
Persistence of Symptoms 15 Months since COVID-19 Diagnosis: Prevalence, Risk Factors and Residual Work Ability
 and
and
Abstract
:1. Background
2. Methods
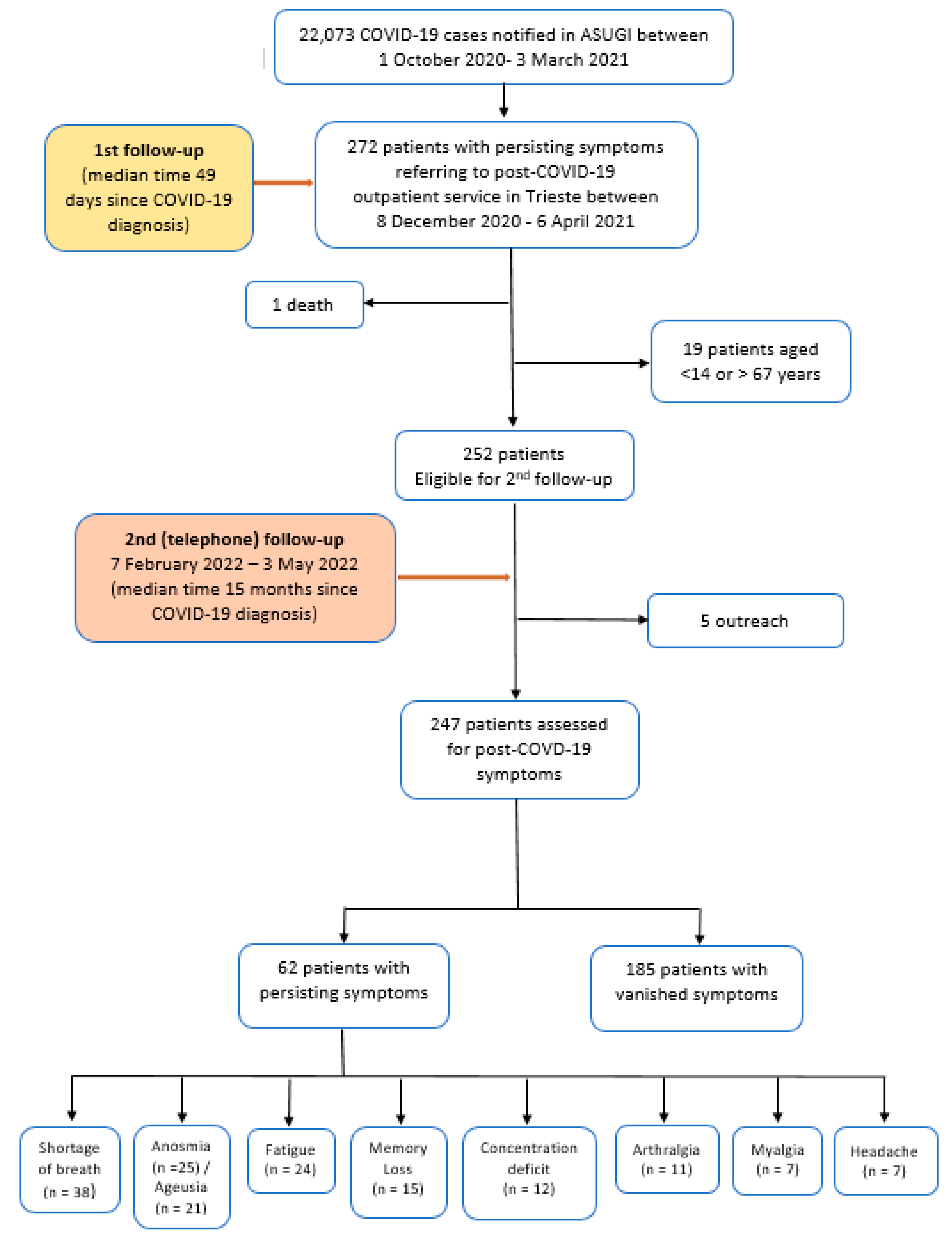
- were of working age (i.e., 14–67 years, by Italian law);
- had symptoms persisting for at least three weeks since positive swab test for SARS-CoV-2;
- attended the Long-COVID-19 outpatient clinic of Trieste;
- provided an informed consent to participate to the study.
- Patients were excluded in case of:
- Age < 14 or >67 years
- death during study period;
- inability to sustain a telephone follow-up interview (due to medical reasons as dementia, speech disorders, language barriers, psychiatric disorders, among other);
- refusal to participate to the study;
- loss to follow up.
- 6: No hindrance;
- 5: I am able to do my job, but it causes me some symptoms;
- 4: I must sometimes slow down my work pace or change my work methods;
- 3: I must often slow down my work pace or change my work methods;
- 2: I feel I am able to do only part time work;
- 1: In my opinion I am entirely unable to work.
2.1. Outcome Measure
2.2. Ethical Considerations
2.3. Statistical Analysis
3. Results
Post COVID-19 Symptoms
4. Discussion
4.1. Key Findings
4.2. Generalizability
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maury, A.; Lyoubi, A.; Peiffer-Smadja, N.; de Broucker, T.; Meppiel, E. Neurological Manifestations Associated with SARS-CoV-2 and Other Coronaviruses: A Narrative Review for Clinicians. Rev. Neurol. 2021, 177, 51–64. [Google Scholar] [CrossRef]
- Sivan, M.; Taylor, S. NICE guide line on long COVID. BMJ 2020, 371, m4938. [Google Scholar] [CrossRef] [PubMed]
- Rostami, Z.; Mastrangelo, G. A Prospective Study on Risk Factors for Acute Kidney Injury and All-Cause Mortality in Hospitalized COVID-19 Patients from Tehran. Iran Front. Immunol. 2022, 13, 874426. [Google Scholar] [PubMed]
- Subramanian, A.; Niranthararkhumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [PubMed]
- European Centre for Disease Prevention and Control. Clinical Characteristics of COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/clinical (accessed on 4 October 2022).
