
Valvular Heart Disease following Anthracycline Therapy—Is It Time to Look beyond Ejection Fraction?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Protocol
2.3. Echocardiography
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Cancer Therapies
3.3. Echocardiographic Examinations
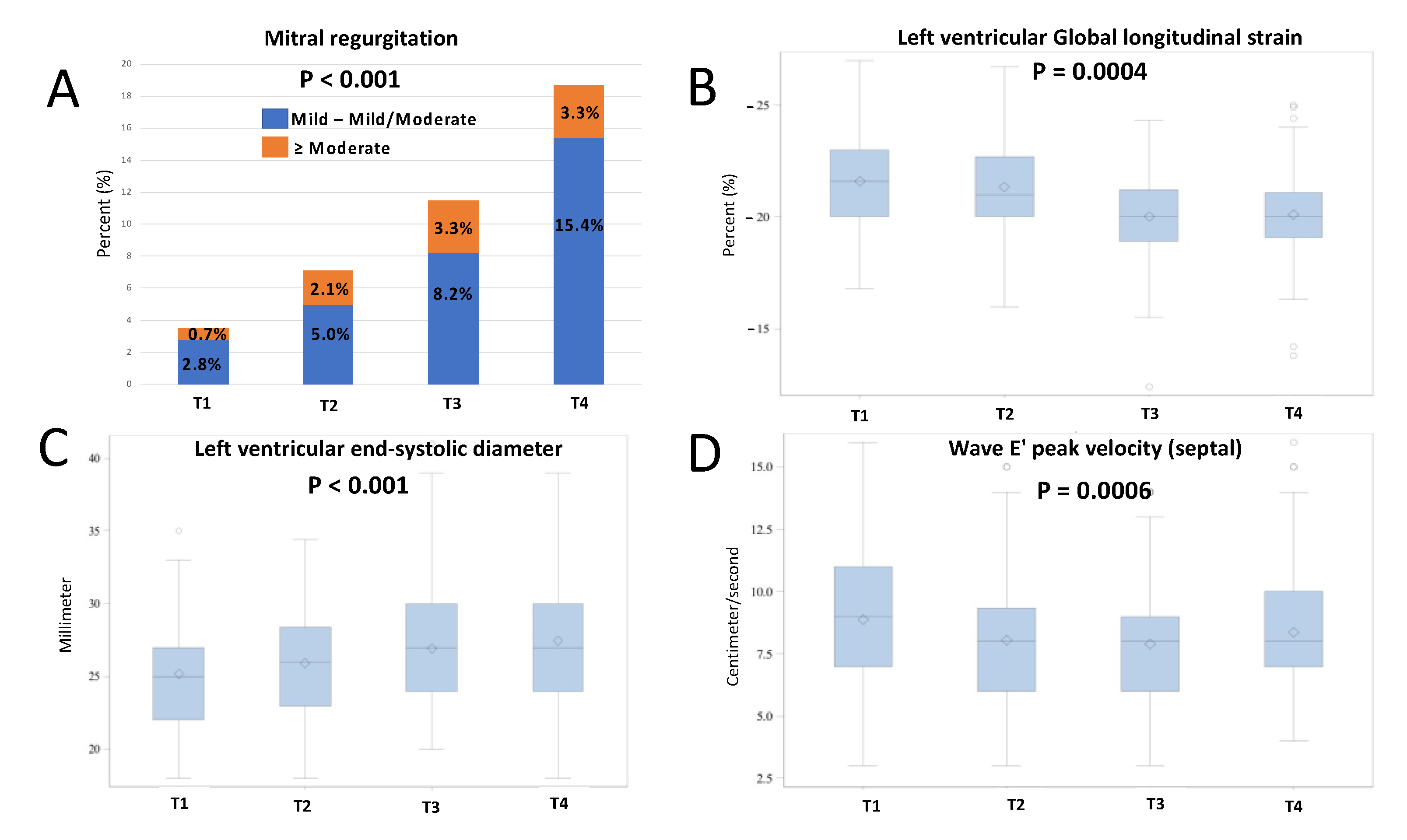
3.4. Echocardiographic Parameters
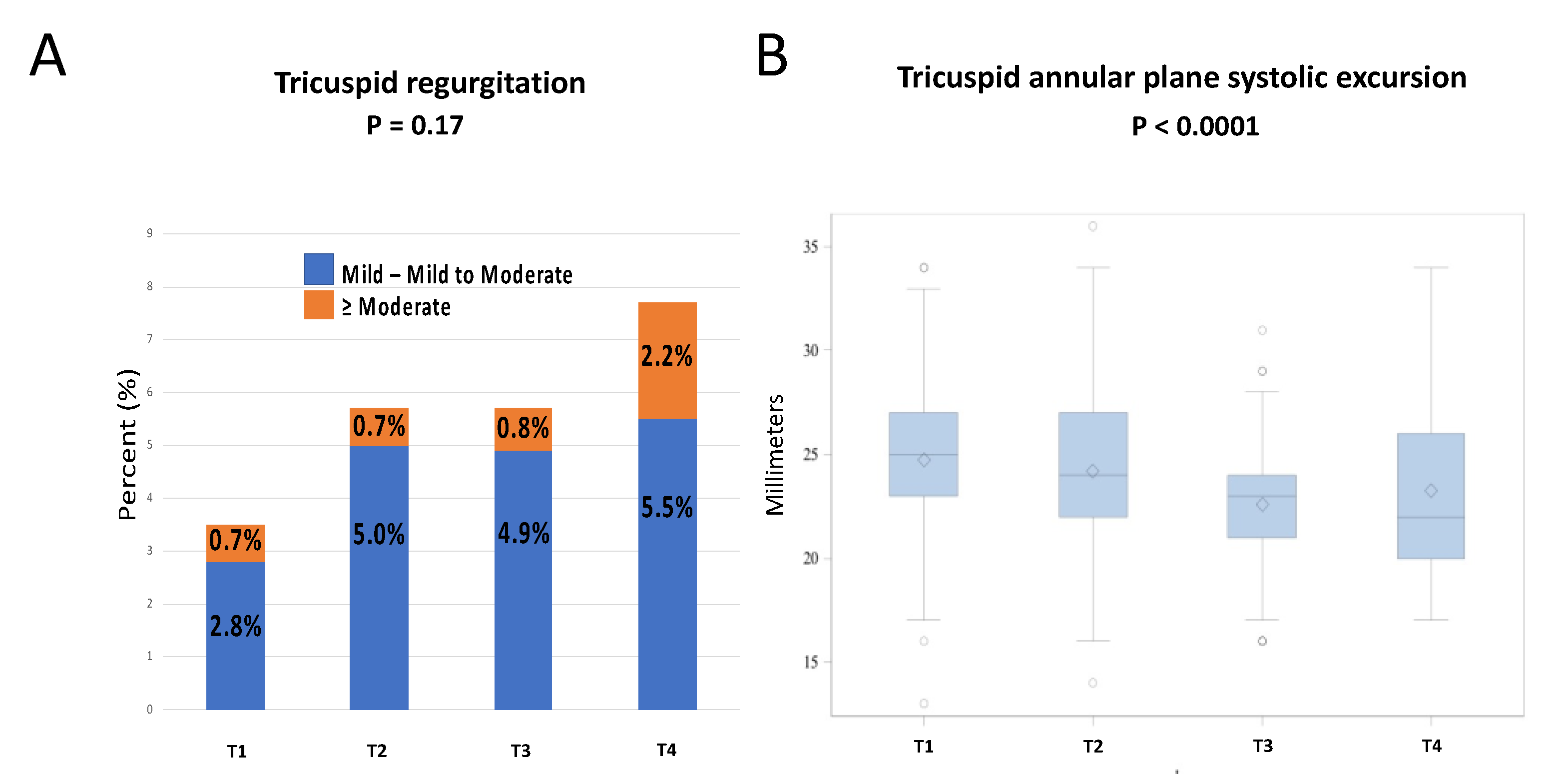
3.5. Valvular Parameters
3.6. Predictors of Deterioration of Mitral Function
3.7. Cardiotoxicity and Cardiovascular Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.; DeSantis, C.; Virgo, K.; Stein, K.; Mariotto, A.; Smith, T.; Cooper, D.; Gansler, T.; Lerro, C.; Fedewa, S.; et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J. Clin. 2012, 62, 220–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancellotti, P.; Anker, S.D.; Donal, E.; Edvardsen, T.; Popescu, B.A.; Farmakis, D.; Filippatos, G.; Habib, G.; Maggioni, A.P.; Jerusalem, G.; et al. EACVI/HFA Cardiac Oncology Toxicity Registry in breast cancer patients: Rationale, study design, and methodology (EACVI/HFA COT Registry)—EURObservational Research Program of the European Society of Cardiology. Eur. Heart. J. Cardiovasc. Imaging 2015, 16, 466–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart. J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Patnaik, J.L.; Byers, T.; DiGuiseppi, C.; Dabelea, D.; Denberg, T.D. Cardiovascular disease competes with breast cancer as the leading cause of death for older females diagnosed with breast cancer: A retrospective cohort study. Breast Cancer Res. 2011, 13, R64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vejpongsa, P.; Yeh, E.T. Prevention of anthracycline-induced cardiotoxicity: Challenges and opportunities. J. Am. Coll. Cardiol. 2014, 64, 938–945. [Google Scholar] [CrossRef] [Green Version]
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [Green Version]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar] [CrossRef]
- Quiñones, M.A.; Greenberg, B.H.; Kopelen, H.A.; Koilpillai, C.; Limacher, M.C.; Shindler, D.M.; Shelton, B.J.; Weiner, D.H. Echocardiographic predictors of clinical outcome in patients with left ventricular dysfunction enrolled in the SOLVD registry and trials: Significance of left ventricular hypertrophy. Studies of Left Ventricular Dysfunction. J. Am. Coll. Cardiol. 2000, 35, 1237–1244. [Google Scholar] [CrossRef] [Green Version]
