
Mediterranean Dietary Pattern and Cardiovascular Risk in Pregnant Women

 , ,
, , 
Abstract
:1. Introduction
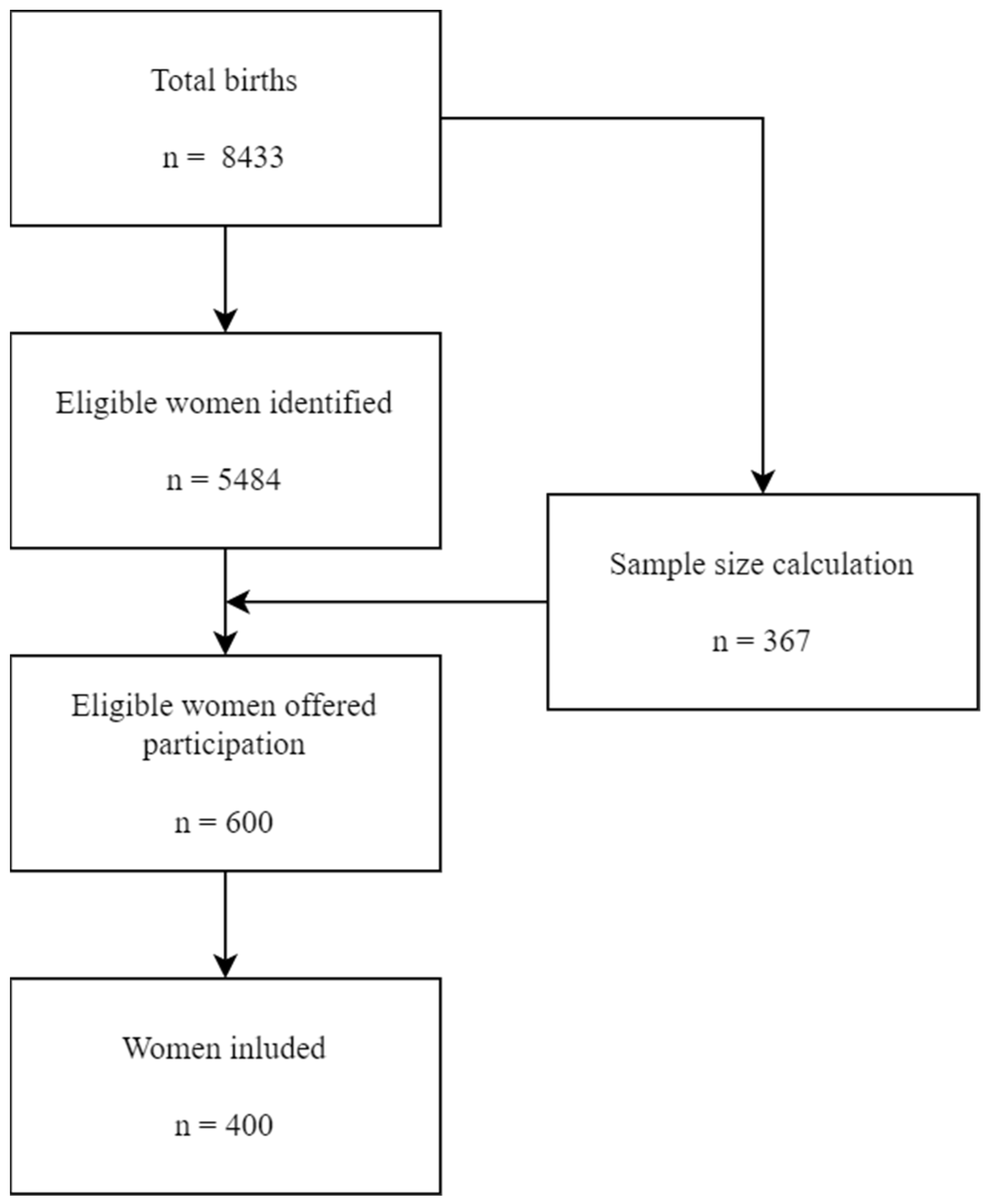
2. Materials and Methods
2.1. Personal Characteristics
2.2. Dietary Assessment
2.3. Statistics
3. Results
3.1. Sociodemographic Characteristics
3.2. Cardiovascular Risk
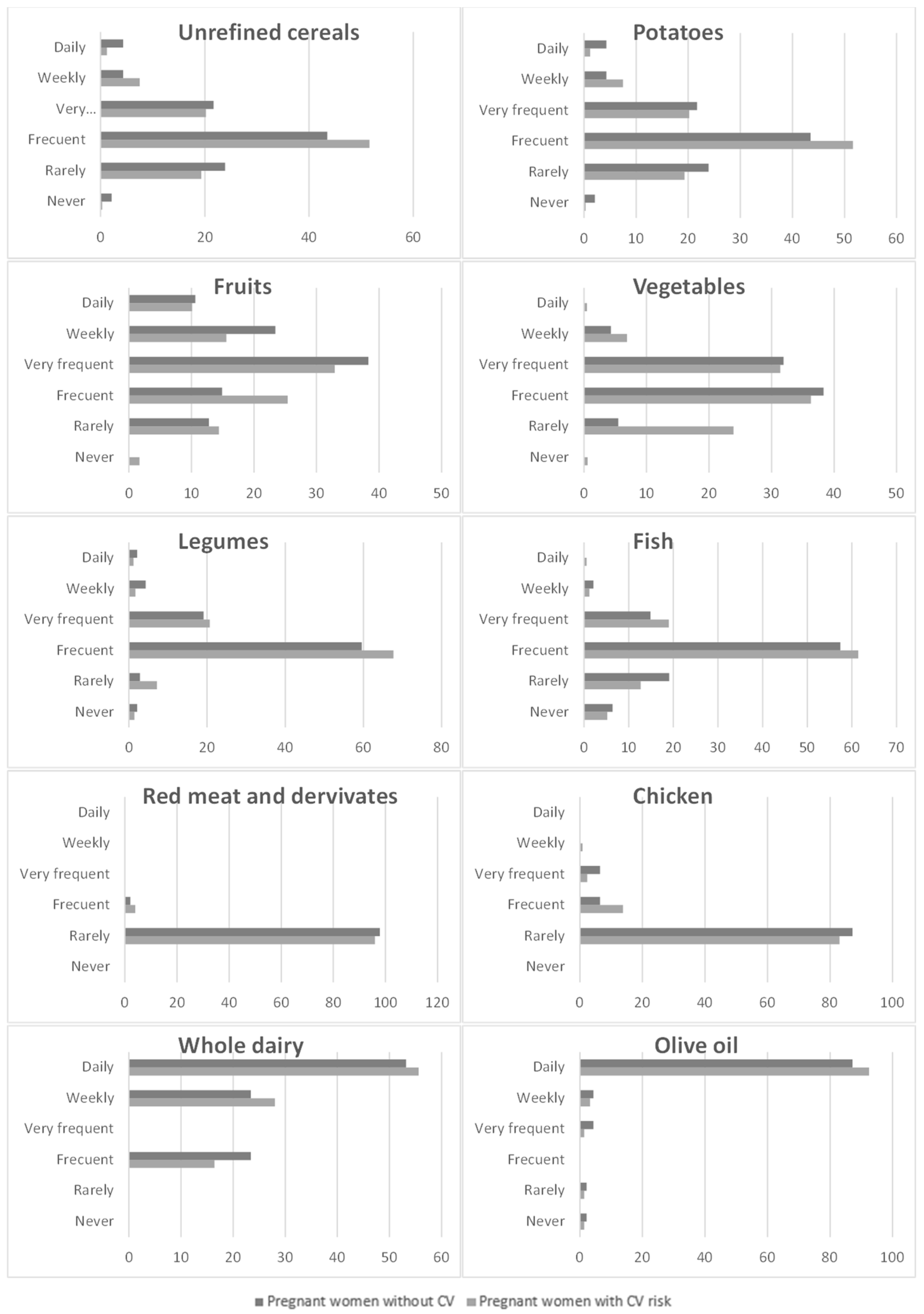
3.3. Food Consumption Corresponding to Mediterranean Dietary Pattern
3.4. Outcomes
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martínez García, R.M.; Jiménez Ortega, A.I.; Navia Lombán, B. Suplementos En Gestación: Últimas Recomendaciones. Nutr. Hosp. 2016, 33, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toca, M.D.C.; Tonietti, M.; Vecchiarelli, C. Nutrición pre y posnatal: Impacto a largo plazo en la salud. Arch. Argent. Pediatr. 2015, 113, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Gernand, A.D.; Schulze, K.J.; Stewart, C.P.; West, K.P., Jr.; Christian, P. Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nat. Rev. Endocrinol. 2016, 12, 274–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lowensohn, R.I.; Stadler, D.D.; Naze, C. Current Concepts of Maternal Nutrition. Obstet. Gynecol. Surv. 2016, 71, 413–426. [Google Scholar] [CrossRef] [Green Version]
- Castelló, A.; Researchers, O.B.O.M.-S.; Amiano, P.; de Larrea, N.F.; Martín, V.; Alonso, M.H.; Castaño-Vinyals, G.; Pérez-Gómez, B.; Olmedo-Requena, R.; Guevara, M.; et al. Low adherence to the western and high adherence to the mediterranean dietary patterns could prevent colorectal cancer. Eur. J. Nutr. 2018, 58, 1495–1505. [Google Scholar] [CrossRef]
- Castro-Diehl, C.; Wood, A.C.; Redline, S.; Reid, M.; Johnson, D.A.; Maras, J.E.; Jacobs, D.R., Jr.; Shea, S.; Crawford, A.; St-Onge, M. Mediterranean Diet Pattern and Sleep Duration and Insomnia Symptoms in the Multi-Ethnic Study of Atherosclerosis. Sleep 2018, 41, zsy158. [Google Scholar] [CrossRef]
- Amati, F.; Hassounah, S.; Swaka, A. The Impact of Mediterranean Dietary Patterns During Pregnancy on Maternal and Offspring Health. Nutrients 2019, 11, 1098. [Google Scholar] [CrossRef] [Green Version]
- Vitale, M.; Masulli, M.; Calabrese, I.; Rivellese, A.A.; Bonora, E.; Signorini, S.; Perriello, G.; Squatrito, S.; Buzzetti, R.; Sartore, G.; et al. Impact of a Mediterranean Dietary Pattern and Its Components on Cardiovascular Risk Factors, Glucose Control, and Body Weight in People with Type 2 Diabetes: A Real-Life Study. Nutrients 2018, 10, 1067. [Google Scholar] [CrossRef] [Green Version]
- Godos, J.; Castellano, S.; Marranzano, M. Adherence to a Mediterranean Dietary Pattern Is Associated with Higher Quality of Life in a Cohort of Italian Adults. Nutrients 2019, 11, 981. [Google Scholar] [CrossRef] [Green Version]
- Parisi, F.; Rousian, M.; Huijgen, N.A.; Koning, A.H.; Willemsen, S.P.; de Vries, J.H.; Cetin, I.; Steegers, E.A.; Steegers-Theunissen, R. Periconceptional Maternal ‘high Fish and Olive Oil, Low Meat’dietary Pattern is Associated with Increased Embryonic Growth: The Rotterdam Periconceptional Cohort (Predict) Study. Ultrasound Obstet. Gynecol. 2017, 50, 709–716. [Google Scholar] [CrossRef]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61 (Suppl. 6), 1402S–1406S. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Roman-Viñas, B.; Sanchez-Villegas, A.; Guasch-Ferré, M.; Corella, D.; La Vecchia, C. Benefits of the Mediterranean diet: Epidemiological and molecular aspects. Mol. Asp. Med. 2019, 67, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Martini, D. Health Benefits of Mediterranean Diet. Nutrients 2019, 11, 1802. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Willett, W.C. The Mediterranean diet and health: A comprehensive overview. J. Intern. Med. 2021, 290, 549–566. [Google Scholar] [CrossRef] [PubMed]
- Galbete, C.; Schwingshackl, L.; Schwedhelm, C.; Boeing, H.; Schulze, M.B. Evaluating Mediterranean diet and risk of chronic disease in cohort studies: An umbrella review of meta-analyses. Eur. J. Epidemiol. 2018, 33, 909–931. [Google Scholar] [CrossRef] [Green Version]