- Carfì, A.; Bernabei, R.; Landi, F. Group for the GAC-19 P-ACS. Persistent symptoms in patients after acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; Di Cristianziano, V.; Osebold, L.; et al. Post-COVID syndrome in non-hospitalised patients with COVID-19: A longitudinal prospective cohort study. Lancet Reg. Health Eur. 2021, 6, 100122. [Google Scholar] [CrossRef]
- Tleyjeh, I.M.; Saddik, B.; Ramakrishan, R.; AlSwaidan, N.; AlAnazi, A.; Alhazmi, D.; Aloufi, A.; AlSumait, F.; Berbari, E.F.; Halwani, R. Long term predictors of breathlessness, exercise intolerance, chronic fatigue and well-being in hospitalized patients with COVID-19: A cohort study with 4 months median follow-up. J. Infect. Public Health 2022, 15, 21–28. [Google Scholar] [CrossRef]
- Santoyo-Mora, M.; Villaseñor-Mora, C.; Cardona-Torres, L.M.; Martínez-Nolasco, J.J.; Barranco-Gutiérrez, A.I.; Padilla-Medina, J.A.; Bravo-Sánchez, M.G. COVID-19 Long-Term Effects: Is There an Impact on the Simple Reaction Time and Alternative-Forced Choice on Recovered Patients? Brain Sci. 2022, 12, 1258. [Google Scholar] [CrossRef]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The immunology and immunopathology of COVID19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef]
- World Health Organization. A Clinical Case Definition of Post COVID-19 Condition by a Delphi Consensus. 2021. Available online: https://apps.who.int/iris/handle/10665/345824 (accessed on 3 October 2022).
- World Health Organization. Coronavirus Disease (COVID-19): Post COVID-19 Condition. 2021. Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-(covid-19)-post-covid-19-condition (accessed on 9 October 2022).
- NICE. Covid-19 Rapid Guideline: Managing the Long-Term Effects of COVID-19. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 9 October 2022).
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 Long-Term Effects of COVID-19: A Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global Prevalence of Post COVID-19 Condition or Long COVID: A Meta-Analysis and Systematic Review. J. Infect. Dis. 2022, 16, jiac136. [Google Scholar]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Venturelli, S.; Benatti, S.V.; Casati, M.; Binda, F.; Zuglian, G.; Imeri, G.; Conti, C.; Biffi, A.M.; Spada, M.S.; Bondi, E.; et al. Surviving COVID-19 in Bergamo province: A post-acute outpatient re-evaluation. Epidemiol. Infect. 2021, 149, e32. [Google Scholar] [CrossRef]
- Whitaker, M.; Elliott, J.; Chadeau-Hyam, M.; Riley, S.; Darzi, A.; Cooke, G.; Ward, H.; Elliott, P. Persistent COVID-19 symptoms in a community study of 606,434 people in England. Nat. Commun. 2022, 13, 1957. [Google Scholar] [CrossRef]
- Naik, S.; Haldar, S.N.; Soneja, M.; Mundadan, N.G.; Garg, P.; Mittal, A.; Desai, D.; Trilangi, P.K.; Chakraborty, S.; Begam, N.N.; et al. Post COVID-19 sequelae: A prospective observational study from Northern India. Drug Discov. Ther. 2021, 15, 254–260. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Blomberg, B.; Mohn, K.G.; Brokstad, K.A.; Zhou, F.; Linchausen, D.W.; Hansen, B.A.; Lartey, S.; Onyango, T.B.; Kuwelker, K.; Sævik, M.; et al. Long COVID in a prospective cohort of home-isolated patients. Nat. Med. 2021, 27, 1607–1613. [Google Scholar] [CrossRef]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: Results from a prospective UK cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef]
- Evans, R.A.; McAuley, H.; Harrison, E.M.; Shikotra, A.; Singapuri, A.; Sereno, M.; Elneima, O.; Docherty, A.B.; I Lone, N.; Leavy, O.C.; et al. Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): A UK multicentre, prospective cohort study. Lancet Respir. Med. 2021, 9, 1275–1287. [Google Scholar] [CrossRef]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Di Gessa, G.; et al. Long COVID burden and risk factors in 10 UK longitudinal studies and electronic health records. Nat. Commun. 2022, 13, 3528. [Google Scholar] [CrossRef] [PubMed]
- Savarraj, J.P.J.; Burkett, A.B.; Hinds, S.N.; Paz, A.S.; Assing, A.; Juneja, S.; Colpo, G.D.; Torres, L.F.; Cho, S.-M.; Gusdon, A.M.; et al. Pain and Other Neurological Symptoms Are Present at 3 Months After Hospitalization in COVID-19. Patients. Front. Pain Res. 2021, 2, 737961. [Google Scholar] [CrossRef] [PubMed]
- Cabrera Martimbianco, A.L.; Pacheco, R.L.; Bagattini, Â.M.; Riera, R. Frequency, signs and symptoms, and criteria adopted for long COVID-19: A systematic review. Int. J. Clin. Pract. 2021, 7, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Tleyjeh, I.M.; Saddik, B.; Alswaidan, N.; AlAnazi, A.; Ramakrishnan, R.K.; Alhazmi, D.; Aloufi, A.; AlSumait, F.; Berbari, E.; Halwani, R. Prevalence and predictors of Post-Acute COVID-19 Syndrome (PACS) after hospital discharge: A cohort study with 4 months median follow-up. PLoS ONE 2021, 16, e0260568. [Google Scholar] [CrossRef]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Huang, L.; Li, X.; Gu, X.; Zhang, H.; Ren, L.; Guo, L.; Liu, M.; Wang, Y.; Cui, D.; Wang, Y.; et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: A longitudinal cohort study. Lancet Respir. Med. 2022, 10, 863–876. [Google Scholar] [CrossRef]