- Santoro, C.; Arpino, G.; Esposito, R.; Lembo, M.; Paciolla, I.; Cardalesi, C.; De Simone, G.; Trimarco, B.; De Placido, S.; Galderisi, M. 2D and 3D strain for detection of subclinical anthracycline cardiotoxicity in breast cancer patients: A balance with feasibility. Eur. Heart. J. Cardiovasc. Imaging 2017, 18, 930–936. [Google Scholar] [CrossRef]
- Cardinale, D.; Colombo, A.; Lamantia, G.; Colombo, N.; Civelli, M.; De Giacomi, G.; Rubino, M.; Veglia, F.; Fiorentini, C.; Cipolla, C.M. Anthracycline-induced cardiomyopathy: Clinical relevance and response to pharmacologic therapy. J. Am. Coll. Cardiol. 2010, 55, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive heart failure in patients treated with doxorubicin: A retrospective analysis of three trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Cohen, V.; Gosavi, S.; Carver, J.R.; Wiegers, S.E.; Martin, R.P.; et al. Early detection and prediction of cardiotoxicity in chemotherapy-treated patients. Am. J. Cardiol. 2011, 107, 1375–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laufer-Perl, M.; Derakhshesh, M.; Milwidsky, A.; Mor, L.; Ravid, D.; Amrami, N.; Sherez, J.; Keren, G.; Topilsky, Y.; Arbel, Y. Usefulness of Global Longitudinal Strain for Early Identification of Subclinical Left Ventricular Dysfunction in Patients with Active Cancer. Amer. J. Cardiol. 2018, 122, 1784–1789. [Google Scholar] [CrossRef] [PubMed]
- Aleman, B.M.; van den Belt-Dusebout, A.W.; De Bruin, M.L.; van’t Veer, M.B.; Baaijens, M.H.A.; de Boer, J.P.; Hart, A.A.M.; Klokman, W.J.; Kuenen, M.A.; Ouwens, G.M.; et al. Late cardiotoxicity after treatment for Hodgkin lymphoma. Blood 2007, 109, 1878–1886. [Google Scholar] [CrossRef] [Green Version]
- Laufer-Perl, M.; Arnold, J.H.; Mor, L.; Amrami, N.; Derakhshesh, M.; Moshkovits, Y.; Sadeh, B.; Arbel, Y.; Topilsky, Y.; Rozenbaum, Z. The association of reduced global longitudinal strain with cancer therapy-related cardiac dysfunction among patients receiving cancer therapy. Clin. Res. Cardiol. 2020, 109, 255–262. [Google Scholar] [CrossRef]
- Laufer-Perl, M.; Mor, L.; Milwidsky, A.; Derakhshesh, M.; Amrami, N.; Moshkovits, Y.; Arnold, J.; Topilsky, Y.; Arbel, Y.; Rozenbaum, Z. Cancer Therapeutics-Related Cardiac Dysfunction among Patients with Active Breast Cancer: A Cardio-Oncology Registry. Isr. Med. Assoc. J. 2020, 22, 564–568. [Google Scholar]
