
The Allosteric Antagonist of the Sigma-2 Receptors—Elayta (CT1812) as a Therapeutic Candidate for Mild to Moderate Alzheimer’s Disease: A Scoping Systematic Review

 ,
,
Abstract
:1. Introduction
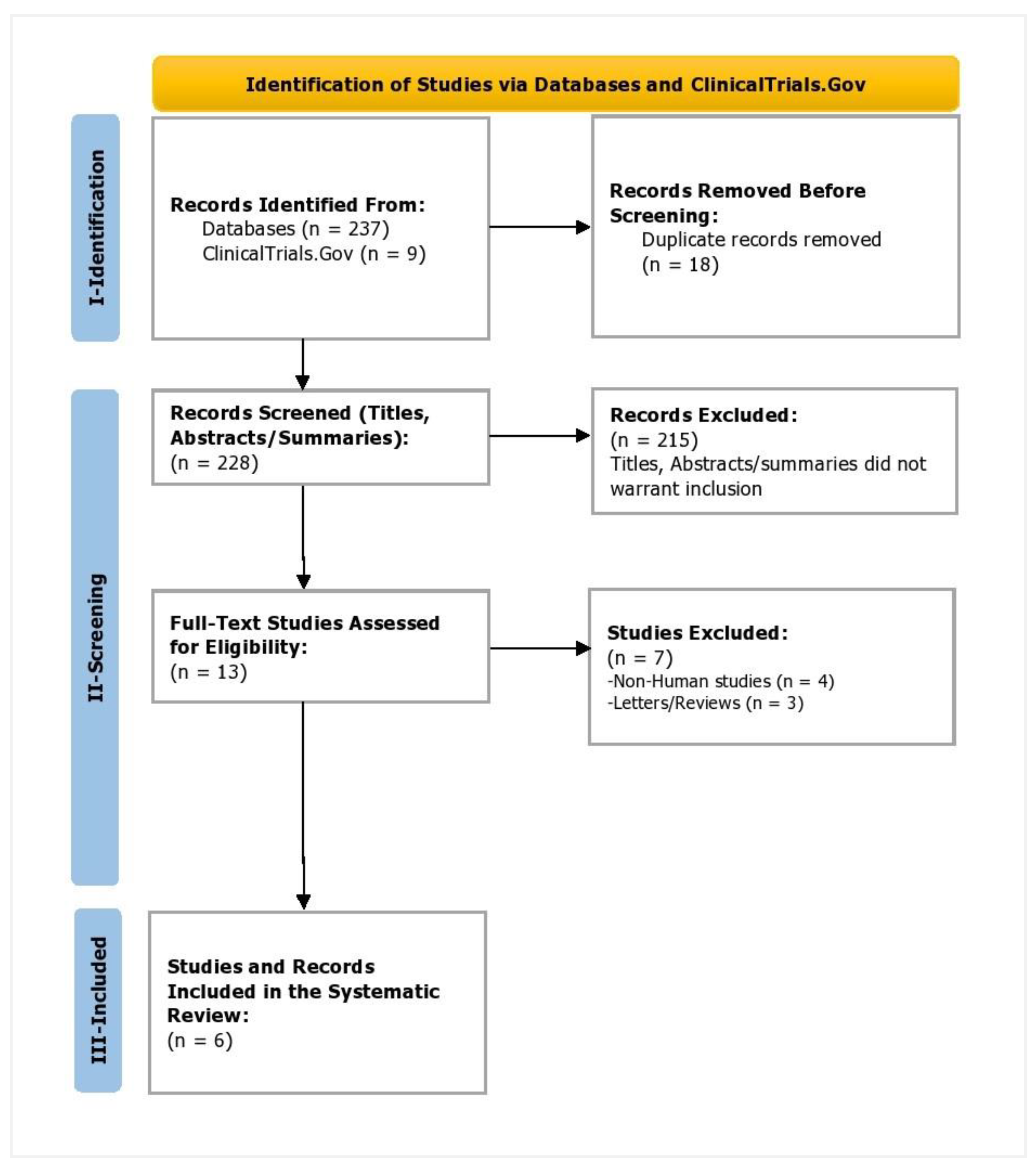
2. Materials and Methods
3. Results
3.1. Characteristics of the Included Trials
3.2. Participant Characteristics, Safety, and Efficacy Outcomes
3.3. Ongoing Clinical Trials
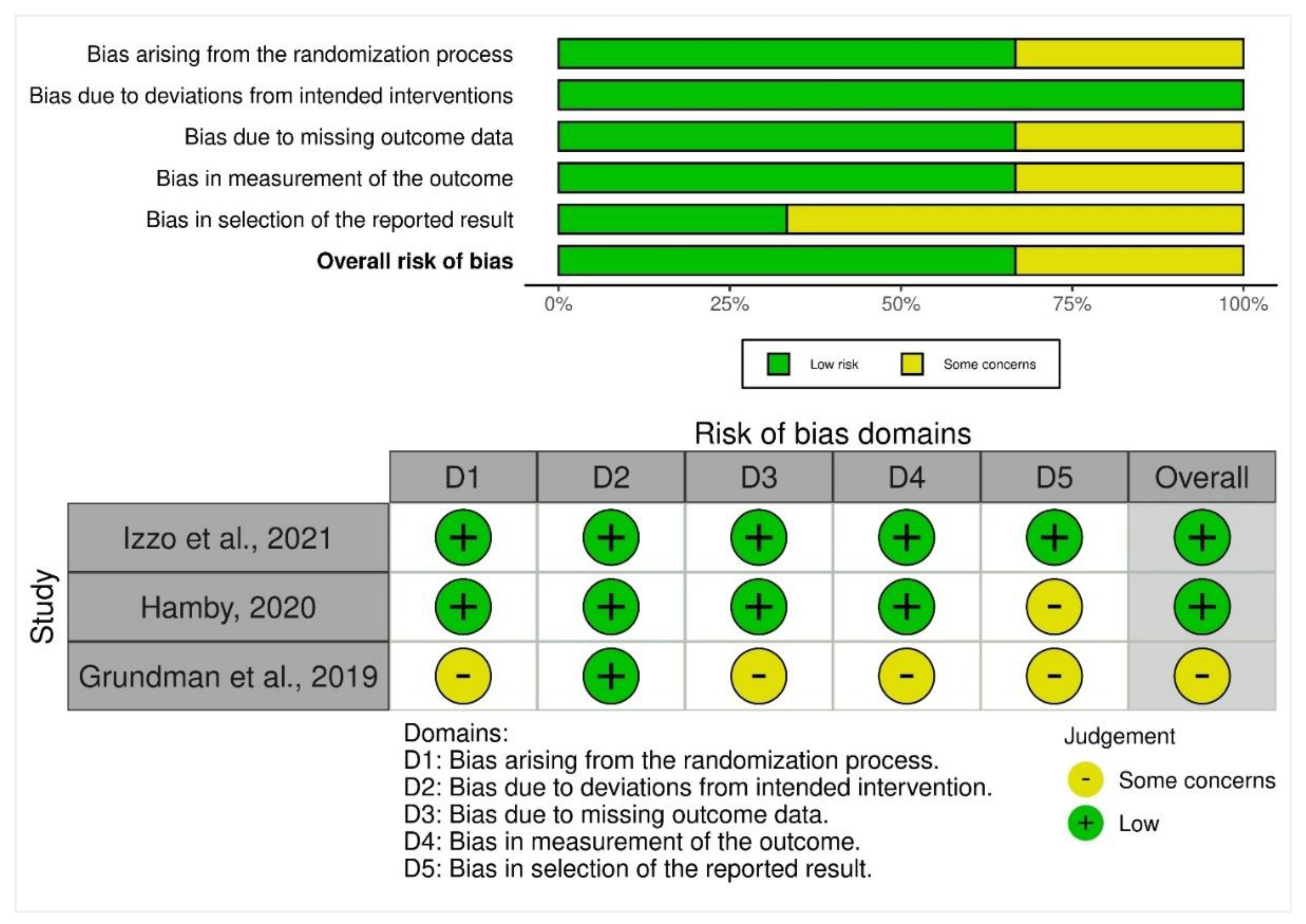
3.4. Quality Appraisal of the Included Trials
4. Discussion
4.1. Limitations
4.2. Implications for Clinical Care
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, X.; Li, C.; Ding, G.; Heng, Y.; Li, A.; Wang, W.; Hou, H.; Wen, J.; Zhang, Y. The Burden of Alzheimer’s Disease Mortality in the United States, 1999-2018. J. Alzheimer’s Dis. 2021, 82, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Chopade, P.; Chopade, N.; Zhao, Z.; Mitragotri, S.; Liao, R.; Chandran Suja, V. Alzheimer’s and Parkinson’s Disease Therapies in the Clinic. Bioeng. Transl. Med. 2022, e10367. [Google Scholar] [CrossRef]
- Deuschl, G.; Beghi, E.; Fazekas, F.; Varga, T.; Christoforidi, K.A.; Sipido, E.; Bassetti, C.L.; Vos, T.; Feigin, V.L. The Burden of Neurological Diseases in Europe: An Analysis for the Global Burden of Disease Study 2017. Lancet Public Health 2020, 5, e551–e567. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Qin, W.; Zhu, M.; Jia, J. Model-Based Projection of Dementia Prevalence in China and Worldwide: 2020–2050. J. Alzheimer’s Dis. 2021, 82, 1823–1831. [Google Scholar] [CrossRef]
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T. Estimation of the Global Prevalence of Dementia in 2019 and Forecasted Prevalence in 2050: An Analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef]