- Sykes, D.L.; Holdswoth, L.; Jawad, N. Post-COVID-19 Symptom Burden: What is Long-COVID and How Should We Manage It? Lung 2021, 199, 113–119. [Google Scholar] [CrossRef]
- Buonsenso, D.; Munblit, D.; De Rose, C.; Sinatti, D.; Ricchiuto, A.; Carfi, A.; Valentini, P. Preliminary evidence on long COVID in children. Acta Paediatr. 2021, 110, 2208–2211. [Google Scholar] [CrossRef]
- Damanti, S.; Cilla, M.; Cilona, M.; Fici, A.; Merolla, A.; Pacioni, G.; De Lorenzo, R.; Martinenghi, S.; Vitali, G.; Magnaghi, C.; et al. Prevalence of Long COVID-19 Symptoms After Hospital Discharge in Frail and Robust Patients. Front. Med. 2022, 9, 834887. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. eClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Blitshteyn, S.; Whiteson, J.H.; Abramoff, B.; Azola, A.; Bartels, M.N.; Bhavaraju-Sanka, R.; Chung, T.; Fleming, T.K.; Henning, E.; Miglis, M.G.; et al. Multi-disciplinary collaborative consensus guidance statement on the assessment and treatment of autonomic dysfunction in patients with post-acute sequelae of SARS-CoV-2 infection (PASC). PMR 2022, 14, 1270–1291. [Google Scholar] [CrossRef] [PubMed]
- Chudzik, M.; Babicki, M.; Kapusta, G.; Kałuzińska-Kołat, Z.; Kołat, D.; Jankowski, P.; Mastalerz-Migas, A. Long-COVID Clinical Features and Risk Factors: A Retrospective Analysis of Patients from the STOP-COVID Registry of the PoLoCOV Study. Viruses 2022, 14, 1755. [Google Scholar] [CrossRef] [PubMed]
- Van Kessel, S.A.M.; Hartman, T.C.O.; Lucassen, P.L.B.J.; van Jaarsveld, C.H.M. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2022, 39, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Afshar, Y.; Gaw, S.L.; Flaherman, V.J.; Chambers, B.D.; Krakow, D.; Berghella, V.; Shamshirsaz, A.A.; Boatin, A.A.; Aldrovandi, G.; Greiner, A.; et al. Clinical presentation of coronavirus disease 2019 (COVID-19) in pregnant and recently pregnant people. Obstet. Gynecol. 2020, 136, 1117–1125. [Google Scholar] [CrossRef]
- Willyard, C. Could tiny blood clots cause long COVID’s puzzling symptoms? Nature 2022, 608, 662–664. [Google Scholar] [CrossRef]
- Sankar, K.; Gould, M.K.; Prescott, H.C. Psychological Morbidity After COVID-19 Critical Illness. Chest 2022. [Google Scholar] [CrossRef]
- Lai, C.-C.; Hsu, C.K.; Yen, M.Y.; Lee, P.I.; Ko, W.C.; Hsueh, P.R. Long COVID: An inevitable sequela of SARS-CoV-2 infection. J. Microbiol. Immunol. Infect. 2022. [Google Scholar] [CrossRef]
- Maes, M.; Al_Rubaye, H.T.; Almulla, A.F.; Al-Hadrawi, D.S.; Stoyanova, K.; Kubera, M.; Al-Hakeim, H.K. Lowered Quality of Life in Long COVID Is Predicted by Affective Symptoms, Chronic Fatigue Syndrome, Inflammation and Neuroimmunotoxic Pathways. Int. J. Environ. Res. Public Health 2022, 19, 10362. [Google Scholar] [CrossRef]
- Hugon, J. Long-COVID: Cognitive deficits (brain fog) and brain lesions in non-hospitalized patients. Presse Med. 2021, 51, 104090. [Google Scholar] [CrossRef]
- Ramani, A.; Muller, S.; Ostermann, O.N.; Gabriel, E.; Abida-Islam, P.; Müller-Schiffmann, A.; Mariappan, A.; Goureau, O.; Gruell, H.; Walker, A.; et al. SARS-CoV-2 targets neurons of 3D human brain organoids SARS-CoV-2 targets neurons of 3D human brain organoids. EMBO J. 2020, 39, e106230. [Google Scholar] [CrossRef]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent neurologic symptoms and cognitive dysfunction in non-hospitalized Covid-19 “long haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef] [PubMed]
- Young, P.; Finn, B.C.; Bruetman, J.; Pellegrini, D.; Kremer, A. The chronic asthenia syndrome: A clinical approach. Medicina 2010, 70, 284–292. [Google Scholar] [PubMed]
- Pretorius, E.; Vlok, M.; Venter, C.; Bezuidenhout, J.A.; Laubscher, G.J.; Steenkamp, J.; Kell, D.B. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc. Diabetol. 2021, 20, 172. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, E.; Venter, C.; Laubscher, C.J.; Kotze, M.J.; Oladejo, S.O.; Watson, L.R.; Rajaratnam, K.; Watson, B.W.; Kell, D.B. Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Cardiovasc. Diabetol. 2022, 21, 148. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depression Fact Sheet. Updated 22 March 2018. Available online: http://www.who.int/mediacentre/factsheets/fs369/en/ (accessed on 7 October 2022).