- Dernini, S.; Berry, E.M.; Serra-Majem, L.; La Vecchia, C.; Capone, R.; Medina, F.X.; Aranceta-Bartrina, J.; Belahsen, R.; Burlingame, B.; Calabrese, G.; et al. Med Diet 4.0: The Mediterranean diet with four sustainable benefits. Public Health Nutr. 2017, 20, 1322–1330. [Google Scholar] [CrossRef] [Green Version]
- Tarraga Lopez, P.J.; Panisello Royo, J.M.; Carbayo Herencia, J.A.; Carro, A.; Rosich, N.; Panisello, M.; Allins Presas, J.; Solera Albero, J. Changes in Adherence to the Mediterranean Diet Observed in a Spanish Population during Confinement for the SARS-CoV-2 Pandemic. Nutr. Hosp. 2021, 38, 109–120. [Google Scholar] [CrossRef]
- Blas, A.; Garrido, A.; Unver, O.; Willaarts, B. A comparison of the Mediterranean diet and current food consumption patterns in Spain from a nutritional and water perspective. Sci. Total Environ. 2019, 664, 1020–1029. [Google Scholar] [CrossRef]
- Zaragoza-Martí, A.; Ruiz-Ródenas, N.; Herranz-Chofre, I.; Sánchez-SanSegundo, M.; Delgado, V.d.l.C.S.; Hurtado-Sánchez, J.A. Adherence to the Mediterranean Diet in Pregnancy and Its Benefits on Maternal-Fetal Health: A Systematic Review of the Literature. Front. Nutr. 2022, 9, 813942. [Google Scholar] [CrossRef]
- Kibret, K.T.; Chojenta, C.; Gresham, E.; Tegegne, T.K.; Loxton, D. Maternal dietary patterns and risk of adverse pregnancy (hypertensive disorders of pregnancy and gestational diabetes mellitus) and birth (preterm birth and low birth weight) outcomes: A systematic review and meta-analysis. Public Health Nutr. 2018, 22, 506–520. [Google Scholar] [CrossRef]
- AlAufi, N.S.; Chan, Y.M.; Waly, M.I.; Chin, Y.S.; Yusof, B.-N.M.; Ahmad, N. Application of Mediterranean Diet in Cardiovascular Diseases and Type 2 Diabetes Mellitus: Motivations and Challenges. Nutrients 2022, 14, 2777. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health: A Critical Review. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.; Ilyas, I.; Little, P.J.; Li, H.; Kamato, D.; Zheng, X.; Luo, S.; Li, Z.; Liu, P.; Han, J.; et al. Endothelial Dysfunction in Atherosclerotic Cardiovascular Diseases and Beyond: From Mechanism to Pharmacotherapies. Pharmacol. Rev. 2021, 73, 924–967. [Google Scholar] [CrossRef]
- Yubero-Serrano, E.M.; Fernandez-Gandara, C.; Garcia-Rios, A.; Rangel-Zuñiga, O.A.; Gutierrez-Mariscal, F.M.; Torres-Peña, J.D.; Marin, C.; Lopez-Moreno, J.; Castaño, J.P.; Delgado-Lista, J.; et al. Mediterranean diet and endothelial function in patients with coronary heart disease: An analysis of the CORDIOPREV randomized controlled trial. PLoS Med. 2020, 17, e1003282. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases Country Profiles; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Zhou, S.J.; Flynn, A.C.; Malek, L.; Greco, R.; Moran, L.; Martin, J.C. The Assessment of Diet Quality and Its Effects on Health Outcomes Pre-pregnancy and during Pregnancy. Semin. Reprod. Med. 2016, 34, 083–092. [Google Scholar] [CrossRef]
- Gaillard, R. Maternal obesity during pregnancy and cardiovascular development and disease in the offspring. Eur. J. Epidemiol. 2015, 30, 1141–1152. [Google Scholar] [CrossRef] [Green Version]
- Nelson, S.M.; Matthews, P.; Poston, L. Maternal metabolism and obesity: Modifiable determinants of pregnancy outcome. Hum. Reprod. Update 2010, 16, 255–275. [Google Scholar] [CrossRef] [Green Version]
- Koletzko, B.; Brands, B.; Chourdakis, M.; Cramer, S.; Grote, V.; Hellmuth, C.; Kirchberg, F.; Prell, C.; Rzehak, P.; Uhl, O.; et al. The Power of Programming and the EarlyNutrition Project: Opportunities for Health Promotion by Nutrition during the First Thousand Days of Life and Beyond. Ann. Nutr. Metab. 2014, 64, 187–196. [Google Scholar] [CrossRef]
