

Identification of Suitable Drug Combinations for Treating COVID-19 Using a Novel Machine Learning Approach: The RAIN Method

 , and
, and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Stage I: Systematic Review
2.2. Research Question and Keyword Determination according to PICO Instructions
2.3. Searching Articles
2.4. Identifying Articles
2.5. Study Selections, Based on Inclusion and Exclusion Criteria
2.6. Inclusion and Exclusion Criteria according to the Research Question
2.7. Quality Evaluation of Studies
2.8. Data Extraction
2.9. Stage 2: Artificial Intelligence
2.10. Combining p-Values
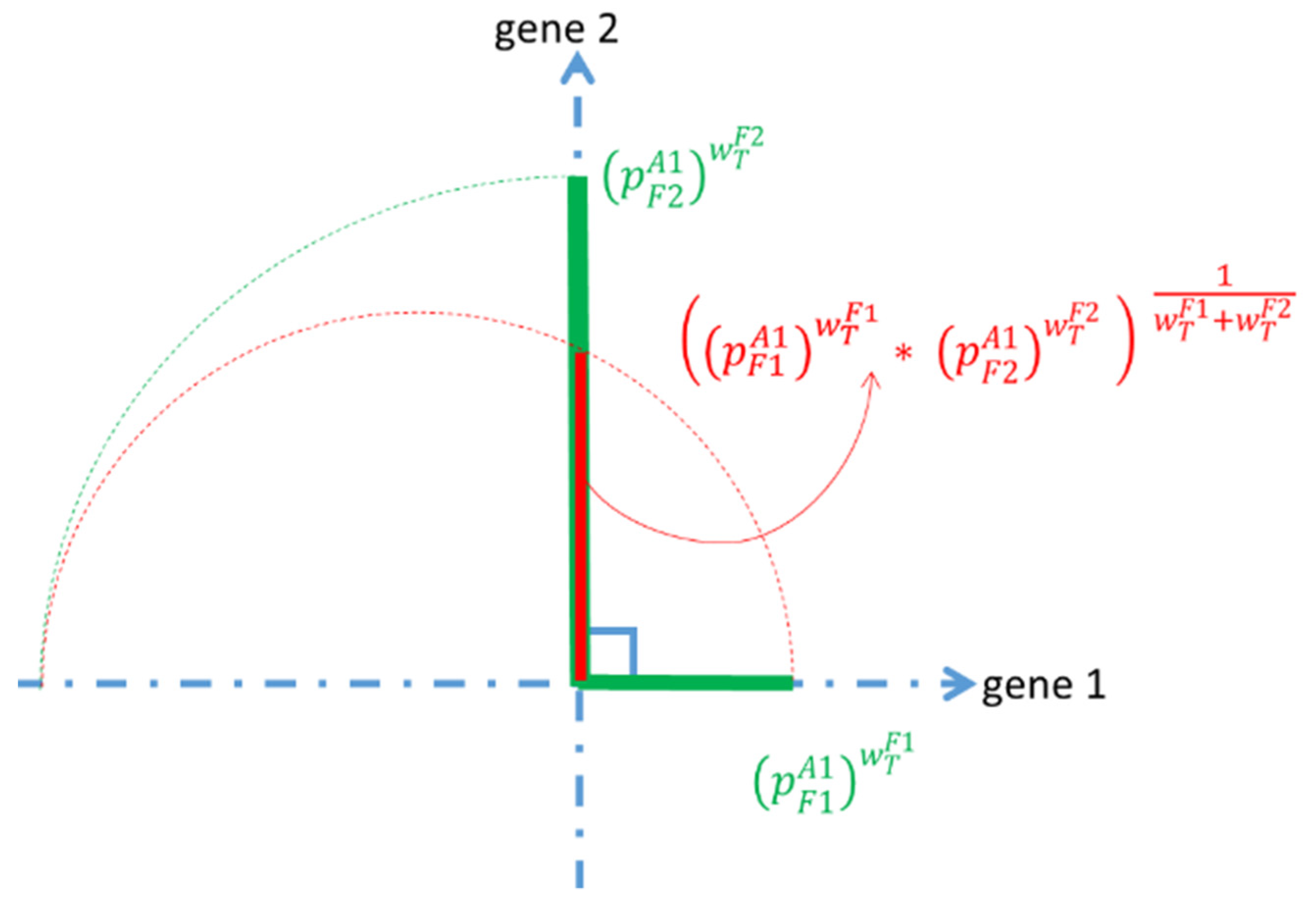
2.11. Using the Formula
2.12. Power Means
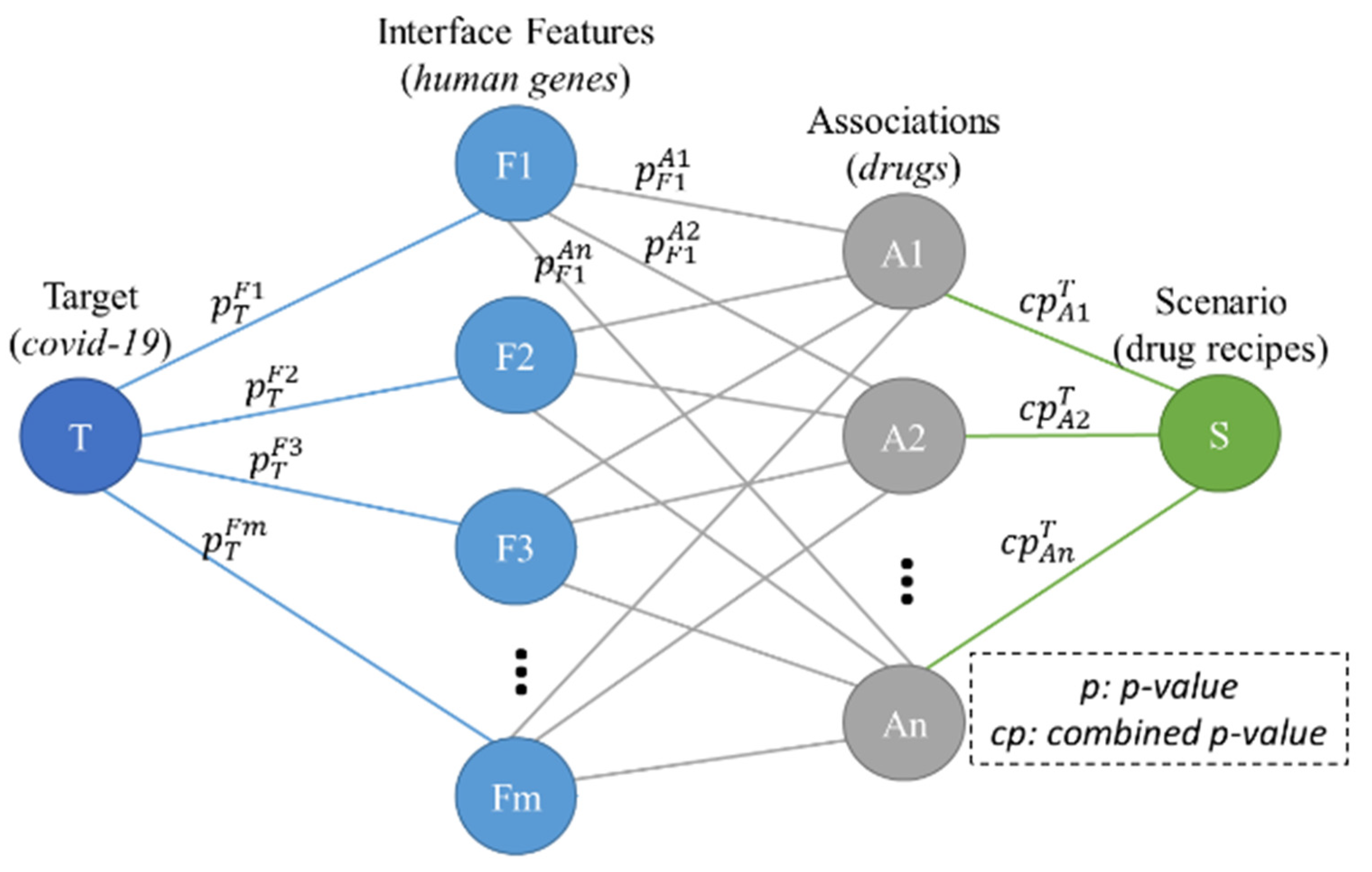
2.13. The Proposed AI Models
2.14. The Forward Step
2.15. The Backward Step
3. Results
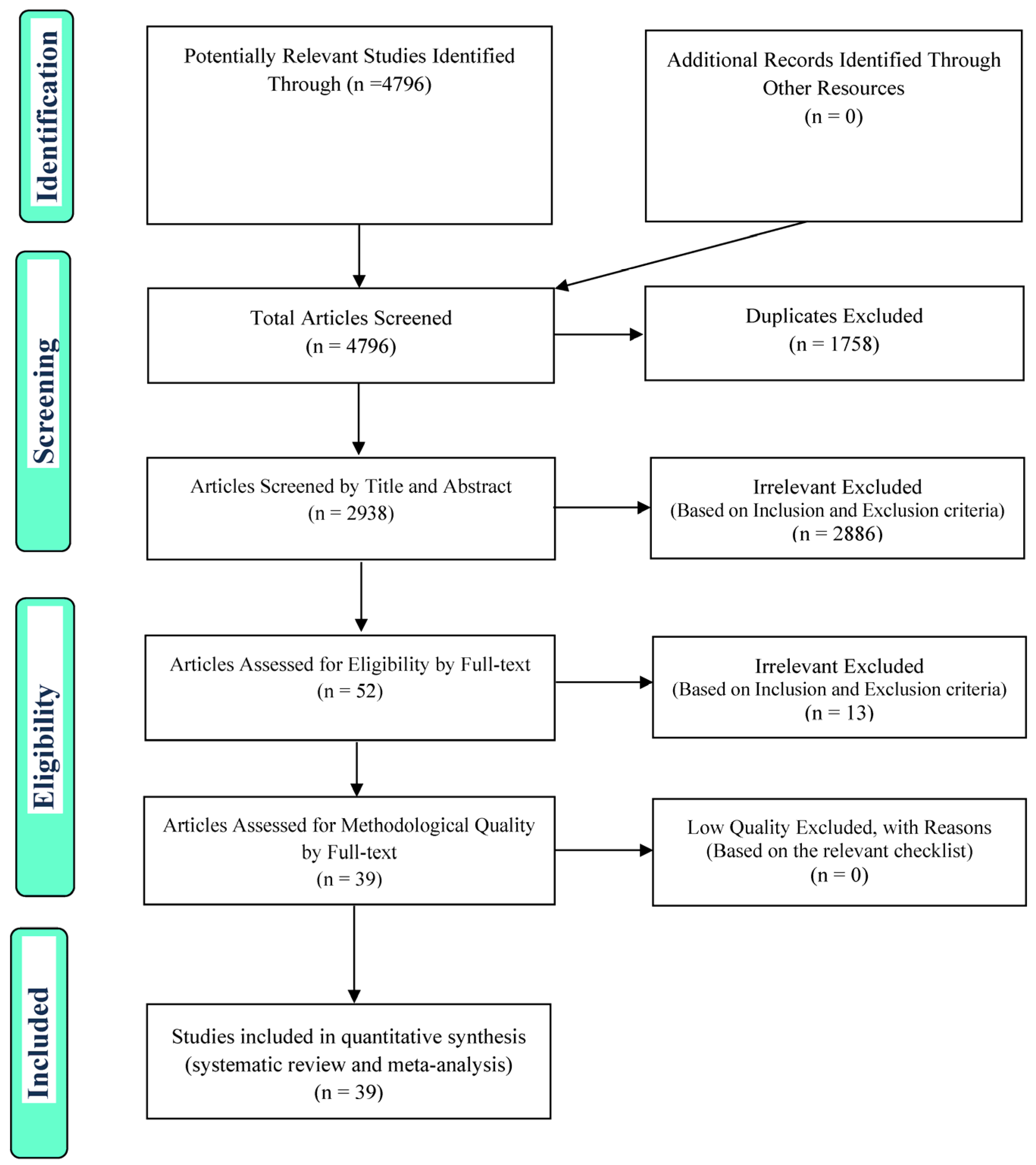
3.1. Systematic Review
3.2. Artificial Intelligence
- -
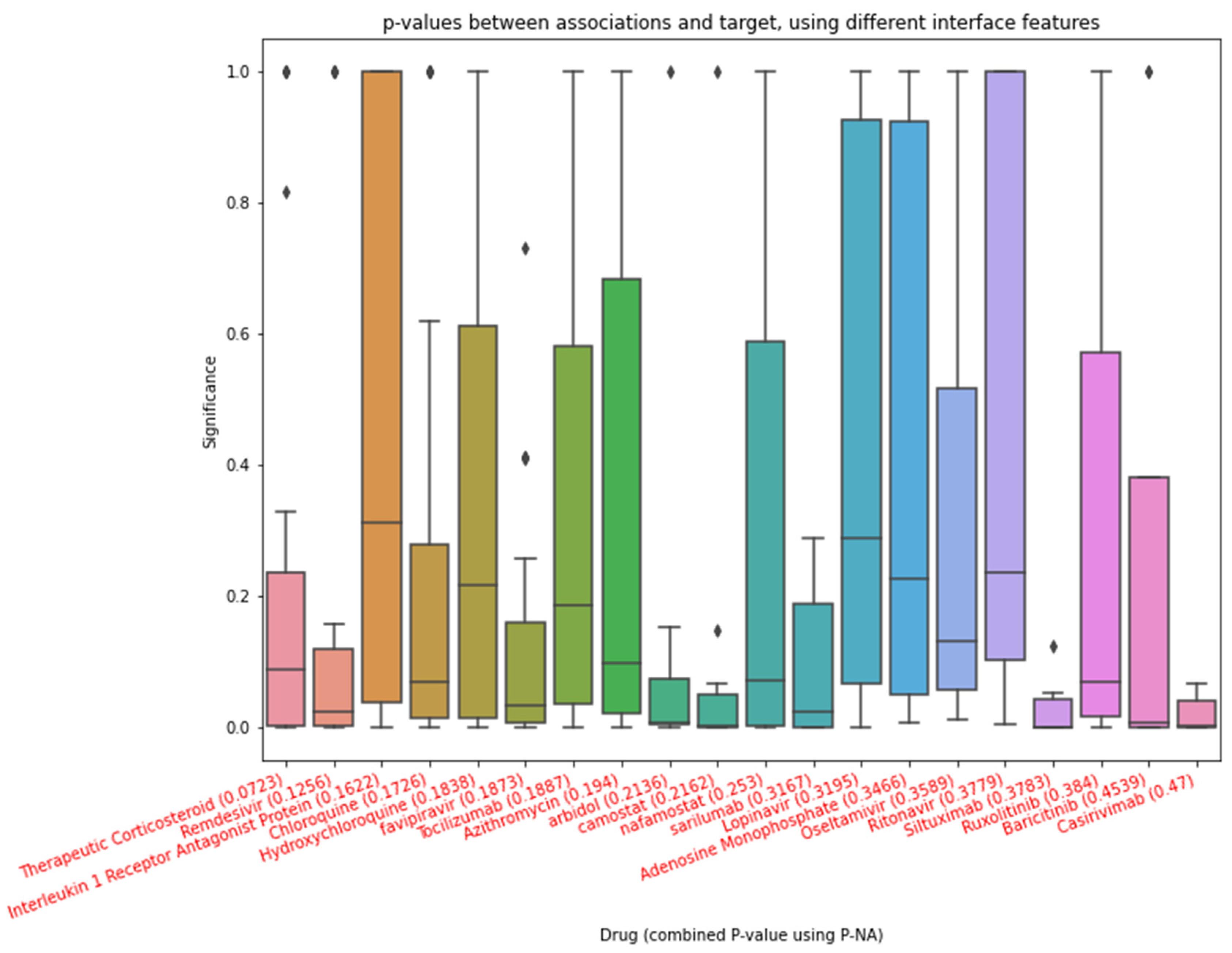
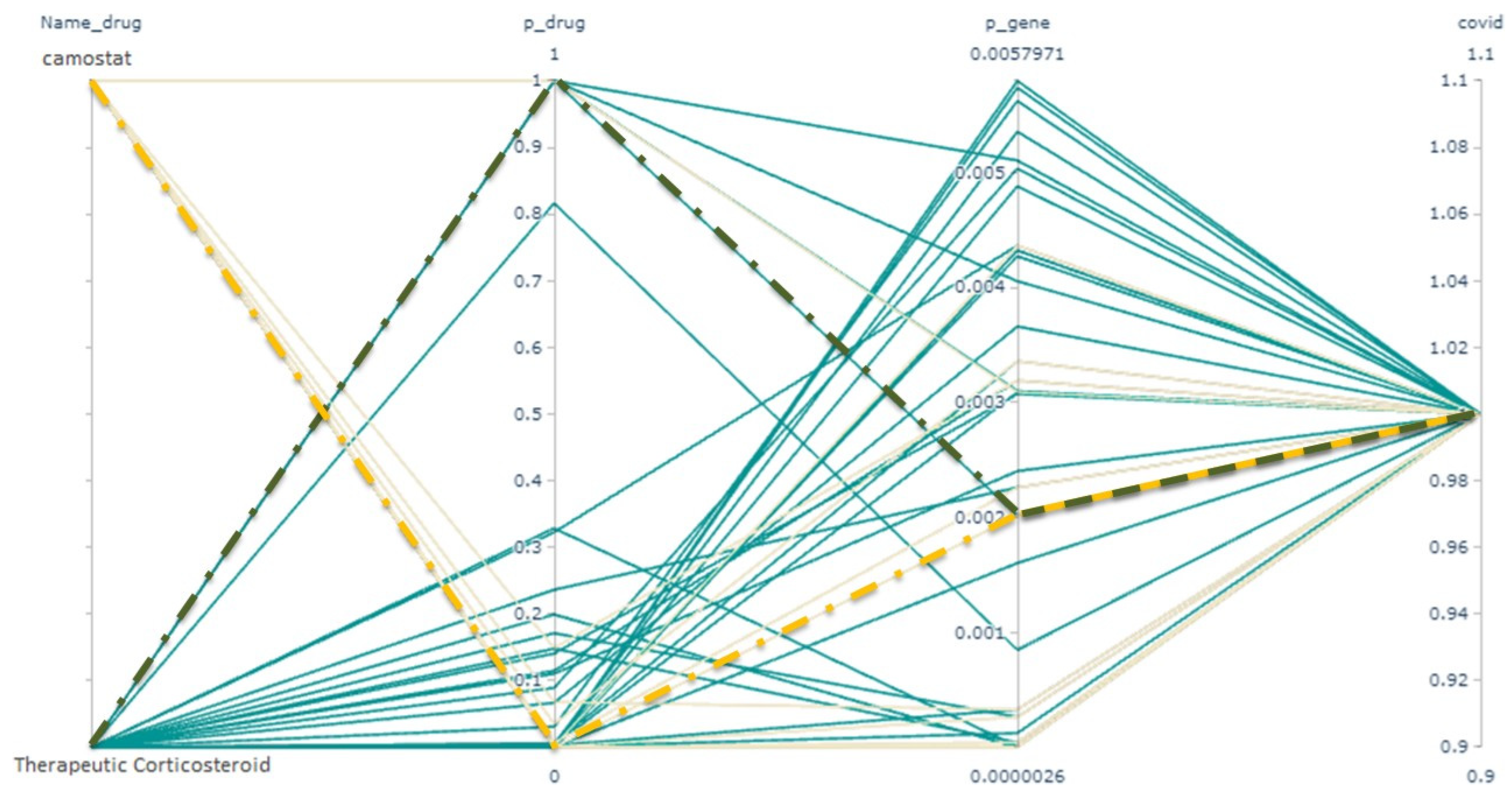
- Therapeutic corticosteroid with a combined p-value of 0.07;
- -
- Camostat with a combined p-value of 0.02, on the condition that the therapeutic corticosteroid is selected in this scenario.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ‘Therapeutic Corticosteroid’ (0.07234703) + ‘Camostat’ (0.024973529) |
| ‘Remdesivir’(0.125641) + ‘Azithromycin’ (0.032386) |
| ‘Interleukin 1 Receptor Antagonist Protein’ (0.162201) + ‘Camostat’ (0.026755) |
| ‘Chloroquine’ (0.172638) + ‘Favipiravir’ (0.083871) + ‘Camostat’ (0.046428) |
| ‘Hydroxychloroquine’ (0.183845) + ‘Azithromycin’ (0.07669) + ‘Camostat’ (0.044154) |
| ‘Interleukin 1 Receptor Antagonist Protein’ (0.162201) + ‘Camostat’ (0.026755) + ‘Azithromycin’ (0.010872) + ‘Tocilizumab’ (0.008609) + ‘Oseltamivir’ (0.006937) |
| ‘Interleukin 1 Receptor Antagonist Protein’(0.162201) + ’Camostat’(0.026755) + ’Chloroquine’(0.014835) + ’Favipiravir’ (0.00952)+ ’Tocilizumab’(0.007638) |
| ‘Therapeutic Corticosteroid’ (0.07234703) + ‘Camostat’ (0.024973529) + ‘Oseltamivir’ (0.017227) + ‘Remdesivir’ (0.011593) + ‘Tocilizumab’(0.009214) |
4. Discussion
4.1. Advantages of WGM in Combining p-Values
4.2. Drawbacks of the p-NA
4.3. Alternatives for Associations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Ghasemi, H.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Khaledi-Paveh, B.; Hosseinian-Far, M. The prevalence of sleep disturbances among physicians and nurses facing the COVID-19 patients: A systematic review and meta-analysis. Glob. Health 2020, 16, 92. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Khan, H.; Khan, S.; Nawaz, M. Epidemiological and clinical characteristics of coronavirus disease (COVID-19) cases at a screening clinic during the early outbreak period: A single-centre study. J. Med. Microbiol. 2020, 69, 1114–1123. [Google Scholar] [CrossRef] [PubMed]
- Ivashchenko, A.A.; Dmitriev, K.A.; Vostokova, N.V.; Azarova, V.N.; Blinow, A.A.; Egorova, A.N.; Gordeev, I.G.; Ilin, A.P.; Karapetian, R.N.; Kravchenko, D.V.; et al. AVIFAVIR for Treatment of Patients with Moderate Coronavirus Disease 2019 (COVID-19): Interim Results of a Phase II/III Multicenter Randomized Clinical Trial. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Luo, F.; Liu, C.; Xiong, N.; Xu, Z.; Zhang, W.; Yang, M.; Wang, Y.; Liu, D.; Yu, C.; et al. Effect of a genetically engineered interferon-alpha versus traditional interferon-alpha in the treatment of moderate-to-severe COVID-19: A randomised clinical trial. Ann. Med. 2021, 53, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Pessoa-Amorim, G.; Mafham, M.M. The RECOVERY trial: Cardiovascular implications of a large, simple randomized trial in COVID-19. Cardiovasc. Res. 2021, 117, e110–e113. [Google Scholar] [CrossRef]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L. COVID-19 and cardiovascular disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef]
- Fitsiori, A.; Pugin, D.; Thieffry, C.; Lalive, P.; Vargas, M.I. COVID-19 is Associated with an Unusual Pattern of Brain Microbleeds in Critically Ill Patients. J. Neuroimaging 2020, 30, 593–597. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S.; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef]
- Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Izcovich, A.; Kum, E.; Pardo-Hernandez, H.; Qasim, A.; Martinez, J.P.D.; Rochwerg, B. Drug treatments for COVID-19: Living systematic review and network meta-analysis. BMJ 2020, 370, m2980. [Google Scholar] [CrossRef]
- Alimadadi, A.; Aryal, S.; Manandhar, I.; Munroe, P.B.; Joe, B.; Cheng, X. Artificial intelligence and machine learning to fight COVID-19. Physiol. Genom. 2020, 52, 200–202. [Google Scholar] [CrossRef] [PubMed]
- Syeda, H.B.; Syed, M.; Sexton, K.W.; Syed, S.; Begum, S.; Syed, F.; Prior, F.; Yu, F., Jr. Role of Machine Learning Techniques to Tackle the COVID-19 Crisis: Systematic Review. JMIR Med. Inform. 2021, 9, e23811. [Google Scholar] [CrossRef]
- Vaishya, R.; Javaid, M.; Khan, I.H.; Haleem, A. Artificial Intelligence (AI) applications for COVID-19 pandemic. Diabetes Metab. Syndr. 2020, 14, 337–339. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Dai, H.; Damiani, G.; Behzadifar, M.; Martini, M.; Wu, J. How Big Data and Artificial Intelligence Can Help Better Manage the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 3176. [Google Scholar] [CrossRef]
- De Crescenzo, F.; Amato, L.; Cruciani, F.; Moynihan, L.P.; D’Alò, G.L.; Vecchi, S.; Saulle, R.; Mitrova, Z.; Di Franco, V.; Addis, A.; et al. Comparative Effectiveness of Pharmacological Interventions for COVID-19: A Systematic Review and Network Meta-Analysis. Front. Pharmacol. 2021, 12, 649472. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Shan, J.; Gong, Z.; Kuang, J.; Gao, Y. Comparative effectiveness and safety of antiviral agents for patients with COVID-19: Protocol for a systematic review and individual-patient data network meta-analysis. PLoS ONE 2020, 15, e0241947. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.-L.; Wang, Y.-M.; Wu, Z.-Q.; Xiang, Z.-C.; Guo, L.; Xu, T.; Jiang, Y.-Z.; Xiong, Y.; Li, Y.-J.; Li, X.-W. Identification of a novel coronavirus causing severe pneumonia in human: A descriptive study. Chin. Med. J. 2020, 133, 1015. [Google Scholar] [CrossRef]