- Kendler, K.S.; Gardner, C.O. Sex Differences in the Pathways to Major Depression: A Study of Opposite-Sex Twin Pairs. J. Psychiatry 2014, 171, 426–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurer, D.M.; Raymond, T.J.; Davis, B.N. Depression: Screening and Diagnosis. Am. Fam. Physician 2018, 98, 508–515. [Google Scholar]
- Kendler, K.S.; Gardner, C.O.; Prescott, C.A. Toward a comprehensive developmental model for major depression in men. Am. J. Psychiatry 2006, 163, 115–124. [Google Scholar] [CrossRef]
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Yuan, K.; Zheng, Y.B.; Wang, Y.J.; Sun, Y.-K.; Gong, Y.-M.; Huang, Y.-T.; Chen, X.; Liu, X.-X.; Zhong, Y.; Su, S.-Z.; et al. A systematic review and meta-analysis on prevalence of and risk factors associated with depression, anxiety and insomnia in infectious diseases, including COVID-19: A call to action. Mol. Psychiatry 2022, 27, 1–9. [Google Scholar]
- Cegolon, L.; Ronchese, F.; Ricci, F.; Negro, C.; Larese Filon, F. SARS-CoV-2 Infection in Health Care Workers of Trieste (North-Eastern Italy), 1 October 2020–7 February 2022: Occupational Risk and the Impact of the Omicron Variant. Viruses 2022, 14, 1663. [Google Scholar] [CrossRef]
- Cegolon, L.; Negro, C.; Mastrangelo, G.; Larese Filon, F. Primary SARS-CoV-2 Infections, Re-infections and Vaccine Effectiveness during the Omicron Transmission Period in Healthcare Workers of Trieste and Gorizia (Northeast Italy), 1 December 2021–31 May 2022. Viruses 2022, 14, 2688. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symptoms Duration N (%) | Total | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Group A (<200 Days) | Group B (200+ Days) | ||||||
| Total patients—N (row %) | 125 (50.6) | 122 (49.4) | 247 (100) | ||||
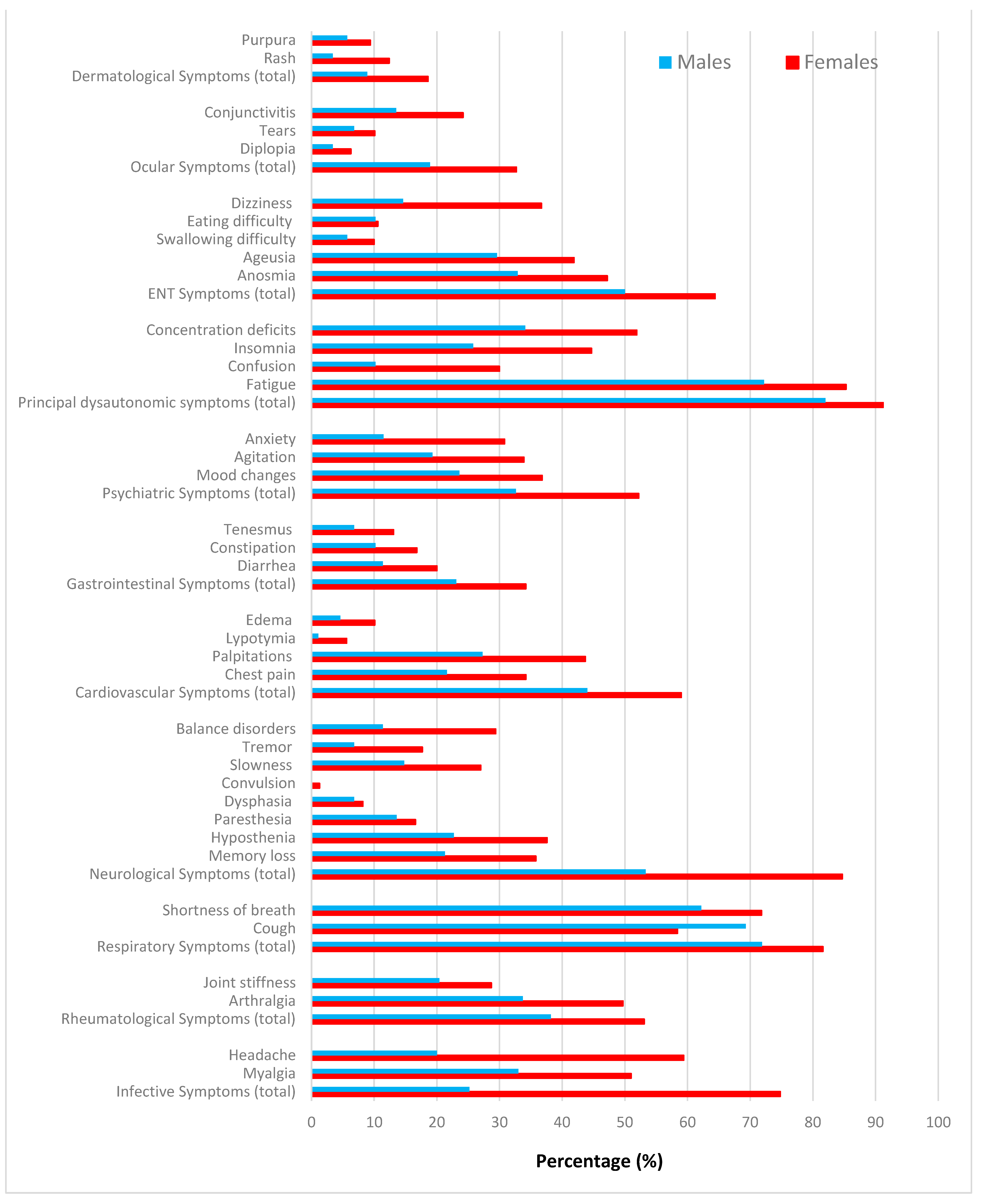
| Sex | Females | 81 (64.8) | 78 (63.9) | 159 (64.4) | 0.880 | ||
| Males | 44 (35.2) | 44 (36.1) | 88 (35.6) | ||||
| Age (years) | (Mean± SD) | 46.8 ± 10.7 | 49.5 ± 10.2 | 48.1 ± 10.5 | 0.020 * | ||
| Smoking | Non smokers | 59 (47.2) | 69 (56.6) | 128 (51.8) | 0.319 | ||
| Smokers | 37 (29.6) | 28 (22.9) | 65 (26.3) | ||||
| Ex-smokers | 29 (23.2) | 25 (20.5) | 54 (21.9) | ||||
| BMI (Kg/m2) | Mean± SD | 25.2 ± 5.1 | 27.2 ± 6.2 | 26.2 ± 5.7 | 0.004 * | ||
| <25 | 57 (45.6) | 50 (41) | 107 (43.3) | 0.100 | |||
| 25–30 | 28 (22.4) | 31 (25.4) | 59 (23.9) | ||||
| >30 | 15 (12.0) | 29 | 81 (32.8) | ||||
| Missing | 25 (20) | 12 (9.8) | 37 (15.0) | ||||
| Pre-existing Comorbidities | No | 77 (61.6) | 62 (50.8) | 139 (56.3) | 0.080 | ||
| Yes | 48 (38.4) | 60 (49.2) | 108 (43.7) | ||||
| Pre-existing Comorbidities | Hypertension | 15 (12) | 20 (16.4) | 35 (14.2) | 0.322 | ||
