
Fatty Acid Composition of Milk from Mothers with Normal Weight, Obesity, or Gestational Diabetes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Milk Samples
2.2. Preparation of Fatty Acid Esters
2.3. Gas Chromatography
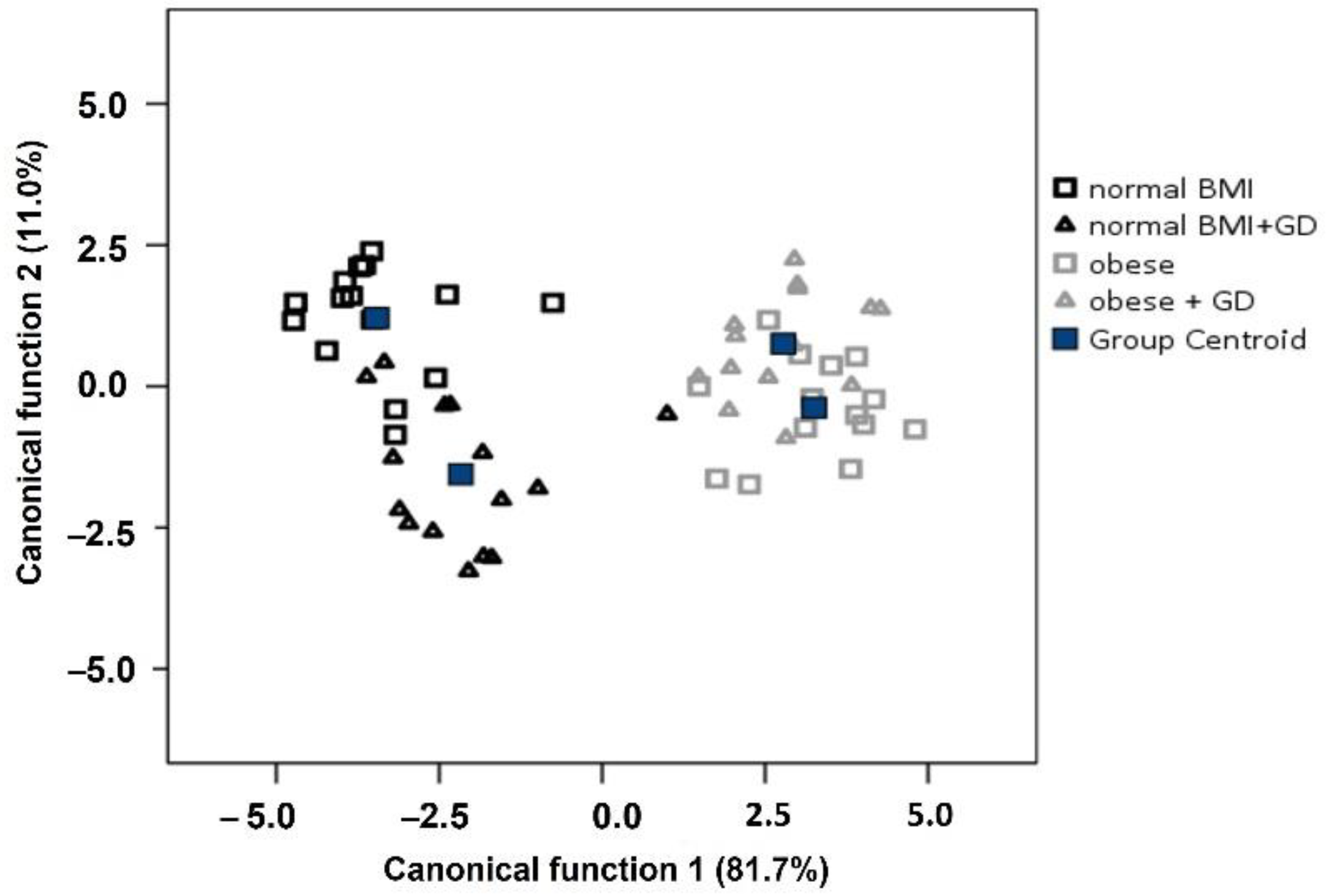
2.4. Statistical Analysis
