
The Surgical Treatment of Osteoarthritis

 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Background
2. Arthroscopy
2.1. Spine
2.2. Shoulder
2.3. Elbow
2.4. Wrist and Hand
2.5. Hip
2.6. Knee
2.7. Ankle and Foot
3. Preservation
3.1. Spine
3.2. Shoulder
3.3. Elbow
3.4. Wrist and Hand
3.5. Hip
3.6. Knee
3.7. Ankle and Foot
4. Arthrodesis
4.1. Spine
4.2. Shoulder
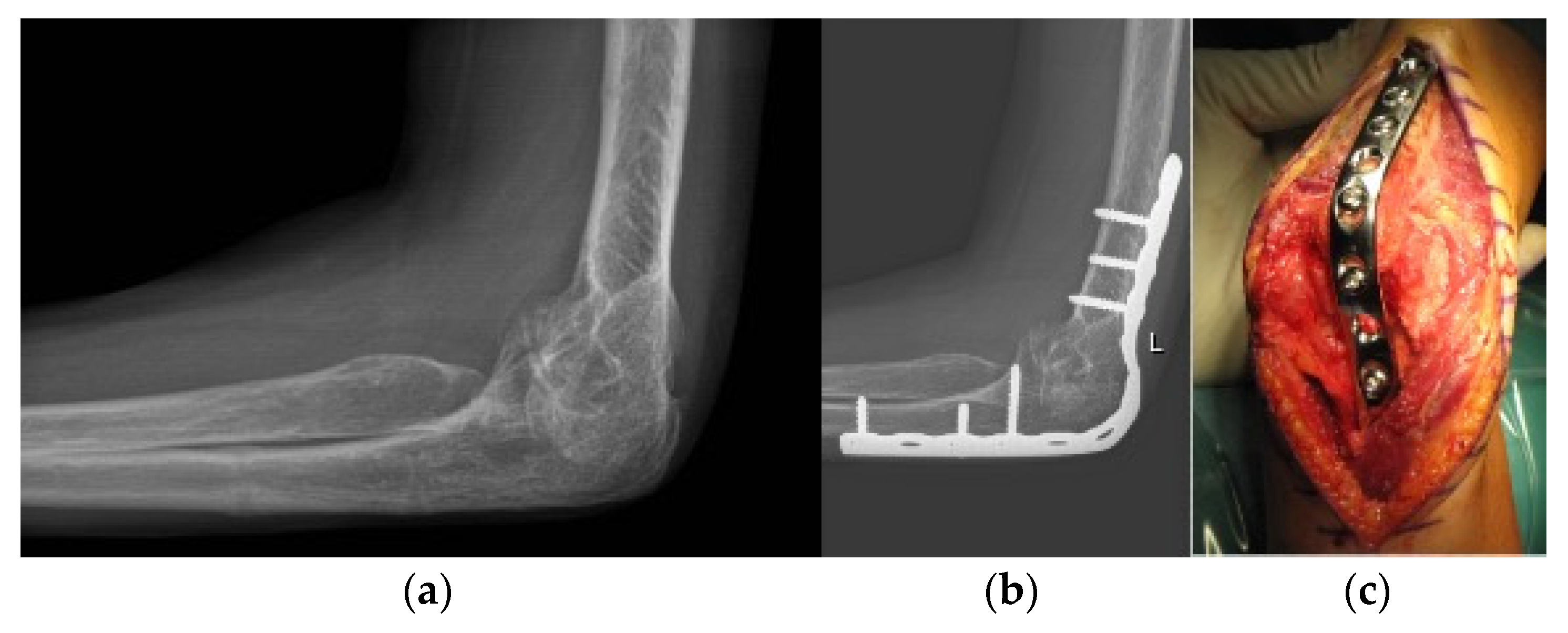
4.3. Elbow
4.4. Wrist and Hand
4.5. Hip
4.6. Knee
4.7. Ankle and Foot
5. Replacement
5.1. Spine
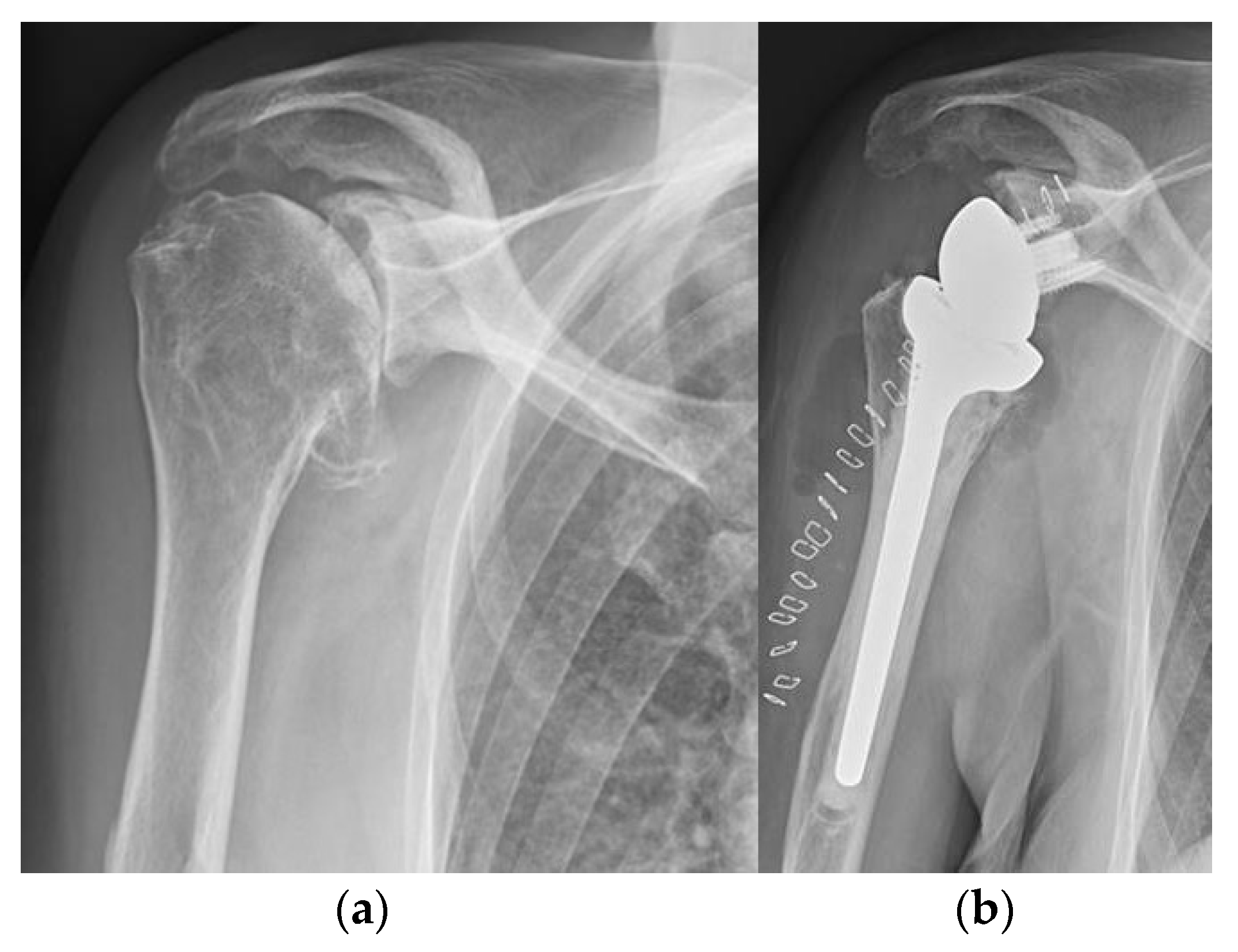
5.2. Shoulder
5.3. Elbow
5.4. Wrist and Hand
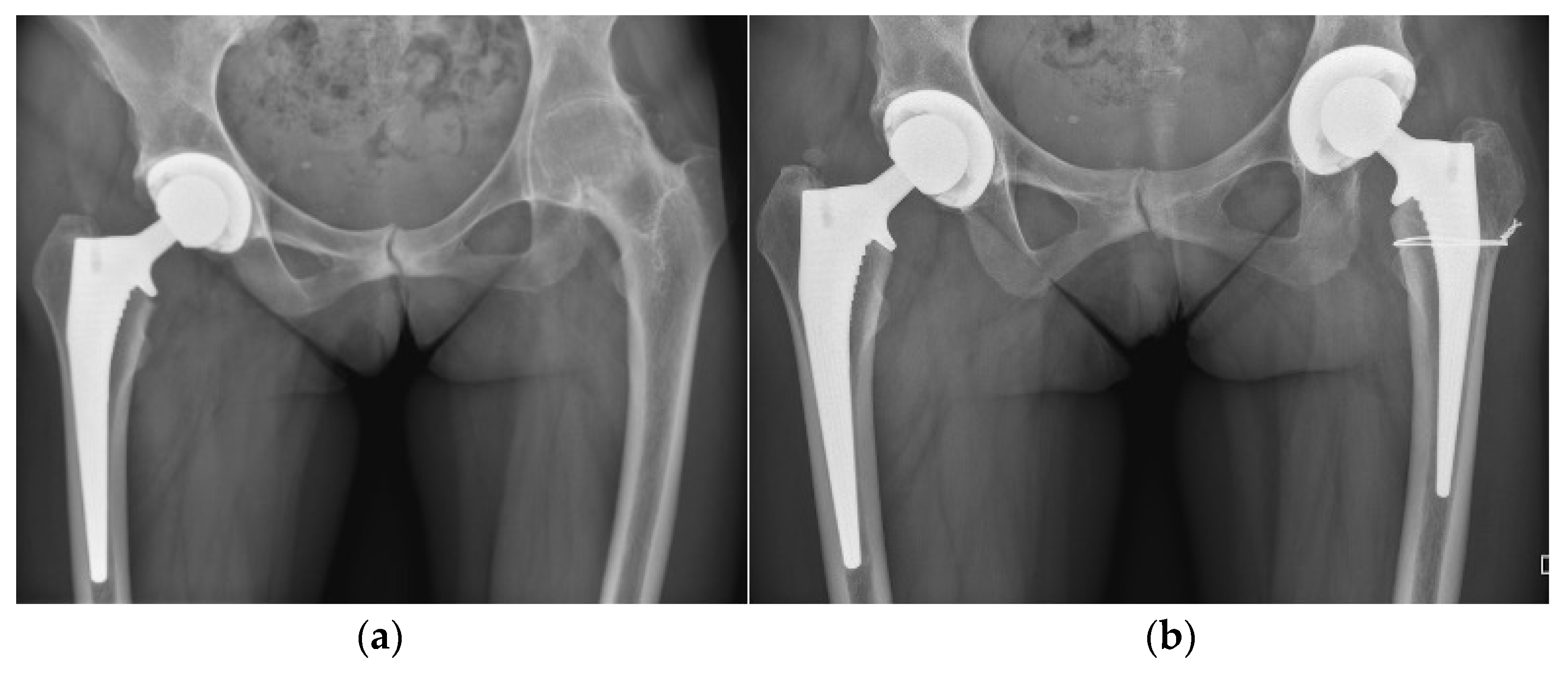
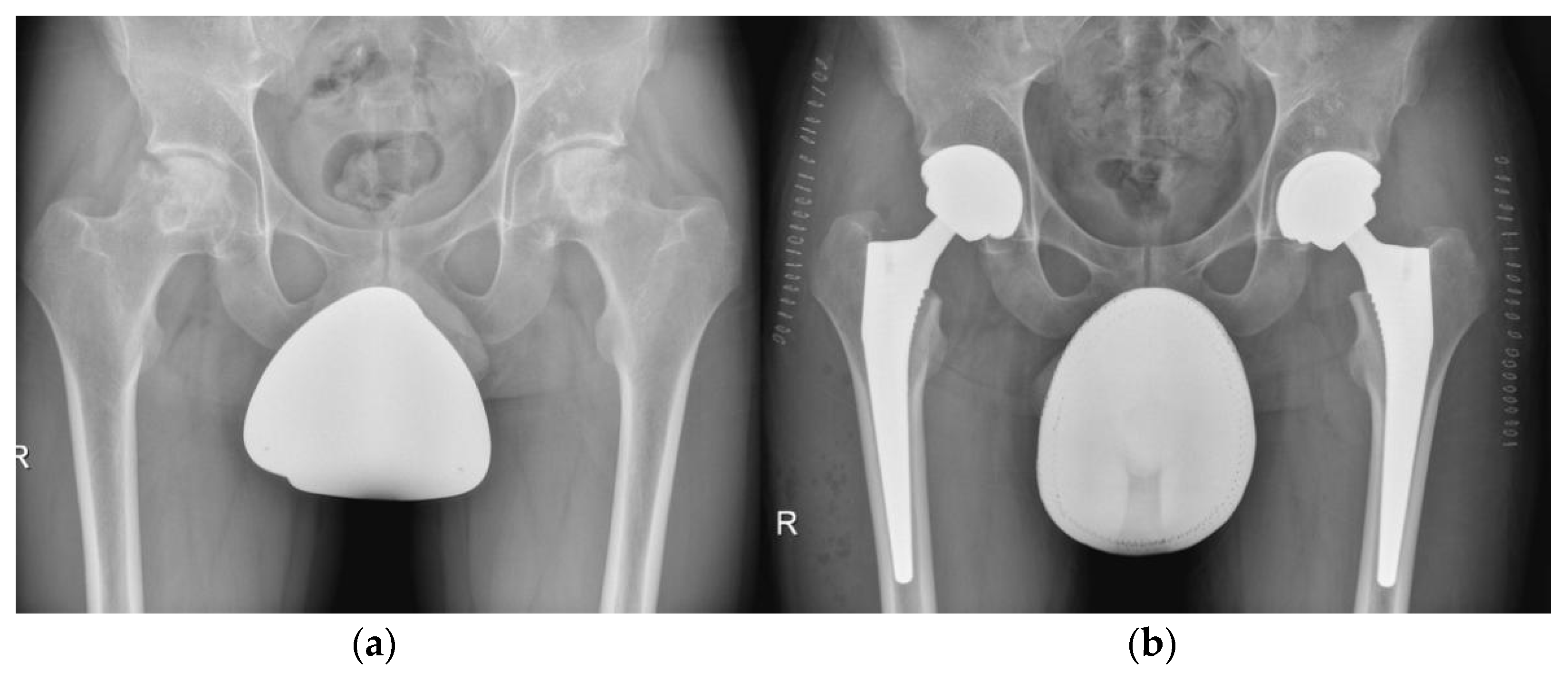
5.5. Hip
5.6. Knee
5.7. Ankle and Foot
6. Computer-Assisted Orthopaedic Surgery
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Glyn-Jones, S.; Palmer, A.J.R.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef]
- Bijlsma, J.W.; Berenbaum, F.; Lafeber, F.P. Osteoarthritis: An Update with Relevance for Clinical Practice. Lancet 2011, 377, 2115–2126. [Google Scholar] [CrossRef]
- Busija, L.; Bridgett, L.; Williams, S.R.M.; Osborne, R.H.; Buchbinder, R.; March, L.; Fransen, M. Osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2010, 24, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Ebell, M.H. Osteoarthritis: Rapid Evidence Review. Am. Fam. Physician 2018, 97, 523–526. [Google Scholar]
- Levesque, J.N.; Shah, A.; Ekhtiari, S.; Yan, J.R.; Thornley, P.; Williams, D.S. Three-Dimensional Printing in Orthopaedic Surgery: A Scoping Review. EFORT Open Rev. 2020, 5, 430–441. [Google Scholar] [CrossRef]
- Goyal, N.D.; Panchnadikar, V.M. A Novel Tracker-Less, Universal, Image-Based, Computer-Assisted Navigation in Orthopaedic Trauma—A Pilot Study. Indian J. Orthop. 2021, 55, 466–472. [Google Scholar] [CrossRef]
- Jud, L.; Fotouhi, J.; Andronic, O.; Aichmair, A.; Osgood, G.; Navab, N.; Farshad, M. Applicability of Augmented Reality in Orthopedic Surgery—A Systematic Review. BMC Musculoskelet. Disord. 2020, 21, 103. [Google Scholar] [CrossRef]
- Simpson, A.K.; Lightsey, H.M.; Xiong, G.X.; Crawford, A.M.; Minamide, A.; Schoenfeld, A.J. Spinal Endoscopy: Evidence, Techniques, Global Trends, and Future Projections. Spine J. 2021, 22, 64–74. [Google Scholar] [CrossRef]
- Van Thiel, G.S.; Sheehan, S.; Frank, R.M.; Slabaugh, M.; Cole, B.J.; Nicholson, G.P.; Romeo, A.A.; Verma, N.N. Retrospective Analysis of Arthroscopic Management of Glenohumeral Degenerative Disease. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2010, 26, 1451–1455. [Google Scholar] [CrossRef]
- Millett, P.J.; Horan, M.P.; Pennock, A.T.; Rios, D. Comprehensive Arthroscopic Management (CAM) Procedure: Clinical Results of a Joint-Preserving Arthroscopic Treatment for Young, Active Patients with Advanced Shoulder Osteoarthritis. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2013, 29, 440–448. [Google Scholar] [CrossRef]
- de Beer, J.F.; Bhatia, D.N.; van Rooyen, K.S.; Du Toit, D.F. Arthroscopic Debridement and Biological Resurfacing of the Glenoid in Glenohumeral Arthritis. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2010, 18, 1767–1773. [Google Scholar] [CrossRef] [PubMed]
