
Super-Responders in Moderate–Severe Psoriasis under Guselkumab Treatment: Myths, Realities and Future Perspectives

 ,
,  ,
,
Abstract
:1. Introduction
- To study the clinical and demographic differences in super-responders and in those who are not;
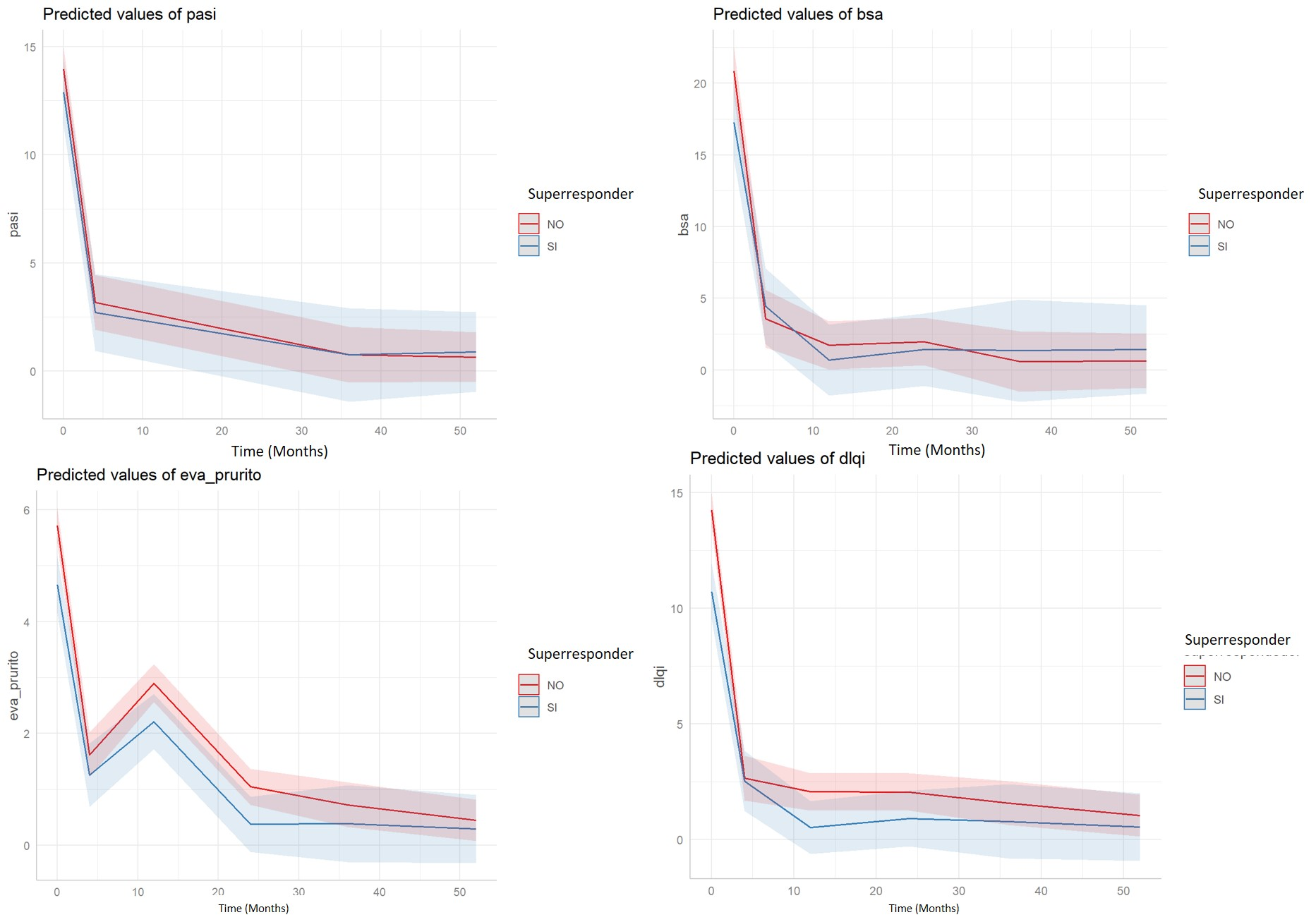
- To analyze the differences in the variables under study (PASI—Psoriasis activity skin index, BSA—Body surface area-, DLQI—Dermatology life quality index, and VAS—Visual analogic scale-pruritus) between both groups of patients (SR/non-SR) throughout the study period (baseline, 12, 24, 36, 52, 76 and 104 weeks);
- To perform a multivariate logistic analysis to find the baseline demographic and pathological characteristics that may be associated with the response of super-responders.