- Sun, J.; He, W.-T.; Wang, L.; Lai, A.; Ji, X.; Zhai, X.; Li, G.; Suchard, M.A.; Tian, J.; Zhou, J. COVID-19: Epidemiology, evolution, and cross-disciplinary perspectives. Trends Mol. Med. 2020, 26, 483–495. [Google Scholar] [CrossRef]
- Ogunrinola, O.O.; Kanmodi, R.I.; Ogunrinola, O.A. Medicinal plants as immune booster in the palliative management of viral diseases: A perspective on coronavirus. Food Front. 2021, 3, 83–95. [Google Scholar] [CrossRef]
- Fisher, R.A. Statistical Methods for Research Workers. Biological Monographs and Manuals. No. V., 11th ed.; Oliver and Boyd: London, UK, 1950. [Google Scholar]
- Lipták, T. On the combination of independent tests. Magyar Tud. Akad. Mat. Kutató Int. Közl. 1958, 3, 171–197. [Google Scholar]
- Zaykin, D.V. Optimally weighted Z-test is a powerful method for combining probabilities in meta-analysis. J. Evol. Biol. 2011, 24, 1836–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Won, S.; Morris, N.; Lu, Q.; Elston, R.C. Choosing an optimal method to combine p-values. Stat. Med. 2009, 28, 1537–1553. [Google Scholar] [CrossRef] [PubMed]
- Saxton, M.J. Diffusion of DNA-binding species in the nucleus: A transient anomalous subdiffusion model. Biophys. J. 2020, 118, 2151–2167. [Google Scholar] [CrossRef]
- Stebbing, J.; Phelan, A.; Griffin, I.; Tucker, C.; Oechsle, O.; Smith, D.; Richardson, P. COVID-19: Combining antiviral and anti-inflammatory treatments. Lancet Infect. Dis. 2020, 20, 400–402. [Google Scholar] [CrossRef]
- Favalli, E.G.; Biggioggero, M.; Maioli, G.; Caporali, R. Baricitinib for COVID-19: A suitable treatment? Lancet Infect. Dis. 2020, 20, 1012–1013. [Google Scholar] [CrossRef]
- Abella, B.S.; Jolkovsky, E.L.; Biney, B.T.; Uspal, J.E.; Hyman, M.C.; Frank, I.; Hensley, S.E.; Gill, S.; Vogl, D.T.; Maillard, I.; et al. Efficacy and Safety of Hydroxychloroquine vs Placebo for Pre-exposure SARS-CoV-2 Prophylaxis among Health Care Workers: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 195–202. [Google Scholar] [CrossRef]
- Barnabas, R.V.; Brown, E.R.; Bershteyn, A.; Stankiewicz Karita, H.C.; Johnston, C.; Thorpe, L.E.; Kottkamp, A.; Neuzil, K.M.; Laufer, M.K.; Deming, M.; et al. Hydroxychloroquine as Postexposure Prophylaxis to Prevent Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Randomized Trial. Ann. Intern. Med. 2021, 174, 344–352. [Google Scholar] [CrossRef]
- Boulware, D.R.; Pullen, M.F.; Bangdiwala, A.S.; Pastick, K.A.; Lofgren, S.M.; Okafor, E.C.; Skipper, C.P.; Nascene, A.A.; Nicol, M.R.; Abassi, M.; et al. A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for COVID-19. N. Engl. J. Med. 2020, 383, 517–525. [Google Scholar] [CrossRef]
- Brown, S.M.; Peltan, I.; Kumar, N.; Leither, L.; Webb, B.J.; Starr, N.; Grissom, C.K.; Buckel, W.R.; Srivastava, R.; Butler, A.M.; et al. Hydroxychloroquine versus azithromycin for hospitalized patients with COVID-19: Results of a randomized, active comparator trial. Ann. Am. Thorac. Soc. 2021, 18, 590–597. [Google Scholar] [CrossRef]
- Garibaldi, B.T.; Wang, K.; Robinson, M.L.; Zeger, S.L.; Bandeen-Roche, K.; Wang, M.C.; Alexander, G.C.; Gupta, A.; Bollinger, R.; Xu, Y. Comparison of Time to Clinical Improvement with vs without Remdesivir Treatment in Hospitalized Patients with COVID-19. JAMA Netw. Open 2021, 4, e213071. [Google Scholar] [CrossRef]
- Langer-Gould, A.; Smith, J.B.; Gonzales, E.G.; Castillo, R.D.; Figueroa, J.G.; Ramanathan, A.; Li, B.H.; Gould, M.K. Early identification of COVID-19 cytokine storm and treatment with anakinra or tocilizumab. Int. J. Infect. Dis. 2020, 99, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, H.; Davoudi-Monfared, E.; Nourian, A.; Khalili, H.; Hajizadeh, N.; Jalalabadi, N.Z.; Fazeli, M.R.; Ghazaeian, M.; Yekaninejad, M.S. Interferon β-1b in treatment of severe COVID-19: A randomized clinical trial. Int. Immunopharmacol. 2020, 88, 106903. [Google Scholar] [CrossRef] [PubMed]
- Satlin, M.J.; Goyal, P.; Magleby, R.; Maldarelli, G.A.; Pham, K.; Kondo, M.; Schenc, E.J.; Rennert, H.; Westblad, L.F.; Cho, J.J.; et al. Safety, tolerability, and clinical outcomes of hydroxychloroquine for hospitalized patients with coronavirus 2019 disease. PLoS ONE 2020, 15, e0236778. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Semler, M.W.; Leither, L.M.; Casey, J.D.; Angus, D.C.; Brower, R.G.; Chang, S.Y.; Collins, S.P.; Eppensteiner, J.C.; Filbin, M.R.; et al. Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients with COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 2165–2176. [Google Scholar] [CrossRef]
- Skipper, C.P.; Pastick, K.A.; Engen, N.W.; Bangdiwala, A.S.; Abassi, M.; Lofgren, S.M.; Williams, D.A.; Okafor, E.C.; Pullen, M.F.; Nicol, M.R.; et al. Hydroxychloroquine in Nonhospitalized Adults with Early COVID-19: A Randomized Trial. Ann. Intern. Med. 2020, 173, 623–631. [Google Scholar] [CrossRef]
- Ulrich, R.J.; Troxel, A.B.; Carmody, E.; Eapen, J.; Bäcker, M.; DeHovitz, J.A.; Prasad, P.J.; Li, Y.; Delgado, C.; Jrada, M.; et al. Treating COVID-19 with hydroxychloroquine (TEACH): A multicenter, double-blind randomized controlled trial in hospitalized patients. In Open Forum Infectious Diseases; Oxford University Press: Cary, NC, USA, 2020; p. 7. [Google Scholar]
- Ansarin, K.; Tolouian, R.; Ardalan, M.; Taghizadieh, A.; Varshochi, M.; Teimouri, S.; Vaezi, T.; Valizadeh, H.; Saleh, P.; Safiri, S.; et al. Effect of bromhexine on clinical outcomes and mortality in COVID-19 patients: A randomized clinical trial. BioImpacts 2020, 10, 209–215. [Google Scholar] [CrossRef]