- Alfadhli, E.M. Gestational Diabetes Mellitus. Saudi Med. J. 2015, 36, 399. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Milias, G.A.; Pitsavos, C.; Stefanadis, C. MedDietScore: A computer program that evaluates the adherence to the Mediterranean dietary pattern and its relation to cardiovascular disease risk. Comput. Methods Programs Biomed. 2006, 83, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) and National Research Council (US). Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain during Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartrina, J.A.; Val, M.V.A.; Aldalur, E.M.; de Victoria Muñoz, E.M.; Anta, R.M.O.; Rodrigo, C.P.; Izquierdo, J.Q.; Martín, A.R.; Viñas, B.R.; Castell, G.S. Guías Alimentarias Para La Población Española (SENC, Diciembre 2016): La Nueva Pirámide De La Alimentación Saludable. Nutr. Hosp. Órgano Of. Soc. Española Nutr. Parenter. Y Enter. 2016, 33, 1–48. [Google Scholar]
- Dapcich, V.; Salvador Castell, G.; Ribas Barba, L.; Pérez Rodrigo, C.; Aranceta Bartrina, J.; Serra Majem, L. Guía de la Alimentación Saludable; SENC: Tokyo, Japan, 2004. [Google Scholar]
- Farré Rovira, R.; Cameán Fernández, A.M.; Vidal Carou, M.d.C.; López-Santacruz Serraller, A.; Teruel Muñoz, V.; Teseo Canales, E. Informe Del Comité Científico De La Agencia Española De Seguridad Alimentaria Y Nutrición (AESAN) En Relación a Los Niveles De Mercurio Establecidos Para Los Productos De La Pesca. Rev. Del Com. Científico AESAN 2011, 13, 29–36. [Google Scholar]
- De Caterina, R.; Zampolli, A.; Del Turco, S.; Madonna, R.; Massaro, M. Nutritional mechanisms that influence cardiovascular disease. Am. J. Clin. Nutr. 2006, 83, 421S–426S. [Google Scholar] [CrossRef] [Green Version]
- Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Evaluación Nutricional de la Dieta Española. I. Energía y Macronutrientes. Sobre Datos de la Encuesta Nacional DeIngesta Dietética (ENIDE); AESAN: Madrid, Spain, 2011. [Google Scholar]
- León-Muñoz, L.M.; Guallar-Castillón, P.; Graciani, A.; López-García, E.; Mesas, A.E.; Aguilera, M.T.; Banegas, J.R.; Rodríguez-Artalejo, F. Adherence to the Mediterranean Diet Pattern Has Declined in Spanish Adults. J. Nutr. 2012, 142, 1843–1850. [Google Scholar] [CrossRef] [Green Version]
- Chatzi, L.; Torrent, M.; Romieu, I.; Garcia-Esteban, R.; Ferrer, C.; Vioque, J.; Kogevinas, M.; Sunyer, J. Mediterranean diet in pregnancy is protective for wheeze and atopy in childhood. Thorax 2008, 63, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Mariscal-Arcas, M.; Lopez-Martinez, C.; Granada, A.; Olea, N.; Lorenzo-Tovar, M.; Olea-Serrano, F. Organochlorine pesticides in umbilical cord blood serum of women from Southern Spain and adherence to the Mediterranean diet. Food Chem. Toxicol. 2010, 48, 1311–1315. [Google Scholar] [CrossRef]
- Gesteiro, E.; Bastida, S.; Rodríguez Bernal, B.; Sánchez-Muniz, F.J. Adherence to Mediterranean Diet during Pregnancy and Serum Lipid, Lipoprotein and Homocysteine Concentrations at Birth. Eur. J. Nutr. 2015, 54, 1191–1199. [Google Scholar] [CrossRef]
- Peraita-Costa, I.; Llopis-González, A.; Perales-Marín, A.; Sanz, F.; Llopis-Morales, A.; Morales-Suárez-Varela, M. A Retrospective Cross-Sectional Population-Based Study on Prenatal Levels of Adherence to the Mediterranean Diet: Maternal Profile and Effects on the Newborn. Int. J. Environ. Res. Public Health 2018, 15, 1530. [Google Scholar] [CrossRef] [Green Version]
- Olmedo-Requena, R.; Fernández, J.G.; Prieto, C.A.; Moreno, J.M.; Bueno-Cavanillas, A.; Jiménez-Moleón, J.J. Factors associated with a low adherence to a Mediterranean diet pattern in healthy Spanish women before pregnancy. Public Health Nutr. 2013, 17, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Paredes, C.; Hsu, R.C.; Tong, A.; Johnson, J.R. Obesity and Pregnancy. NeoReviews 2021, 22, e78–e87. [Google Scholar] [CrossRef]
