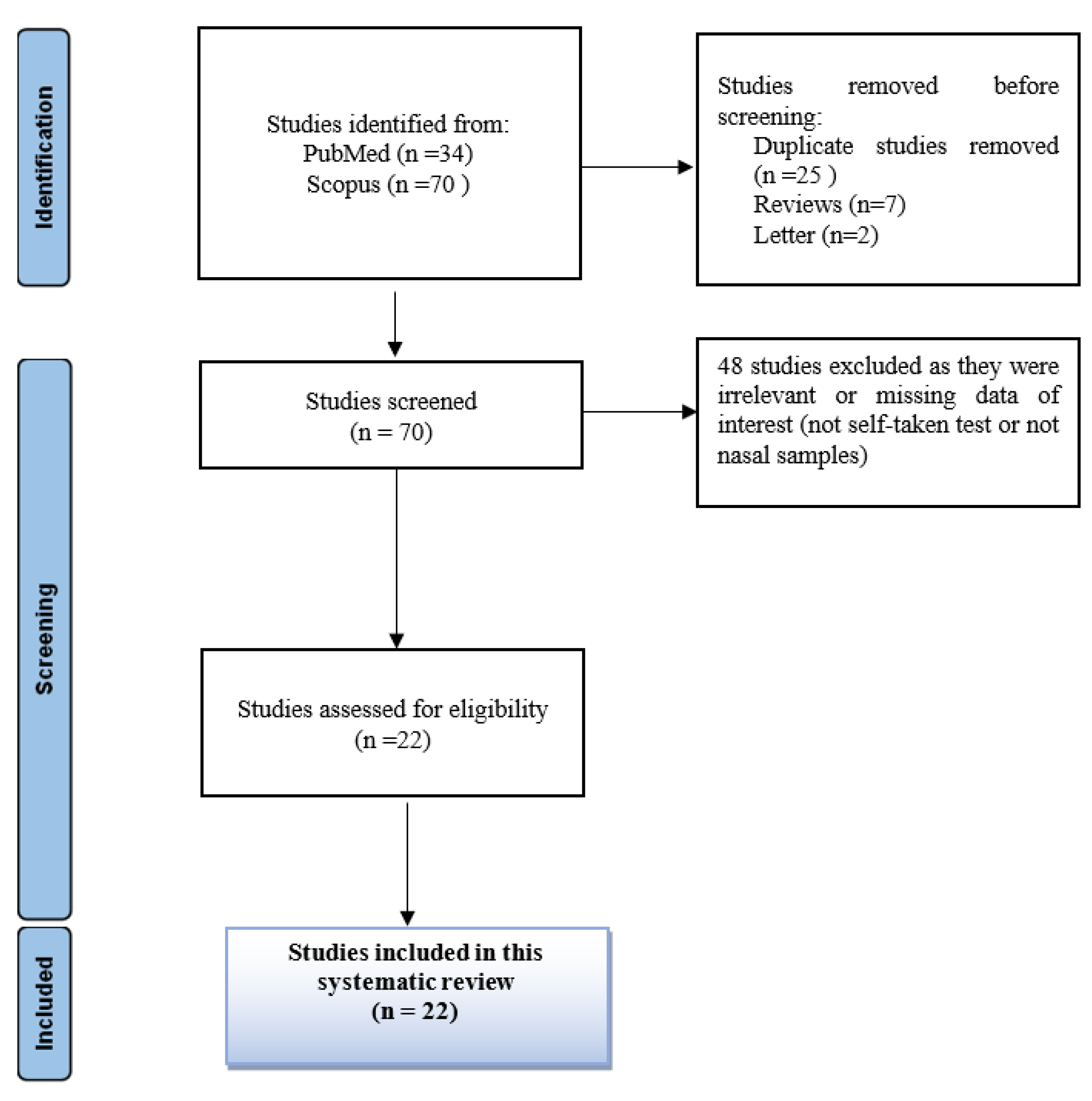
3.1. Study Selection
3.2. Study Characteristics
- Sensitivity = TP/(TP + FN);
- Specificity = TN/(TN + FP);
- Negative predictive value (NPV) = TN/(TN + FN);
- Positive predictive value (PPV) = TP/(TP + FP);
- Accuracy = (TP + TN)/(TP + TN + FP + FN).
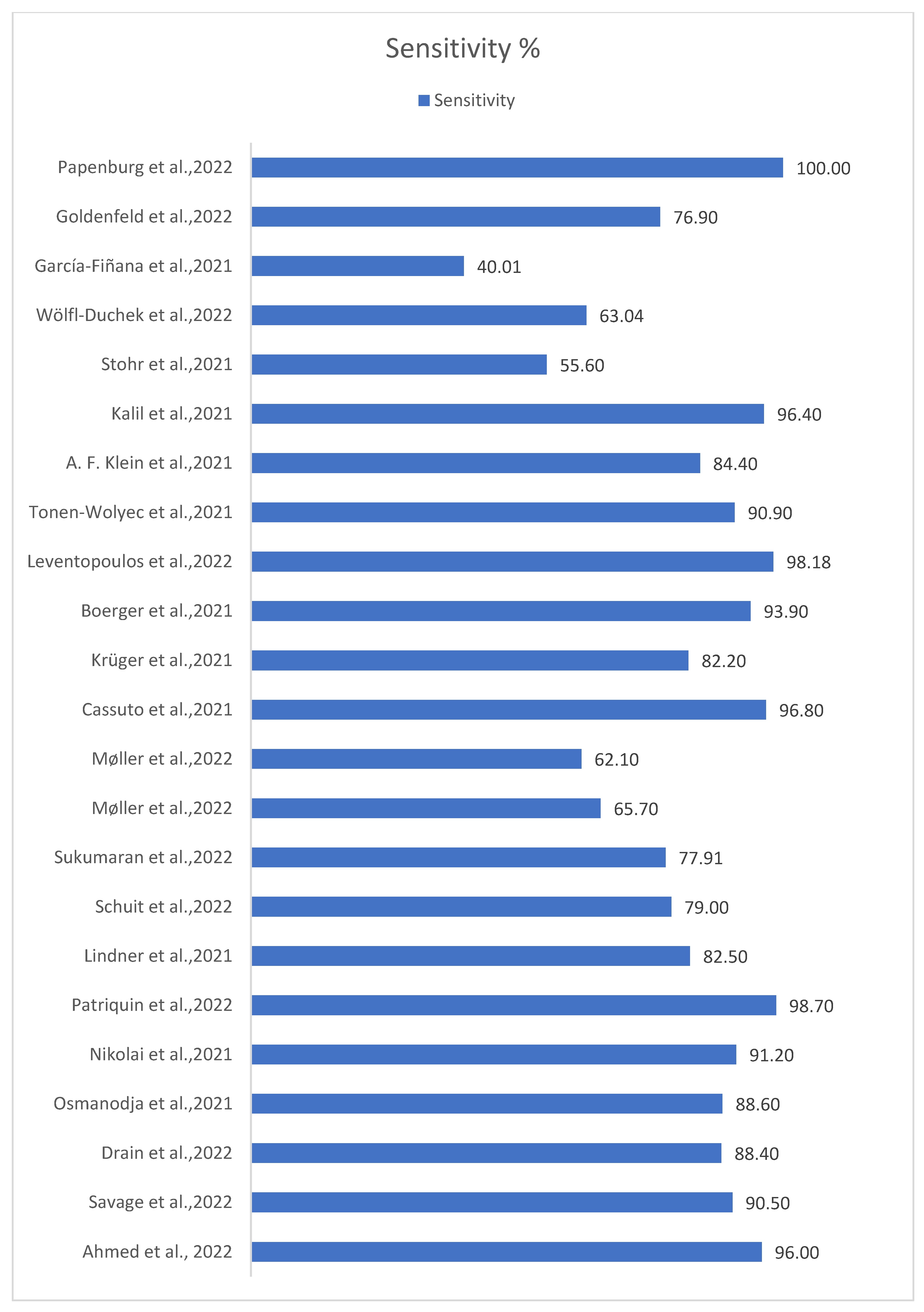
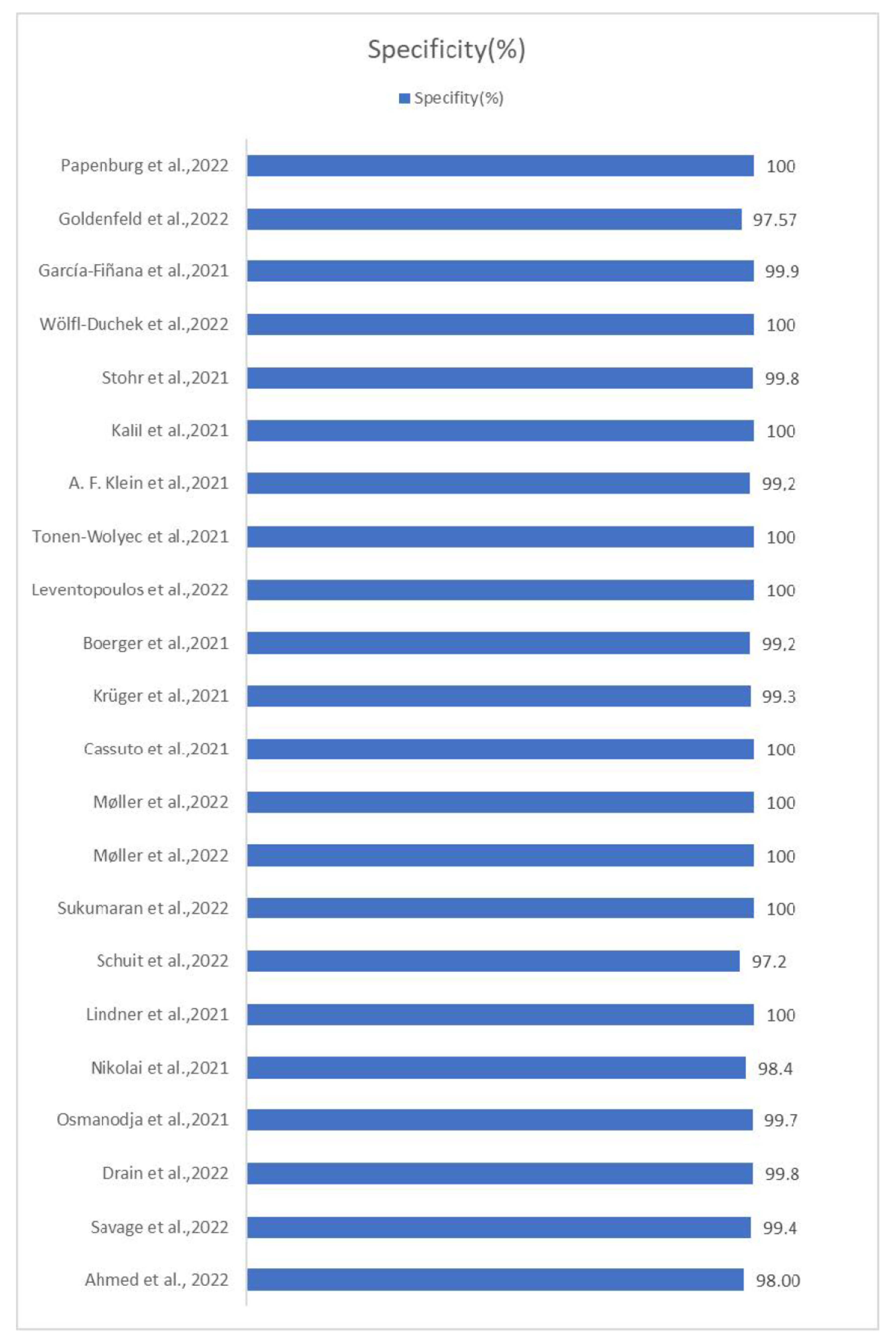
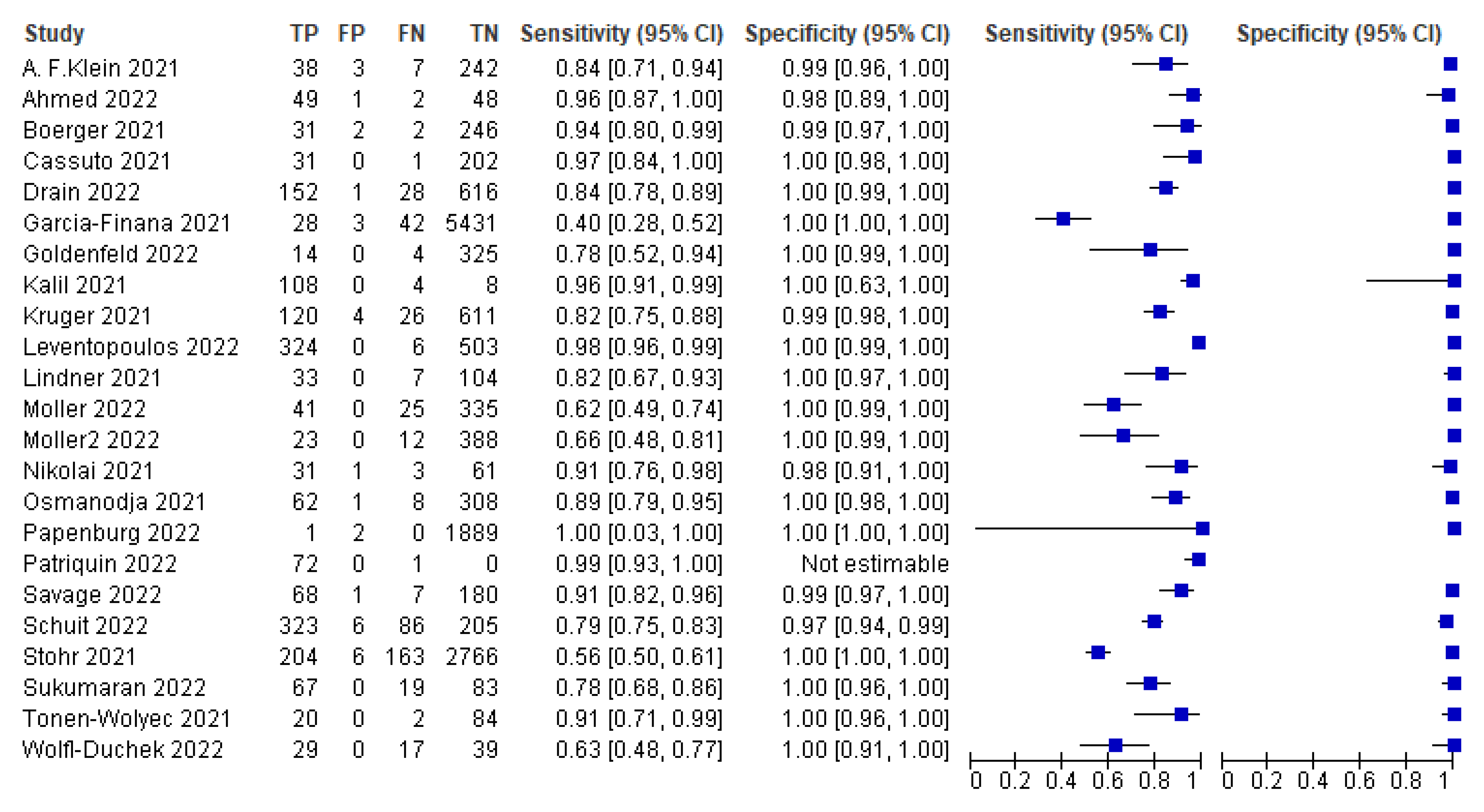
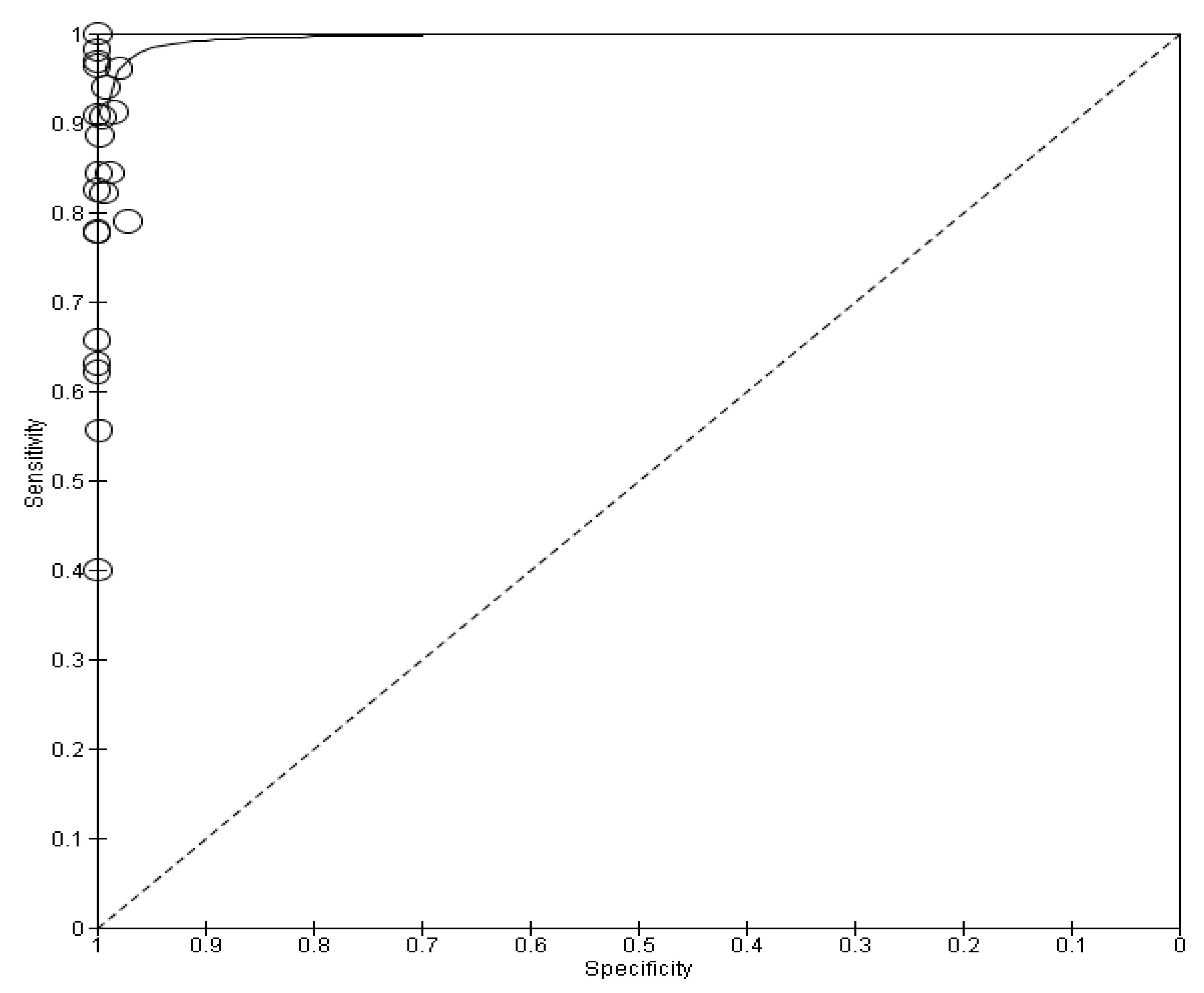
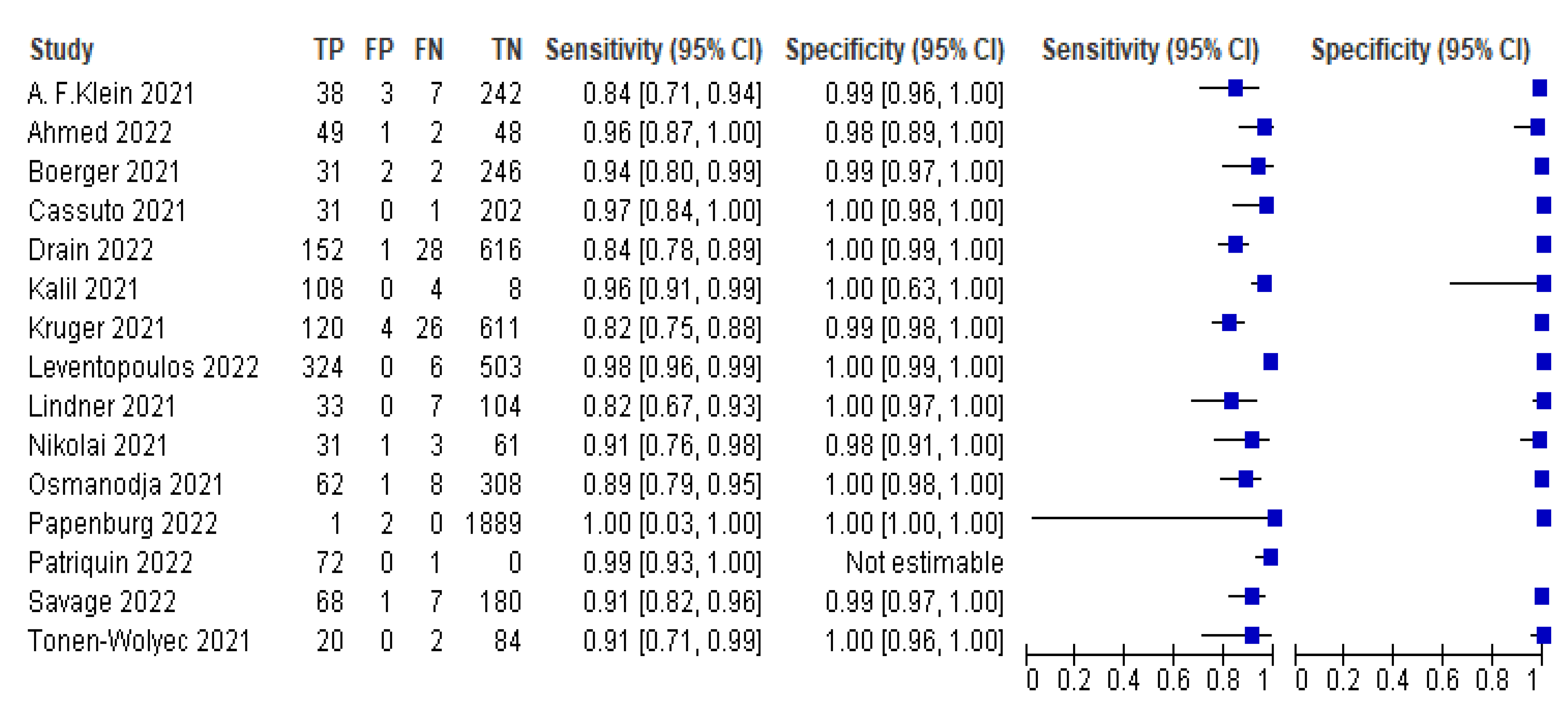
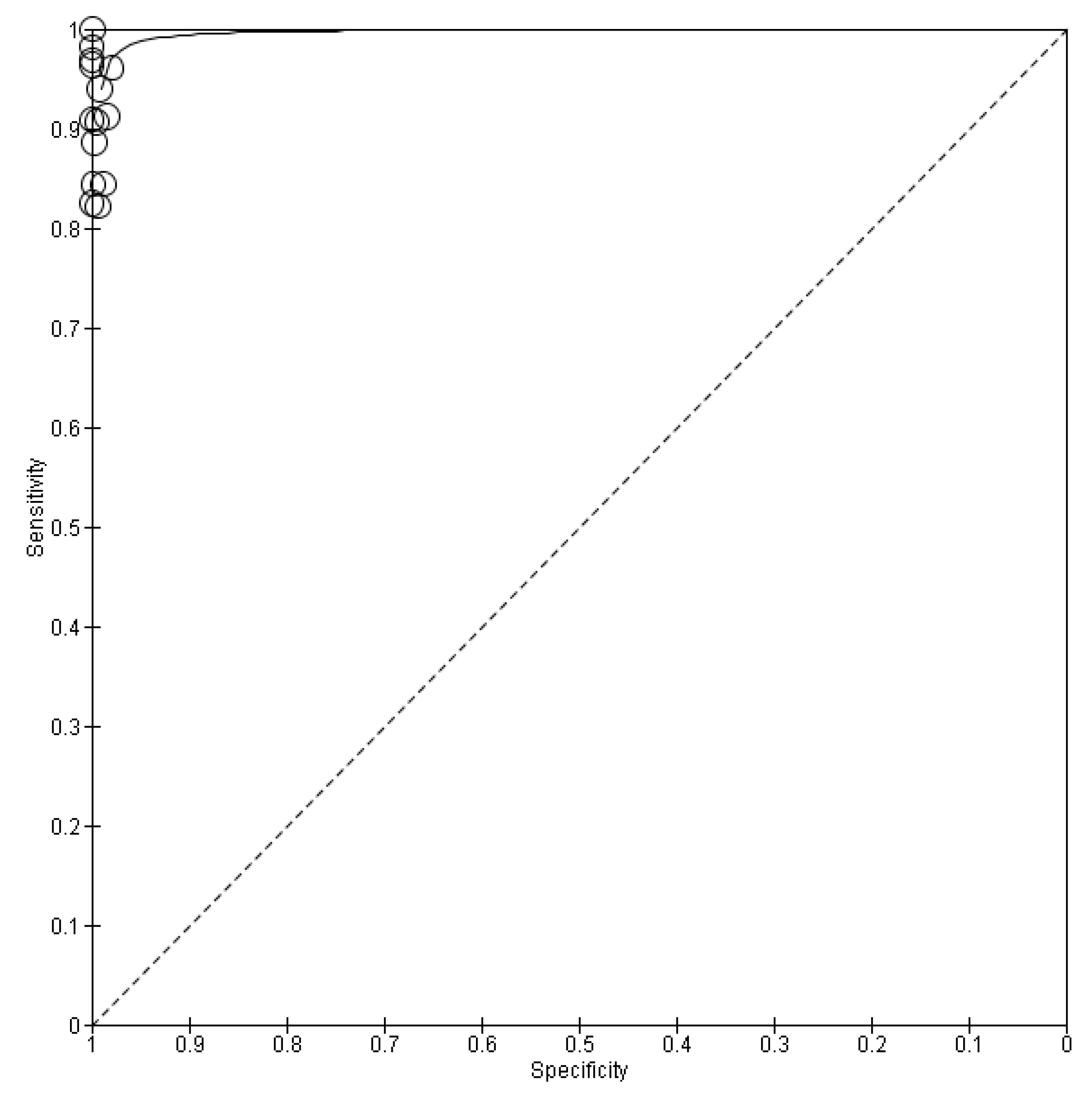
3.3. Meta-Analysis
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Shi, Y.; Wang, G.; Cai, X.-P.; Deng, J.-W.; Zheng, L.; Zhu, H.-H.; Zheng, M.; Yang, B.; Chen, Z. An overview of COVID-19. J. Zhejiang Univ. Sci. B 2020, 21, 343–360. [Google Scholar] [CrossRef]
- Umakanthan, S.; Sahu, P.; Ranade, A.V.; Bukelo, M.M.; Rao, J.S.; Lf, A.-M.; Dahal, S.; Kumar, H.; Kv, D. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad. Med. J. 2020, 96, 753–768. [Google Scholar] [CrossRef]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Song, W.-J.; Hui, C.K.M.; Hull, J.H.; Birring, S.S.; McGarvey, L.; Mazzone, S.B.; Chung, K.F. Confronting COVID-19-associated cough and the post-COVID syndrome: Role of viral neurotropism, neuroinflammation, and neuroimmune responses. Lancet Respir. Med. 2021, 9, 533–544. [Google Scholar] [CrossRef]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef]
- D’Cruz, R.J.; Currier, A.W.; Sampson, V.B. Laboratory Testing Methods for Novel Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2). Front. Cell Dev. Biol. 2020, 8, 468. [Google Scholar] [CrossRef] [PubMed]