- Hochstadt, A.; Arnold, J.; Rosen, R.; Sherez, C.; Sherez, J.; Mor, L.; Derakhshesh, M.; Moshkovits, Y.; Merdler, I.; Arbel, Y.; et al. Diastolic strain time as predictor for systolic dysfunction among patients with active breast cancer. Echocardiography 2020, 37, 1890–1896. [Google Scholar] [CrossRef]
- Laufer-Perl, M.; Arias, O.; Dorfman, S.S.; Baruch, G.; Rothschild, E.; Beer, G.; Hasson, S.P.; Arbel, Y.; Rozenbaum, Z.; Topilsky, Y.; et al. Left Atrial Strain changes in patients with breast cancer during anthracycline therapy. Int. J. Caridol. 2021, 330, 238–244. [Google Scholar] [CrossRef]
- Hochstadt, A.; Arnold, J.; Rosen, R.; Sherez, C.; Sherez, J.; Mor, L.; Moshkovits, Y.; Merdler, I.; Szekely, Y.; Arbel, Y.; et al. Longitudinal diastolic strain slope as an early sign for systolic dysfunction among patients with active cancer. Clin. Res. Cardiol. 2021, 110, 569–578. [Google Scholar] [CrossRef]
- Arnold, J.H.; Rozenbaum, Z.; Hochstadt, A.; Rosen, R.; Sherez, C.; Sivan, A.; Mor, L.; Moshkovits, Y.; Sadeh, B.; Havakuk, O.; et al. Diastolic function as an early marker for systolic dysfunction and all-cause mortality among cancer patients. Echocardiography 2021, 38, 540–548. [Google Scholar] [CrossRef]
- Chang, H.M.; Moudgil, R.; Scarabelli, T.; Okwuosa, T.M.; Yeh, E.T.H. Cardiovascular. Cardiovascular Complications of Cancer Therapy: Best Practices in Diagnosis, Prevention, and Management: Part 1. J. Am. Coll. Cardiol. 2017, 70, 2536–2551. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef] [PubMed]
- Teo, S.G.; Yang, H.; Chai, P.; Yeo, T.C. Impact of left ventricular diastolic dysfunction on left atrial volume and function: A volumetric analysis. Eur. J. Echocardiogr. 2010, 11, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Amer. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–788. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Allen, J.; Thomson, J.D.; Lewis, I.J.; Gibbs, J.L. Mitral regurgitation after anthracycline treatment for childhood malignancy. Heart 2001, 85, 430–432. [Google Scholar] [CrossRef] [Green Version]