- Anderl, W.; Kriegleder, B.; Neumaier, M.; Laky, B.; Heuberer, P. Arthroscopic Partial Shoulder Resurfacing. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2015, 23, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Gobezie, R.; Lenarz, C.J.; Wanner, J.P.; Streit, J.J. All-Arthroscopic Biologic Total Shoulder Resurfacing. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2011, 27, 1588–1593. [Google Scholar] [CrossRef] [PubMed]
- Kroonen, L.T.; Piper, S.L.; Ghatan, A.C. Arthroscopic Management of Elbow Osteoarthritis. J. Hand Surg. 2017, 42, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Laulan, J.; Marteau, E.; Bacle, G. Wrist Osteoarthritis. Orthop. Traumatol. Surg. Res. OTSR 2015, 101, S1–S9. [Google Scholar] [CrossRef] [Green Version]
- Logan, J.S.; Warwick, D. The Treatment of Arthritis of the Wrist. Bone Jt. J. 2015, 97-B, 1303–1308. [Google Scholar] [CrossRef]
- Weiss, N.D.; Molina, R.A.; Gwin, S. Arthroscopic Proximal Row Carpectomy. J. Hand Surg. 2011, 36, 577–582. [Google Scholar] [CrossRef]
- Gottschalk, M.B.; Patel, N.N.; Boden, A.L.; Kakar, S. Treatment of Basilar Thumb Arthritis: A Critical Analysis Review. JBJS Rev. 2018, 6, e4. [Google Scholar] [CrossRef]
- Jamil, M.; Dandachli, W.; Noordin, S.; Witt, J. Hip Arthroscopy: Indications, Outcomes and Complications. Int. J. Surg. 2018, 54, 341–344. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Delcogliano, M.; Giordano, G.; Bonanzinga, T.; Marcacci, M.; Zaffagnini, S. Novel Nano-Composite Multilayered Biomaterial for the Treatment of Patellofemoral Cartilage Lesions. In Patellofemoral Pain, Instability, and Arthritis; Springer: Berlin/Heidelberg, Germany, 2010; pp. 255–262. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Perdisa, F.; Tetta, C.; Di Martino, A.; Marcacci, M. Arthroscopic Mosaicplasty: Long-Term Outcome and Joint Degeneration Progression. Knee 2015, 22, 36–40. [Google Scholar] [CrossRef]
- Sadlik, B.; Wiewiorski, M. Implantation of a Collagen Matrix for an AMIC Repair during Dry Arthroscopy. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2015, 23, 2349–2352. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.S.; Lee, J.H. Arthroscopic Treatment for Osteoarthritic Knee. Knee Surg. Relat. Res. 2012, 24, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavender, C.; Lycans, D.; Sina Adil, S.A.; Kopiec, A.; Schmicker, T. Incisionless Partial Medial Meniscectomy. Arthrosc. Tech. 2020, 9, e375–e378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osti, L.; Del Buono, A.; Maffulli, N. Arthroscopic Debridement of the Ankle for Mild to Moderate Osteoarthritis: A Midterm Follow-up Study in Former Professional Soccer Players. J. Orthop. Surg. 2016, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Coetzee, J.C.; Giza, E.; Schon, L.C.; Berlet, G.C.; Neufeld, S.; Stone, R.M.; Wilson, E.L. Treatment of Osteochondral Lesions of the Talus with Particulated Juvenile Cartilage. Foot Ankle Int. 2013, 34, 1205–1211. [Google Scholar] [CrossRef]