- Filchakova, O.; Dossym, D.; Ilyas, A.; Kuanysheva, T.; Abdizhamil, A.; Bukasov, R. Review of COVID-19 testing and diagnostic methods. Talanta 2022, 244, 123409. [Google Scholar] [CrossRef]
- Fenollar, F.; Bouam, A.; Ballouche, M.; Fuster, L.; Prudent, E.; Colson, P.; Tissot-Dupont, H.; Million, M.; Drancourt, M.; Raoult, D.; et al. Evaluation of the Panbio COVID-19 Rapid Antigen Detection Test Device for the Screening of Patients with COVID-19. J. Clin. Microbiol. 2021, 59, e02589-20. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19: Laboratory and diagnosis of World Health Organization. In Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Nikolai, O.; Rohardt, C.; Tobian, F.; Junge, A.; Corman, V.M.; Jones, T.C.; Gaeddert, M.; Lainati, F.; Sacks, J.A.; Seybold, J.; et al. Anterior nasal versus nasal mid-turbinate sampling for a SARS-CoV-2 antigen-detecting rapid test: Does localisation or professional collection matter? Infect. Dis. 2021, 53, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Patriquin, G.; LeBlanc, J.J.; Williams, C.; Hatchette, T.F.; Ross, J.; Barrett, L.; Davidson, R. Comparison between Nasal and Nasopharyngeal Swabs for SARS-CoV-2 Rapid Antigen Detection in an Asymptomatic Population, and Direct Confirmation by RT-PCR from the Residual Buffer. Microbiol. Spectr. 2022, 10, e0245521. [Google Scholar] [CrossRef]
- Lindner, A.K.; Nikolai, O.; Rohardt, C.; Kausch, F.; Wintel, M.; Gertler, M.; Burock, S.; Hörig, M.; Bernhard, J.; Tobian, F.; et al. Diagnostic accuracy and feasibility of patient self-testing with a SARS-CoV-2 antigen-detecting rapid test. J. Clin. Virol. 2021, 141, 104874. [Google Scholar] [CrossRef]