- Clay, E.; Zhou, J.; Yi, Z.-M.; Zhai, S.; Toumi, M. Economic Burden for Alzheimer’s Disease in China from 2010 to 2050: A Modelling Study. J. Mark. Access Health Policy 2019, 7, 1667195. [Google Scholar] [CrossRef]
- McGill-Carter, T. Market Analysis Alzheimer’s Disease 2020. J Psychiatry 2020, 22, 21–22. [Google Scholar]
- Parnetti, L.; Chipi, E.; Salvadori, N.; D’Andrea, K.; Eusebi, P. Prevalence and Risk of Progression of Preclinical Alzheimer’s Disease Stages: A Systematic Review and Meta-Analysis. Alzheimers. Res. Ther. 2019, 11, 1–13. [Google Scholar] [CrossRef]
- Jack, C.R.; Therneau, T.M.; Weigand, S.D.; Wiste, H.J.; Knopman, D.S.; Vemuri, P.; Lowe, V.J.; Mielke, M.M.; Roberts, R.O.; Machulda, M.M. Prevalence of Biologically vs Clinically Defined Alzheimer Spectrum Entities Using the National Institute on Aging–Alzheimer’s Association Research Framework. JAMA Neurol. 2019, 76, 1174–1183. [Google Scholar] [CrossRef] [Green Version]
- Davidson, M.; Beeri, M.S. Cost of Alzheimer’s Disease. Dialogues Clin. Neurosci. 2000, 2, 157–161. [Google Scholar] [CrossRef]
- El-Hayek, Y.H.; Wiley, R.E.; Khoury, C.P.; Daya, R.P.; Ballard, C.; Evans, A.R.; Karran, M.; Molinuevo, J.L.; Norton, M.; Atri, A. Tip of the Iceberg: Assessing the Global Socioeconomic Costs of Alzheimer’s Disease and Related Dementias and Strategic Implications for Stakeholders. J. Alzheimer’s Dis. 2019, 70, 323–341. [Google Scholar] [CrossRef] [PubMed]
- Wong, W. Economic Burden of Alzheimer Disease and Managed Care Considerations. Am. J. Manag. Care 2020, 26, S177–S183. [Google Scholar] [PubMed]
- Jeremic, D.; Jiménez-Díaz, L.; Navarro-López, J.D. Past, Present and Future of Therapeutic Strategies against Amyloid-β Peptides in Alzheimer’s Disease: A Systematic Review. Ageing Res. Rev. 2021, 72, 101496. [Google Scholar] [CrossRef] [PubMed]