- DeSandis, B.A.; Haleem, A.M.; Sofka, C.M.; O’Malley, M.J.; Drakos, M.C. Arthroscopic Treatment of Osteochondral Lesions of the Talus Using Juvenile Articular Cartilage Allograft and Autologous Bone Marrow Aspirate Concentration. J. Foot Ankle Surg. 2018, 57, 273–280. [Google Scholar] [CrossRef]
- Levaj, I.; Knežević, I.; Dimnjaković, D.; Smoljanović, T.; Bojanić, I. First Metatarsophalangeal Joint Arthroscopy of 36 Consecutive Cases. Acta Chir. Orthop. Traumatol. Cech. 2021, 88, 211–216. [Google Scholar]
- York, P.J.; Wydra, F.B.; Belton, M.E.; Vidal, A.F. Joint Preservation Techniques in Orthopaedic Surgery. Sports Health Multidiscip. Approach 2017, 9, 545–554. [Google Scholar] [CrossRef]
- Kanakamedala, A.C.; Hurley, E.T.; Manjunath, A.K.; Jazrawi, L.M.; Alaia, M.J.; Strauss, E.J. High Tibial Osteotomies for the Treatment of Osteoarthritis of the Knee. JBJS Rev. 2022, 10, e21.00127. [Google Scholar] [CrossRef]
- Murtagh, R.; Castellvi, A.E. Motion Preservation Surgery in the Spine. Neuroimaging Clin. N. Am. 2014, 24, 287–294. [Google Scholar] [CrossRef]
- Bae, D.S.; Waters, P.M. External Rotation Humeral Osteotomy for Brachial Plexus Birth Palsy. Tech. Hand Up. Extrem. Surg. 2007, 11, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, A.; Hirschowitz, D.; Arden, G.P. The Treatment of Arthritis of the Shoulder Joint by Double Osteotomy. Int. Orthop. 1979, 3, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Brooks-Hill, A.L.; Forster, B.B.; van Wyngaarden, C.; Hawkins, R.; Regan, W.D. Weber Osteotomy for Large Hill-Sachs Defects: Clinical and CT Assessments. Clin. Orthop. 2013, 471, 2548–2555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waltenspül, M.; Häller, T.; Ernstbrunner, L.; Wyss, S.; Wieser, K.; Gerber, C. Long-Term Results after Posterior Open Glenoid Wedge Osteotomy for Posterior Shoulder Instability Associated with Excessive Glenoid Retroversion. J. Shoulder Elb. Surg. 2022, 31, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Catalan, N.; Sanchez-Sotelo, J. Primary Elbow Osteoarthritis: Evaluation and Management. J. Clin. Orthop. Trauma 2021, 19, 67–74. [Google Scholar] [CrossRef]
- Kwak, J.-M.; Jeon, I.-H. Surgical Management for Primary Osteoarthritis of the Elbow. J. Orthop. Surg. Hong Kong 2021, 29, 2309499020988174. [Google Scholar] [CrossRef]
- Baghdadi, Y.M.K.; Morrey, B.F.; Sanchez-Sotelo, J. Anconeus Interposition Arthroplasty: Mid- to Long-Term Results. Clin. Orthop. 2014, 472, 2151–2161. [Google Scholar] [CrossRef] [Green Version]
- Kunz, M.; Ma, B.; Rudan, J.F.; Ellis, R.E.; Pichora, D.R. Image-Guided Distal Radius Osteotomy Using Patient-Specific Instrument Guides. J. Hand Surg. 2013, 38, 1618–1624. [Google Scholar] [CrossRef]
- Nacke, E.; Paksima, N. The Evaluation and Treatment of the Arthritic Distal Radioulnar Joint. Bull. Hosp. Jt. Dis. 2015, 73, 141–147. [Google Scholar]
- Hanke, M.S.; Schmaranzer, F.; Steppacher, S.D.; Lerch, T.D.; Siebenrock, K.A. Hip Preservation. EFORT Open Rev. 2020, 5, 630–640. [Google Scholar] [CrossRef]