- Schuit, E.; Venekamp, R.P.; Hooft, L.; Veldhuijzen, I.K.; Bijllaardt, W.V.D.; Pas, S.D.; Zwart, V.F.; Lodder, E.B.; Hellwich, M.; Koppelman, M.; et al. Diagnostic accuracy of COVID-19 rapid antigen tests with unsupervised self-sampling in people with symptoms in the omicron period: Cross sectional study. BMJ 2022, 378, e071215. [Google Scholar] [CrossRef]
- Sukumaran, A.; Suvekbala, V.; Thomas, R.E.; Raj, A.; Thomas, T.; Abhijith, B.L.; Jose, J.; Paul, J.K.; Vasudevan, D.M. Diagnostic Accuracy of SARS-CoV-2 Nucleocapsid Antigen Self-Test in Comparison to Reverse Transcriptase–Polymerase Chain Reaction. J. Appl. Lab. Med. 2022, 7, 871–880. [Google Scholar] [CrossRef]
- Møller, I.J.B.; Utke, A.R.; Rysgaard, U.K.; Østergaard, L.J.; Jespersen, S. Diagnostic performance, user acceptability, and safety of unsupervised SARS-CoV-2 rapid antigen-detecting tests performed at home. Int. J. Infect. Dis. 2022, 116, 358–364. [Google Scholar] [CrossRef]
- Cassuto, N.G.; Gravier, A.; Colin, M.; Theillay, A.; Pires-Roteira, D.; Pallay, S.; Serreau, R.; Hocqueloux, L.; Prazuck, T. Evaluation of a SARS-CoV-2 antigen-detecting rapid diagnostic test as a self-test: Diagnostic performance and usability. J. Med. Virol. 2021, 93, 6686–6692. [Google Scholar] [CrossRef]