- Plascencia-Villa, G.; Perry, G. Status and Future Directions of Clinical Trials in Alzheimer’s Disease. Int. Rev. Neurobiol. 2020, 154, 3–50. [Google Scholar]
- Oumata, N.; Lu, K.; Teng, Y.; Cavé, C.; Peng, Y.; Galons, H.; Roques, B.P. Molecular Mechanisms in Alzheimer’s Disease and Related Potential Treatments Such as Structural Target Convergence of Antibodies and Simple Organic Molecules. Eur. J. Med. Chem. 2022, 240, 114578. [Google Scholar] [CrossRef]
- Davies, K. Cognition Thinks It Has an Alzheimer’s Blockbuster. GEN Edge 2020, 2, 317–324. [Google Scholar] [CrossRef]
- Grundman, M.; Morgan, R.; Lickliter, J.D.; Schneider, L.S.; DeKosky, S.; Izzo, N.J.; Guttendorf, R.; Higgin, M.; Pribyl, J.; Mozzoni, K. A Phase 1 Clinical Trial of the Sigma-2 Receptor Complex Allosteric Antagonist CT1812, a Novel Therapeutic Candidate for Alzheimer’s Disease. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 20–26. [Google Scholar] [CrossRef]
- Izzo, N.J.; Staniszewski, A.; To, L.; Fa, M.; Teich, A.F.; Saeed, F.; Wostein, H.; Walko III, T.; Vaswani, A.; Wardius, M. Alzheimer’s Therapeutics Targeting Amyloid Beta 1–42 Oligomers I: Abeta 42 Oligomer Binding to Specific Neuronal Receptors Is Displaced by Drug Candidates That Improve Cognitive Deficits. PLoS ONE 2014, 9, e111898. [Google Scholar] [CrossRef]
- Izzo, N.J.; Xu, J.; Zeng, C.; Kirk, M.J.; Mozzoni, K.; Silky, C.; Rehak, C.; Yurko, R.; Look, G.; Rishton, G. Alzheimer’s Therapeutics Targeting Amyloid Beta 1–42 Oligomers II: Sigma-2/PGRMC1 Receptors Mediate Abeta 42 Oligomer Binding and Synaptotoxicity. PLoS ONE 2014, 9, e111899. [Google Scholar] [CrossRef]
- Doroszkiewicz, J.; Mroczko, B. New Possibilities in the Therapeutic Approach to Alzheimer’s Disease. Int. J. Mol. Sci. 2022, 23, 8902. [Google Scholar] [CrossRef]