- Brumat, P.; Mihalič, R.; Kovač, S.; Trebše, R. Acute Femoral Lengthening in Adults Using Step-Cut Osteotomy, Traction Table, and Proximal Femoral Locking Plate Fixation: Surgical Technique and Report of Three Cases. Indian J. Orthop. 2022, 56, 559–565. [Google Scholar] [CrossRef]
- Wolcott, M.; Traub, S.; Efird, C. High Tibial Osteotomies in the Young Active Patient. Int. Orthop. 2010, 34, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomoll, A.H. High Tibial Osteotomy for the Treatment of Unicompartmental Knee Osteoarthritis: A Review of the Literature, Indications, and Technique. Phys. Sportsmed. 2011, 39, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Saragaglia, D.; Sigwalt, L.; Rubens-Duval, B.; Chedal-Bornu, B.; Pailhe, R. Concept of Combined Femoral and Tibial Osteotomies. J. Knee Surg. 2017, 30, 756–763. [Google Scholar] [CrossRef]
- Valderrabano, V.; Horisberger, M.; Russell, I.; Dougall, H.; Hintermann, B. Etiology of Ankle Osteoarthritis. Clin. Orthop. 2009, 467, 1800–1806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chopra, V.; Stone, P.; Ng, A. Supramalleolar Osteotomies. Clin. Podiatr. Med. Surg. 2017, 34, 445–460. [Google Scholar] [CrossRef] [PubMed]
- Colin, F. Tibia Dome-Shaped Osteotomy for a Valgus Deformity in a Ball-AndSocket Ankle Joint: A Case Report. Clin. Res. Foot Ankle 2013, 1, 116. [Google Scholar] [CrossRef]
- Zhao, H.; Liang, X.; Li, Y.; Yu, G.; Niu, W.; Zhang, Y. The Role of Fibular for Supramalleolar Osteotomy in Treatment of Varus Ankle Arthritis: A Biomechanical and Clinical Study. J. Orthop. Surg. 2016, 11, 127. [Google Scholar] [CrossRef] [Green Version]
- Ho, B.; Baumhauer, J. Hallux Rigidus. EFORT Open Rev. 2017, 2, 13–20. [Google Scholar] [CrossRef]
- Reid, J.J.; Johnson, J.S.; Wang, J.C. Challenges to Bone Formation in Spinal Fusion. J. Biomech. 2011, 44, 213–220. [Google Scholar] [CrossRef]
- Rao, P.J.; Pelletier, M.H.; Walsh, W.R.; Mobbs, R.J. Spine Interbody Implants: Material Selection and Modification, Functionalization and Bioactivation of Surfaces to Improve Osseointegration. Orthop. Surg. 2014, 6, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Kamineni, S.; Unger, R.Z.; Desai, R. Shoulder Arthrodesis in the Management of Glenohumeral Pathologies. J. Shoulder Elb. Arthroplast. 2019, 3, 2471549219850655. [Google Scholar] [CrossRef]
- Porcellini, G.; Savoie, F.H.; Campi, F.; Merolla, G.; Paladini, P. Arthroscopically Assisted Shoulder Arthrodesis: Is It an Effective Technique? Arthroscopy 2014, 30, 1550–1556. [Google Scholar] [CrossRef] [PubMed]
- Syal, A.; MacDonald, P. Arthroscopic Arthrodesis of the Shoulder: A Report of Two Cases. J. Shoulder Elb. Surg. 2008, 17, e23–e25. [Google Scholar] [CrossRef] [PubMed]
- Karuppaiah, K. Is There a Role for Elbow Arthrodesis in 21st Century—Current Concepts and Overview of Surgical Techniques. J. Clin. Orthop. Trauma 2021, 20, 101466. [Google Scholar] [CrossRef]
- Dean, B.; Henari, S.; Thurley, N.; Little, C.; McNab, I.; Riley, N. Therapeutic Interventions for Osteoarthritis of the Wrist: A Systematic Review and Meta-Analysis. F1000Research 2018, 7, 1484. [Google Scholar] [CrossRef]