- Krüger, L.J.; Klein, J.A.F.; Tobian, F.; Gaeddert, M.; Lainati, F.; Klemm, S.; Schnitzler, P.; Bartenschlager, R.; Cerikan, B.; Neufeldt, C.J.; et al. Evaluation of accuracy, exclusivity, limit-of-detection and ease-of-use of LumiraDx™: An antigen-detecting point-of-care device for SARS-CoV-2. Infection 2021, 50, 395–406. [Google Scholar] [CrossRef]
- Boerger, A.C.; Buckwalter, S.; Fernholz, E.C.; Jannetto, P.J.; Binnicker, M.J.; Reed, K.; Walchak, R.; Woodliff, E.; Johnson, M.; Pritt, B.S. Evaluation of Self-Collected Midturbinate Nasal Swabs and Saliva for Detection of SARS-CoV-2 RNA. J. Clin. Microbiol. 2021, 59, e0084821. [Google Scholar] [CrossRef]
- Tonen-Wolyec, S.; Dupont, R.; Awaida, N.; Batina-Agasa, S.; Hayette, M.-P.; Bélec, L. Evaluation of the Practicability of Biosynex Antigen Self-Test COVID-19 AG+ for the Detection of SARS-CoV-2 Nucleocapsid Protein from Self-Collected Nasal Mid-Turbinate Secretions in the General Public in France. Diagnostics 2021, 11, 2217. [Google Scholar] [CrossRef]
- Kalil, M.N.A.; Yusof, W.; Ahmed, N.; Fauzi, M.H.; Abu Bakar, M.A.; Sjahid, A.S.; Hassan, R.; Yean, C.Y. Performance Validation of COVID-19 Self-Conduct Buccal and Nasal Swabs RTK-Antigen Diagnostic Kit. Diagnostics 2021, 11, 2245. [Google Scholar] [CrossRef]
- Stohr, J.J.J.M.; Zwart, V.F.; Goderski, G.; Meijer, A.; Nagel-Imming, C.R.S.; Kluytmans-van den Bergh, M.F.Q.; Pas, S.D.; van den Oetelaar, F.; Hellwich, M.; Gan, K.H.; et al. Self-testing for the detection of SARS-CoV-2 infection with rapid antigen tests for people with suspected COVID-19 in the community. Clin. Microbiol. Infect. 2022, 28, 695–700. [Google Scholar] [CrossRef]