- Wethal, T.; Lund, M.B.; Edvardsen, T.; Fossa, S.D.; Pripp, A.H.; Holte, H.; Kjekshus, J.; Fossa, A. Valvular dysfunction and left ventricular changes in Hodgkin’s lymphoma survivors. A longitudinal study. Br. J. Cancer 2009, 101, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Van Nimwegen, F.A.; Schaapveld, M.; Janus, C.P.; Krol, A.D.G.; Petersen, E.J.; Raemaekers, J.M.M.; Kok, W.E.M.; Aleman, B.M.P.; Van Leeuwen, F.E. Cardiovascular disease after Hodgkin lymphoma treatment: 40-year disease risk. JAMA Intern. Med. 2015, 175, 1007–1017. [Google Scholar] [CrossRef]
- Mulrooney, D.A.; Yeazel, M.W.; Leisenring, W.M.; Kawashima, T.; Mertens, A.C.; Mitby, P.; Stovall, M.; Donaldson, S.S.; Green, D.M.; Sklar, C.A.; et al. Cardiac outcomes in a cohort of adult survivors of childhood and adolescent cancer: Retrospective analysis of the Childhood Cancer Survivor Study cohort. BMJ 2009, 339, b4606. [Google Scholar] [CrossRef] [Green Version]
- Lange, S.A.; Jung, J.; Jaeck, A.; Hitschold, T.; Ebner, B. Subclinical Myocardial Impairment Occurred in Septal and Anterior LV Wall Segments After Anthracycline-Embedded Chemotherapy and did not Worsen During Adjuvant Trastuzumab Treatment in Breast Cancer Patients. Cardiovasc. Toxicol. 2016, 16, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Oki, T.; Fukuda, N.; Iuchi, A.; Tabata, T.; Yamada, H.; Fukuda, K.; Manabe, K.; Ito, S. Possible mechanisms of mitral regurgitation in dilated hearts: A study using transesophageal echocardiography. Clin. Cardiol. 1996, 19, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.B.; Youn, H.J. Pathophysiology and preventive strategies of anthracycline-induced cardiotoxicity. Korean J. Intern. Med. 2016, 31, 625–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Zhu, Y.; Lin, X.; Fang, L.; Yan, X. Mitral regurgitation after anthracycline-based chemotherapy in an adult patient with breast cancer: A case report. Medicine 2017, 96, e9004. [Google Scholar] [CrossRef]
- Murbraech, K.; Wethal, T.; Smeland, K.B.; Holte, H.; Loge, J.H.; Holte, E.; Rösner, A.; Dalen, H.; Kiserud, C.E.; Aakhus, S. Valvular Dysfunction in Lymphoma Survivors Treated with Autologous Stem Cell Transplantation: A National Cross-Sectional Study. J. Am. Coll. Cardiol. Cardiovasc. Imaging 2016, 9, 230–239. [Google Scholar] [CrossRef]
- Lange, S.A.; Ebner, B.; Wess, A.; Kögel, M.; Gajda, M.; Hitschold, T.; Jung, J. Echocardiography signs of early cardiac impairment in patients with breast cancer and trastuzumab therapy. Clin. Res. Cardiol. 2012, 101, 415–426. [Google Scholar] [CrossRef]