2. Material and Methods
2.1. Study Design
2.2. Patients
- (1)
- Adult moderate-to-severe plaque PSO patients;
- (2)
- PSO diagnosis since ≥1 year;
- (3)
- Treatment with Guselkumab (GUS) > 24 weeks. Patients received GUS following data sheet specifications (100 mg administered subcutaneously at weeks 0 and 4, followed by maintenance every 8 weeks).
- (1)
- Other types of PSO different than psoriasis vulgaris;
- (2)
- Inability to sign the informed consent document.
2.3. Definition of Superresponder
2.4. Statistical Analysis
3. Results
- (a)
- Patients with depression have reduced odds of being a super-responder by a factor of 0.182 (risk reduction of 82%, although the confidence interval is very wide);
- (b)
- For each unit increase in the VAS_pruritus, the odds of being a super-responder are reduced by a factor of 0.826 (17.4% reduction);
- (c)
- For each unit increase in the DLQI, the odds of being a super-responder are reduced by a factor of 0.909 (9.1% reduction).
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harvey, E.S.; Langton, D.; Katelaris, C.; Stevens, S.; Farah, C.S.; Gillman, A.; Harrington, J.; Hew, M.; Kritikos, V.; Radhakrishna, N.; et al. Mepolizumab effectiveness and identification of super-responders in severe asthma. Eur. Respir. J. 2020, 55, 1902420. [Google Scholar] [CrossRef] [PubMed]
- Prasad, V.; Vandross, A. Characteristics of Exceptional or Super Responders to Cancer Drugs. Mayo Clin. Proc. 2015, 90, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, C.T.; Peix, A.; de Amorim Fernandes, F.; Giubbini, R.; Karthikeyan, G.; Massardo, T.; Patel, C.; Pabon, L.M.; Jimenez-Heffernan, A.; Alexanderson, E.; et al. Clinical and gated SPECT MPI parameters associated with super-response to cardiac resynchronization therapy. J. Nucl. Cardiol. 2022, 29, 1166–1174. [Google Scholar] [CrossRef] [PubMed]
- Agache, I.; Rocha, C.; Pereira, A.; Song, Y.; Alonso-Coello, P.; Solà, I.; Beltran, J.; Posso, M.; Akdis, C.A.; Akdis, M.; et al. Efficacy and safety of treatment with omalizumab for chronic spontaneous urticaria: A systematic review for the EAACI Biologicals Guidelines. Allergy 2021, 76, 59–70. [Google Scholar] [CrossRef]
- Spertino, J.; Curto Barredo, L.; Rozas Muñoz, E.; Figueras Nart, I.; Gimenez Arnau, A.; Serra Baldrich, E.; Bonfill-Ortí, M.; Expósito-Serrano, V.; Guilabert, A.; Melé Ninot, G.; et al. Algorithm for Treatment of Chronic Spontaneous Urticaria with Omalizumab. Actas Dermosifiliogr. 2018, 109, 771–776. [Google Scholar] [CrossRef]
- Curto-Barredo, L.; Pujol, R.M.; Roura-Vives, G.; Gimenez-Arnau, A.M. Chronic urticaria phenotypes: Clinical differences regarding triggers, activity, prognosis and therapeutic response. Eur. J. Dermatol. 2019, 29, 627–635. [Google Scholar] [CrossRef]
- Kocatürk, E.; Başkan, E.B.; Küçük, Ö.S.; Özdemir, M.; Örnek, S.; Can, P.K.; Haşal, E.; Engin, B.; Atakan, N.; Alpsoy, E. Omalizumab versus cyclosporin-A for the treatment of chronic spontaneous urticaria: Can we define better-responding endotypes? An. Bras. Dermatol. 2022, 97, 592–600. [Google Scholar] [CrossRef]