- Giberson-Chen, C.C.; Leland, H.A.; Benavent, K.A.; Harper, C.M.; Earp, B.E.; Rozental, T.D. Functional Outcomes After Sauve-Kapandji Arthrodesis. J. Hand Surg. 2020, 45, 408–416. [Google Scholar] [CrossRef]
- Beaulé, P.E.; Matta, J.M.; Mast, J.W. Hip Arthrodesis: Current Indications and Techniques. J. Am. Acad. Orthop. Surg. 2002, 10, 249–258. [Google Scholar] [CrossRef]
- Wood, J.H.; Conway, J.D. Advanced Concepts in Knee Arthrodesis. World J. Orthop. 2015, 6, 202–210. [Google Scholar] [CrossRef]
- Acquitter, Y.; Hulet, C.; Souquet, D.; Pierre, A.; Locker, B.; Vielpeau, C. Arthroscopic knee arthrodesis: 4 cases. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2004, 90, 65–70. [Google Scholar] [CrossRef]
- Waszczykowski, M.; Niedzielski, K.; Radek, M.; Fabis, J. Arthroscopic-Assisted Arthrodesis of the Knee Joint With the Ilizarov Technique: A Case Report and Literature Review. Medicine 2016, 95, e2540. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Yang, L.; Yin, L. Arthroscopic Arthrodesis for Ankle Arthritis without Bone Graft. J. Orthop. Surg. 2016, 11, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cottino, U.; Collo, G.; Morino, L.; Cosentino, A.; Gallina, V.; Deregibus, M.; Tellini, A. Arthroscopic Ankle Arthrodesis: A Review. Curr. Rev. Musculoskelet. Med. 2012, 5, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Mangwani, J.; Afifi, H.; Faroug, R. Arthroscopic Ankle Arthrodesis—Surgical Technique. J. Arthrosc. Surg. Sports Med. 2021, 2, 135–140. [Google Scholar] [CrossRef]
- Roussignol, X. Arthroscopic Tibiotalar and Subtalar Joint Arthrodesis. Orthop. Traumatol. Surg. Res. OTSR 2016, 102, S195–S203. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, C.N.; Scholten, P.E.; Krips, R. A 2-Portal Endoscopic Approach for Diagnosis and Treatment of Posterior Ankle Pathology. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2000, 16, 871–876. [Google Scholar] [CrossRef]
- Hart, J.A.L. Joint Replacement Surgery. Med. J. Aust. 2004, 180, S27–S30. [Google Scholar] [CrossRef]
- Callanan, G.; Radcliff, K.E. Cervical Total Disc Replacement: Long-Term Outcomes. Update Motion Preserv. Technol. 2021, 32, 461–472. [Google Scholar] [CrossRef]
- Franco, D.; Largoza, G.; Montenegro, T.S.; Gonzalez, G.A.; Hines, K.; Harrop, J. Lumbar Total Disc Replacement: Current Usage. Neurosurg. Clin. N. Am. 2021, 32, 511–519. [Google Scholar] [CrossRef]
- Mattei, L.; Mortera, S.; Arrigoni, C.; Castoldi, F. Anatomic Shoulder Arthroplasty: An Update on Indications, Technique, Results and Complication Rates. Joints 2015, 3, 72–77. [Google Scholar] [CrossRef] [Green Version]
- van den Bekerom, M.P.J.; Geervliet, P.C.; Somford, M.P.; van den Borne, M.P.J.; Boer, R. Total Shoulder Arthroplasty versus Hemiarthroplasty for Glenohumeral Arthritis: A Systematic Review of the Literature at Long-Term Follow-Up. Int. J. Shoulder Surg. 2013, 7, 110–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trofa, D.; Rajaee, S.S.; Smith, E.L. Nationwide Trends in Total Shoulder Arthroplasty and Hemiarthroplasty for Osteoarthritis. Am. J. Orthop. 2014, 43, 166–172. [Google Scholar] [PubMed]