- Davoudi-Monfared, E.; Rahmani, H.; Khalili, H.; Hajiabdolbaghi, M.; Salehi, M.; Abbasian, L.; Kazemzadeh, H.; Yekaninejad, M.S. A randomized clinical trial of the efficacy and safety of interferon β-1a in treatment of severe COVID-19. Antimicrob. Agents Chemother. 2020, 64, e01061-20. [Google Scholar] [CrossRef]
- Eslami, G.; Mousaviasl, S.; Radmanesh, E.; Jelvay, S.; Bitaraf, S.; Simmons, B.; Wentzel, H.; Hill, A.; Sadeghi, A.; Freeman, J.; et al. The impact of sofosbuvir/daclatasvir or ribavirin in patients with severe COVID-19. J. Antimicrob. Chemother. 2020, 75, 3366–3372. [Google Scholar] [CrossRef]
- Kasgari, H.A.; Moradi, S.; Shabani, A.M.; Babamahmoodi, F.; Davoudi Badabi, A.R.; Davoudi, L.; Alikhani, A.; Omran, A.H.; Saeedi, M.; Merat, S.; et al. Evaluation of the efficacy of sofosbuvir plus daclatasvir in combination with ribavirin for hospitalized COVID-19 patients with moderate disease compared with standard care: A single-centre, randomized controlled trial. J. Antimicrob. Chemother. 2020, 75, 3373–3378. [Google Scholar] [CrossRef]
- Nojomi, M.; Yassin, Z.; Keyvani, H.; Makiani, M.J.; Roham, M.; Laali, A.; Dehghan, N.; Navaei, M.; Ranjbar, M. Effect of Arbidol (Umifenovir) on COVID-19: A randomized controlled trial. BMC Infect. Dis. 2020, 20, 954. [Google Scholar] [CrossRef]
- Roozbeh, F.; Saeedi, M.; Alizadeh-Navaei, R.; Hedayatizadeh-Omran, A.; Merat, S.; Wentzel, H.; Levi, J.; Hill, A.; Shamshirian, A. Sofosbuvir and daclatasvir for the treatment of COVID-19 outpatients: A double-blind, randomized controlled trial. J. Antimicrob. Chemother. 2021, 76, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, A.; Asgari, A.A.; Norouzi, A.; Kheiri, Z.; Anushirvani, A.; Montazeri, M.; Hosamirudsai, H.; Afhami, S.; Akbarpour, E.; Aliannejad, R.; et al. Sofosbuvir and daclatasvir compared with standard of care in the treatment of patients admitted to hospital with moderate or severe coronavirus infection (COVID-19): A randomized controlled trial. J. Antimicrob. Chemother. 2020, 75, 3379–3385. [Google Scholar] [CrossRef] [PubMed]
- Sekhavati, E.; Jafari, F.; SeyedAlinaghi, S.; Jamalimoghadamsiahkali, S.; Sadr, S.; Tabarestani, M.; Pirhayati, M.; Zendehdel, A.; Manafi, N.; Hajiabdolbaghi, M.; et al. Safety and effectiveness of azithromycin in patients with COVID-19: An open-label randomised trial. Int. J. Antimicrob. Agents 2020, 56, 106143. [Google Scholar] [CrossRef] [PubMed]
- Ayerbe, L.; Risco, C.; Ayis, S. The association between treatment with heparin and survival in patients with COVID-19. J. Thromb. Thrombolysis 2020, 50, 298–301. [Google Scholar] [CrossRef]
- Ayerbe, L.; Risco-Risco, C.; Ayis, S. The association of treatment with hydroxychloroquine and hospital mortality in COVID-19 patients. Intern. Emerg. Med. 2020, 15, 1501–1506. [Google Scholar] [CrossRef]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcalá Díaz, J.F.; López Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef]
- Mitjà, O.; Corbacho-Monné, M.; Ubals, M.; Alemany, A.; Suñer, C.; Tebé, C.; Tobias, A.; Peñafiel, J.; Ballana, E.; Pérez, C.A.; et al. A cluster-randomized trial of hydroxychloroquine for prevention of COVID-19. N. Engl. J. Med. 2021, 384, 417–427. [Google Scholar] [CrossRef]
- Dequin, P.F.; Heming, N.; Meziani, F.; Plantefève, G.; Voiriot, G.; Badié, J.; François, B.; Aubron, C.; Ricard, J.D.; Ehrmann, S.; et al. Effect of Hydrocortisone on 21-Day Mortality or Respiratory Support among Critically Ill Patients with COVID-19: A Randomized Clinical Trial. JAMA 2020, 324, 1298–1306. [Google Scholar] [CrossRef]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Hermine, O.; Mariette, X.; Tharaux, P.L.; Resche-Rigon, M.; Porcher, R.; Ravaud, P. Effect of Tocilizumab vs Usual Care in Adults Hospitalized with COVID-19 and Moderate or Severe Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 32–40. [Google Scholar] [CrossRef]
- Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; Prudon, B.; et al. Effect of hydroxychloroquine in hospitalized patients with COVID-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar]
- Horby, P.W.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Emberson, J.; Palfreeman, A.; Raw, J.; Elmahi, E.; Prudon, B.; et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.P.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without azithromycin in mild-to-moderate COVID-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef] [PubMed]
- Furtado, R.H.M.; Berwanger, O.; Fonseca, H.A.; Corrêa, T.D.; Ferraz, L.R.; Lapa, M.G.; Zampieri, F.G.; Veiga, V.C.; Azevedo, L.C.P.; Rosa, R.G.; et al. Azithromycin in addition to standard of care versus standard of care alone in the treatment of patients admitted to the hospital with severe COVID-19 in Brazil (COALITION II): A randomised clinical trial. Lancet 2020, 396, 959–967. [Google Scholar] [CrossRef]
- Lyngbakken, M.N.; Berdal, J.E.; Eskesen, A.; Kvale, D.; Olsen, I.C.; Rueegg, C.S.; Rangberg, A.; Jonassen, C.M.; Omland, T.; Røsjø, H.; et al. A pragmatic randomized controlled trial reports lack of efficacy of hydroxychloroquine on coronavirus disease 2019 viral kinetics. Nat. Commun. 2020, 11, 5284. [Google Scholar] [CrossRef]
- Tang, W.; Cao, Z.; Han, M.; Wang, Z.; Chen, J.; Sun, W.; Wu, Y.; Xiao, W.; Liu, S.; Chen, E.; et al. Hydroxychloroquine in patients with mainly mild to moderate coronavirus disease 2019: Open label, randomised controlled trial. BMJ 2020, 369, m1849. [Google Scholar] [CrossRef]
- Urwyler, P.; Moser, S.; Charitos, P.; Heijnen, I.A.F.M.; Rudin, M.; Sommer, G.; Giannetti, B.M.; Bassetti, S.; Sendi, P.; Trendelenburg, M.; et al. Treatment of COVID-19 With Conestat Alfa, a Regulator of the Complement, Contact Activation and Kallikrein-Kinin System. Front. Immunol. 2020, 11, 2072. [Google Scholar] [CrossRef]
- Salvarani, C.; Dolci, G.; Massari, M.; Merlo, D.F.; Cavuto, S.; Savoldi, L.; Bruzzi, P.; Boni, F.; Braglia, L.; Turrà, C.; et al. Effect of Tocilizumab vs Standard Care on Clinical Worsening in Patients Hospitalized with COVID-19 Pneumonia: A Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 24–31. [Google Scholar] [CrossRef]