- Curto-Barredo, L.; Archilla, L.R.; Vives, G.R.; Pujol, R.M.; Giménez-Arnau, A.M. Clinical Features of Chronic Spontaneous Urticaria that Predict Disease Prognosis and Refractoriness to Standard Treatment. Acta Derm.-Venereol. 2018, 98, 641–647. [Google Scholar] [CrossRef]
- Cao, Y.; Hong, F.; Conlon, D.M.; Sidur, L.; Smith, K.M.; Fang, Y.; Cuff, C.A.; Kaymakcalan, Z.; Ruzek, M.C. Potential predictive biomarkers of adalimumab response in patients with hidradenitis suppurativa. Br. J. Dermatol. 2021, 185, 804–814. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Domínguez-Cruz, J.; Navarro-Triviño, F.J.; Galán-Gutiérrez, M.; Armario-Hita, J.C.; Pereyra-Rodriguez, J.J. Atopic Dermatitis: Background, Objectives and Future Perspectives (Superresponders). Life 2022, 12, 1192. [Google Scholar] [CrossRef]
- Ariëns, L.F.; van der Schaft, J.; Spekhorst, L.S.; Bakker, D.S.; Romeijn, G.L.; Kouwenhoven, T.A.; Kamsteeg, M.; Voorberg, A.N.; Oosting, A.J.; de Ridder, I.; et al. Dupilumab shows long-term effectiveness in a large cohort of treatment-refractory atopic dermatitis patients in daily practice: 52-Week results from the Dutch BioDay registry. J. Am. Acad. Dermatol. 2021, 84, 1000–1009. [Google Scholar] [CrossRef] [PubMed]
- Nettis, E.; Ferrucci, S.M.; Ortoncelli, M.; Pellacani, G.; Foti, C.; Di Leo, E.; Patruno, C.; Rongioletti, F.; Argenziano, G.; Macchia, L.; et al. Use of Dupilumab in 543 Adult Patients with Moderate-to-Severe Atopic Dermatitis: A Multicenter, Retrospective Study. J. Investig. Allergol. Clin. Immunol. 2022, 32, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S.; Bansal, A.; Simpson, E.L.; Boguniewicz, M.; Blauvelt, A.; Siegfried, E.C.; Guttman-Yassky, E.; Hultsch, T.; Chen, Z.; Mina-Osorio, P.; et al. Clinically Meaningful Responses to Dupilumab in Adolescents with Uncontrolled Moderate-to-Severe Atopic Dermatitis: Post-hoc Analyses from a Randomized Clinical Trial. Am. J. Clin. Dermatol. 2020, 21, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Simpson, E.L.; Boguniewicz, M.; De Bruin-Weller, M.S.; Foley, P.; Kataoka, Y.; Bégo-Le-Bagousse, G.; Chen, Z.; Shumel, B.; Chao, J.; et al. Dupilumab Provides Rapid and Sustained Clinically Meaningful Responses in Adults with Moderate-to-severe Atopic Dermatitis. Acta Derm.-Venereol. 2021, 101, adv00585. [Google Scholar] [CrossRef] [PubMed]
- Canonica, G.W.; Bourdin, A.; Peters, A.T.; Desrosiers, M.; Bachert, C.; Weidinger, S.; Simpson, E.L.; Daizadeh, N.; Chen, Z.; Kamat, S.; et al. Dupilumab Demonstrates Rapid Onset of Response across Three Type 2 Inflammatory Diseases. J. Allergy Clin. Immunol. Pract. 2022, 10, 1515–1526. [Google Scholar] [CrossRef] [PubMed]
- Talamonti, M.; D’Adamio, S.; Galluccio, T.; Andreani, M.; Pastorino, R.; Egan, C.G.; Bianchi, L.; Galluzzo, M. High-resolution HLA typing identifies a new ‘super responder’ subgroup of HLA-C*06:02-positive psoriatic patients: HLA-C*06:02/HLA-C*04, in response to ustekinumab. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e364–e367. [Google Scholar] [CrossRef] [PubMed]
- Feldman SR, Merola JF, Pariser DM, Zhang J, Zhao Y, Mendelsohn AM; et al Clinical implications and predictive values of early PASI responses to tildrakizumab in patients with moderate-to-severe plaque psoriasis. J. Dermatol. Treat. 2022, 33, 1670–1675. [Google Scholar] [CrossRef]