- Hampel, H.; Vergallo, A.; Caraci, F.; Cuello, A.C.; Lemercier, P.; Vellas, B.; Giudici, K.V.; Baldacci, F.; Hänisch, B.; Haberkamp, M. Future Avenues for Alzheimer’s Disease Detection and Therapy: Liquid Biopsy, Intracellular Signaling Modulation, Systems Pharmacology Drug Discovery. Neuropharmacology 2021, 185, 108081. [Google Scholar] [CrossRef] [PubMed]
- Breijyeh, Z.; Karaman, R. Comprehensive Review on Alzheimer’s Disease: Causes and Treatment. Molecules 2020, 25, 5789. [Google Scholar] [CrossRef] [PubMed]
- Waybright, L.; Rehak, C.; Watto, E.; Caggiano, A.; Hamby, M.E. Unbiased Omics Analyses of the Sigma-2 Antagonist CT1812 in Age-Related Diseases and Models. Invest. Ophthalmol. Vis. Sci. 2021, 62, 267. [Google Scholar]
- Rishton, G.M.; Look, G.C.; Ni, Z.-J.; Zhang, J.; Wang, Y.; Huang, Y.; Wu, X.; Izzo, N.J.; LaBarbera, K.M.; Limegrover, C.S. Discovery of Investigational Drug CT1812, an Antagonist of the Sigma-2 Receptor Complex for Alzheimer’s Disease. ACS Med. Chem. Lett. 2021, 12, 1389–1395. [Google Scholar] [CrossRef] [PubMed]
- Maurice, T. Bi-Phasic Dose Response in the Preclinical and Clinical Developments of Sigma-1 Receptor Ligands for the Treatment of Neurodegenerative Disorders. Expert Opin. Drug Discov. 2021, 16, 373–389. [Google Scholar] [CrossRef]
- NIH, N.I. NIA-Funded Active Alzheimer’s and Related Dementias Clinical Trials and Studies|National Institute on Aging. Available online: https://www.nia.nih.gov/research/ongoing-AD-trials (accessed on 16 November 2022).
- Cognition Therapeutics Cognition Therapeutics Receives Fast Track Designation from U.S. FDA for First-in-Class Alzheimer’s Candidate, CT1812. Available online: https://cogrx.com/cognition-therapeutics-receives-fast-track-designation-from-u-s-fda-for-first-in-class-alzheimers-candidate-ct1812/ (accessed on 16 November 2022).