- Lofgren, S.M.; Nicol, M.R.; Bangdiwala, A.S.; Pastick, K.A.; Okafor, E.C.; Skipper, C.P.; Pullen, M.F.; Engen, N.W.; Abassi, M.; Williams, D.A.; et al. Safety of Hydroxychloroquine among Outpatient Clinical Trial Participants for COVID-19. Open Forum Infect. Dis. 2020, 7, ofaa500. [Google Scholar] [CrossRef]
- Abd-Elsalam, S.; Esmail, E.S.; Khalaf, M.; Abdo, E.F.; Medhat, M.A.; El Ghafar, M.S.A.; Ahmed, O.A.; Soliman, S.; Serangawy, G.N.; Alboraie, M. Hydroxychloroquine in the treatment of COVID-19: A multicenter randomized controlled study. Am. J. Trop. Med. Hyg. 2020, 103, 1635–1639. [Google Scholar] [CrossRef]
- Chen, C.P.; Lin, Y.C.; Chen, T.C.; Tseng, T.Y.; Wong, H.L.; Kuo, C.Y.; Lin, W.P.; Huang, S.R.; Wang, W.Y.; Liao, J.H.; et al. A multicenter, randomized, open-label, controlled trial to evaluate the efficacy and tolerability of hydroxychloroquine and a retrospective study in adult patients with mild to moderate coronavirus disease 2019 (COVID-19). PLoS ONE 2020, 15, e0242763. [Google Scholar] [CrossRef] [PubMed]
- Deftereos, S.G.; Giannopoulos, G.; Vrachatis, D.A.; Siasos, G.D.; Giotaki, S.G.; Gargalianos, P.; Metallidis, S.; Sianos, G.; Baltagiannis, S.; Panagopoulos, P.; et al. Effect of Colchicine vs Standard Care on Cardiac and Inflammatory Biomarkers and Clinical Outcomes in Patients Hospitalized with Coronavirus Disease 2019: The GRECCO-19 Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e2013136. [Google Scholar] [CrossRef] [PubMed]
- Annweiler, C.; Hanotte, B.; Grandin de l’Eprevier, C.; Sabatier, J.M.; Lafaie, L.; Célarier, T. Vitamin D and survival in COVID-19 patients: A quasi-experimental study. J. Steroid Biochem. Mol. Biol. 2020, 204, 105771. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Li, L.; Shen, A.; Chen, Y.; Qi, Z. Rational use of tocilizumab in the treatment of novel coronavirus pneumonia. Clin. Drug Investig. 2020, 40, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Capra, R.; De Rossi, N.; Mattioli, F.; Romanelli, G.; Scarpazza, C.; Sormani, M.P.; Cossi, S. Impact of low dose tocilizumab on mortality rate in patients with COVID-19 related pneumonia. Eur. J. Intern. Med. 2020, 76, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Rehman, S.; Majeed, T.; Ansari, M.A.; Ali, U.; Sabit, H.; Al-Suhaimi, E.A. Current scenario of COVID-19 in pediatric age group and physiology of immune and thymus response. Saudi J. Biol. Sci. 2020, 27, 2567–2573. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S. Remdesivir for the treatment of COVID-19. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Eastman, R.T.; Roth, J.S.; Brimacombe, K.R.; Simeonov, A.; Shen, M.; Patnaik, S.; Hall, M.D. Remdesivir: A review of its discovery and development leading to emergency use authorization for treatment of COVID-19. ACS Cent. Sci. 2020, 6, 672–683. [Google Scholar] [CrossRef]
- Arshad, S.; Kilgore, P.; Chaudhry, Z.S.; Jacobsen, G.; Wang, D.D.; Huitsing, K.; Brar, I.; Alangaden, G.J.; Ramesh, M.S.; McKinnon, J.E. Treatment with hydroxychloroquine, azithromycin, and combination in patients hospitalized with COVID-19. Int. J. Infect. Dis. 2020, 97, 396–403. [Google Scholar] [CrossRef]
- Heidary, F.; Gharebaghi, R. Ivermectin: A systematic review from antiviral effects to COVID-19 complementary regimen. J. Antibiot. 2020, 73, 593–602. [Google Scholar] [CrossRef]
- Turkia, M. A Timeline of Ivermectin-Related Events in the COVID-19 Pandemic. Available online: https://www.researchgate.net/profile/Mika-Turkia/publication/350610718_A_Timeline_of_Ivermectin-Related_Events_in_the_COVID-19_Pandemic_April_3_2021/links/6068b4a4458515614d32e5de/A-Timeline-of-Ivermectin-Related-Events-in-the-COVID-19-Pandemic-April-3-2021.pdf (accessed on 3 August 2022).
- Million, M.; Lagier, J.-C.; Gautret, P.; Colson, P.; Fournier, P.-E.; Amrane, S.; Hocquart, M.; Mailhe, M.; Esteves-Vieira, V.; Doudier, B. Early treatment of COVID-19 patients with hydroxychloroquine and azithromycin: A retrospective analysis of 1061 cases in Marseille, France. Travel Med. Infect. Dis. 2020, 35, 101738. [Google Scholar] [CrossRef] [PubMed]
- Gutin, G.; Yeo, A.; Zverovich, A. Traveling salesman should not be greedy: Domination analysis of greedy-type heuristics for the TSP. Discret. Appl. Math. 2002, 117, 81–86. [Google Scholar] [CrossRef] [Green Version]
- Cantini, F.; Goletti, D.; Petrone, L.; Najafi Fard, S.; Niccoli, L.; Foti, R. Immune Therapy, or Antiviral Therapy, or Both for COVID-19: A Systematic Review. Drugs 2020, 80, 1929–1946. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Guihur, A.; Rebeaud, M.; Mulot, M.; Peiffer-Smadja, N.; Mahamat-Saleh, Y. Effect of hydroxychloroquine with or without azithromycin on the mortality of COVID-19 patients: A systematic review and meta-analysis. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 27, 19–27. [Google Scholar]
- Rosenberg, E.S.; Dufort, E.M.; Udo, T.; Wilberschied, L.A.; Kumar, J.; Tesoriero, J.; Weinberg, P.; Kirkwood, J.; Muse, A.; DeHovitz, J.; et al. Association of Treatment with Hydroxychloroquine or Azithromycin with In-Hospital Mortality in Patients With COVID-19 in New York State. JAMA 2020, 323, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.H.; Frigault, M.J.; Serling-Boyd, N.J.; Fernandes, A.D.; Harvey, L.; Foulkes, A.S.; Horick, N.K.; Healy, B.C.; Shah, R.; Bensaci, A.M.; et al. Efficacy of Tocilizumab in Patients Hospitalized with COVID-19. N. Engl. J. Med. 2020, 383, 2333–2344. [Google Scholar] [CrossRef]
- Whitlock, M.C. Combining probability from independent tests: The weighted Z-method is superior to Fisher’s approach. J. Evol. Biol. 2005, 18, 1368–1373. [Google Scholar] [CrossRef]
- Mosteller, F.; Bush, R.R. Selected Quantitative Techniques; Addison-Wesley: Boston, MA, USA, 1954. [Google Scholar]
- Fleming, P.J.; Wallace, J.J. How not to lie with statistics: The correct way to summarize benchmark results. Commun. ACM 1986, 29, 218–221. [Google Scholar] [CrossRef]