| Diabetes | 2 (1.6) | 6 (4.9) | 8 (3.2) | 0.141 | |||
| Cardiovascular Disease | 6 (4.8) | 7 (5.7) | 13 (5.3) | 0.741 | |||
| Thyroid Disease | 19 (15.2) | 21 (17.2) | 40 (16.2) | 0.668 | |||
| Asthma | 7 (5.6) | 9 (7.4) | 16 (6.5) | 0.571 | |||
| COPD | 6 (4.8) | 7 (5.7) | 13 (5.3) | 0.741 | |||
| Cancer | 3 (2.4) | 2 (1.6) | 5 (2.0) | 0.671 | |||
| Allergy | 18 (14.4) | 19 (15.6) | 37 (15.0) | 0.796 | |||
| Depression | No | 118 (94.4) | 102 (83.6) | 193 (78.1) | 0.007 | ||
| Yes | 7 (5.6) | 20 (16.4) | 27 (10.9) | ||||
| COVID-19 care | Primary | 70 (56) | 69 (56.56) | 139 (56.3) | 0.990 | ||
| Hospital | Total | 55 (44) | 53 (43.44) | 108 (43.7) | 0.990 | ||
| Non-Intensive Care | 53 (42.4) | 52 (42.64) | 105 (42.5) | 0.930 | |||
| Intensive Care | 2 (1.6) | 1 (0.8) | 3 (1.2) | 0.576 | |||
| Occupation | Blue Collar workers | 15 (12) | 14 (11.5) | 29 (11.7) | 0.514 | ||
| White Collar workers | 38 (30.4) | 32 (26.2) | 70 (28.3) | ||||
| Health Care workers | 29 (23.2) | 36 (29.5) | 65 (26.3) | ||||
| Trade and transport workers | 11 (8.8) | 14 (11.5) | 25 (10.1) | ||||
| Law enforcement’s | 5 (4) | 7 (5.7) | 12 (4.9) | ||||
| Education workers | 22 (17.6) | 12 (9.8) | 34 (13.8) | ||||
| Other (unemployed, housewives, retirees) | 5 (4) | 7 (5.7) | 12 (4.9) | ||||
| Re-infection | No | 101 (80.8) | 106 (86.9) | 207 (83.8) | 0.194 | ||
| Yes | 24 (19.2) | 16 (13.1) | 40 (16.2) | ||||
| Post-COVID-19 Vaccination | No | 16 (12.8) | 16 (13.1) | 32 (13.0) | 0.941 | ||
| Yes | 109 (87.2) | 106 (86.9) | 215 (87.0) | ||||
| Novel condition developed after COVID-19 | No | 103 (82.4) | 93 (77.5) | 196 (79.4) | 0.418 | ||
| Yes | 22 (17.6) | 27 (22.5) | 49 (19.8) | ||||
| Work Ability Index (WAI) | Mean± SD | 5.18 ± 1.08 | 4.5 ± 1.44 | 4.9 ± 1.3 | <0.001 * | ||
| No obstacles to work (6) | 66 (52.8) | 39 (32.2) | 105 (42.7) | 0.003 | |||
| Some symptoms (5) | 31 (24.8) | 33 (27.3) | 64 (26.0) | ||||
| Occasionally slowing down (4) | 17 (13.6) | 18 (14.9) | 35 (14.2) | ||||
| Frequently slowing down (3) | 8 (6.4) | 22 (18.2) | 30 (12.2) | ||||
| Only part time work (2) | 2 (1.6) | 2 (1.6) | 4 (1.2) | ||||
| Unable to work at all (1) | 1 (0.8) | 7 (5.8) | 8 (3.2) | ||||
| Symptoms | Duration N (Col %) | p-Value * | Post-COVID-19 FU N (Col %) | p-Value ** | ||
|---|---|---|---|---|---|---|
| (<200 Days) | (200+ Days) | 1st | 2nd | |||
| Total Patients | 125 (50.6) | 122 (49.4) | 247 (100) | 247 (100) | ||
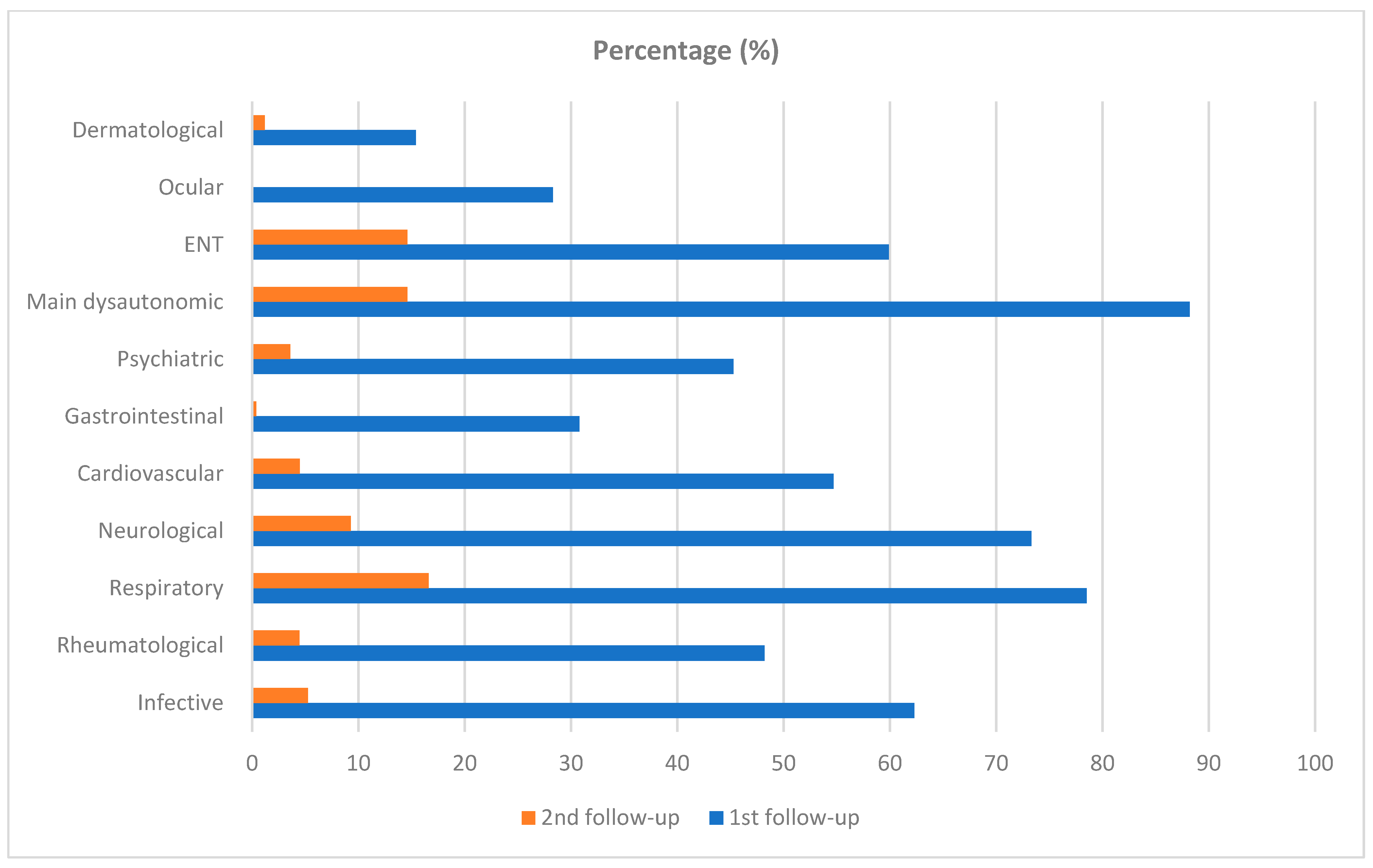
| With persisting symptoms | 125 (100) | 122 (100) | 247 (100) | 62 (25.1) | <0.001 | |
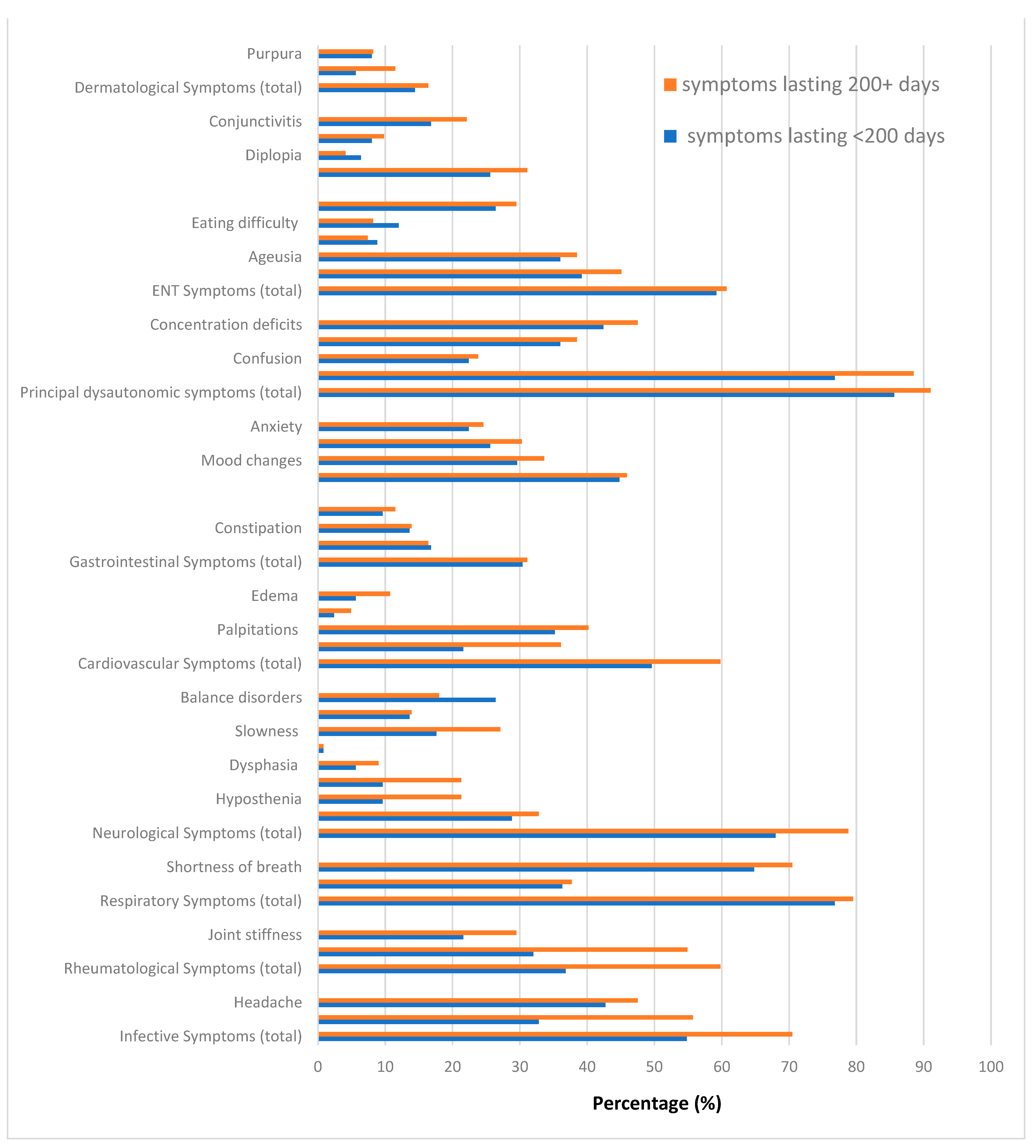