- Bloom, M.W.; Hamo, C.E.; Cardinale, D.; Nohria, A.; Baer, L.; Skopicki, H.; Lenihan, D.J.; Gheorghiade, M.; Lyon, A.R.; Butler, J. Cancer Therapy-Related Cardiac Dysfunction and Heart Failure: Part 1: Definitions, Pathophysiology, Risk Factors, and Imaging. Circ. Heart Fail 2016, 9, e002661. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Baseline Data | |
| Age (years), mean ± SD | 51 ± 12 |
| Weight (kg), median (IQR) | 66 (57–76) |
| Height (cm), mean ± SD | 163 ± 7 |
| BSA (m2), median (IQR) | 1.72 (1.62–1.86) |
| Medical History | |
| Hypertension, n (%) | 25 (18) |
| Diabetes mellitus, n (%) | 16 (11) |
| Hyperlipidemia, n (%) | 19 (14) |
| Smoking (current or past), n (%) | 37 (26) |
| COPD, n (%) | 1 (1) |
| Atrial fibrillation, n (%) | 3 (2) |
| Coronary artery disease, n (%) | 2 (1) |
| CVA/TIA, n (%) | 4 (3) |
| Chemotherapy | |
| Cyclophosphamide, n (%) | 141 (100) |
| Paclitaxel, n (%) | 129 (92) |
| Carboplatin, n (%) | 13 (9) |
| Trastuzumab/pertuzumab, n (%) | 33 (23) |
| Left breast radiation, n (%) | 39 (28) |
| Medications | |
| ACEI/ARB, n (%) | 21 (15) |
| Beta blockers, n (%) | 11 (8) |
| Statins, n (%) | 20 (14) |
| Anti-aggregation, n (%) | 10 (7) |
| Time of Examination | p-Value | ||||
|---|---|---|---|---|---|
| T1 (n = 141) | T2 (n = 141) | T3 (n = 122) | T4 (n = 91) | ||
| LV ejection fraction (%), mean ± SD | 60.2 ± 1.5 | 59.8 ± 1.2 | 59.4 ± 2.1 | 59.2 ± 2.7 | 0.0004 |
| LV ejection fraction <53%, n (%) | 0 (0) | 0 (0) | 4 (3) | 4 (4) | 0.002 |
| LV ejection fraction absolute decrease >10%, n (%) | 2 (1) | 6 (5) | 6 (7) | 0.04 | |
| LV GLS (%), median (IQR) | −21.6 (−20.0–−23.0) | −21.0 (−20.0–−22.7) | −20.0 (−18.9–−21.2) | −20.0 (−19.1–−21.1) | <0.0001 |
| LV end-systolic diameter (mm), median (IQR) | 25 (22–27) | 26 (23–28) | 27 (24–30) | 27 (24–30) | <0.0001 |
| LV end-diastolic diameter (mm), mean ± SD | 44.2 ± 3.6 | 44.5 ± 3.8 | 44.7 ± 3.9 | 45.0 ± 4.0 | 0.36 |
| IVS (mm), mean ± SD | 9.0 ± 1.4 | 9.1 ± 1.9 | 8.9 ± 1.3 | 8.7 ± 1.3 | 0.41 |
| LV mass (g), mean ± SD | 135.7 ± 34 | 136.9 ± 40 | 135.4 ± 32 | 137.1 ± 36 | 0.82 |
| LA volume index (mL/m2), mean ± SD | 28.6 ± 7 | 29.6 ± 9 | 28.2 ± 8 | 29.5 ± 9 | 0.19 |
| Diastolic dysfunction ≥ grade 1, n (%) | 26 (19) | 31 (24) | 34 (28) | 21 (24) | 0.23 |