- Reich, K.; Strober, B.; Langley, R.; Song, M.; Shen, Y.K.; You, Y.; Foley, P.; Blauvelt, A. Characterization of super responders to guselkumab treatment in moderate to severe psoriasis: Results from the VOYAGE 1 and 2 clinical trials. J. Am. Acad. Dermatol. 2020, 83, AB145. [Google Scholar] [CrossRef]
- Talamonti, M.; Galluzzo, M.; van den Reek, J.M.; de Jong, E.M.; Lambert, J.L.W.; Malagoli, P.; Bianchi, L.; Costanzo, A. Role of the HLA-C*06 allele in clinical response to ustekinumab: Evidence from real life in a large cohort of European patients. Br. J. Dermatol. 2017, 177, 489–496. [Google Scholar] [CrossRef]
- Raposo, I.; Carvalho, C.; Bettencourt, A.; Da Silva, B.M.; Leite, L.; Selores, M.; Torres, T. Psoriasis pharmacogenetics: HLA-Cw*0602 as a marker of therapeutic response to ustekinumab. Eur. J. Dermatol. 2017, 27, 528–530. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Rodriguez-Fernandez-Freire, L.; Armario-Hita, J.C.; Pérez-Gil, A.; Galán-Gutiérrez, M. Super responders to guselkumab treatment in moderate-to-severe psoriasis: A real clinical practice pilot series. Int. J. Dermatol. 2022, 61, 1029–1033. [Google Scholar] [CrossRef] [PubMed]
- Eyerich, K.; Weisenseel, P.; Pinter, A.; Schäkel, K.; Asadullah, K.; Wegner, S.; Muñoz-Elias, E.J.; Bartz, H.; Taut, F.J.; Reich, K. IL-23 blockade with guselkumab potentially modifies psoriasis pathogenesis: Rationale and study protocol of a phase 3b, randomised, double-blind, multicentre study in participants with moderate-to-severe plaque-type psoriasis (GUIDE). BMJ Open 2021, 11, e049822. [Google Scholar] [CrossRef] [PubMed]
- Schaekel, K.; Reich, K.; Asadullah, K.; Pinter, A.; Jullien, D.; Weisenseel, P.; Paul, C.; Gomez-Camacho, M.; Wegner, S.; Personke, Y.; et al. Early disease intervention in psoriasis leads to a faster and higher rate of complete skin clearance: Week 28 results from the GUIDE study. In Proceedings of the ISDS Conference, New York, NY, USA, 3–6 November 2021. [Google Scholar]
- Schäkel, K. Prognostic factors for early PASI 100 response in psoriasis patients treated with guselkumab: Results from the GUIDE study. Poster presented at the AAD. J. Am. Acad. Dermatol. 2022, 76. [Google Scholar]
- Blauvelt, A.; Papp, K.A.; Griffiths, C.E.M.; Randazzo, B.; Wasfi, Y.; Shen, Y.-K.; Li, S.; Kimball, A.B. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the continuous treatment of patients with moderate to severe psoriasis: Results from the phase III, double-blinded, placebo- and active comparator-controlled voyage 1 trial. J. Am. Acad. Dermatol. 2017, 76, 405–417. [Google Scholar] [PubMed]
- Papp, K.A.; Blauvelt, A.; Kimball, A.B.; Han, C.; Randazzo, B.; Wasfi, Y.; Shen, Y.K.; Li, S.; Griffiths, C.E.M. Patient-reported symptoms and signs of moderate-to-severe psoriasis treated with guselkumab or adalimumab: Results from the randomized voyage 1 trial. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1515–1522. [Google Scholar] [CrossRef]