| Infective Symptoms (total) | 68 (55.2) | 86 (70.5) | 0.014 | 155 (62.3) | 13 (5.3) | <0.001 |
| Myalgia § | 41 (32.8) | 68 (55.7) | <0.001 | 109 (44.1) | 7 (2.8) | <0.001 |
| Headache § | 53 (42.7) | 58 (47.5) | 0.404 | 111 (44.9) | 7 (2.8) | <0.001 |
| Rheumatological Symptoms (total) | 46 (36.8) | 73 (59.8) | <0.001 | 119 (48.2) | 11 (4.5) | <0.001 |
| Arthralgia | 40 (32.0) | 67 (54.9) | <0.001 | 107 (43.3) | 11 (4.5) | <0.001 |
| Joint stiffness | 27 (21.6) | 36 (29.5) | 0.127 | 63 (25.5) | 3 (1.2) | <0.001 |
| Respiratory Symptoms (total) | 96 (60.8) | 97 (79.5) | 0.784 | 194 (78.5) | 41 (16.6) | 0.210 |
| Cough | 45 (36.3) | 49 (40.2) | 0.636 | 91 (36.8) | 4 (1.6) | <0.001 |
| Shortness of breath § | 81 (64.8) | 92(75.4) | 0.226 | 172 (69.6) | 38 (15.3) | <0.001 |
| Neurological Symptoms (total) | 85 (68.0) | 96 (78.7) | 0.092 | 181 (73.3) | 23 (9.3) | <0.001 |
| Memory loss § | 36 (28.8) | 40 (32.8) | 0.525 | 76 (30.8) | 15 (6.1) | <0.001 |
| Hyposthenia § | 33 (26.4) | 46 (37.7) | 0.056 | 79 (32.0) | 7 (2.8) | <0.001 |
| Paresthesia § | 12 (9.6) | 26 (21.3) | 0.011 | 38 (15.4) | 3 (1.2) | <0.001 |
| Dysphasia | 7 (5.6) | 11 (9.0) | 0.225 | 18 (7.3) | 3 (1.2) | <0.001 |
| Convulsion | 1 (0.8) | 1 (0.8) | 0.991 | 2 (1.0) | 1 (0.4) | <0.001 |
| Slowness | 22 (17.6) | 33 (27.1) | 0.063 | 55 (22.3) | 1 (0.4) | <0.001 |
| Tremor | 17 (13.6) | 17 (13.9) | 0.919 | 34 (13.8) | 2 (0.8) | <0.001 |
| Balance disorders | 33 (26.4) | 22 (18.0) | 0.114 | 55 (22.3) | 0 | <0.001 |
| Cardiovascular Symptoms (total) | 62 (49.6) | 73 (59.8) | 0.210 | 135 (54.7) | 11 (4.5) | <0.001 |
| Chest pain § | 28 (22.4) | 46(37.7) | 0.011 | 72 (29.1) | 2 (0.8) | <0.001 |
| Palpitations § | 44 (35.2) | 50 (41.0) | 0.376 | 93 (37.7) | 9 (3.6) | <0.001 |
| Lipothymia § | 3 (2.4) | 7 (5.7) | 0.188 | 9 (3.6) | 0 | <0.001 |
| Edema | 7 (5.6) | 13 (10.7) | 0.145 | 20 (8.1) | 0 | <0.001 |
| Gastrointestinal Symptoms | 38 (30.4) | 38 (31.1) | 0.934 | 76 (30.8) | 1 (0.4) | <0.001 |
| Diarrhea § | 21 (16.8) | 21 (16.4) | 0.954 | 41 (16.6) | 1 (0.4) | <0.001 |
| Constipation § | 17 (13.6) | 17 (13.9) | 0.939 | 34 (13.8) | 0 | <0.001 |
| Tenesmus | 12 (9.6) | 14 (11.5) | 0.631 | 26 (10.5) | 0 | <0.001 |
| Psychiatric Symptoms (total) | 56 (44.8) | 56 (45.9) | 0.908 | 112 (45.3) | 9 (3.6) | 0.385 |
| Mood changes | 37 (29.6) | 43 (35.2) | 0.391 | 78 (31.6) | 9 (3.6) | <0.001 |
| Agitation | 32 (25.6) | 40 (32.9) | 0.264 | 69 (27.9) | 0 | <0.001 |
| Anxiety | 28 (22.4) | 31 (25.4) | 0.654 | 58 (23.5) | 2 (0.8) | <0.001 |
| Main dysautonomic symptoms | 107 (85.6) | 111 (91.0) | 0.262 | 218 (88.2) | 36 (14.6) | <0.001 |
| Fatigue § | 96 (76.8) | 108 (88.5) | 0.127 | 198 (80.2) | 24 (9.7) | 0.003 |