| Diastolic dysfunction ≥ grade 2, n (%) | 5 (4) | 5 (4) | 6 (5) | 5 (6) | 0.42 |
| E/A ratio, median (IQR) | 1.16 (0.96–1.41) | 1.09 (0.87–1.30) | 1.00 (0.83–1.34) | 1.10 (0.89–1.37) | 0.02 |
| Deceleration time (ms), median (IQR) | 178 (149–203) | 178 (149–207) | 187 (154–209) | 180 (161–216) | 0.43 |
| Wave e’ peak velocity—septal (cm/s), mean ± SD | 8.9 ± 2.6 | 8.1 ± 2.5 | 7.9 ± 2.5 | 8.4 ± 2.7 | 0.0006 |
| Wave e’ peak velocity—lateral (cm/s), mean ± SD | 11.0 ± 2.9 | 10.4 ± 3.3 | 10.1 ± 3.3 | 10.1 ± 3.2 | 0.05 |
| E/e’ ratio average, median (IQR) | 7.8 (6.8–10.1) | 8.0 (6.7–10.1) | 8.0 (6.3–10.0) | 8.0 (6.0–10.8) | 0.63 |
| TAPSE (mm), median (IQR) | 25 (23–27) | 24 (22–27) | 23 (21–24) | 22 (20–26) | <0.0001 |
| SPAP (mmHg), mean ± SD | 26.4 ± 5 | 26.6 ± 6 | 24.9 ± 5 | 26.5 ± 6 | 0.05 |
| Time of Examination | p-Value | ||||
|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | ||
| All Patients n = 141 | n = 141 | n = 141 | n = 122 | n = 91 | |
| Mitral regurgitation ≥ mild, n (%) | 5 (4) | 10 (7) | 14 (12 | 17 (19) | <0.0001 |
| Mitral regurgitation ≥ moderate, n (%) | 1 (1) | 3 (2) | 4 (3) | 3 (3) | 0.13 |
| Tricuspid regurgitation ≥ mild, n (%) | 5 (4) | 8 (6) | 7 (6) | 7 (8) | 0.19 |
| Tricuspid regurgitation ≥ moderate, n (%) | 1 (1) | 1 (1) | 1 (1) | 2 (2) | 0.32 |
| Aortic stenosis ≥ mild, n (%) | 0 | 0 | 0 | 0 | - |
| Mitral stenosis ≥ mild, n (%) | 0 | 0 | 0 | 0 | - |
| Aortic regurgitation ≥ mild, n (%) | 0 | 3 (2) | 1 (1) | 1 (1) | 0.57 |
| Concomitant trastuzumab therapy n = 33 | n = 33 | n = 33 | n = 32 | n = 29 | |
| Mitral regurgitation ≥ mild, n (%) | 2 (6) | 4 (12) | 10 (31) | 9 (31) | 0.003 |
| Mitral regurgitation ≥ moderate, n (%) | 1 (3) | 2 (6) | 3 (9) | 2 (7) | 0.43 |
| Tricuspid regurgitation ≥ mild, n (%) | 2 (6) | 2 (6) | 4 (13) | 4 (14) | 0.21 |
| Tricuspid regurgitation ≥ moderate, n (%) | 1 (3) | 1 (3) | 0 (0) | 1 (3) | 0.86 |
| Aortic regurgitation ≥ mild, n (%) | 0 | 0 | 0 | 0 | - |
| No concomitant trastuzumab therapy n = 108 | n = 108 | n = 108 | n = 90 | n = 62 | |
| Mitral regurgitation ≥ mild, n (%) | 3 (3) | 6 (6) | 4 (4) | 8 (13) | 0.02 |
| Mitral regurgitation ≥ moderate, n (%) | 0 (0) | 1 (1) | 1 (1) | 1 (2) | 0.25 |
| Tricuspid regurgitation ≥ mild, n (%) | 3 (3) | 6 (6) | 3 (3) | 3 (5) | 0.67 |
| Tricuspid regurgitation ≥ moderate, n (%) | 0 (0) | 0 (0) | 1 (1) | 1 (2) | 0.11 |