- Wölfl-Duchek, M.; Bergmann, F.; Jorda, A.; Weber, M.; Müller, M.; Seitz, T.; Zoufaly, A.; Strassl, R.; Zeitlinger, M.; Herkner, H.; et al. Sensitivity and Specificity of SARS-CoV-2 Rapid Antigen Detection Tests Using Oral, Anterior Nasal, and Nasopharyngeal Swabs: A Diagnostic Accuracy Study. Microbiol. Spectr. 2022, 10, e0202921. [Google Scholar] [CrossRef]
- García-Fiñana, M.; Hughes, D.M.; Cheyne, C.P.; Burnside, G.; Stockbridge, M.; Fowler, T.A.; Fowler, V.L.; Wilcox, M.H.; Semple, M.G.; Buchan, I. Performance of the Innova SARS-CoV-2 antigen rapid lateral flow test in the Liverpool asymptomatic testing pilot: Population based cohort study. BMJ 2021, 374, n1637. [Google Scholar] [CrossRef]
- Goldenfeld, M.B.; Cohen, C.M.-P.; Gilboa, M.; Pessach, I.M.M.-P.; Mehnick, B.R.M.; Tal, I.R.M.; Meltzer, L.B.; Amit, S.M.-P.; Gonen, T.B.; Afek, A.M.-M.; et al. Rapid Antigen Tests for Safe School Opening in the COVID-19 Pandemic Era. Pediatr. Infect. Dis. J. 2022, 41, e312–e317. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Schueler, S.; Schuetz, G.M.; Dewey, M. The Revised QUADAS-2 Tool. Ann. Intern. Med. 2012, 156, 323. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Parikh, R.; Mathai, A.; Parikh, S.; Sekhar, G.C.; Thomas, R. Understanding and using sensitivity, specificity and predictive values. Indian J. Ophthalmol. 2008, 56, 45–50. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Pandemic—Emergency Use Listing Procedure (EUL) Open for IVDs. Available online: https://extranet.who.int/pqweb/vitro-diagnostics/coronavirus-disease-covid-19-pandemic-%E2%80%94-emergency-use-listing-procedure-eul-open (accessed on 24 October 2022).