| Confusion | 28 (22.4) | 29 (23.8) | 0.826 | 57 (23.1) | 4 (1.6) | <0.001 |
| Insomnia § | 45 (36.0) | 47 (38.5) | 0.515 | 92 (37.2) | 5 (2.0) | <0.001 |
| Concentration deficits | 53 (42.4) | 58 (47.5) | 0.404 | 111 (44.9) | 12 (4.8) | <0.001 |
| Fatigue & Concentration deficit § | 45 (36.0) | 55 (45.1) | 0.176 | 101 (40.9) | 4 (2.0) | <0.001 |
| ENT Symptoms (total) | 74 (59.2) | 74 (60.7) | 0.877 | 148 (59.9) | 36 (14.6) | <0.001 |
| Anosmia | 49 (39.2) | 55 (45.1) | 0.349 | 104 (42.1) | 25 (10.1) | <0.001 |
| Ageusia | 45 (36.0) | 47 (38.5) | 0.682 | 92 (37.2) | 21 (8.5) | <0.001 |
| Swallowing difficulty § | 11 (8.8) | 9 (7.4) | 0.682 | 20 (8.1) | 3 (1.2) | <0.001 |
| Eating difficulty § | 15 (12.0) | 10 (8.2) | 0.322 | 25 (10.1) | 0 | <0.001 |
| Dizziness § | 33 (26.4) | 36 (29.5) | 0.586 | 69 (27.9) | 7 (2.8) | <0.001 |
| Ocular Symptoms (total) | 32 (25.6) | 38 (31.1) | 0.423 | 70 (28.3) | 0 | <0.001 |
| Diplopia | 8 (6.4) | 5 (4.1) | 0.418 | 13 (5.3) | 0 | <0.001 |
| Tears | 10 (8.0) | 12 (9.8) | 0.613 | 22 (8.9) | 0 | <0.001 |
| Conjunctivitis | 21 (16.8) | 27 (22.1) | 0.158 | 48 (19.4) | 0 | <0.001 |
| Dermatological Symptoms (total) | 18 (14.4) | 20 (16.4) | 0.745 | 38 (15.4) | 3 (4.8) | <0.001 |
| Rash § | 7 (5.6) | 14 (1.1) | 0.098 | 21 (8.5) | 3 (4.8) | <0.001 |
| Purpura | 10 (8.0) | 10 (8.2) | 0.955 | 20 (8.1) | 0 | <0.001 |
| Factors | Post-COVID-19 Symptoms | |||||
|---|---|---|---|---|---|---|
| Respiratory aOR (95% CI) | Neurological aOR (95% CI) | Psychiatric aOR (95% CI) | Dysautonomic aOR (95% CI) | WAI aRC (95% CI) | ||
| 1st follow up (median time: 49 days since COVID-19 diagnosis) | ||||||
| Female | Reference | Reference | Reference | Reference | NA | |
| Male | 0.52 (0.25; 1.07) | 0.16 (0.08; 0.35) | 0.43 (0.23; 0.80) | 0.41 (0.19; 1.28) | ||
| Age (years, linear term) | 0.98 (0.95; 1.02) | 1.04 (1.01; 1.08) | 1.00 (0.98; 1.03) | 0.98 (0.93; 1.02) | ||
| BMI (Kg/m2, linear term) | 1.04 (0.97; 1.12) | 1.01 (0.94; 1.08) | 0.98 (0.93; 1.03) | 1.02 (0.93; 1.12) | ||
| Smoking | No | Reference | Reference | Reference | Reference | |
| Yes | 0.85 (0.41; 1.75) | 1.2 (0.59; 2.48) | 1.85 (0.03; 3.34) | 0.46 (0.17; 1.21) | ||
| Co-Morbidities * | No | Reference | Reference | Reference | Reference | |
| Yes | 1.10 (0.52; 2.33) | 0.86 (0.41; 1.82) | 1.03 (0.55; 1.90) | 1.53 (0.56; 4.2) | ||
| Depression | No | Reference | Reference | Reference | Reference | |
| Yes | 0.78 (0.26; 2.34) | 1.47 (0.42–5.20) | 6.35 (2.01; 20.11) | Omitted | ||
| COVID-19 care | Primary | Reference | Reference | Reference | Reference | |
| Hospital | 0.88 (0.42; 1.83) | 0.69 (0.33; 1.43) | 0.81 (0.44; 1.49) | 0.33 (0.11; 0.90) | ||