- Zhang, B.; Chen, G.; Fan, T.; Chen, Z. Resurfacing Hemiarthroplasty versus Stemmed Hemiarthroplasty for Glenohumeral Osteoarthritis: A Meta-Analysis. Arthroplasty 2020, 2, 25. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.L.; Barrett, W.P.; Jackins, S.E.; Matsen, F.A. Glenoid Loosening in Total Shoulder Arthroplasty. Association with Rotator Cuff Deficiency. J. Arthroplast. 1988, 3, 39–46. [Google Scholar] [CrossRef]
- Zuckerman, J.D.; Scott, A.J.; Gallagher, M.A. Hemiarthroplasty for Cuff Tear Arthropathy. J. Shoulder Elb. Surg. 2000, 9, 169–172. [Google Scholar] [CrossRef]
- Chawla, H.; Gamradt, S. Reverse Total Shoulder Arthroplasty: Technique, Decision-Making and Exposure Tips. Curr. Rev. Musculoskelet. Med. 2020, 13, 180–185. [Google Scholar] [CrossRef]
- Zhang, D.; Chen, N. Total Elbow Arthroplasty. J. Hand Surg. 2019, 44, 487–495. [Google Scholar] [CrossRef]
- Calcagni, M.; Giesen, T. Distal Radioulnar Joint Arthroplasty with Implants: A Systematic Review. EFORT Open Rev. 2016, 1, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Mellon, S.J.; Liddle, A.D.; Pandit, H. Hip Replacement: Landmark Surgery in Modern Medical History. Maturitas 2013, 75, 221–226. [Google Scholar] [CrossRef]
- Zagra, L. Advances in Hip Arthroplasty Surgery: What Is Justified? EFORT Open Rev. 2017, 2, 171–178. [Google Scholar] [CrossRef]
- Learmonth, I.D.; Young, C.; Rorabeck, C. The Operation of the Century: Total Hip Replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Kovac, S.; Pisot, V.; Trebse, R.; Rotter, A. Fifty-One-Year Survival of a Judet Polymethylmethacrylate Hip Prosthesis. J. Arthroplast. 2004, 19, 664–667. [Google Scholar] [CrossRef]
- Salih, S.; Hamer, A. Hip and Knee Replacement. Surg. Oxf. 2013, 31, 482–487. [Google Scholar] [CrossRef]
- Trebše, R.; Valič, M.; Savarin, D.; Milošev, I.; Levašič, V. Survival Rate of Total Hip Replacements with Matched and with Mixed Components with 10.7 Years Mean Follow-Up. Hip Int. J. Clin. Exp. Res. Hip Pathol. Ther. 2022, 32, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Pizones, J.; García-Rey, E. Pelvic Motion the Key to Understanding Spine–Hip Interaction. EFORT Open Rev. 2020, 5, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Brumat, P.; Pompe, B.; Antolič, V.; Mavčič, B. The Impact of Canal Flare Index on Leg Length Discrepancy after Total Hip Arthroplasty. Arch. Orthop. Trauma Surg. 2018, 138, 123–129. [Google Scholar] [CrossRef]
- Girard, J. Hip Resurfacing: International Perspectives: Review Article. HSS J. 2017, 13, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, D.; Kamath, A.F.; Zingg, P.; Dora, C. Double Mobility Cup Total Hip Arthroplasty in Patients at High Risk for Dislocation: A Single-Center Analysis. Arch. Orthop. Trauma Surg. 2015, 135, 1755–1762. [Google Scholar] [CrossRef]
- Schmitt, J.; Lange, T.; Günther, K.-P.; Kopkow, C.; Rataj, E.; Apfelbacher, C.; Aringer, M.; Böhle, E.; Bork, H.; Dreinhöfer, K.; et al. Indication Criteria for Total Knee Arthroplasty in Patients with Osteoarthritis—A Multi-Perspective Consensus Study. Z. Orthop. Unf. 2017, 155, 539–548. [Google Scholar] [CrossRef]