- Grieger, J.A.; Hutchesson, M.J.; Cooray, S.D.; Khomami, M.B.; Zaman, S.; Segan, L.; Teede, H.; Moran, L.J. A review of maternal overweight and obesity and its impact on cardiometabolic outcomes during pregnancy and postpartum. Ther. Adv. Reprod. Health 2021, 15, 2633494120986544. [Google Scholar] [CrossRef] [PubMed]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean Diet and Health Outcomes in the SUN Cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef] [Green Version]
- Stüber, T.N.; Künzel, E.C.; Zollner, U.; Rehn, M.; Wöckel, A.; Hönig, A. Prevalence and Associated Risk Factors for Obesity During Pregnancy Over Time. Geburtshilfe Und Frauenheilkd. 2015, 75, 923–928. [Google Scholar] [CrossRef] [Green Version]
- Zhou, A.; Xiong, C.; Hu, R.; Zhang, Y.; Bassig, B.A.; Triche, E.W.; Yang, S.; Qiu, L.; Zhang, Y.; Yao, C.; et al. Pre-Pregnancy BMI, Gestational Weight Gain, and the Risk of Hypertensive Disorders of Pregnancy: A Cohort Study in Wuhan, China. PLoS ONE 2015, 10, e0136291. [Google Scholar] [CrossRef]
- Silva-del Valle, M.A.; Sánchez-Villegas, A.; Serra-Majem, L. Association between the Adherence to the Mediterranean Diet and Overweight and Obesity in Pregnant Women in Gran Canaria. Nutr. Hosp. 2013, 28, 654–659. [Google Scholar] [PubMed]
- Serra-Majem, L. Efficacy of Diets in Weight Loss Regimens: Is the Mediterranean Diet Appropiate? Pol. Arch. Med. Wewn. 2008, 118, 691–693. [Google Scholar] [CrossRef]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.L.; Boyle, J.A.; Harrison, C.L.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; et al. Gestational weight gain across continents and ethnicity: Systematic review and meta-analysis of maternal and infant outcomes in more than one million women. BMC Med. 2018, 16, 153. [Google Scholar] [CrossRef] [Green Version]
- Champion, M.L.; Harper, L.M. Gestational Weight Gain: Update on Outcomes and Interventions. Curr. Diabetes Rep. 2020, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- McDowell, M.; Cain, M.A.; Brumley, J. Excessive Gestational Weight Gain. J. Midwifery Womens Health 2019, 64, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Radwan, H.; Hashim, M.; Hasan, H.; Abbas, N.; Obaid, R.R.S.; Al Ghazal, H.; Naja, F. Adherence to the Mediterranean diet during pregnancy is associated with lower odds of excessive gestational weight gain and postpartum weight retention: Results of the Mother-Infant Study Cohort. Br. J. Nutr. 2021, 128, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Al Wattar, H.B.; Dodds, J.; Placzek, A.; Beresford, L.; Spyreli, E.; Moore, A.; Gonzalez Carreras, F.J.; Austin, F.; Murugesu, N.; Roseboom, T.J. Mediterranean-Style Diet in Pregnant Women with Metabolic Risk Factors (ESTEEM): A Pragmatic Multicentre Randomised Trial. PLoS Med. 2019, 16, e1002857. [Google Scholar]
- Pathirana, M.M.; Lassi, Z.; Ali, A.; Arstall, M.; Roberts, C.T.; Andraweera, P.H. Cardiovascular risk factors in women with previous gestational diabetes mellitus: A systematic review and meta-analysis. Rev. Endocr. Metab. Disord. 2020, 22, 729–761. [Google Scholar] [CrossRef]
- Sullivan, S.D.; Umans, J.G.; Ratner, R. Gestational Diabetes: Implications for Cardiovascular Health. Curr. Diabetes Rep. 2011, 12, 43–52. [Google Scholar] [CrossRef]
- Shin, D.; Lee, K.W.; Song, W.O. Dietary Patterns during Pregnancy Are Associated with Risk of Gestational Diabetes Mellitus. Nutrients 2015, 7, 9369–9382. [Google Scholar] [CrossRef] [Green Version]
- de la Torre, N.G.; Assaf-Balut, C.; Varas, I.J.; del Valle, L.; Durán, A.; Fuentes, M.; del Prado, N.; Bordiú, E.; Valerio, J.J.; Herraiz, M.A.; et al. Effectiveness of Following Mediterranean Diet Recommendations in the Real World in the Incidence of Gestational Diabetes Mellitus (GDM) and Adverse Maternal-Foetal Outcomes: A Prospective, Universal, Interventional Study with a Single Group. The St Carlos Study. Nutrients 2019, 11, 1210. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Schulze, M.B.; Solomon, C.G.; Hu, F.B. A prospective study of dietary patterns, meat intake and the risk of gestational diabetes mellitus. Diabetologia 2006, 49, 2604–2613. [Google Scholar] [CrossRef] [Green Version]