- Reich, K.; Armstrong, A.W.; Foley, P.; Song, M.; Wasfi, Y.; Randazzo, B.; Li, S.; Shen, Y.-K.; Gordon, K.B. Efficacy and safety of guselkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of patients with moderate to severe psoriasis with randomized withdrawal and retreatment: Results from the phase III, double-blind, placebo- and active comparator-controlled voyage 2 trial. J. Am. Acad. Dermatol. 2017, 76, 418–431. [Google Scholar]
- Loft, N.; Egeberg, A.; Rasmussen, M.K.; Bryld, L.E.; Nissen, C.V.; Dam, T.N.; Ajgeiy, K.K.; Iversen, L.; Skov, L. Prevalence and characterization of treatment-refractory psoriasis and super-responders to biologic treatment: A nationwide study. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1284–1291. [Google Scholar] [CrossRef] [PubMed]
- Xie, K.K.; Braue, A.; Martyres, R.; Varigos, G. Baseline patients’ characteristics as predictors for therapeutic survival and response in patients with psoriasis on biological treatments. Australas. J. Dermatol. 2018, 59, e247–e252. [Google Scholar] [CrossRef]
- Yiu, Z.Z.N.; Becher, G.; Kirby, B.; Laws, P.; Reynolds, N.J.; Smith, C.H.; Warren, R.B.; Griffiths, C.E.M.; BADBIR Study Group. Drug Survival Associated with Effectiveness and Safety of Treatment with Guselkumab, Ixekizumab, Secukinumab, Ustekinumab, and Adalimumab in Patients with Psoriasis. JAMA Dermatol. 2022, e222909. [Google Scholar] [CrossRef]
- Rodriguez Fernandez-Freire, L.; Galán-Gutierrez, M.; Armario-Hita, J.C.; Perez-Gil, A.; Ruiz-Villaverde, R. Guselkumab: Short-term effectiveness and safety in real clinical practice. Dermatol. Ther. 2020, 33, e13344. [Google Scholar] [CrossRef]
- Ruiz-Villaverde, R.; Rodriguez-Fernandez-Freire, L.; Armario-Hita, J.C.; Pérez-Gil, A.; Galán-Gutiérrez, M. Guselkumab: Mid-term effectiveness, drug survival, and safety in real clinical practice. Dermatol. Ther. 2021, 34, e14798. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Villaverde, R.; Rodriguez-Fernandez-Freire, L.; Armario-Hita, J.C.; Pérez-Gil, A.; Chinchay, F.V.; Galán-Gutiérrez, M. Guselkumab as a switching strategy after anti-TNFα, anti-IL17, or anti-IL12/23 therapies in moderate-to-severe psoriasis. Dermatol. Ther. 2022, e15760. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| . | Non-SR | SR | p-Value |
|---|---|---|---|
| N = 72 | N = 28 | ||
| Sex | 0.692 | ||
| Male | 44 (61.1%) | 19 (67.9%) | |
| Female | 28 (38.9%) | 9 (32.1%) | |
| Age (Years) | 51.6 (14.8) | 47.1 (13.4) | 0.153 |
| Family History of PSO | 12 (23.1%) | 7 (31.8%) | 0.620 |
| Time of evolution (Years) | 19.0 [11.0;29.0] | 22.5 [11.0;26.8] | 0.797 |
| Weight (kg) | 85.0 [75.0;97.2] | 83.5 [69.5;90.2] | 0.449 |
| Height (cm) | 170 [162;178] | 175 [169;178] | 0.156 |
| BMI | 29.8 [26.3;32.0] | 26.9 [23.5;30.7] | 0.062 |
| Obesity | 35 (48.6%) | 8 (28.6%) | 0.111 |
| PsA | 14 (19.7%) | 5 (17.9%) | 1.000 |
| Diabetes | 15 (21.1%) | 4 (14.3%) | 0.621 |
| Hypertension | 19 (26.8%) | 6 (21.4%) | 0.769 |
| Dyslipidemia | 28 (39.4%) | 10 (35.7%) | 0.910 |
| Depression: | 12 (16.9%) | 1 (3.57%) | 0.102 |
| Nonalcoholic Fatty Liver | 9 (12.7%) | 4 (14.3%) | 1.000 |
| n_previous systemic treatments: | 0.494 | ||
| 0 | 3 (4.17%) | 0 (0.00%) | |