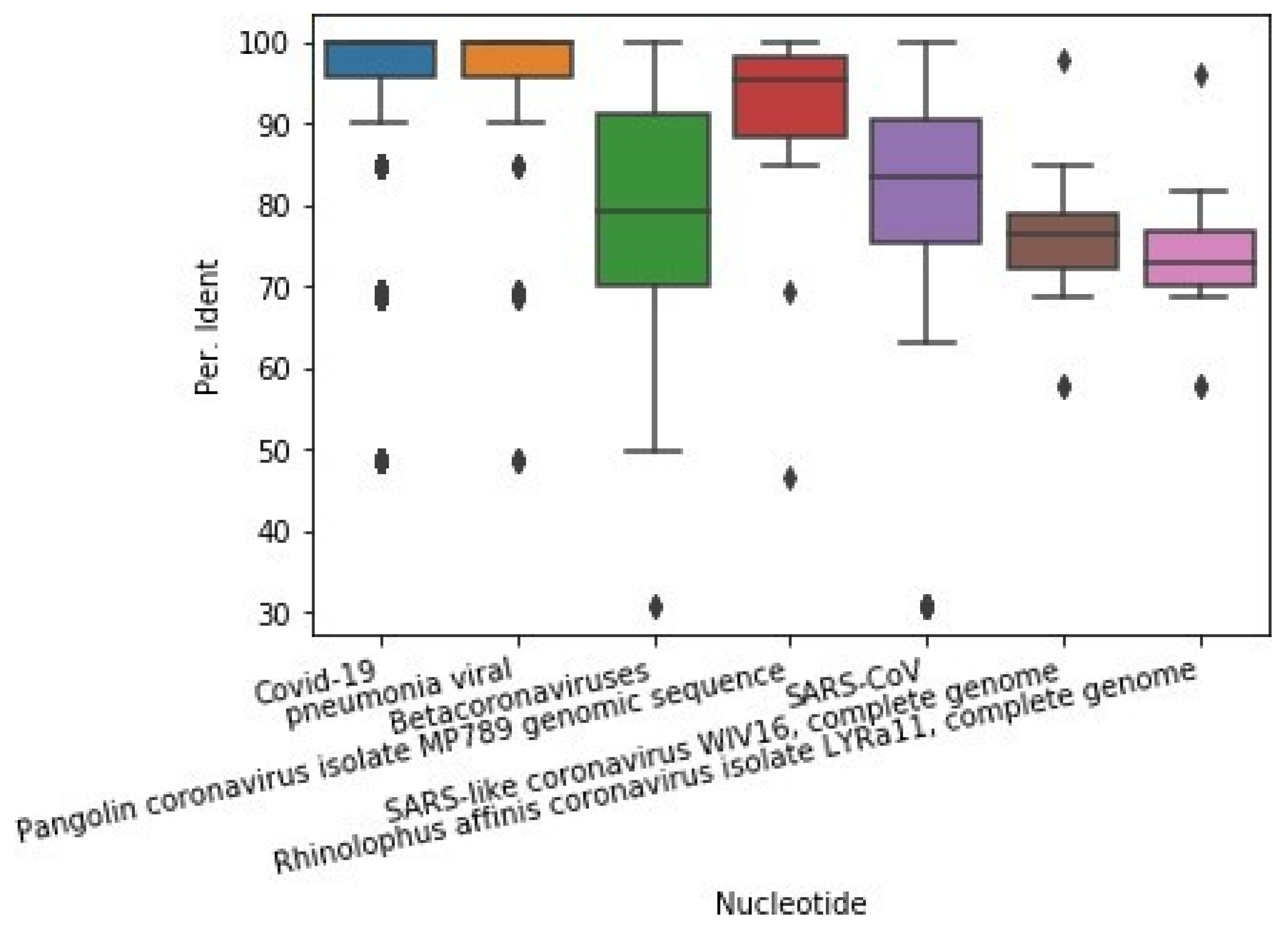
| Nucleotide | Count | Mean per Ident | std per Ident | Mean E-Value | std E-Value | Mean Query Cover | std Query Cover |
|---|---|---|---|---|---|---|---|
| Pneumonia viral | 163 | 94.99 | 11.8 | 3.99 × 10−2 | 2.24 × 10−1 | 99.76 | 1.36 |
| Pangolin coronavirus isolate MP789 | 22 | 91.19 | 11.95 | 7.27 × 10−2 | 3.33 × 10−1 | 99.91 | 0.29 |
| SARS-CoV | 2518 | 90.06 | 12.78 | 2.12 × 10−2 | 1.65 × 10−1 | 99.58 | 1.62 |
| Betacoronaviruses | 815 | 80.34 | 12.91 | 7.36 × 10−8 | 1.56 × 10−6 | 99.63 | 1.59 |
| SARS-like coronavirus WIV16 | 17 | 75.08 | 9.001 | 3.53 × 10−22 | 9.67 × 10−22 | 99.76 | 0.64 |
| Rhinolophus affinis coronavirus | 12 | 73.27 | 9.777 | 3.33 × 10−12 | 1 | 1.11 × 10−11 | 99.92 |
| First Author, Year, (Ref) | Site | Intervention Group (Participants, Mean Age, Male%, Drug) | Procedure Intervention Group | Control Group/Placebo (Participants, Mean Age (SD), Male%, Drug) | Procedure Control Group | Parameters | Comments |
|---|---|---|---|---|---|---|---|
| Abd-Elsalam, S. 2020, [62] | Egypt | 97 patients with COVID-19, 40.35 ± 18.65, HCQ+ standard care | HCQ 400 mg twice daily (in day 1) then HCQ 200 mg twice daily (in day 2–15) with standard care treatment by the Egyptian MOH for 15 days | 97 patients with COVID–19, 41.09 ± 20.07, Standard care | Standard care treatment by the Egyptian MOH for 15 days | Risk of mortality in HCQ treatment: OR = 0.824, p = 0.725 | HCQ treatment was not significantly associated with reduced mortality in COVID-19 patients |
| Abella, B.S. 2021, [27] | America | 66 HCWs with the aim of the prevention, 31 (20–66), HCQ | HCQ 200 mg tablets in 3 times a day with food (8 week) | 66 HCWs | Placebo group received custom-molded identically sized and shaped microcrystalline cellulose tablets | N/A | HCQ had no advantage in preventing COVID-19 in HCWs |
| Annweiler, C. 2020, [65] | France | 57 residents with COVID-19 from nursing-home, 87.7 ± 9.3, 21% Vitamin D supplement | Take a vitamin D3 supplement during COVID-19 or in the month before | 9 residents with COVID-19 from nursing-home, 87.4 ± 7.2, 33% | N/A | Risk of mortality: HR = 0.11, p = 0.003 OSCI score: Β = −3.84, p = 0.001 | Vitamin D3 supplement bolus reduced the severity of the disease and increased the survival of the elderly |
| Ansarin, K. 2020, [38] | Iran | 39 patients in ICU, 58.4 ± 13.7, 48.8%, Bromhexine hydrochloride and standard care | oral bromhexine hydrochloride 8 mg three times a day and standard care (Hydroxychloroquine 200 mg/d for two weeks) for two weeks | 39 patients in ICU, 61.1 ± 16.1, 61.5%, Standard care | Hydroxychloroquine 200 mg/d for two weeks | ICU admissions: 2 out of 39 intervention V.S 11 out of 39 control, p = 0.006 Intubation 1 out of 39 intervention vs. 9 out of 39 control, p = 0.007 Death 0 in intervention vs. 5 in control, p = 0.027 | Timely administration of oral bromhexine reduced mortality, reduced transfer to ICU, reduced intubation |
| Ayerbe, L. 2020, [46] | Spain | 1734 COVID-19 patients, 68.77 ± 15.09, 60.4%, Heparin | Heparin in 2–15 days | N/A | N/A | Adjusted OR for age and gender = 0.55, p = 0.003, OR oxygen < 90%, and temperature > 37 °C = 0.54, p = 0.003 Other drugs were included as covariates OR = 0.42, p < 0.001 | Heparin appeared to be involved in reducing mortality. However, randomized controlled trials are required for further investigation. |
| Ayerbe, L. 2020, [47] | Spain | 1857 patients with COVID-19, 67.11 ± 15.51, 62.04%, HCQ | HCQ in 2–15 days | N/A | N/A | Adjusted for age and gender, with OR = 0.44, p < 0.001, OR oxygen < 90%, and temperature > 37 °C = 0.45, p = < 0.001 | HCQ appeared to be involved in reducing mortality. However, randomized controlled trials are required for further investigation |
| Barnabas, R.V. 2021, [28] | America | 353 40 (27–51), 39%, HCQ | HCQ (400 mg/d for 3 days followed by 200 mg/d for 11 days) | 336, 38 (26–50), 41% Ascorbic acid | Ascorbic acid (500 mg/d followed by 250 mg/d) | HR SARS-CoV-2 acquisition = 1.10, p > 0.20 Frequency of participants experiencing adverse events: 66 in HCQ group vs. 46 in control group, p = 0.026 | The results of the study indicate a significant effect of HCQ as prevention after exposure to the prevention of SARS-CoV-2 infection. |
| Boulware, D.R. 2020, [29] | America | 414, 41 (33–51), 47.3%, HCQ | HCQ (800 mg once, followed by 600 mg in 6 to 8 h, then 600 mg daily for 4 additional days) | 407, 40 (32–50), 49.4% | Placebo folate tablets, which were similar in appearance to the HCQ | The incidence of new illness: 11.8% in HCQ group vs. 14.4% in placebo group | The incidence of new illness compatible with COVID-19 did not differ significantly between groups |
| Brown, S.M. 2021, [30] | America | 42, 51 (42–60), 54% HCQ | HCQ, drug was held if QTc > 500 msec | 43, 58 (43–68), 67, Azithromycin | Azithromycin was held if QTc > 500 msec | _ | Studies have shown that neither drug is superior to the other. It was also observed that renal complications of HCQ were greater than azithromycin, which may be due to chance |
| Cavalcanti, A.B. 2020, [55] | Brazil | 217, 49.6 ± 14.2, 56.7%, HCQ plus plus azithromycin, 221, 51.3 ± 14.5, 64.3%, HCQ | Standard care plus HCQ at a dose of 400 mg twice daily plus azithromycin at a dose of 500 mg once daily for 7 days standard care plus HCQ at a dose of 400 mg twice daily | 227, 49.9 ± 15.1, 54.2%, Standard care | Standard care | OR (HCQ alone): 1.21, p = 1 OR (HCQ plus azithromycin) = 0.99, p = 1 | The use of HCQ alone or with azithromycin did not improve clinical status at 15 days compared with standard care |
| Chen, C.P. 2020 [63] | Taiwan | 21, 33 ± 12 52.4%, HCQ | HCQ (400 mg twice for 1 d or HCQ 200 mg twice daily for 6 days) plus standard care | 12, 32.8 ± 8.3, 66.7 | Standard care | Neither study demonstrated that HCQ shortened viral shedding in mild to moderate COVID-19 subjects. | |