- Skarpas, G.A.; Karzis, K.; Xifara, A.; Zarokosta, M.; Zoulamoglou, M.; Piperos, T.; Mariolis-Sapsakos, T.; Michos, I.V.; Kazakos, K. The Effect of PCL to Knee Proprioception in TKA: A Prospective Study. Clin. Case Rep. Rev. 2017, 3, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Kolisek, F.R.; McGrath, M.S.; Marker, D.R.; Jessup, N.; Seyler, T.M.; Mont, M.A.; Lowry Barnes, C. Posterior-Stabilized versus Posterior Cruciate Ligament-Retaining Total Knee Arthroplasty. Iowa Orthop. J. 2009, 29, 23–27. [Google Scholar] [PubMed]
- Capella, M.; Dolfin, M.; Saccia, F. Mobile Bearing and Fixed Bearing Total Knee Arthroplasty. Ann. Transl. Med. 2016, 4, 127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niinimäki, T.; Eskelinen, A.; Mäkelä, K.; Ohtonen, P.; Puhto, A.-P.; Remes, V. Unicompartmental Knee Arthroplasty Survivorship Is Lower than TKA Survivorship: A 27-Year Finnish Registry Study. Clin. Orthop. 2014, 472, 1496–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campi, S.; Tibrewal, S.; Cuthbert, R.; Tibrewal, S.B. Unicompartmental Knee Replacement—Current Perspectives. J. Clin. Orthop. Trauma 2018, 9, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Adukia, V.; Mangwani, J.; Issac, R.; Hussain, S.; Parker, L. Current Concepts in the Management of Ankle Arthritis. J. Clin. Orthop. Trauma 2020, 11, 388–398. [Google Scholar] [CrossRef]
- Wąsik, J.; Stołtny, T.; Leksowska-Pawliczek, M.; Pasek, J.; Szcześniak, M.; Ostałowska, A.; Kasperczyk, S.; Koczy, B. Ankle Osteoarthritis—Arthroplasty or Arthrodesis? Ortop. Traumatol. Rehabil. 2018, 20, 361–370. [Google Scholar] [CrossRef]
- Bernasconi, A.; De Franco, C.; Iorio, P.; Smeraglia, F.; Rizzo, M.; Balato, G. Use of Synthetic Cartilage Implant (Cartiva®) for Degeneration of the First and Second Metatarsophalangeal Joint: What Is the Current Evidence? J. Biol. Regul. Homeost. Agents 2020, 34, 15–21. [Google Scholar]
- Smyth, N.A.; Murawski, C.D.; Hannon, C.P.; Kaplan, J.R.; Aiyer, A.A. The Use of a Synthetic Cartilage Implant for Hallux Rigidus: A Systematic Review. Foot Ankle Spec. 2021, 14, 366–371. [Google Scholar] [CrossRef]
- Picard, F.; Deakin, A.H.; Riches, P.E.; Deep, K.; Baines, J. Computer Assisted Orthopaedic Surgery: Past, Present and Future. Med. Eng. Phys. 2019, 72, 55–65. [Google Scholar] [CrossRef]
- Kubicek, J.; Tomanec, F.; Cerny, M.; Vilimek, D.; Kalova, M.; Oczka, D. Recent Trends, Technical Concepts and Components of Computer-Assisted Orthopedic Surgery Systems: A Comprehensive Review. Sensors 2019, 19, 5199. [Google Scholar] [CrossRef] [Green Version]
- Zheng, G.; Nolte, L.P. Computer-Assisted Orthopedic Surgery: Current State and Future Perspective. Front. Surg. 2015, 2, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zdravkovic, V.; Bilic, R. Computer-Assisted Preoperative Planning (CAPP) in Orthopaedic Surgery. Comput. Methods Programs Biomed. 1990, 32, 141–146. [Google Scholar] [CrossRef]