- Radesky, J.S.; Oken, E.; Rifas-Shiman, S.L.; Kleinman, K.P.; Rich-Edwards, J.W.; Gillman, M.W. Diet during early pregnancy and development of gestational diabetes. Paediatr. Périnat. Epidemiol. 2007, 22, 47–59. [Google Scholar] [CrossRef] [Green Version]
- Karamanos, B.; Thanopoulou, A.; Anastasiou, E.; Assaad-Khalil, S.; Albache, N.; Bachaoui, M.; Slama, C.B.; El Ghomari, H.; Jotic, A.; Lalic, N.; et al. Relation of the Mediterranean diet with the incidence of gestational diabetes. Eur. J. Clin. Nutr. 2013, 68, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brantsæter, A.L.; Haugen, M.; Samuelsen, S.O.; Torjusen, H.; Trogstad, L.; Alexander, J.; Magnus, P.; Meltzer, H.M. A Dietary Pattern Characterized by High Intake of Vegetables, Fruits, and Vegetable Oils Is Associated with Reduced Risk of Preeclampsia in Nulliparous Pregnant Norwegian Women. J. Nutr. 2009, 139, 1162–1168. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Gong, Y.; Della Corte, K.; Yu, D.; Xue, H.; Shan, S.; Tian, G.; Liang, Y.; Zhang, J.; He, F.; et al. Relevance of dietary glycemic index, glycemic load and fiber intake before and during pregnancy for the risk of gestational diabetes mellitus and maternal glucose homeostasis. Clin. Nutr. 2021, 40, 2791–2799. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, T.L.; Anderson, M.A.; Chartier-Logan, C.; Friedman, J.E.; Barbour, L.A. Strategies in the Nutritional Management of Gestational Diabetes. Clin. Obstet. Gynecol. 2013, 56, 803–815. [Google Scholar] [CrossRef] [Green Version]
- Chatzi, L.; Mendez, M.; Garcia, R.; Roumeliotaki, T.; Ibarluzea, J.; Tardon, A.; Amiano, P.; Lertxundi, A.; Iñiguez, C.; Vioque, J.; et al. Mediterranean diet adherence during pregnancy and fetal growth: INMA (Spain) and RHEA (Greece) mother–child cohort studies. Br. J. Nutr. 2011, 107, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Northstone, K.; Emmett, P.; Rogers, I. Dietary patterns in pregnancy and associations with socio-demographic and lifestyle factors. Eur. J. Clin. Nutr. 2008, 62, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Toledo, E.; Hu, F.B.; Estruch, R.; Buil-Cosiales, P.; Corella, D.; Salas-Salvadó, J.; Covas, M.I.; Arós, F.; Gómez-Gracia, E.; Fiol, M.; et al. Effect of the Mediterranean diet on blood pressure in the PREDIMED trial: Results from a randomized controlled trial. BMC Med. 2013, 11, 207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Liu, S.; Solomon, C.G.; Hu, F.B. Dietary Fiber Intake, Dietary Glycemic Load, and the Risk for Gestational Diabetes Mellitus. Diabetes Care 2006, 29, 2223–2230. [Google Scholar] [CrossRef] [Green Version]
- Negi, R.; Pande, D.; Karki, K.; Kumar, A.; Khanna, R.S.; Khanna, H.D. Trace elements and antioxidant enzymes associated with oxidative stress in the pre-eclamptic/eclamptic mothers during fetal circulation. Clin. Nutr. 2012, 31, 946–950. [Google Scholar] [CrossRef]
- Davenport, M.H.; Ruchat, S.M.; Poitras, V.J.; Jaramillo Garcia, A.; Gray, C.E.; Barrowman, N.; Skow, R.J.; Meah, V.L.; Riske, L.; Sobierajski, F.; et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 1367–1375. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Kominiarek, M.A.; Rajan, P. Nutrition Recommendations in Pregnancy and Lactation. Med. Clin. N. Am. 2016, 100, 1199–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malesza, I.J.; Bartkowiak-Wieczorek, J.; Winkler-Galicki, J.; Nowicka, A.; Dzięciołowska, D.; Błaszczyk, M.; Gajniak, P.; Słowińska, K.; Niepolski, L.; Walkowiak, J. The Dark Side of Iron: The Relationship between Iron, Inflammation and Gut Microbiota in Selected Diseases Associated with Iron Deficiency Anaemia—A Narrative Review. Nutrients 2022, 14, 3478. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Bernal, C.L.; Ramon, R.; Quiles, J.; Murcia, M.; Navarrete-Munoz, E.M.; Vioque, J.; Ballester, F.; Rebagliato, M. Dietary Intake in Pregnant Women in a Spanish Mediterranean Area: As Good as it is Supposed to be? Public Health Nutr. 2013, 16, 1379–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spadafranca, A.; Piuri, G.; Bulfoni, C.; Liguori, I.; Battezzati, A.; Bertoli, S.; Speciani, A.F.; Ferrazzi, E. Adherence to the Mediterranean Diet and Serum Adiponectin Levels in Pregnancy: Results from a Cohort Study in Normal Weight Caucasian Women. Nutrients 2018, 10, 928. [Google Scholar] [CrossRef] [Green Version]