- Abate, C.; Niso, M.; Berardi, F. Sigma-2 Receptor: Past, Present and Perspectives on Multiple Therapeutic Exploitations. Future Med. Chem. 2018, 10, 1997–2018. [Google Scholar] [CrossRef]
- Izzo, N.J.; Yuede, C.M.; LaBarbera, K.M.; Limegrover, C.S.; Rehak, C.; Yurko, R.; Waybright, L.; Look, G.; Rishton, G.; Safferstein, H. Preclinical and Clinical Biomarker Studies of CT1812: A Novel Approach to Alzheimer’s Disease Modification. Alzheimer’s Dement. 2021, 17, 1365–1382. [Google Scholar] [CrossRef] [PubMed]
- Weller, J.; Budson, A. Current Understanding of Alzheimer’s Disease Diagnosis and Treatment. F1000Research 2018, 7, F1000. [Google Scholar] [CrossRef] [Green Version]
- Limegrover, C.S.; LeVine, H.; Izzo, N.J.; Yurko, R.; Mozzoni, K.; Rehak, C.; Sadlek, K.; Safferstein, H.; Catalano, S.M. Alzheimer’s Protection Effect of A673T Mutation May Be Driven by Lower Aβ Oligomer Binding Affinity. J. Neurochem. 2021, 157, 1316–1330. [Google Scholar] [CrossRef]
- Limegrover, C.S.; Yurko, R.; Izzo, N.J.; LaBarbera, K.M.; Rehak, C.; Look, G.; Rishton, G.; Safferstein, H.; Catalano, S.M. Sigma-2 Receptor Antagonists Rescue Neuronal Dysfunction Induced by Parkinson’s Patient Brain-Derived α-Synuclein. J. Neurosci. Res. 2021, 99, 1161–1176. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Cochrane RoB 2: A Revised Cochrane Risk-of-Bias Tool for Randomized Trials. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 7 August 2022).
- Therapeutics, C. Clinical Trial of CT1812 in Mild to Moderate Alzheimer’s Disease. Clin. gov Identifier NCT02907567, 2016. Available online: https://clinicaltrials.gov/ct2/show/NCT02907567 (accessed on 16 November 2022).
- Hamby Effect of CT1812 Treatment on Brain Synaptic Density. Available online: https://clinicaltrials.gov/ct2/show/NCT03493282 (accessed on 16 November 2022).
- Carson, R.E.; van Dyck, C.H.; Mecca, A.P.; Schneider, L.S.; Grundman, M.; DeKosky, S.T.; Morgan, R.; LaBarbera, K.; Hamby, M.E.; Izzo, N.J. A Pilot Study to Evaluate the Effect of CT1812 Treatment on Synaptic Density in Participants with Mild to Moderate Alzheimer’s Disease: FDG-PET, FMRI and Biomarker Outcomes. In Proceedings of the 2021 Alzheimer’s Association International Conference, Denver, CO, USA, 26–30 June 2021. [Google Scholar]
- ClinicalTrials.gov CT1812|Alzheimer Disease—ClinicalTrials.Gov. Available online: https://clinicaltrials.gov/ct2/results?term=CT1812&cond=Alzheimer+Disease&Search=Apply&age_v=&gndr=&type=&rslt= (accessed on 16 November 2022).
- Cognition Therapeutics Cognition Therapeutics Reports Drug-Drug Interaction Results for CT1812, a Disease-Modifying Alzheimer’s Disease Candidate. Available online: https://cogrx.com/cognition-therapeutics-reports-drug-drug-interaction-results-for-ct1812-a-disease-modifying-alzheimers-disease-candidate/ (accessed on 16 November 2022).