- Jian, M.-J.; Chung, H.-Y.; Chang, C.-K.; Lin, J.-C.; Yeh, K.-M.; Chen, C.-W.; Lin, D.-Y.; Chang, F.-Y.; Hung, K.-S.; Perng, C.-L.; et al. SARS-CoV-2 variants with T135I nucleocapsid mutations may affect antigen test performance. Int. J. Infect. Dis. 2021, 114, 112–114. [Google Scholar] [CrossRef]
- Ahmed, N.; Kalil, M.N.A.; Yusof, W.; Abu Bakar, M.A.; Sjahid, A.S.; Hassan, R.; Fauzi, M.H.; Yean, C.Y. A Performance Assessment Study of Different Clinical Samples for Rapid COVID-19 Antigen Diagnosis Tests. Diagnostics 2022, 12, 847. [Google Scholar] [CrossRef]
- Savage, H.R.; Finch, L.; Body, R.; Watkins, R.L.; Hayward, G.; Cook, E.; Cubas-Atienzar, A.I.; Cuevas, L.E.; MacPherson, P.; Adams, E.R.; et al. A prospective diagnostic evaluation of accuracy of self-taken and healthcare worker-taken swabs for rapid COVID-19 testing. PLoS ONE 2022, 17, e0270715. [Google Scholar] [CrossRef]
- Drain, P.K.; Bemer, M.; Morton, J.F.; Dalmat, R.; Abdille, H.; Thomas, K.K.; Uppal, T.K.; Hau, D.; Green, H.R.; Gates-Hollingsworth, M.A.; et al. Accuracy of 2 Rapid Antigen Tests During 3 Phases of SARS-CoV-2 Variants. JAMA Netw. Open 2022, 5, e2228143. [Google Scholar] [CrossRef]
- Osmanodja, B.; Budde, K.; Zickler, D.; Naik, M.; Hofmann, J.; Gertler, M.; Hülso, C.; Rössig, H.; Horn, P.; Seybold, J.; et al. Accuracy of a Novel SARS-CoV-2 Antigen-Detecting Rapid Diagnostic Test from Standardized Self-Collected Anterior Nasal Swabs. J. Clin. Med. 2021, 10, 2099. [Google Scholar] [CrossRef]
- Papenburg, J.; Campbell, J.R.; Caya, C.; Dion, C.; Corsini, R.; Cheng, M.P.; Menzies, D.; Yansouni, C.P. Adequacy of Serial Self-performed SARS-CoV-2 Rapid Antigen Detection Testing for Longitudinal Mass Screening in the Workplace. JAMA Netw. Open 2022, 5, e2210559. [Google Scholar] [CrossRef]
- Leventopoulos, M.; Michou, V.; Papadimitropoulos, M.; Vourva, E.; Manias, N.G.; Kavvadas, H.P.; Nikolopoulos, D.; Tsilivakos, V.; Georgoulias, G. Evaluation of the Boson rapid Ag test vs RT–PCR for use as a self–testing platform. Diagn. Microbiol. Infect. Dis. 2022, 104, 115786. [Google Scholar] [CrossRef]
- Klein, J.A.F.; Krüger, L.J.; Tobian, F.; Gaeddert, M.; Lainati, F.; Schnitzler, P.; Lindner, A.K.; Nikolai, O.; Knorr, B.; Welker, A.; et al. Head-to-head performance comparison of self-collected nasal versus professional-collected nasopharyngeal swab for a WHO-listed SARS-CoV-2 antigen-detecting rapid diagnostic test. Med. Microbiol. Immunol. 2021, 210, 181–186. [Google Scholar] [CrossRef]
- Böger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control 2020, 49, 21–29. [Google Scholar] [CrossRef]
- Garg, A.; Ghoshal, U.; Patel, S.S.; Singh, D.V.; Arya, A.K.; Vasanth, S.; Pandey, A.; Srivastava, N. Evaluation of seven commercial RT-PCR kits for COVID-19 testing in pooled clinical specimens. J. Med. Virol. 2020, 93, 2281–2286. [Google Scholar] [CrossRef]
- Jing, M.; Bond, R.; Robertson, L.J.; Moore, J.; Kowalczyk, A.; Price, R.; Burns, W.; Nesbit, M.A.; McLaughlin, J.; Moore, T. User experience of home-based AbC-19 SARS-CoV-2 antibody rapid lateral flow immunoassay test. Sci. Rep. 2022, 12, 1173. [Google Scholar] [CrossRef]
- Parvu, V.; Gary, D.S.; Mann, J.; Lin, Y.-C.; Mills, D.; Cooper, L.; Andrews, J.C.; Manabe, Y.C.; Pekosz, A.; Cooper, C.K. Factors that Influence the Reported Sensitivity of Rapid Antigen Testing for SARS-CoV-2. Front. Microbiol. 2021, 12, 714242. [Google Scholar] [CrossRef]
- Amer, R.M.; Samir, M.; Gaber, O.A.; El-Deeb, N.A.; Abdelmoaty, A.A.; Ahmed, A.A.; Samy, W.; Atta, A.H.; Walaa, M.; Anis, R.H. Diagnostic performance of rapid antigen test for COVID-19 and the effect of viral load, sampling time, subject’s clinical and laboratory parameters on test accuracy. J. Infect. Public Health 2021, 14, 1446–1453. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Khurana, S.; Das, R.; Srigyan, D.; Singh, A.; Mittal, A.; Singh, P.; Soneja, M.; Kumar, A.; Singh, A.K.; et al. Rapid chromatographic immunoassay-based evaluation of COVID-19: A cross-sectional, diagnostic test accuracy study & its implications for COVID-19 management in India. Indian J. Med. Res. 2020, 153, 126–131. [Google Scholar] [CrossRef]
- Zhao, L.; Li, L.; Liu, G.-Q.; Chen, L.; Liu, X.; Zhu, J.; Li, B. Effect of freeze–thaw cycles on the molecular weight and size distribution of gluten. Food Res. Int. 2013, 53, 409–416. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.A.; Herigon, J.C.; Benedetti, A.; Pollock, N.R.; Denkinger, C.M. Performance of Saliva, Oropharyngeal Swabs, and Nasal Swabs for SARS-CoV-2 Molecular Detection: A Systematic Review and Meta-analysis. J. Clin. Microbiol. 2021, 59, e02881-20. [Google Scholar] [CrossRef]
- Brümmer, L.E.; Katzenschlager, S.; Gaeddert, M.; Erdmann, C.; Schmitz, S.; Bota, M.; Grilli, M.; Larmann, J.; Weigand, M.A.; Pollock, N.R.; et al. Accuracy of novel antigen rapid diagnostics for SARS-CoV-2: A living systematic review and meta-analysis. PLoS Med. 2021, 18, e1003735. [Google Scholar] [CrossRef]