| Davoudi-Monfared, E. 2020 [39] | Iran | 42, 56.50, 52.4%, IFN | 44 micrograms/mL (12 million IU/mL) of interferon β-1a was subcutaneously injected three times weekly for two consecutive weeks | 39, 61.00, 56.4, Control | National protocol medications | Overall mortality: OR = 2.5, p < 0.05, Early administration reduced mortality: OR = 13.5 | The use of IFN had a significant effect on reducing mortality |
| Deftereos, S.G. 2020, [64] | Greek | 55, 63, 56.4%, Colchicine | 1.5 mg loading dose followed by 0.5 mg after 60 min and maintenance doses of 0.5 mg twice daily plus standard care | 50, 65, 60 | Standard care | Clinical deterioration control vs. intervention: OR = 0.11, p = 0.02 | Participants who received colchicine had statistically significantly improved time to clinical deterioration |
| Dequin, P.F. 2020, [50] | France | 76, 63.1 (51.5–70.8), 71.1%, HCQ | 200 mg/d until day 7 and then decreased to 100 mg/d for 4 days and 50 mg/d for 3 days, for a total of 14 days | 73, 66.3 (53.5–72.7), 68.5, Placebo | Standard care | _ | Low-dose hydrocortisone, compared with placebo, did not significantly reduce treatment failure |
| Entrenas Castillo, M. 2020, [48] | Spain | 50, 53.14 ± 10.77, 54% Calcifediol | (400 mg every 12 h on the first day, and 200 mg every 12 h for the following 5 days), azithromycin (500 mg orally for 5 days PLUS oral calcifediol (0.532 mg) | 26, 52.77 ± 9.35, 69%, Control | (400 mg every 12 h on the first day, and 200 mg every 12 h for the following 5 days), azithromycin (500 mg orally for 5 days | Multivariate risk estimate odds ratio for ICU: intervention vs. control OR = 0.02 | Calcifediol in combination with standard treatment significantly reduced the need for ICU treatment in patients requiring hospitalization due to COVID-19 |
| Eslami, G. 2020, [40] | Iran | 35, 62 (47–69), 49% sofosbuvir/daclatasvir | One arm received a single daily pill containing 400 mg sofosbuvir and 60 mg daclatasvir | 27, 60 (43–73), 52, Ribavirin | 600 mg ribavirin every 12 h | relative risk of death for patients treated with sofosbuvir/daclatasvir: RR = 0.17, p = 0.02 relative risk of number needed to treat for benefit: RR: 3.6, p < 0.01 | Treatment of patients with severe COVID-19 with sofosbuvir/daclatasvir was significantly more effective than ribavirin through improved clinical symptoms |
| Furtado, R.H.M. 2020, [56] | Brazil | 214, 59.4 (49.3–70.0), 60%, Azithromycin | Azithromycin (500 mg via oral, nasogastric, or intravenous administration once daily for 10 days) plus standard of care (HCQ 400 mg twice daily for 10 days) | 183, 60.2 (52.0–70.1) 67%, Control | Standard of care (HCQ 400 mg twice daily for 10 days) | OR = 1.36, p = 0.11 | There was no significant difference in terms of side effects and effective treatment between the two groups |
| Garibaldi, B.T. 2021, [31] | America | 342, 60 (46–69), 55.3%, remdesivir | Remdesivir plus corticosteroid administration. | 1957, 60 (44–74), 51.3%, Control | Without remidisivir treatment | Clinical improvement: HR = 1.47, Mortality: HR = 0.7 p > 0.05 | The differences between the two groups were not significant in terms of mortality reduction and recovery rate |
| Gautret, P. 2020, [51] | France | 20, 51.2 ± 18.7, 45%, HCQ | Hydroxychloroquine sulfate 200 mg, three times per day for ten days | 16, 37.3 ± 24.0, 37.5%, Control | Standard care | _ | Twenty cases were treated in this study and showed a significant reduction in the viral carriage at D6 post-inclusion compared to controls |
| Hermine, O. 2021, [52] | France | 63, 64.0 (57.1–74.3), 70%, Tocilizumab | 8mg/kg, intravenously plus usual care on day 1 and on day 3 if clinically indicated | 67, 63.3 (57.1–72.3), 66%, | Usual care | Noninvasive ventilation (NIV) or mechanical ventilation (MV) or more died in the TCZ group than in the UC group: HR = 0.58, | May reduce the risk of NIV, MV, and death. Further studies are needed to confirm these preliminary results. |
| Horby, P. 2020, [53] | England | 1561, 65.2 ± 15.2, 61.5%, HCQ | A 200 mg tablet containing a 155 mg base equivalent) in a loading dose of four tablets (total dose, 800 mg) at baseline and at 6 h, which was followed by two tablets (total dose, 400 mg) starting at 12 h after the initial dose and then every 12 h for the next 9 days | 3155, 65.4 ± 15.4, 62.6% | Usual care | Death within 28 days: RR = 1.09. p = 0.15 discharged from the hospital alive within 28: RR = 0.9, invasive mechanical ventilation or death: RR: 1.14 | Among patients hospitalized with COVID-19, those who received HCQ did not have a lower incidence of death at 28 days than those who received usual care |
| Horby, P.W. 2020, [54] | England | 1616, 66·0 ± 16·0, 60%, Lopinavir–ritonavir | (400 mg and 100 mg, respectively) by mouth for 10 days | 3424, 66·4 ± 15·8, 61% | Usual care | died within 28: RR = 1.03, p = 0.6. Discharged from hospital alive within 28 days: RR = 0.98, p = 0.53 invasive mechanical ventilation or death: RR = 1.09, p = 0.092 | In patients admitted to hospital with COVID-19, lopinavir–ritonavir was not associated with reductions in 28-day mortality, duration of hospital stay, or risk of progressing to invasive mechanical ventilation or death |
| Kasgari, H.A. 2020, [41] | Iran | 24, 45 (38–69), 46%, sofosbuvir/daclatasvir/ribavirin | 400 mg sofosbuvir, 60 mg daclatasvir, and 1200 mg ribavirin | 24, 60 (47.5–68.5), 29% | Standard care | Number of ICU admission: intervention vs. control (0 versus 4, p = 0.109) Number of deaths: intervention vs. control (0 versus 3, p = 0.234) | The number of ICU admissions in the sofosbuvir/daclatasvir/ribavirin group was not significantly lower than the control group There was no difference in the number of deaths between the groups |
| Langer-Gould, A. 2020, [32] | America | 52, 59.8 ± 11.7, 86% Tocilizumab | 1–4 doses of tocilizumab median of 14 days | 41, 58.8 (12.7), 68.3%, Anakinra | Anakinra, a median of 14 days | _ | _ |