- Catalano, S.; Grundman, M.; Schneider, L.; DeKosky, S.; Morgan, R.; Higgin, M.; Pribyl, J.; Mozzoni, K.; Izzo, N.; Safferstein, H.; et al. P4-381: A Two-Part, Double-Blind, Placebo Controlled Phase 1 Study of the Safety and Pharmacokinetics of Single and Multiple Ascending Doses of CT1812 in Health Volunteers. Alzheimer’s Dement. 2016, 12, P1183–P1184. [Google Scholar] [CrossRef]
- Nygaard, H.B. Targeting Fyn Kinase in Alzheimer’s Disease. Biol. Psychiatry 2018, 83, 369–376. [Google Scholar] [CrossRef]
- Gong, C.-X.; Liu, F.; Iqbal, K. Multifactorial Hypothesis and Multi-Targets for Alzheimer’s Disease. J. Alzheimer’s Dis. 2018, 64, S107–S117. [Google Scholar] [CrossRef] [PubMed]
- Chasioti, D.; Yan, J.; Nho, K.; Saykin, A.J. Progress in Polygenic Composite Scores in Alzheimer’s and Other Complex Diseases. Trends Genet. 2019, 35, 371–382. [Google Scholar] [CrossRef]
- Iturria-Medina, Y.; Carbonell, F.M.; Sotero, R.C.; Chouinard-Decorte, F.; Evans, A.C.; Initiative, A.D.N. Multifactorial Causal Model of Brain (Dis) Organization and Therapeutic Intervention: Application to Alzheimer’s Disease. Neuroimage 2017, 152, 60–77. [Google Scholar] [CrossRef] [Green Version]
- Colom-Cadena, M.; Tulloch, J.; Jackson, R.J.; Catterson, J.H.; Rose, J.; Davies, C.; Hooley, M.; Anton-Fernandez, A.; Dunnett, S.; Tempelaar, R. TMEM97 Increases in Synapses and Is a Potential Synaptic Aβ Binding Partner in Human Alzheimer’s Disease. bioRxiv 2021. [Google Scholar] [CrossRef]
- Colom-Cadena, M.; Spires-Jones, T.; Zetterberg, H.; Blennow, K.; Caggiano, A.; DeKosky, S.T.; Fillit, H.; Harrison, J.E.; Schneider, L.S.; Scheltens, P. The Clinical Promise of Biomarkers of Synapse Damage or Loss in Alzheimer’s Disease. Alzheimers. Res. Ther. 2020, 12, 1–12. [Google Scholar] [CrossRef]
- Sabino, V.; Cottone, P.; Parylak, S.L.; Steardo, L.; Zorrilla, E.P. Sigma-1 Receptor Knockout Mice Display a Depressive-like Phenotype. Behav. Brain Res. 2009, 198, 472–476. [Google Scholar] [CrossRef] [Green Version]
- Maurice, T. Beneficial Effect of the Σ1 Receptor Agonist PRE-084 against the Spatial Learning Deficits in Aged Rats. Eur. J. Pharmacol. 2001, 431, 223–227. [Google Scholar] [CrossRef]
- Fehér, Á.; Juhász, A.; László, A.; Kálmán Jr, J.; Pákáski, M.; Kálmán, J.; Janka, Z. Association between a Variant of the Sigma-1 Receptor Gene and Alzheimer’s Disease. Neurosci. Lett. 2012, 517, 136–139. [Google Scholar] [CrossRef]
- Jia, H.; Zhang, Y.; Huang, Y. Imaging Sigma Receptors in the Brain: New Opportunities for Diagnosis of Alzheimer’s Disease and Therapeutic Development. Neurosci. Lett. 2019, 691, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Van Giau, V.; Bagyinszky, E.; Youn, Y.C.; An, S.S.A.; Kim, S. APP, PSEN1, and PSEN2 Mutations in Asian Patients with Early-Onset Alzheimer Disease. Int. J. Mol. Sci. 2019, 20, 4757. [Google Scholar] [CrossRef] [PubMed]
- Reitz, C.; Rogaeva, E.; Beecham, G.W. Late-Onset vs Nonmendelian Early-Onset Alzheimer Disease: A Distinction without a Difference? Neurol. Genet. 2020, 6, e512. [Google Scholar] [CrossRef] [PubMed]
- Van Giau, V.; Senanarong, V.; Bagyinszky, E.; An, S.S.A.; Kim, S. Analysis of 50 Neurodegenerative Genes in Clinically Diagnosed Early-Onset Alzheimer’s Disease. Int. J. Mol. Sci. 2019, 20, 1514. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Trial ID | Author | Year | Country | Title | Journal | Phase | Design | Inclusion Criteria | Pharmacologic Intervention | Outcome Measures |
|---|---|---|---|---|---|---|---|---|---|---|
| NCT02907567 [35] | Izzo et al. | 2021 | Australia | Preclinical and clinical biomarker studies of CT1812: A novel approach to Alzheimer’s disease modification | Alzheimer’s and Dementia | Phase Ib/IIa | Randomized, double-blind, placebo-controlled | Men and women aged 50–80 with mild to moderate AD as per the 2011 NIA-AA criteria, with MRI diagnosis, MMSE (18–26), without active depression, and a GDS < 6 | Two doses of CT1812 in adults with mild to moderate AD for 28 days compared to a placebo | Treatment-emergent adverse events (physical exams; monitoring of vital signs, ECGs, and clinical and laboratory assessments) |