- Duchen, K.; Faresjö, O.; Klingberg, S.; Faresjö, T.; Ludvigsson, J. Fatty fish intake in mothers during pregnancy and in their children in relation to the development of obesity and overweight in childhood: The prospective ABIS study. Obes. Sci. Pract. 2019, 6, 57–69. [Google Scholar] [CrossRef] [Green Version]
- Mori, T.A. Marine OMEGA-3 fatty acids in the prevention of cardiovascular disease. Fitoterapia 2017, 123, 51–58. [Google Scholar] [CrossRef]
- Campoy, C.; Cabero, L.; Sanjurjo, P.; Serra-Majem, L.; Anadón, A.; Morán, J.; Fraga, J. Actualización, Recomendaciones Y Consenso Sobre El Papel De Los Ácidos Grasos Poliinsaturados De Cadena Larga En La Gestación, Lactancia Y Primer Año De Vida. Med. Clínica 2010, 135, 75–82. [Google Scholar] [CrossRef]
- Middleton, P.; Gomersall, J.C.; Gould, J.F.; Shepherd, E.; Olsen, S.F.; Makrides, M. Omega-3 Fatty Acid Addition during Pregnancy. Cochrane Database Syst. Rev. 2018, 11, CD003402. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Women with Cardiovascular Risk (n = 349) % (95%CI)/Mean ± SD | Women without Cardiovascular Risk (n = 51) % (95%CI)/Mean ± SD | p-Value * | |
|---|---|---|---|
| n (%) | 87.25 [83.48–90.27] | 12.75 [9.72–16.51] | - |
| Age (years) | 32.38 ± 5.73 | 33.31 ± 5.55 | 0.291 |
| Pre-pregnancy weight (Kg) Final weight (Kg) Weight gained (Kg) | 65.00 ± 12.67 76.89 ± 13.12 12.00 ± 8.80 | 63.99 ± 12.06 76.73 ± 12.78 12.74 ± 5.13 | 0.600 0.935 0.571 |
| BMI before pregnancy BMI 3rd trimester | 24.25 ± 5.10 28.77 ± 5.16 | 24.25 ± 4.45 29.05 ± 4.56 | 0.994 0.712 |
| Height (m) | 1.63 ± 0.06 | 1.62 ± 0.06 | 0.513 |
| Nulliparous (%) | 51.00 [45.63–56.64] | 50.00 [35.42–64.57] | 0.997 |
| Race/Ethnicity European African American Asian | 84.00 [79.58–87.56] 4.60 [2.73–7.48] 9.40 [6.69–13.14] 2.00 [0.88–4.27] | 91.70 [79.12–97.29] 6.30 [1.62–18.20] 2.00 [0.10–12.47] 0.00 [0.00–9.23] | 0.161 0.883 0.150 - |
| Gestation weeks | 39.25 ± 1.93 | 38.70 ± 2.21 | 0.072 |
| Gestational diabetes (%) | 9.73 [6.84–13.58] | 6.97 [1.81–20.12] | 0.606 |
| Education No formal education Primary Secondary Tertiary | 4.29 [2.42–6.98] 14.32 [10.82–18.44] 45.27 [39.98–50.66] 36.10 [31.05–41.38] | 1.96 [0.10–11.79] 11.76 [4.44–23.86] 29.41 [17.48–43.82] 50.98 [36.77–65.04] | 0.679 0.622 0.032 0.040 |
| Employment status Employed Unemployed | 65.61 [60.37–70.59] 34.38 [29.40–39.62] | 64.70 [50.06–77.56] 27.45 [15.89–41.74] | 0.898 0.327 |
| Place of residence Urban (Population > 10,000) Rural (Population < 10,000) | 100.0 [100.0–100.0] 0.0 [0.00–0.00] | 100.0 [100.0–100.0] 0.0 [0.00–0.00] | - - |
| Physical activity (%) None Light Moderate | 77.10 [72.23–81.31] 22.90 [18.24–28.63] 66.05 [59.37–71.03] 11.05 [7.14–14.49] | 79.20 [66.45–89.71] 20.80 [11.11–38.03] 62.50 [46.91–77.43] 16.70 [7.69–32.64] | 0.502 0.817 0.717 0.321 |
| Tobacco use in 1st trimester (%) | 13.18 [9.90–17.29] | 10.41 [3.89–23.44] | 0.004 |
| Alcohol consumption (%) | 2.50 [1.26–5.02] | 6.25 [1.62–18.20] | 0.165 |
| Folic acid intake (%) | 71.34 [66.24–75.97] | 54.16 [39.30–68.36] | 0.202 |
| Iron intake (%) | 82.70 [78.22–86.45] | 81.25 [66.89–90.56] | 0.803 |
| Vitamin supplements (%) | 87.57 [83.51–90.76] | 80.85 [66.27–90.35] | 0.202 |
| Food supplements (%) | 0.28 [0.015–1.84] | 0.00 [0.00–9.23] | 0.710 |
| Never (0 Times/Month) % [95%CI] | Rarely (1–4 Times/Month) % [95%CI] | Frequent (5–8 Times/Month) % [95%CI] | Very frequent (9–12 Times/Month) % [95%CI] | Weekly (13–18 Times/Month) % [95%CI] | Daily (>18 Times/Month) % [95%CI] | p-Value * | |