| Lofgren, S.M. 2020, [61] | Canada | 658, _ _ HCQ | 800 mg load dosing, followed by 600 mg 6–8 h later, and then 600 mg daily for 5 days in total. | 654, _ _ Placebo | _ | Data from 3 outpatient COVID-19 trials demonstrated that gastrointestinal side effects were common but mild with the use of hydroxychloroquine, whereas serious side effects were rare | |
| Lyngbakken, M. N. 2020, [57] | Norway | 27, 56 (41, 72), 70.4% HCQ | At a dose of 400 mg twice daily for 7 days) | 26, 69 (51, 74), 61.5% | Standard care | Died in hospital: OR = 1.11, p > 0.05 | Therapy with hydroxychloroquine did not impact SARS-CoV-2 viral kinetics in patients admitted to hospital with moderately severe COVID-19. |
| Mitjà, O. 2021, [49] | Spain | 1116, 48.6 ± 18.7, 27.3 HCQ | The drug at a dose of 800 mg once, followed by 400 mg daily for 6 days | 1198, 27, 27% | Usual care | The incidence of PCR-confirmed symptomatic COVID-19: RR = 0.86, p > 0.05 | Post-exposure-therapy with HCQ did not prevent SARS-CoV-2 infection or symptomatic COVID-19 in healthy persons exposed to a PCR-positive case patient |
| Nojomi, M. 2020, [42] | Iran | 50, 56.6 ± 17.8, 66% Arbidol plus HCQ | HCQ (400 mg BD on first day) followed by ARB (200 mg TDS) 7 to 14 days | 50, 56.6 ± 17.8, 54% Kaletra plus HCQ | HCQ (400 mg on first day) followed by 400 mg Kaletra (lopinavir/ritonavir) BD 7 to 14 days | _ | Our findings showed that arbidol, compared to Kaletra, significantly contributes to clinical and laboratory improvements, including peripheral oxygen saturation, requiring ICU admissions, duration of hospitalization |
| Rahmani, H. 2020, [33] | America | 33, 60 (47–73), 60.6% Interferon | IFN β-1b (250 mcg subcutaneously every other day for two consecutive weeks) | 33, 61 (50–71), 57.5% Control | (lopinavir/ritonavir or atazanavir/ritonavir plus HCQ for 7–10 days) | Time to clinical improvement: HR= 2.30, p = 0.002. discharged patients OR = 3.09, p = 0.03 ICU admission rate: p = 0.04 All-cause 28-day mortality: 6.06% vs. 18.18%, p = 0.12 | IFN β-1b was effective in shortening the time to clinical improvement without serious adverse events in patients with severe COVID-19. Furthermore, admission in ICU and need for invasive mechanical ventilation decreased following administration of IFN β-1b |
| Roozbeh, F. 2021, [43] | Iran | 27, 43 (37–52), 44%, sofosbuvir/daclatasvir | Azithromycin capsules (500 mg for 6 days) with naproxen tablets (500 mg, twice daily for 7 days), as well as 40 mg pantoprazole tablets.,plus single daily oral tablet containing 400 mg sofosbuvir and 60 mg daclatasvir with HCQ (200 mg twice daily) for 7 days, | 28, 47.5 (37–53), 50% | Azithromycin capsules (500 mg for 6 days) with naproxen tablets (500 mg, twice daily for 7 days), as well as 40 mg pantoprazole tablets. | _ | Sofosbuvir/daclatasvir did not significantly alleviate symptoms after 7 days of treatment compared with control. Although fewer hospitalizations were observed in the sofosbuvir/daclatasvir arm, this was not statistically significant. Sofosbuvir/daclatasvir significantly reduced the number of patients with fatigue and dyspnea after 1 month |
| Sadeghi, A. 2020, [44] | Iran | 33, 58 (38–65), 61% sofosbuvir/daclatasvir | HCQ 200 mg twice daily with or without lopinavir/ritonavir 200 mg/50 mg twice daily PLUS single daily oral tablet containing 400 mg sofosbuvir and 60 mg daclatasvir and standard care 14 days | 33, 62 (49–70), 42% Control | HCQ 200 mg twice daily with or without lopinavir/ritonavir 200 mg/50 mg twice daily. | Clinical recovery within 14 days: 88% VS. 66%. p = 0.076, Median duration of hospitalization: 6 days vs. 8 days, p = 0.029. Incidence of hospital discharge: (Gray’s p = 0.041). | The addition of sofosbuvir and daclatasvir to standard care significantly reduced the duration of hospital stay compared with standard care alone. Although fewer deaths were observed in the treatment arm, this was not statistically significant. |
| Salvarani, C. 2021, [60] | Italy | 60, 61.5 (51.5–73.5), 66.7%, Tocilizumab | Tocilizumab intravenously within 8 h from randomization at a dose of 8 mg/kg up to a maximum of 800 mg, followed by a second dose after 12 h. | 66, 60.0 (54.0–69.0), 56.1%, Standard care | supportive care following the treatment protocols of each center | clinical worsening: RR: 1.05, died before 30: 2 vs. 1 patients Intubated: 6 vs. 5 patients | No benefit toward disease progression was observed compared with standard care. |
| Satlin, M.J. 2020, [34] | America | 153, 62 (47–74), 63% HCQ | A dosage of 600 mg of HCQ every 12 h for two doses, followed by 400 mg daily for four additional days | N/A | N/A | - | HCQ appears to be reasonably safe and tolerable in most hospitalized patients with COVID-19. However, nearly one half of patients did not improve with this treatment |
| Sekhavati, E. 2020, [45] | Iran | 56, 54.38 ± 15.92, 50%, Azithromycin | Oral AZM 500 mg daily, oral LPV/r 400/100 mg twice daily, and oral HCQ 400 mg daily (5 days) | 55, 59.89 ± 15.55, 41.8% | Oral LPV/r 400/100 mg twice daily and oral HCQ 400 mg daily (5 days) | SpO 2 at discharge: Hedges g: −0.461, RR at discharge: 0.721 Length of hospital stay: 0.618 | The SpO 2 levels at discharge were significantly higher, the respiratory rate was lower, and the duration of admission was shorter in the case group. There was no significant difference in the mortality rate between the two groups |
| Self, W.H. 2020, [35] | America | 242, 58 (45–69), 55.8%, HCQ | 400 mg of HCQ sulfate in pill form twice a day for the first 2 doses and then 200 mg in pill form twice a day for the subsequent 8 doses, for a total of 10 doses over 5 days | 237, 57 (43–68), 55.7% | Matching placebo in the same dosing frequency. Patients discharged from the hospital before day 5 continued the trial medication after discharge to complete the 10-dose course | Clinical status: aOR = 1.02, p > 0.05, died: aOR = 1.07, p > 0.05 | Among adults hospitalized with respiratory illness from COVID-19, treatment with HCQ compared with placebo did not significantly improve clinical status at day 14 |