| NCT03493282 [36] | Hamby | 2020 | USA | A Pilot Synaptic Vesicle Glycoprotein 2A (SV2A) PET Study to Evaluate the Effect of CT1812 Treatment on Synaptic Density in Participants With Mild to Moderate Alzheimer’s Disease | Alzheimer’s Association International Conference | Phase I/II | Single-center, randomized, double-blind, placebo-controlled, parallel-group study | Men and women aged 50–85 years diagnosed with mild-to-moderate AD as per the 2011 NIA-AA criteria and with 6-month cognitive decline, MMSE (18–26), and with positive amyloid scan | CT1812 300 mg or 100 mg orally compared to placebo for up to 180 days | Number of participants with treatment-related adverse events and serious adverse events over 30 weeks; and changes in brain synaptic density over six months using the SV2A PET ligand 11C-UCB-J |
| NCT02570997 and NCT03716427 [17,37] | Grundman et al. | 2019 | USA | A phase 1 clinical trial of the sigma-2 receptor complex allosteric antagonist CT1812, a novel therapeutic candidate for Alzheimer’s disease | Alzheimer’s and Dementia: Translational Research and Clinical Interventions | Phase I | A two-part, randomized, double-blind, placebo-controlled study | Men and women aged between 18–55, or 65–75 years in good health with BMI (19–34 km/m2), normal ECG and blood pressure, and non-smokers | Part A: Healthy young subjects with one dose of CT1812 at 10 mg, increased to 30, 90, 180, 450, and 1120 mg across six cohorts; the seventh cohort received a single 90 mg dosage; all dosages were given over 3 days Part B: Healthy young subjects with the same dose once daily for 14 days at 280 mg, followed by 560 and 840 mg in three cohorts; the fourth cohort had healthy elderly subjects aged 65 or above and received 560 mg compared to a placebo daily for two weeks | Safety and tolerability; and plasma pharmacokinetics in parts A (single ascending dose-SAD/food-effect study) and B (multiple ascending dose-MAD) |
| Author, Year | Sample Size | Age (Years) | Gender | Efficacy | Safety |
|---|---|---|---|---|---|
| Izzo et al., 2021 [29] | 19 | 70.2 years (SD = 9.2) | 9 F, 10 M | Day 28: Amyloid beta(Aβ) oligomers’ concentration measured via Western blot analysis in CT1812-treated AD patient CSF increases compared to the patient baseline and vs. placebo (p = 0.014, t-test, n = 3 placebo, 10 CT1812-treated), provided supporting evidence of clinical target engagement; synaptic damage proteins neurogranin B concentration measured via ELISA and synaptotagmin-1 C measured by LC-MS/MS decreased compared to the patient baseline and vs. placebo (p = 0.05 covariance, placebo = 5, CT1812 = 11 and p = 0.011, placebo = 4, CT1812 = 9), respectively | No adverse events concerning the safety of participants were reported |
| Hamby, 2020 [36] | 23 | 70 years (SD = 8.8) | 11 F, 12 M | Until day 180: the distribution volume ratio (DVR) mean (SE) change from baseline in 300 mg, 100 mg, and placebo groups was −0.043 (0.02), −0.019 (0.02), and 0 (0.02), respectively. Aβ 40 (pg/mL) mean change (SE) over 6 months for 300 mg, 100 mg, and placebo groups were −594 (381.57), 517.7 (445.24), and 222.25 (397.27), respectively. In comparison, for Tau (pg/mL), the 6-month mean (SE) score outcomes were −84.08 (111.96), 121.22 (131.96), and 36.74 (120.7), respectively. Concerning change from the baseline in the cognitive composite (6 ASAS-COG items and 4 NTB items), the 300 mg, 100 mg, and placebo groups had mean (SE) score changes of −0.33 (0.109), −0.11 (0.102) and −0.1 (0.109), respectively. The mean change (SE) for MMSE outcomes in 300 mg, 100 mg, and placebo groups were −2.92 (1.54), −1.26 (1.45), and −0.74 (1.55), respectively. | With high-dose CT1812 (300 mg), mild treatment-emergent adverse events (TEAE) were observed in 85.7% of patients, whereas 4/8 of low-dose (100 mg) patients (50%) reported mild TEAE; with placebo, 4/6 (66.7%) reported mild TEAE; discontinuation was somewhat comparable in both CT1812 (4/15; 26.7%) and placebo (1/6; 16.7%) groups |