|---|---|---|---|---|---|---|---|
| Women with cardiovascular risk (n = 349) | |||||||
| Unrefined cereals | 0.3 [0.15–1.83] | 19.3 [15.27–23.80] | 51.6 [45.91–56.63] | 20.2 [16.06–24.72] | 7.5 [5.01–10.85] | 1.2 [0.36–3.11] | <0.001 |
| Potatoes | 0.9 [0.22–2.70] | 67.1 [61.22–71.36] | 24.9 [20.28–29.57] | 4.9 [2.95–7.83] | 1.7 [0.70–3.89] | 0.6 [0.09–2.28] | <0.001 |
| Fruits | 1.7 [0.70–3.89] | 14.4 [10.91–18.54] | 25.4 [20.81–30.17] | 32.9 [27.82–37.89] | 15.6 [1.90–19.79] | 10.1 [7.17–13.78] | <0.001 |
| Vegetables | 0.6 [0.09–2.28] | 23.9 [19.48–29.67] | 36.3 [31.10–41.41] | 31.4 [26.46–36.42] | 6.9 [4.78–10.52] | 0.5 [0.09–2.28] | <0.001 |
| Legumes | 1.4 [0.52–3.50] | 7.2 [4.78–10.52] | 67.7 [62.10–72.17] | 20.7 [16.58–25.33] | 1.7 [0.70–3.89] | 1.2 [0.36–3.11] | <0.001 |
| Fish | 5.2 [3.17–8.17] | 12.7 [9.40–16.66] | 61.4 [55.67–66.13] | 19.0 [15.01–23.5] | 1.2 [0.36–3.11] | 0.6 [0.09–2.28] | <0.001 |
| Red meat and derivatives | 0.0 [0.00–1.35] | 96.0 [92.51–87.26] | 4.0 [2.29–6.79] | 0.0 [0.00–1.35] | 0.0 [0.00–1.35] | 0.0 [0.00–1.35] | <0.001 |
| Chicken | 0.0 [0.00–1.35] | 83.0 [78.03–86.27] | 13.8 [10.40–17.92] | 2.3 [1.06–4.64] | 0.9 [0.22–2.70] | 0.0 [0.00–1.35] | <0.001 |
| Whole dairy | 0.0 [0.00–1.35] | 0.0 [0.00–1.35] | 16.4 [12.69–20.72] | 0.0 [0.00–1.35] | 28.0 [23.22–32.86] | 55.6 [49.91–60.57] | <0.001 |
| Use of olive oil | 1.4 [0.52–3.50] | 1.4 [0.52–3.50] | 0.0 [0.00–1.35] | 1.4 [0.52–3.50] | 3.2 [1.66–5.73] | 92.5 [88.48–94.51] | <0.001 |
| Alcoholic drinks | 100.0 [100.0–100.0] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | - |
| Women without cardiovascular risk (n = 51) | |||||||
| Unrefined cereals | 2.1 [0.10–12.47] | 23.9 [12.51–37.66] | 43.5 [27.93–56.72] | 21.7 [10.95–35.40] | 4.3 [0.72–15.42] | 4.3 [0.72–15.42] | <0.001 |
| Potatoes | 2.1 [0.10–12.47] | 57.4 [41.28–70.22] | 34.0 [20.80–48.51] | 4.3 [0.72–15.42] | 2.1 [0.10–12.47] | 0.0 [0.00–9.23] | <0.001 |
| Fruits | 0.0 [0.00–9.23] | 12.8 [5.18–25.94] | 14.9 [6.54–28.37] | 38.3 [24.32–52.66] | 23.4 [12.51–37.66] | 10.6 [3.89–23.44] | <0.001 |
| Vegetables | 0.0 [0.00–9.23] | 5.5 [14.10–39.89] | 38.3 [24.32–52.66] | 31.9 [9.09–46.40] | 4.3 [0.72–15.42] | 0.0 [0.00–9.23] | <0.001 |
| Legumes | 2.1 [0.10–12.47] | 2.8 [5.18–25.94] | 59.6 [43.27–72.06] | 19.1 [9.43–33.10] | 4.3 [0.72–15.42] | 2.1 [0.10–12.47] | <0.001 |
| Fish | 6.4 [1.62–18.20] | 19.1 [9.43–33.10] | 57.4 [41.70.22] | 14.9 [6.54–28.37] | 2.1 [0.10–12.47] | 0.0 [0.00–9.23] | <0.001 |
| Red meat and derivatives | 0.0 [0.00–9.23] | 97.9 [84.57–99.27] | 2.1 [0.10–12.47] | 0.0 [0.00–9.23] | 0.0 [0.00–9.23] | 0.0 [0.00–9.23] | <0.001 |
| Chicken | 0.0 [0.00–9.23] | 87.2 [71.62–93.45] | 6.4 [1.62–18.20] | 6.4 [1.62–18.20] | 0.0 [0.00–9.23] | 0.0 [0.00–9.23] | <0.001 |
| Whole dairy | 0.0 [0.00–9.23] | 0.0 [0.00–9.23] | 23.4 [12.51–37.66] | 0.0 [0.00–1.35] | 23.4 [12.51–37.66] | 53.2 [37.35–66.47] | <0.001 |
| Use of olive oil | 2.1 [0.10–12.47] | 2.1 [0.10–12.47] | 0.0 [0.00–9.23] | 4.3 [0.72–15.42] | 4.3 [0.72––15.42] | 87.2 [71.62–93.45] | <0.001 |
| Alcoholic drinks | 100.0 [100.0–100.0] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | 0.0 [0.00–0.00] | - |
| Comparative intake ratio (Women with cardiovascular risk/Women without cardiovascular risk) | |||||||
| Unrefined cereals | 0.14 | 0.80 | 1.18 | 0.93 | 1.74 | 0.27 | - |
| Potatoes | 0.42 | 1.16 | 0.73 | 1.13 | 0.80 | 0.60 | - |
| Fruits | 1.70 | 1.12 | 1.70 | 0.85 | 0.66 | 0.95 | - |
| Vegetables | 0.60 | 4.34 | 0.95 | 0.98 | 1.60 | 0.50 | - |
| Legumes | 0.66 | 2.57 | 1.13 | 1.08 | 0.39 | 0.57 | - |
| Fish | 0.81 | 0.66 | 1.07 | 1.27 | 0.57 | 0.60 | - |
| Red meat and derivatives | 1.00 | 0.98 | 1.90 | 1.00 | 1.00 | 1.00 | - |
| Chicken | 1.00 | 0.95 | 2.15 | 0.36 | 0.90 | 1.00 | - |
| Whole dairy | 1.00 | 1.00 | 0.70 | 1.00 | 1.19 | 1.04 | - |
| Use of olive oil | 0.67 | 0.67 | 1.00 | 0.32 | 0.74 | 1.06 | - |
| Alcoholic drinks | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | - |
| SENC Recommendation (Servings/Day) | Compliance | |||
|---|---|---|---|---|
| Women with Cardiovascular Risk (n = 349) % [95%CI] | Women without Cardiovascular Risk (n = 51) % [95%CI] | p-Value * | ||
| Unrefined cereals | 4–5 | 1.2 [0.36–3.11] | 4.3 [0.72–15.42] | - |
| Fruits | 2–3 | 15.6 [1.9–19.79] | 23.4 [12.51–37.66] | 0.147 |
| Vegetables | 2–4 | 6.9 [4.78–10.52] | 4.3 [0.72–15.42] | 0.620 |
| Legumes | 2 ** | 23.6 [19.21–28.36] | 25.5 [14.77–39.91] | 0.754 |
| Fish | 2 ** | 20.8 [16.58–25.33] | 17.0 [8.86–31.36] | 0.588 |
| Red meat and derivatives | 2 ** | 0 | 0 | - |
| Chicken | 2 ** | 3.16 [26.73–36.71] | 6.4 [1.53–17.22] | 0.559 |
| Whole dairy | 3–4 | 55.6 [49.91–60.57] | 53.2 [37.35–66.47] | 0.722 |
| Olive oil | 3–6 | 92.5 [88.48–94.51] | 87.2 [71.62–93.45] | 0.211 |
| Women with Cardiovascular Risk (n = 349) n/% [95%CI] | Women without Cardiovascular Risk (n = 51) % [95%CI] | p-Value * | |
|---|---|---|---|
| Alcohol | 9/2.57 [1.26–5.01] | 3/5.88 [1.53–17.22] | 0.927 |
| Beer | 8/2.29 [1.06–4.64] | 3/5.88 [1.53–17.22] | 0.291 |
| Wine | 3/0.86 [0.22–2.70] | 2/3.92 [0.68–14.59] | 0.600 |
| Spirits | 1/0.28 [0.01–1.83] | 0 | 0.994 |
| Soft drinks | 130/37.24 [32.20–42.58] | 22/43.13 [29.62–57.14] | 0.513 |
| Coffee | 161/46.13 [40.83–51.51] | 23/45.09 [31.38–59.54] | 0.612 |
| Women with Cardiovascular Risk (n = 349) n/% [95%CI] | Women without Cardiovascular Risk (n = 51) % [95%CI] | p * | Relative Risk | Attributable Risk | |
|---|---|---|---|---|---|
| Preeclampsia | 9 (2.58 (1.26–5.01) | 2 (3.92 (0.68–14.59) | 0.928 | 0.94 (0.71–1.24) | - |
| Neonatal ICU admission | 2 (0.57 (0.10–2.28) | 0 | - | - | - |
| Newborn classification for gestational age | |||||
| Normal | 167 (47.52 (42.52–53.22) | 43 (84.31 (70.86–92.51) | 0.001 | 1 | - |
| Small | 176 (50.42 (45.06–55.79) | 8 (15.68 (7.48–29.13) | 0.003 | 1.20 (1.12–1.30) | 16.9% (10.4–22.9) |
| Large | 6 (1.71 (0.69–3.89) | 0 | - | 1.08 (0.79–1.47) | 7.2% (−26.5–32.0) |
| Women with Cardiovascular Risk (n = 349) Mean ± SD | Women without Cardiovascular Risk (n = 51) Mean ± SD | p-Value * | |
|---|---|---|---|
| O’Sullivan test | 129.01 ± 30.12 | 139.75 ± 24.76 | 0.321 |
| Glucose (1st trimester) | 83.57 ± 8.28 | 93.50 ± 14.85 | 0.113 |
| Haematids (1st trimester) | 5.33 ± 2.50 | 9.08 ± 3.47 | <0.001 |
| Hemoglobin (1st trimester) | 13.86 ± 7.93 | 12.57 ± 1.47 | 0.779 |
| Glucose (2nd trimester) | 68.97 ± 17.78 | 72.00 ± 12.40 | 0.868 |
| Haematids (2nd trimester) | 8.02 ± 4.07 | 11.18 ± 2.70 | <0.001 |
| Hemoglobin (2nd trimester) | 22.78 ± 12.15 | 31.95 ± 10.50 | <0.001 |
| Glucose (3rd trimester) | 72.48 ± 13.45 | 74.00 ± 9.90 | 0.876 |
| Haematids (3rd trimester) | 3.91 ± 0.31 | 4.02 ± 0.58 | 0.451 |
| Hemoglobin (3rd trimester) | 11.66 ± 1.02 | 11.03 ± 1.61 | 0.155 |
| Hematocrit (3rd trimester) | 34.96 ± 2.74 | 33.40 ± 4.8 | 0.188 |
| Iron (3rd trimester) | 79.42 ± 48.11 | 44.50 ± 30.41 | 0.31 |
| Ferritin (3rd trimester) | 21.94 ± 26.73 | 6.50 ± 9.19 | 0.418 |
| Hemoglobin (Birth) | 12.03 ± 1.59 | 11.78 ± 1.32 | 0.659 |
| Hematocrit (Birth) | 35.68 ± 4.34 | 35.20 ± 2.97 | 0.757 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales Suárez-Varela, M.; Peraita-Costa, I.; Marín, A.P.; Marcos Puig, B.; Llopis-Morales, A.; Soriano, J.M. Mediterranean Dietary Pattern and Cardiovascular Risk in Pregnant Women. Life 2023, 13, 241. https://doi.org/10.3390/life13010241
Morales Suárez-Varela M, Peraita-Costa I, Marín AP, Marcos Puig B, Llopis-Morales A, Soriano JM. Mediterranean Dietary Pattern and Cardiovascular Risk in Pregnant Women. Life. 2023; 13(1):241. https://doi.org/10.3390/life13010241
Chicago/Turabian StyleMorales Suárez-Varela, María, Isabel Peraita-Costa, Alfredo Perales Marín, Beatriz Marcos Puig, Agustín Llopis-Morales, and Jose M. Soriano. 2023. "Mediterranean Dietary Pattern and Cardiovascular Risk in Pregnant Women" Life 13, no. 1: 241. https://doi.org/10.3390/life13010241