- Hersh, A.; Mahapatra, S.; Weber-Levine, C.; Awosika, T.; Theodore, J.N.; Zakaria, H.M.; Liu, A.; Witham, T.F.; Theodore, N. Augmented Reality in Spine Surgery: A Narrative Review. HSS J. Musculoskelet. J. Hosp. Spec. Surg. 2021, 17, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.D.; Galina, J.; Song, J.; Hasan, S.; Perfetti, D.; Virk, S.; Silber, J.; Essig, D. Impact of Navigation on 30-Day Outcomes for Adult Spinal Deformity Surgery. Glob. Spine J. 2021, 219256822110475. [Google Scholar] [CrossRef]
- Knez, D.; Mohar, J.; Cirman, R.J.; Likar, B.; Pernuš, F.; Vrtovec, T. Variability Analysis of Manual and Computer-Assisted Preoperative Thoracic Pedicle Screw Placement Planning. Spine 2018, 43, 1487–1495. [Google Scholar] [CrossRef]
- Mohar, J. Sacroiliac Fixation with the Aid of a Personalized Navigational Guide in a Patient with Currarino Syndrome. J. Case Rep. Imaging 2020, 4, 100013. [Google Scholar]
- Farshad, M.; Selman, F.; Burkhard, M.D.; Müller, D.; Spirig, J.M. Partial Sacrectomy with Patient-Specific Osteotomy Guides. N. Am. Spine Soc. J. NASSJ 2021, 8, 100090. [Google Scholar] [CrossRef]
- Burns, D.M.; Frank, T.; Whyne, C.M.; Henry, P.D. Glenoid Component Positioning and Guidance Techniques in Anatomic and Reverse Total Shoulder Arthroplasty: A Systematic Review and Meta-Analysis. Shoulder Elb. 2019, 11, 16–28. [Google Scholar] [CrossRef]
- Tanji, A.; Nagura, T.; Iwamoto, T.; Matsumura, N.; Nakamura, M.; Matsumoto, M.; Sato, K. Total Elbow Arthroplasty Using an Augmented Reality-Assisted Surgical Technique. J. Shoulder Elb. Surg. 2022, 31, 175–184. [Google Scholar] [CrossRef]
- Sugiura, Y.; Iwamoto, T.; Suzuki, T.; Kimura, H.; Matsumura, N.; Sato, K.; Nakamura, M.; Matsumoto, M. Computed Tomography-Based Three-Dimensional Preoperative Planning for Total Wrist Arthroplasty. Mod. Rheumatol. Case Rep. 2020, 4, 208–211. [Google Scholar] [CrossRef]
- Brumat, P.; Mihalič, R.; Benulič, Č.; Kristan, A.; Trebše, R. Patient-Specific Template and Electromagnetic Navigation Assisted Bilateral Periacetabular Osteotomy for Staged Correction of Bilateral Injury-Induced Hip Dysplasia: A Case Report. J. Hip Preserv. Surg. 2021, 8, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Shatrov, J.; Parker, D. Computer and Robotic—Assisted Total Knee Arthroplasty: A Review of Outcomes. J. Exp. Orthop. 2020, 7, 70. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; He, P.; Fan, H.; Zhang, C.; Wang, F.; Yang, L. Application of 3D-Printed Personalized Guide in Arthroscopic Ankle Arthrodesis. BioMed Res. Int. 2018, 2018, 3531293. [Google Scholar] [CrossRef] [PubMed] [Green Version]




















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brumat, P.; Kunšič, O.; Novak, S.; Slokar, U.; Pšenica, J.; Topolovec, M.; Mihalič, R.; Trebše, R. The Surgical Treatment of Osteoarthritis. Life 2022, 12, 982. https://doi.org/10.3390/life12070982
Brumat P, Kunšič O, Novak S, Slokar U, Pšenica J, Topolovec M, Mihalič R, Trebše R. The Surgical Treatment of Osteoarthritis. Life. 2022; 12(7):982. https://doi.org/10.3390/life12070982
Chicago/Turabian StyleBrumat, Peter, Ožbej Kunšič, Samo Novak, Urban Slokar, Janez Pšenica, Matevž Topolovec, Rene Mihalič, and Rihard Trebše. 2022. "The Surgical Treatment of Osteoarthritis" Life 12, no. 7: 982. https://doi.org/10.3390/life12070982