| Aortic regurgitation ≥ mild, n (%) | 0 (0) | 3 (3) | 1 (1) | 1 (2) | 0.51 |
| Time of Examination | p-Value | ||||
|---|---|---|---|---|---|
| T1 | T2 | T3 | T4 | ||
| n = 5 | n = 10 | n = 14 | n = 17 | ||
| Vena contracta width (mm) (apical view), mean ± SD | 4.5 ± 1.7 | 5.4 ± 2.2 | 4.9 ± 1.6 | 3.7 ± 1.6 | 0.18 |
| Heart rate (beats/min), mean ± SD | 72 ± 11 | 76 ± 9 | 75 ± 13 | 75 ± 12 | 0.95 |
| Systolic blood pressure (mmHg), mean ± SD | 127 ± 26 | 124 ± 19 | 130 ± 27 | 138 ± 19 | 0.67 |
| Diastolic blood pressure (mmHg), mean ± SD | 77 ± 6 | 71 ± 7 | 72 ± 14 | 76 ± 14 | 0.13 |
| Variable | OR (95%CI) | p-Value |
|---|---|---|
| Age (years) | 1.02 (0.94–1.09) | 0.67 |
| Hypertension | 0.51 (0.03–7.36) | 0.62 |
| Diabetes mellitus | 1.22 (0.06–26.1) | 0.90 |
| Hypercholesterolemia | 0.27 (0.01–6.34) | 0.42 |
| Smoking (current or history) | 0.85 (0.18–4.05) | 0.84 |
| Paclitaxel therapy | 0.20 (0.03–1.61) | 0.13 |
| Trastuzumab/pertuzumab therapy | 5.99 (1.35–26.6) | 0.02 |
| Left breast radiation | 3.98 (0.77–20.5) | 0.09 |
| ACE-I/ARB/BB therapy (at T1) | 0.93 (0.06–15.7) | 0.96 |
| Left ventricular global longitudinal strain (at T1) | 1.19 (0.86–1.65) | 0.28 |
| Left ventricular end-diastolic diameter (at T1) (mm) | 1.00 (0.80–1.29) | 0.99 |
| Interventricular septum (at T1) (mm) | 0.96 (0.47–1.96) | 0.91 |
| Diastolic dysfunction (≥grade 1) (at T1) | 1.01 (0.13–7.71) | 0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zahler, D.; Arnold, J.H.; Bar-On, T.; Raphael, A.; Khoury, S.; Rozenbaum, Z.; Banai, S.; Arbel, Y.; Topilsky, Y.; Laufer-Perl, M. Valvular Heart Disease following Anthracycline Therapy—Is It Time to Look beyond Ejection Fraction? Life 2022, 12, 1275. https://doi.org/10.3390/life12081275
Zahler D, Arnold JH, Bar-On T, Raphael A, Khoury S, Rozenbaum Z, Banai S, Arbel Y, Topilsky Y, Laufer-Perl M. Valvular Heart Disease following Anthracycline Therapy—Is It Time to Look beyond Ejection Fraction? Life. 2022; 12(8):1275. https://doi.org/10.3390/life12081275
Chicago/Turabian StyleZahler, David, Joshua H. Arnold, Tali Bar-On, Ari Raphael, Shafik Khoury, Zach Rozenbaum, Shmuel Banai, Yaron Arbel, Yan Topilsky, and Michal Laufer-Perl. 2022. "Valvular Heart Disease following Anthracycline Therapy—Is It Time to Look beyond Ejection Fraction?" Life 12, no. 8: 1275. https://doi.org/10.3390/life12081275