| 2nd follow up (median time: 15 months since COVID-19 diagnosis) | ||||||
| Sex | Female | Reference | Reference | Reference | Reference | Reference |
| Male | 1.34 (0.61; 2.89) | 0.39 (0.11; 1.36) | omitted | 0.43 (0.16; 1.16) | 0.50 (0.11; 0.88) | |
| Age (years, linear term) | 1.01 (0.97; 1.04) | 1.02 (0.96; 1.08) | 0.94 (0.86; 1.02) | 0.99 (0.95; 1.03) | −0.001 (−0.18; 0.17) | |
| BMI (kg/m2, linear term) | 0.97 (0.90; 1.05) | 1.08 (0.997; 1.16) | 1.07 (0.96; 1.20) | 1.06 (0.99; 1.12) | −0.01 (−0.04; 0.23) | |
| Smoking | No | Reference | Reference | Reference | Reference | Reference |
| Yes | 0.72 (0.34; 1.53) | 0.59 (0.21; 1.43) | 0.98 (0.19; 5.18) | 0.91 (0.40; 2.07) | 0.10 (−0.35; 0.38) | |
| Co-Morbidities * | No | Reference | Reference | Reference | Reference | Reference |
| Yes | 1.10 (0.50; 2.39) | 4.31 (1.27; 14.7) | 3.14 (0.46; 21.2) | 1.93 (0.40; 2.07) | −0.27 (−0.66; 0.11) | |
| Depression | No | Reference | Reference | Reference | Reference | Reference |
| Yes | 0.19 (0.02; 1.47) | 0.43 (0.08; 2.35) | 1.04 (0.13; 8.13) | 1.13 (0.35; 3.77) | −0.06 (−0.63; 0.51) | |
| COVID-19 care | Primary | Reference | Reference | Reference | Reference | Reference |
| Hospital | 0.95 (0.45; 2.03) | 0.57 (0.20; 1.62) | 0.39 (0.07; 2.27) | 1.24 (0.54; 2.84) | 0.29 (−0.08; 0.67) | |
| Factors | aOR (95% CI) | p-Value | |
|---|---|---|---|
| Sex | Females | reference | 0.675 |
| Males | 0.97 (0.65; 1.44) | ||
| Age (years, linear) | 1.03 (1.01; 1.05) | 0.001 | |
| BMI (kg/m2, linear) | 1.03 (1.00; 1.06) | 0.068 | |
| Depression | No | reference | 0.001 |
| Yes | 2.68 (1.60; 4.49) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sansone, D.; Tassinari, A.; Valentinotti, R.; Kontogiannis, D.; Ronchese, F.; Centonze, S.; Maggiore, A.; Cegolon, L.; Filon, F.L. Persistence of Symptoms 15 Months since COVID-19 Diagnosis: Prevalence, Risk Factors and Residual Work Ability. Life 2023, 13, 97. https://doi.org/10.3390/life13010097
Sansone D, Tassinari A, Valentinotti R, Kontogiannis D, Ronchese F, Centonze S, Maggiore A, Cegolon L, Filon FL. Persistence of Symptoms 15 Months since COVID-19 Diagnosis: Prevalence, Risk Factors and Residual Work Ability. Life. 2023; 13(1):97. https://doi.org/10.3390/life13010097
Chicago/Turabian StyleSansone, Donatella, Alice Tassinari, Romina Valentinotti, Dimitra Kontogiannis, Federico Ronchese, Sandro Centonze, Adele Maggiore, Luca Cegolon, and Francesca Larese Filon. 2023. "Persistence of Symptoms 15 Months since COVID-19 Diagnosis: Prevalence, Risk Factors and Residual Work Ability" Life 13, no. 1: 97. https://doi.org/10.3390/life13010097