| Grundman et al., 2019 [17] | 93; SAD = 54, MAD = 39 | SAD Phase: median = 26 years (IQR = 19–55); MAD Phase: young cohort = 28.5 years (IQR = 19–600, elderly cohort = 69 years (IQR = 64–73) | SAD: 16 F, 38 M MAD: 11 F, 28 M | Day 14: CT1812 concentrations in the CSF increased in a dose-dependent manner across two orders of magnitude over two weeks; for 560–840 mg, the average CSF concentrations were at 97–98% receptor occupancy; cognitive scores were similar across the elderly cohort before and after treatment | Treatment-emergent adverse events were reported for 18/42 patients (43%) after single-dose administration of CT1812 and 2/12 patients (17%) after placebo. No deaths or other serious adverse events were reported |
| No. | NCT Number | Title | Status | Conditions | Interventions | Outcome Measures | Participants | Phases | Enrollment | Study Type | Study Designs | Other IDs | Primary Completion Date | Locations |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | NCT05531656 | A Study to Evaluate the Safety and Efficacy of CT1812 in Early Alzheimer’s Disease | Not yet recruiting | Early Alzheimer’s Disease | CT1812 vs. Placebo | Change from baseline in CDR-SB scale; ADAS-Cog 13; ADCS-ADL; CSF concentrations; Plasma measures of changes; Volumetric MRI including hippocampal and whole brain volume change | M/F, 50–85 years | Phase II | 540 | Interventional | Randomized, Parallel Assignment, Quadruple (Participant, Care Provider, Investigator, Outcomes Assessor) Marking, Curative | COG0203 | Aug-26 | NA |
| 2 | NCT04735536 | Pilot Clinical Study of CT1812 in Mild to Moderate Alzheimer’s Disease Using EEG | Recruiting | Alzheimer Disease | CT1812 vs. Placebo | Measurement of CT1812 plasma concentration ratio | M/F, 50–85 years | Phase II | 16 | Interventional | Randomized, Crossover Assignment, Quadruple (Participant, Care Provider, Investigator, Outcomes Assessor) Masking, Curative | COG0202 | 30-Mar-23 | Amsterdam, Netherlands |
| 3 | NCT03507790 | A Study to Evaluate the Safety and Efficacy of CT1812 in Subjects With Mild to Moderate Alzheimer’s Disease. | Recruiting | Mild to Moderate Alzheimer’s Disease | CT1812 vs. Placebo | Number of study participants with treatment-related adverse events and serious adverse events | M/F, 50–85 years | Phase II | 144 | Interventional | Randomized, Parallel Assignment, Quadruple (Participant, Care Provider, Investigator, Outcomes Assessor) Making, Curative | COG0201 | 24-Sep-23 | United States and Australia |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rasheed, A.; Zaheer, A.B.; Munawwar, A.; Sarfraz, Z.; Sarfraz, A.; Robles-Velasco, K.; Cherrez-Ojeda, I. The Allosteric Antagonist of the Sigma-2 Receptors—Elayta (CT1812) as a Therapeutic Candidate for Mild to Moderate Alzheimer’s Disease: A Scoping Systematic Review. Life 2023, 13, 1. https://doi.org/10.3390/life13010001
Rasheed A, Zaheer AB, Munawwar A, Sarfraz Z, Sarfraz A, Robles-Velasco K, Cherrez-Ojeda I. The Allosteric Antagonist of the Sigma-2 Receptors—Elayta (CT1812) as a Therapeutic Candidate for Mild to Moderate Alzheimer’s Disease: A Scoping Systematic Review. Life. 2023; 13(1):1. https://doi.org/10.3390/life13010001
Chicago/Turabian StyleRasheed, Anum, Ahmad Bin Zaheer, Aqsa Munawwar, Zouina Sarfraz, Azza Sarfraz, Karla Robles-Velasco, and Ivan Cherrez-Ojeda. 2023. "The Allosteric Antagonist of the Sigma-2 Receptors—Elayta (CT1812) as a Therapeutic Candidate for Mild to Moderate Alzheimer’s Disease: A Scoping Systematic Review" Life 13, no. 1: 1. https://doi.org/10.3390/life13010001