| Skipper, C. P. 2020, [36] | America | 212, 41 (33–49), 42% HCQ | 800 mg (4 tablets) once, then 600 mg (3 tablets) 6 to 8 h later, then 600 mg (3 tablets) once daily for 4 more days (5 days in total) | 211, 39 (31–50), 45.5 | Folic acid, 400 mcg, placebo tablets | difference in symptom severity: p = 0.117. Medication adverse effects: 43% VS. 24%, p = p < 0.001, Death: p = 0.29 | HCQ did not substantially reduce symptom severity in outpatients with early, mild COVID-19. |
| Tang, W. 2020, [58] | China | 75, 48.0 (14.1), 56% HCQ + standard care | 1200 mg daily for three days followed by a maintenance dose of 800 mg daily. duration: two or three weeks | 75, 44.1 (15.0), 53% | Standard care | _ | HCQ did not result in a significantly higher probability of negative conversion than standard of care alone in patients admitted to hospital with mainly persistent mild to moderate COVID-19 |
| Ulrich, R.J. 2020, [37] | America | 67, 66.5 (16.4), 67.2% HCQ | HCQ 400 mg (2 tablets) by mouth two times per day (day 1) and 200 mg (1 tablet) by mouth two times per day (days 2–5); the five-day | 61, 65.8 (16.0), 50.8% | Citrate was 400 mg (2 tablets) by mouth two times per day (day 1) and 200 mg (1 tablet) by mouth two times per day (days 2–5) | Severe disease progression endpoint: 11 people vs. 6, p = 0.350 | HCQ did not prevent severe outcomes or improve clinical scores |
| Urwyler, P. 2020, [59] | Switzerland | 5, 60 (54–81), 80%, Conestat alfa | Conestat alfa was administered by intravenous injections of 8400 IU followed by 3 additional doses of 4200 IU in 12-h intervals. Five patients | 15, 59 (51–71), 80% | Control | _ | Targeting multiple inflammatory cascades by conestat alfa was safe and associated with clinical improvements in the majority of severe COVID-19 patients |
| Human Gene | p-Value | Scenario 1 | Scenario 2 | Scenario 3 | Scenario 4 | Scenario 5 |
|---|---|---|---|---|---|---|
| ACE2 | 2.58614 × 10−6 | 0.999965 | 0.99999 | 0.9999 | 0.9999 | 0.99999 |
| TMPRSS2 | 1.05708 × 10−5 | 0.99999 | 0.99999 | 0.9999 | 0.9999 | 0.999988 |
| CDSN | 4.51014 × 10−5 | 0.9999 | 0.99993 | 0.999 | 0.9999 | 0.99965 |
| CRP | 0.0001264 | 0.9993 | 0.99994 | 0.9999 | 0.99741 | 0.99999 |
| FURIN | 0.000266511 | 0.99984 | 0.99814 | 0.9990 | 0.9999 | 0.96877 |
| IL6 | 0.000331227 | 0.99978 | 0.99998 | 0.9999 | 0.9999 | 0.999985 |
| SH2D3C | 0.0008493 | 0.18437 | 0.99988 | 0.00084 | 0.98506 | 0.99689 |
| IGHV3-53 | 0.000991476 | 0.00099 | 0.000991 | 0.00099 | 0.000991 | 0.000991 |
| IL1RN | 0.0016043 | 0.99938 | 0.99999 | 0.9999 | 0.99997 | 0.999994 |
| F2 | 0.00201681 | 0.999930 | 0.992066 | 0.9999 | 0.9999 | 0.99998 |
| SH2D3A | 0.00212852 | 0.002128 | 0.002128 | 0.0021 | 0.002128 | 0.00212 |
| BSG | 0.00226155 | 0.99835 | 0.97591 | 0.99303 | 0.9999 | 0.99303 |
| IL6R | 0.00240459 | 0.889887 | 0.99172 | 0.99834 | 0.99951 | 0.998715 |
| LZTFL1 | 0.00241652 | 0.00241 | 0.002416 | 0.002416 | 0.00241 | 0.002416 |
| PSMD1 | 0.00270668 | 0.00270 | 0.00270 | 0.00270 | 0.00270 | 0.00270 |
| DPP4 | 0.00307444 | 0.85959 | 0.97018 | 0.98462 | 0.96566 | 0.55886 |
| TP53 | 0.00308951 | 0.997120 | 0.95810 | 0.62219 | 0.98204 | 0.99089 |
| PORCN | 0.00309865 | 0.003098 | 0.965501 | 0.00309 | 0.952501 | 0.99323 |
| VTN | 0.00319142 | 0.98295 | 0.95893 | 0.92295 | 0.990806 | 0.97145 |
| ACE | 0.00335915 | 0.99980 | 0.89595 | 0.97707 | 0.96491 | 0.98255 |
| CENPJ | 0.00366157 | 0.93348 | 0.98239 | 0.00366 | 0.00366 | 0.90752 |
| FAM214A | 0.00395025 | 0.00395 | 0.00395 | 0.00395 | 0.003950 | 0.003950 |
| F8A2 | 0.00395025 | 0.00395 | 0.00395 | 0.00395 | 0.003950 | 0.003950 |
| SNORA81 | 0.00395025 | 0.0039502 | 0.00395 | 0.00395 | 0.003950 | 0.003950 |
| LOC100506985 | 0.00395025 | 0.003950 | 0.00395 | 0.00395 | 0.003950 | 0.003950 |
| FUT3 | 0.00405499 | 0.004054 | 0.00405 | 0.0040 | 0.00405 | 0.00405 |
| BCL2 | 0.0042722 | 0.99430 | 0.92189 | 0.02736 | 0.99526 | 0.92189 |
| BMND7 | 0.00432166 | 0.99988 | 0.95967 | 0.94800 | 0.948063 | 0.97608 |
| BMND8 | 0.00432166 | 0.99988 | 0.95967 | 0.94800 | 0.948063 | 0.97608 |
| CTSL | 0.00436471 | 0.99935 | 0.99705 | 0.99799 | 0.99999 | 0.99990 |
| SLC6A19 | 0.00471616 | 0.00471 | 0.00471 | 0.00471 | 0.0047161621 | 0.004716 |
| CAT | 0.00488151 | 0.99434 | 0.00488 | 0.77965 | 0.7412232 | 0.90418 |
| IFITM3 | 0.00494488 | 0.00494 | 0.004944 | 0.00494 | 0.00494488 | 0.00494 |
| TRBV11-2 | 0.00499686 | 0.00499 | 0.004996 | 0.00499 | 0.004996 | 0.00499 |
| NAA50 | 0.00503439 | 0.91120 | 0.97522 | 0.00503 | 0.883134 | 0.99118 |
| SLC6A20 | 0.00510482 | 0.00510 | 0.00510 | 0.00510 | 0.88626 | 0.00510 |
| CASP3 | 0.00535504 | 0.99511 | 0.80333 | 0.96211 | 0.998222 | 0.80333 |
| RGAG4 | 0.00539409 | 0.00539 | 0.00539 | 0.00539 | 0.00539 | 0.00539 |
| ENDOU | 0.00559688 | 0.00559 | 0.00559 | 0.00559 | 0.005596 | 0.00559 |
| CXCL10 | 0.00562288 | 0.96926 | 0.88201 | 0.99996 | 0.84129 | 0.97786 |
| ARCN1 | 0.00573792 | 0.99997 | 0.99883 | 0.688791 | 0.96910 | 0.99926 |
| COPD | 0.00579706 | 0.99997 | 0.99883 | 0.69063 | 0.96913 | 0.99926 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiaei, A.; Salari, N.; Boush, M.; Mansouri, K.; Hosseinian-Far, A.; Ghasemi, H.; Mohammadi, M. Identification of Suitable Drug Combinations for Treating COVID-19 Using a Novel Machine Learning Approach: The RAIN Method. Life 2022, 12, 1456. https://doi.org/10.3390/life12091456
Kiaei A, Salari N, Boush M, Mansouri K, Hosseinian-Far A, Ghasemi H, Mohammadi M. Identification of Suitable Drug Combinations for Treating COVID-19 Using a Novel Machine Learning Approach: The RAIN Method. Life. 2022; 12(9):1456. https://doi.org/10.3390/life12091456
Chicago/Turabian StyleKiaei, Aliakbar, Nader Salari, Mahnaz Boush, Kamran Mansouri, Amin Hosseinian-Far, Hooman Ghasemi, and Masoud Mohammadi. 2022. "Identification of Suitable Drug Combinations for Treating COVID-19 Using a Novel Machine Learning Approach: The RAIN Method" Life 12, no. 9: 1456. https://doi.org/10.3390/life12091456