- Dinnes, J.; Sharma, P.; Berhane, S.; van Wyk, S.S.; Nyaaba, N.; Domen, J.; Taylor, M.; Cunningham, J.; Davenport, C.; Dittrich, S.; et al. Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2022, 7, CD013705. [Google Scholar] [CrossRef]
- Winkel, B.; Schram, E.; Gremmels, H.; Debast, S.; Schuurman, R.; Wensing, A.; Bonten, M.; Goedhart, E.; Hofstra, M. Screening for SARS-CoV-2 infection in asymptomatic individuals using the Panbio COVID-19 antigen rapid test (Abbott) compared with RT-PCR: A prospective cohort study. BMJ Open 2021, 11, e048206. [Google Scholar] [CrossRef] [PubMed]
- Love, N.K.; Ready, D.R.; Turner, C.; Yardley, L.; Rubin, G.J.; Hopkins, S.; Oliver, I. The acceptability of testing contacts of confirmed COVID-19 cases using serial, self-administered lateral flow devices as an alternative to self-isolation. J. Med. Microbiol. 2022, 71, 001567. [Google Scholar] [CrossRef]
- Chung, E.; Chow, E.J.; Wilcox, N.C.; Burstein, R.; Brandstetter, E.; Han, P.D.; Fay, K.; Pfau, B.; Adler, A.; Lacombe, K.; et al. Comparison of Symptoms and RNA Levels in Children and Adults with SARS-CoV-2 Infection in the Community Setting. JAMA Pediatr. 2021, 175, e212025. [Google Scholar] [CrossRef]
- Madera, S.; Crawford, E.; Langelier, C.; Tran, N.K.; Thornborrow, E.; Miller, S.; DeRisi, J.L. Nasopharyngeal SARS-CoV-2 viral loads in young children do not differ significantly from those in older children and adults. Sci. Rep. 2021, 11, 3044. [Google Scholar] [CrossRef] [PubMed]
- Xun, G.; Lane, S.T.; Petrov, V.A.; Pepa, B.E.; Zhao, H. A rapid, accurate, scalable, and portable testing system for COVID-19 diagnosis. Nat. Commun. 2021, 12, 2905. [Google Scholar] [CrossRef] [PubMed]
- Porte, L.; Legarraga, P.; Vollrath, V.; Aguilera, X.; Munita, J.M.; Araos, R.; Pizarro, G.; Vial, P.; Iruretagoyena, M.; Dittrich, S.; et al. Evaluation of a novel antigen-based rapid detection test for the diagnosis of SARS-CoV-2 in respiratory samples. Int. J. Infect. Dis. 2020, 99, 328–333. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Location | Total Subjects (% Female/Median Age) | Type of Research | Rat Kit | Sensitivity % | Specificity % | Negative Predictive Value % | Positive Predictive Value % | Accuracy % |
|---|---|---|---|---|---|---|---|---|---|
| Ahmed et al., 2022 [33] | Kelantan, Malaysia | 157 (42, 67/NM) | Cross-sectional study | Κit ProDetect, Medical Innovation Ventures Sdn Bhd, Malaysia | 96.00 | 98.00 | 96.00 | 98.00 | 97.00 |
| Savage et al., 2022 [34] | Liverpool, U.K. | 250 (58.3/40) | Prospective diagnostic accuracy evaluation | Covios COVID-19 Antigen Rapid Diagnostic test | 90.5 | 99.4 | 96.1 | 98.5 | 96.9 |
| Drain et al., 2022 [35] | King County, Washington, U.S.A. | 802 (58.2/37.3) | Clinical diagnostic accuracy study | Ag Detect Rapid Self-Test (InBios International Inc) and BinaxNOWCOVID-19 Ag Card (Abbott Laboratories) | 84.4 | 99.8 | 95.6 | 99.3 | 96.4 |
| Osmanodja et al., 2021 [36] | Berlin, Germany | 379 (NM/NM) | Prospective diagnostic accuracy study | Nasal swab for the Ag-RDT Dräger Antigen Test SARS-CoV-2 by Dräger Safety AG and Co. KGaA, Lübeck, Germany | 88.6 | 99.7 | 99.3 | 98.5 | 99.4 |
| Papenburg et al., 2022 [37] | Montreal, Canada | 278 (43.9/43) | Cross-sectional study | Panbio COVID-19 Ag Rapid Test Device (Abbott Laboratories) | 100 | 100 | 100 | 33.3 | 99.8 |
| Nikolai et al., 2021 [11] | Berlin, Germany | 228 (46.7/34.6) | Prospective diagnostic accuracy study | STANDARD Q COVID-19 Ag Test (SD Biosensor, Korea) | 91.2 | 98.4 | 96.9 | 96.8 | 96.8 |
| Patriquin et al., 2022 [12] | Nova Scotia, Canada | 197 (NM/NM) | Comparative Study | Abbott Panbio COVID-19 Ag rapid test device (Abbott Rapid Diagnostics GmbH, Orlaweg, Germany) | 98.7 | NM | NM | 88.8 | NM |
| Lindner et al., 2021 [13] | Berlin, Germany | 146 (51.4/35) | Prospective diagnostic accuracy study | STANDARD Q COVID-19 Ag Test (SD Biosensor, Inc. Gyeonggi-do, Korea) | 82.5 | 100 | 99.1 | 91.4 | 95.1 |
| Schuit et al., 2022 [14] | The Netherlands | 6497 (NM/NM) | Prospective cross sectional diagnostic test accuracy | Flowflex (Acon Laboratories), MPBio (MP Biomedicals) and Clinitest (Siemens-Healthineers) | 79 | 97.2 | 70.4 | 98.2 | 85.1 |
| Sukumaran et al., 2022 [15] | Kerala, India | 150 (NM/NM) | Validation study | AG-Q COVID-19 N-Ag rapid test kit by Agappe Diagnostics Limited. | 77.91 | 100 | 77.11 | 100 | 87.33 |
| Møller et al., 2022 [16] | Aarhus, Denmark | 827 (50.5/NM) | Prospective diagnostic accuracy study | COVID-19 Antigen Detection Kit-DNA Diagnostic A/S, Risskov, Denmark and the SARS-CoV-2 Antigen Rapid Test-Hangzhou Immuno Biotech Co Ltd, Hangzhou, China) | 65.7 and 62.1 | 100 and 100 | 97 and 93 | 100 and 100 | 97.1 and 93.7 |
| Cassuto et al., 2021 [17] | Paris, France | 239 (NM/NM) | Validation study | COVID-VIRO® Antigen test | 96.8 | 100 | 99.5 | 100 | 99.5 |