| 1 | 10 (13.9%) | 6 (21.4%) | |
| 2 | 43 (59.7%) | 18 (64.3%) | |
| 3 | 16 (22.2%) | 4 (14.3%) | |
| n_previous biological treatments | 2.00 [1.00;3.00] | 2.00 [1.00;3.00] | 0.664 |
| . | PASI | p-Value | BSA | p-Value | VAS Pruritus | p-Value | DLQI | p-Value |
|---|---|---|---|---|---|---|---|---|
| Basal | 13.0 [8.50;16.0] | 0.314 | 17.0 [8.00;24.0] | 0.223 | 5.00 [3.00;6.00] | 0.049 | 11.0 [5.00;15.0] | 0.013 |
| sem4 | 0.60 [0.00;2.75] | 0.005 | 1.00 [0.00;2.75] | 0.009 | 0.00 [0.00;1.00] | 0.034 | 0.00 [0.00;2.00] | 0.057 |
| sem12 | 0.00 [0.00;0.00] | <0.001 | 0.00 [0.00;0.00] | <0.001 | 2.00 [2.00;2.00] | <0.001 | 0.00 [0.00;0.00] | <0.001 |
| sem24 | 0.00 [0.00;0.00] | <0.001 | 0.00 [0.00;0.00] | <0.001 | 0.00 [0.00;0.00] | <0.001 | 0.00 [0.00;0.00] | <0.001 |
| sem36 | 0.00 [0.00;0.00] | <0.001 | 0.00 [0.00;0.00] | <0.001 | 0.00 [0.00;0.00] | 0.044 | 0.00 [0.00;1.00] | 0.043 |
| sem52 | 0.00 [0.00;0.00] | 0.001 | 0.00 [0.00;0.00] | 0.001 | 0.00 [0.00;0.00] | 0.044 | 0.00 [0.00;0.75] | 0.044 |
| Terms | Model.L.R. | d.f. | p Value | C | Dxy | Signif |
|---|---|---|---|---|---|---|
| Sex | 0.399 | 1 | 0.528 | 0.534 | 0.067 | ns |
| Age | 1.958 | 1 | 0.162 | 0.564 | 0.128 | ns |
| Familiar History PsO | 0.603 | 1 | 0.437 | 0.544 | 0.087 | ns |
| Time of evolution | 0.097 | 1 | 0.756 | 0.517 | 0.033 | ns |
| Weight_kg | 0.174 | 1 | 0.677 | 0.549 | 0.098 | ns |
| Height_cm | 2.811 | 1 | 0.094 | 0.592 | 0.183 | ns |
| BMI | 1.993 | 1 | 0.158 | 0.621 | 0.242 | ns |
| Obesity | 3.402 | 1 | 0.065 | 0.600 | 0.200 | ns |
| PsA | 0.045 | 1 | 0.831 | 0.509 | 0.019 | ns |
| Diabetes | 0.635 | 1 | 0.426 | 0.534 | 0.068 | ns |
| Hypertension | 0.309 | 1 | 0.578 | 0.527 | 0.053 | ns |
| Dyslipidemia | 0.118 | 1 | 0.731 | 0.519 | 0.037 | ns |
| Depression | 3.856 | 1 | 0.050 | 0.567 | 0.133 | |
| Nonalcoholic fatty liver | 0.045 | 1 | 0.832 | 0.508 | 0.016 | ns |
| n_previous biological | 0.592 | 1 | 0.441 | 0.527 | 0.055 | ns |
| PASI | 1.553 | 1 | 0.213 | 0.566 | 0.132 | ns |
| BSA | 2.132 | 1 | 0.144 | 0.580 | 0.159 | ns |
| VAS pruritus | 4.698 | 1 | 0.030 | 0.630 | 0.260 | |
| DLQI | 6.891 | 1 | 0.009 | 0.668 | 0.336 | ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Villaverde, R.; Vasquez-Chinchay, F.; Rodriguez-Fernandez-Freire, L.; C. Armario-Hita, J.; Pérez-Gil, A.; Galán-Gutiérrez, M. Super-Responders in Moderate–Severe Psoriasis under Guselkumab Treatment: Myths, Realities and Future Perspectives. Life 2022, 12, 1412. https://doi.org/10.3390/life12091412
Ruiz-Villaverde R, Vasquez-Chinchay F, Rodriguez-Fernandez-Freire L, C. Armario-Hita J, Pérez-Gil A, Galán-Gutiérrez M. Super-Responders in Moderate–Severe Psoriasis under Guselkumab Treatment: Myths, Realities and Future Perspectives. Life. 2022; 12(9):1412. https://doi.org/10.3390/life12091412
Chicago/Turabian StyleRuiz-Villaverde, Ricardo, Fiorella Vasquez-Chinchay, Lourdes Rodriguez-Fernandez-Freire, Jose C. Armario-Hita, Amalia Pérez-Gil, and Manuel Galán-Gutiérrez. 2022. "Super-Responders in Moderate–Severe Psoriasis under Guselkumab Treatment: Myths, Realities and Future Perspectives" Life 12, no. 9: 1412. https://doi.org/10.3390/life12091412