| Krüger et al., 2021 [18] | Heidelberg and Berlin, Germany. | 761 (52/35) | Diagnostic accuracy study | LumiraDx™ | 82.2 | 99.3 | 99.8 | 45.8 | 99.6 |
| Boerger et al., 2021 [19] | Rochester, Minnesota, U.S.A. | 300 (NM/NM) | Prospective diagnostic accuracy study | Flocked MT swab (Copan Diagnostics, Murrieta, CA) | 93.9 | 99.2 | 99.1 | 93.9 | 98.6 |
| Leventopoulos et al., 2022 [38] | Athens, Greece | 833 (46.7/32.94) | Prospective diagnostic accuracy study | Boson Rapid Antigen Test Card | 98.18 | 100 | 98.2 | 100 | 99.28 |
| Tonen-Wolyec et al., 2021 [20] | Paris, France | 106 (62.4/40) | Prospective diagnostic accuracy study | Biosynex Antigen Self-Test COVID-19 AG+ | 90.9 | 100 | 97.6 | 100 | 98.1 |
| Klein et al., 2021 [39] | Heidelberg, Germany | 290 (52.4/42.7) | Prospective diagnostic accuracy study | Panbio™ Ag-RDT (distributed by Abbott) | 84.4 | 99.2 | 99.8 | 88.1 | 96.5 |
| Kalil et al., 2021 [21] | Kelantan, Malaysia | 120 (54.2/NM) | Prospective diagnostic accuracy study | ProdetectTM COVID-19 Antigen rapid self-test | 96.4 | 100 | 66.6 | 100 | 96.6 |
| Stohr et al., 2021 [22] | Breda, the Netherlands | 3201 (56.5/41) | Cross-sectional study | BD-RDT or Roche-RDT | 55.6 | 99.8 | 94.4 | 97.1 | 94.6 |
| Wölfl-Duchek et al., 2022 [23] | Vienna, Austria | 132 (41.3/62.2) | Prospective diagnostic accuracy study | Medomics SARS-CoV-2 antigen test device (Jiangsu Medomics Medical Technology Co., China) | 63.04 | 100 | 70.69 | 100 | 80.46 |
| Garcia-Fiñana et al., 2021 [24] | Liverpool, U.K. | 5869 (NM/NM) | Observational cohort study | Innova LFT | 40 | 99.9 | 99.2 | 90.3 | 99.1 |
| Goldenfeld et al., 2022 [25] | Ramat Gan, Israel | 398 (NM/NM) | Prospective diagnostic accuracy study | Nowcheck RAT (Bionote, South Korea), SD RAT, Roche, SSS Australia) and Panbio RAT, Abbott Diagnostic, Jena | 76.9 | 97.57 | 98.7 | 100 | 98.8 |
| Parameter | Estimate | 2.5% CI | 97.5% CI |
|---|---|---|---|
| Sensitivity | 0.911 | 0.843 | 0.951 |
| Specificity | 0.995 | 0.990 | 0.998 |
| False positive rate | 0.005 | 0.002 | 0.010 |
| Logit (sensitivity) | 2.328 | 1.680 | 2.976 |
| Logit (specificity) | 5.359 | 4.583 | 6.136 |
| Parameter | Estimate | 2.5% CI | 97.5% CI |
|---|---|---|---|
| Sensitivity | 0.988 | 0.962 | 0.996 |
| Specificity | 0.974 | 0.941 | 0.989 |
| False positive rate | 0.026 | 0.011 | 0.059 |
| Logit(sensitivity) | 4.436 | 3.241 | 5.631 |
| Logit(specificity) | 3.634 | 2.774 | 4.494 |
| Risk of Bias | Risk of Bias | Risk of Bias | Risk of Bias | Applicability Concerns | Applicability Concerns | Applicability Concerns | |
|---|---|---|---|---|---|---|---|
| Studies | Patient Selection | Index Test(S) | Reference Standard | Flow And Timing | Patient Selection | Index Test(S) | Reference Standard |
| Ahmed et al., 2022 [33] | L | L | L | L | L | L | L |
| Savage et al., 2022 [34] | L | L | L | L | L | L | L |
| Drain et al., 2022 [35] | L | L | L | L | L | L | L |
| Osmanodja et al., 2021 [36] | L | L | L | L | L | L | L |
| Papenburg et al., 2022 [37] | L | L | L | U | L | L | L |
| Nikolai et al., 2021 [11] | L | L | L | L | L | L | L |
| Patriquin et al., 2022 [12] | L | L | L | U | L | L | L |
| Lindner et al., 2021 [13] | L | L | L | L | L | L | L |
| Schuit et al., 2022 [14] | L | L | L | H | L | L | L |
| Sukumaran et al., 2022 [15] | L | L | L | L | L | L | L |
| Møller et al., 2022 [16] | L | L | L | L | L | L | L |
| Cassuto et al., 2021 [17] | L | L | L | L | L | L | L |
| Krüger et al., 2021 [18] | L | L | L | L | L | L | L |
| Boerger et al., 2021 [19] | L | L | L | L | L | L | L |
| Leventopoulos et al., 2022 [38] | L | L | L | L | L | L | L |
| Tonen-Wolyec et al., 2021 [20] | L | L | L | L | L | L | L |
| Klein et al., 2021 [39] | L | L | L | L | L | L | L |
| Kalil et al., 2021 [21] | L | L | L | L | L | L | L |
| Stohr et al., 2021 [22] | L | L | L | L | L | L | L |
| Wölfl-Duchek et al., 2022 [23] | L | L | L | U | L | L | L |
| García-Fiñana et al., 2021 [24] | L | L | L | L | L | L | L |
| Goldenfeld et al., 2022 [25] | L | L | L | U | L | L | L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karlafti, E.; Tsavdaris, D.; Kotzakioulafi, E.; Kaiafa, G.; Savopoulos, C.; Netta, S.; Michalopoulos, A.; Paramythiotis, D. The Diagnostic Accuracy of SARS-CoV-2 Nasal Rapid Antigen Self-Test: A Systematic Review and Meta-Analysis. Life 2023, 13, 281. https://doi.org/10.3390/life13020281
Karlafti E, Tsavdaris D, Kotzakioulafi E, Kaiafa G, Savopoulos C, Netta S, Michalopoulos A, Paramythiotis D. The Diagnostic Accuracy of SARS-CoV-2 Nasal Rapid Antigen Self-Test: A Systematic Review and Meta-Analysis. Life. 2023; 13(2):281. https://doi.org/10.3390/life13020281
Chicago/Turabian StyleKarlafti, Eleni, Dimitrios Tsavdaris, Evangelia Kotzakioulafi, Georgia Kaiafa, Christos Savopoulos, Smaro Netta, Antonios Michalopoulos, and Daniel Paramythiotis. 2023. "The Diagnostic Accuracy of SARS-CoV-2 Nasal Rapid Antigen Self-Test: A Systematic Review and Meta-Analysis" Life 13, no. 2: 281. https://doi.org/10.3390/life13020281