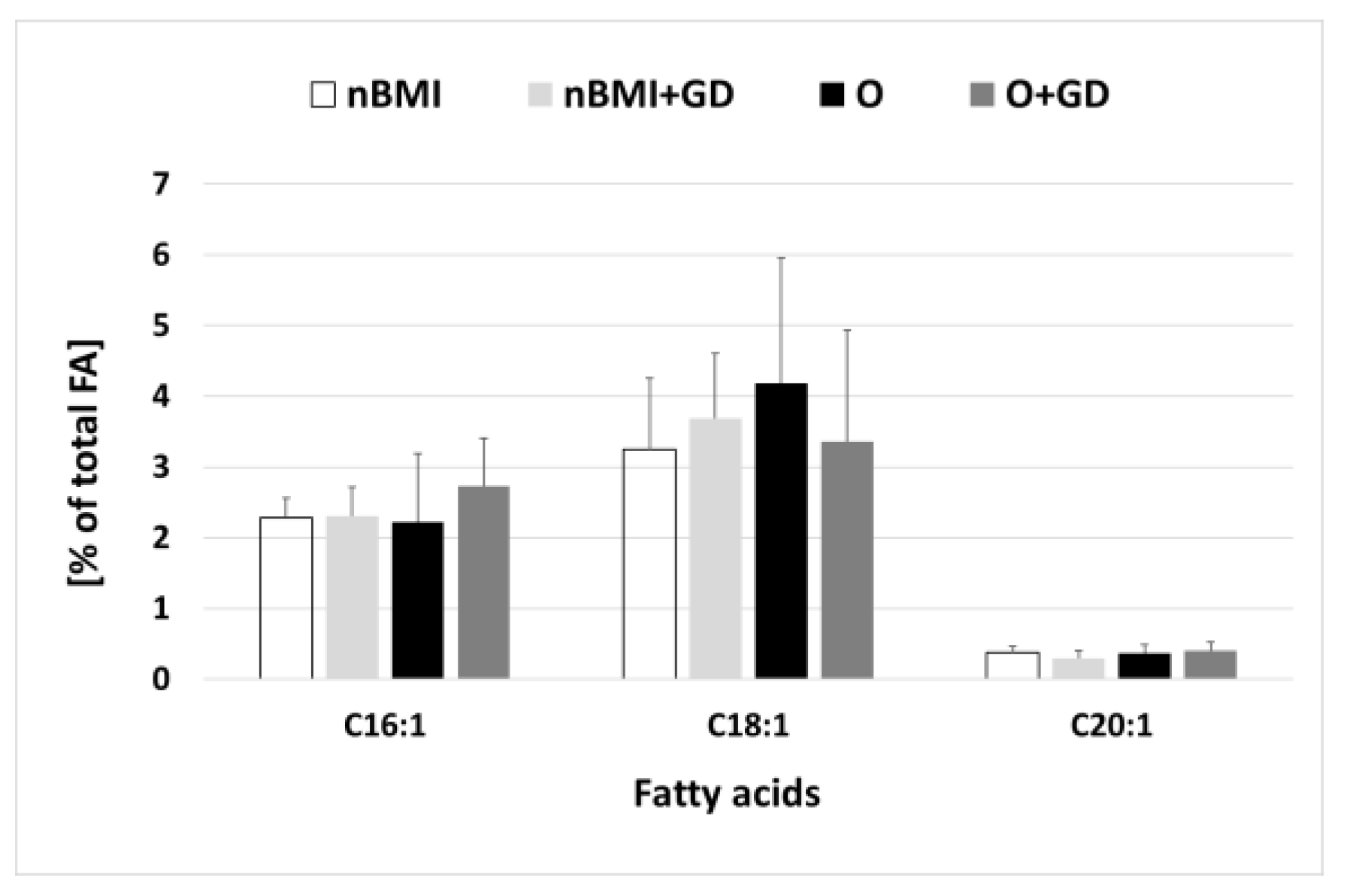
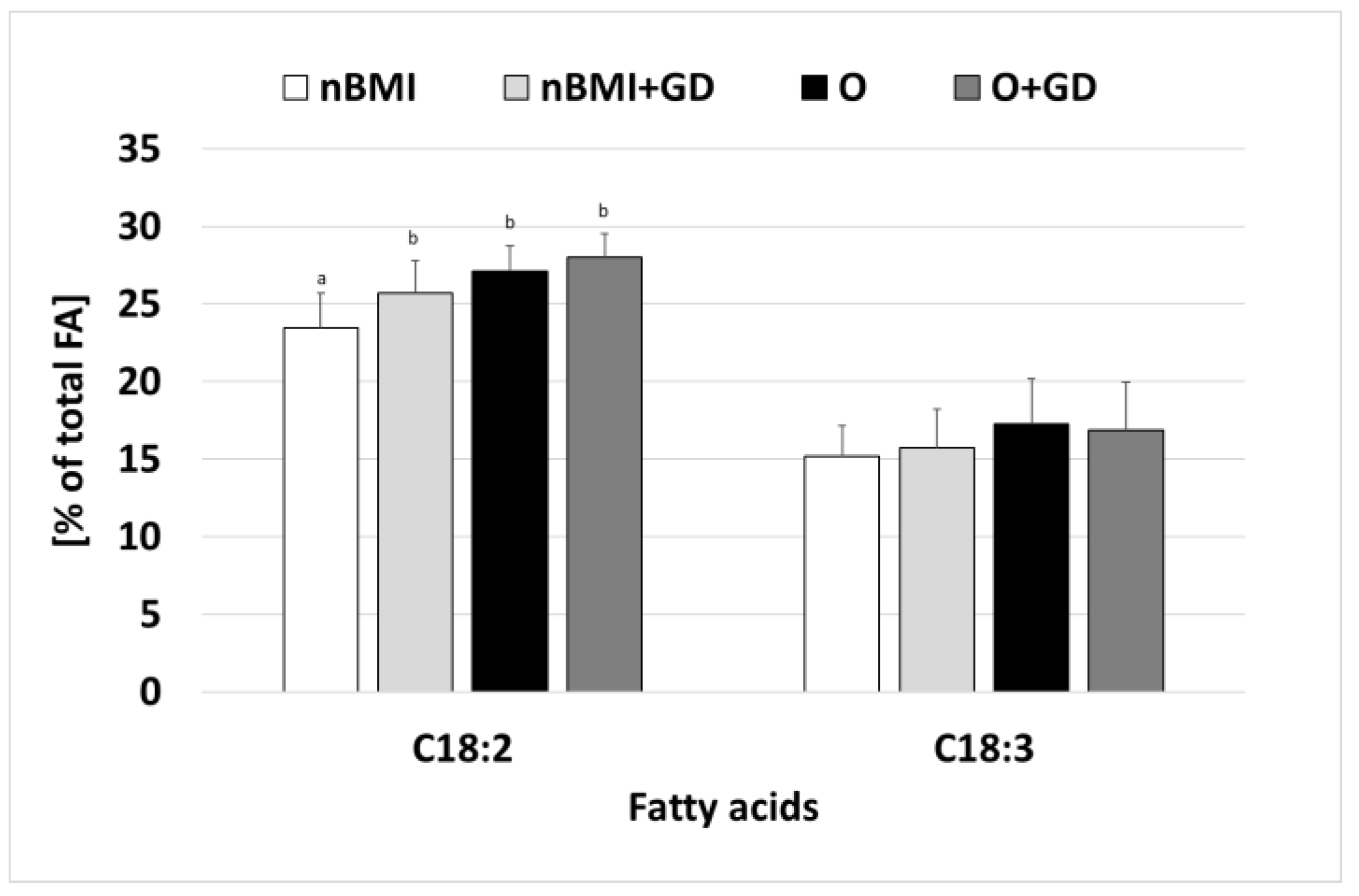
3. Results
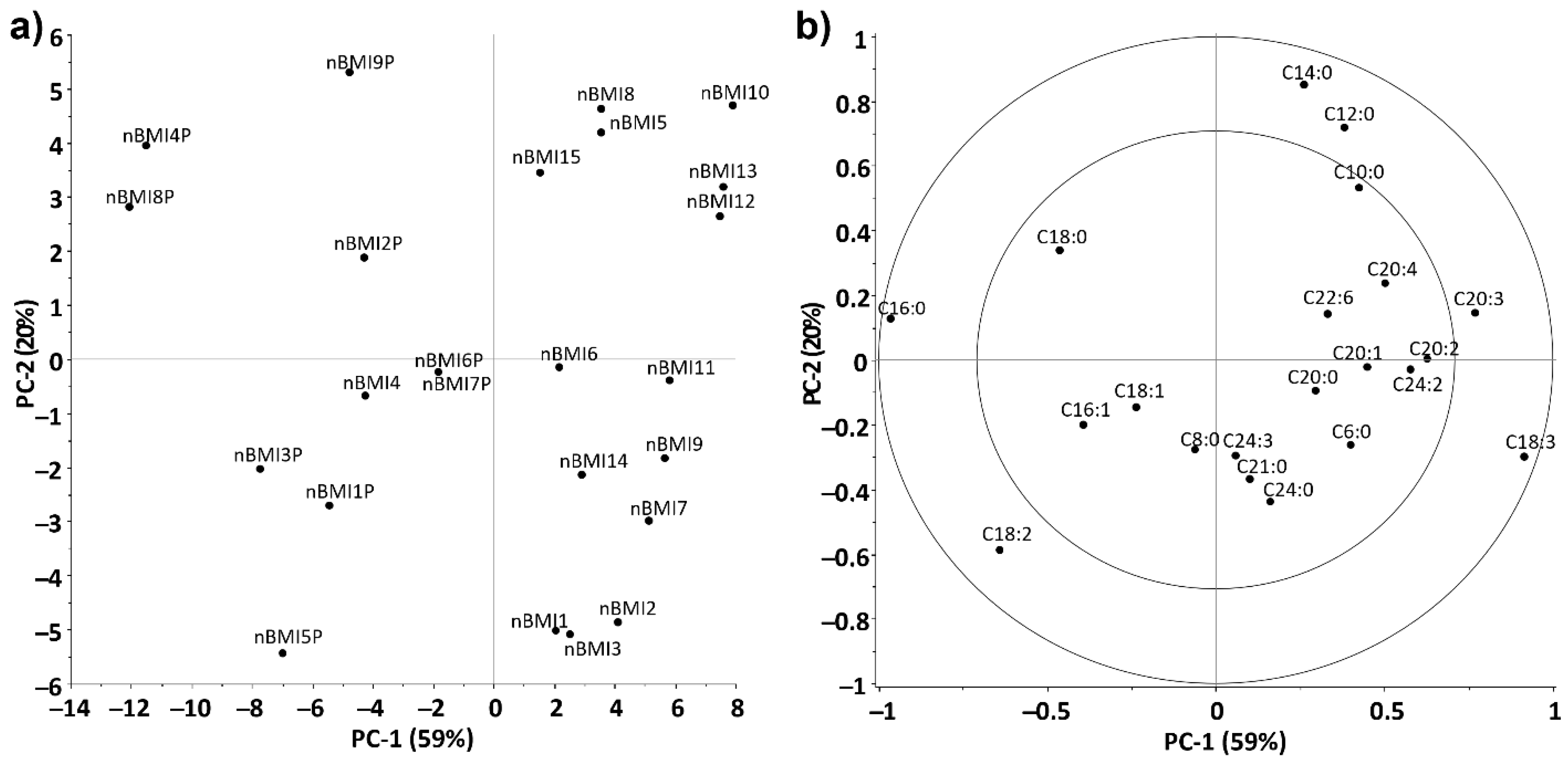
3.1. Statistical Evaluation of Fatty Acid Composition of Ukrainian Breast Milk Samples
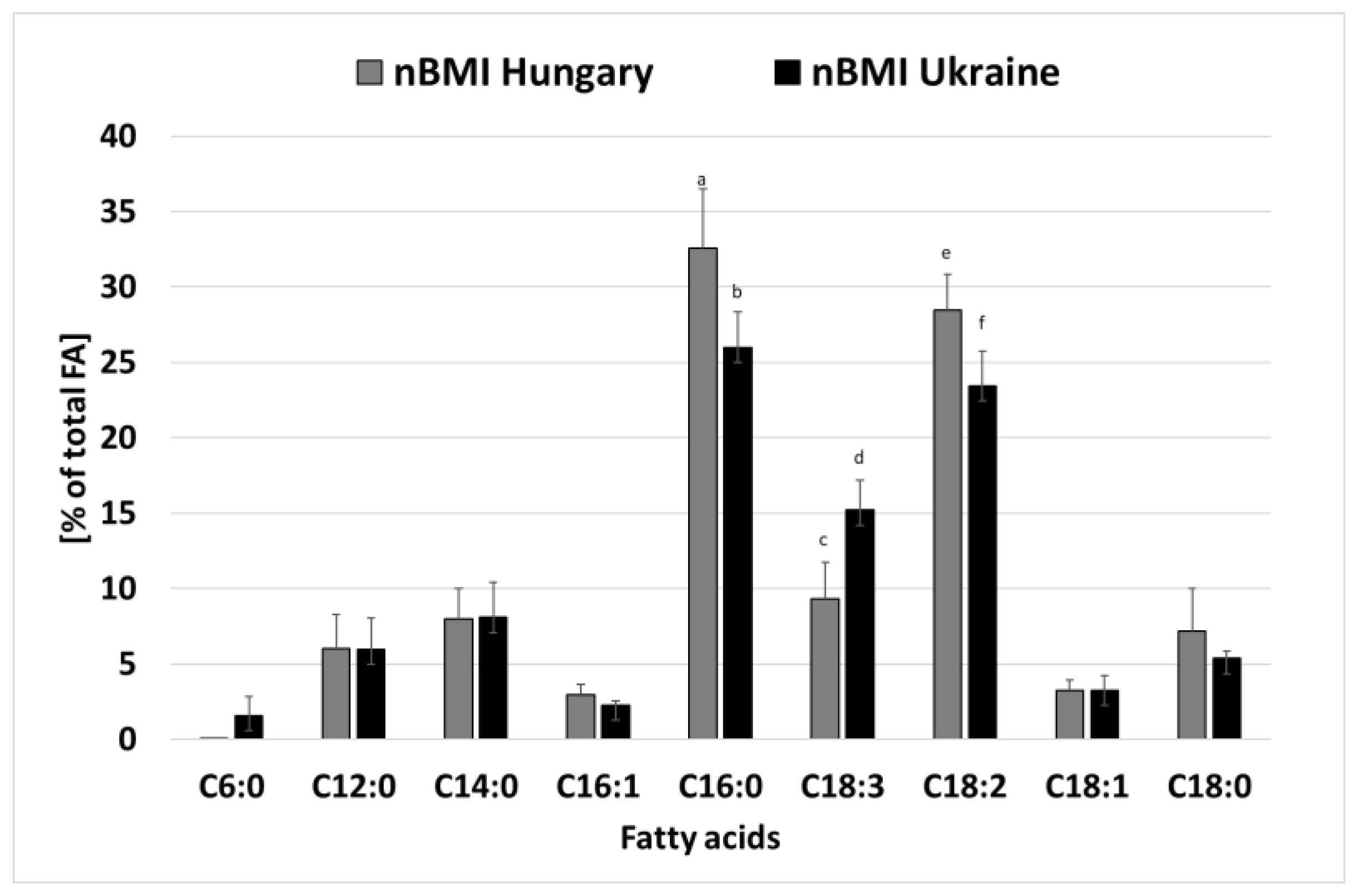
3.2. Comparison of Ukrainian and Hungarian Breastmilk Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vass, R.A.; Roghair, R.D.; Bell, E.F.; Colaizy, T.T.; Schmelzel, M.L.; Johnson, K.J.; Walker, J.R.; Ertl, T. Pituitary glycoprotein hormones in human milk before and after pasteurization or refrigeration. Nutrients 2020, 12, 687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vass, R.A.; Bell, E.F.; Colaizy, T.T.; Schmelzel, M.L.; Johnson, K.J.; Walker, J.R.; Ertl, T.; Roghair, R.D. Hormone levels in preterm and donor human milk before and after Holder pasteurization. Pediatr. Res. 2020, 88, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Vass, R.A.; Kiss, G.; Bell, E.F.; Roghair, R.D.; Miseta, A.; Bódis, J.; Funke, S.; Ertl, T. Breast milk for term and preterm infants-own mother’s milk or donor milk? Nutrients 2021, 13, 424. [Google Scholar] [CrossRef] [PubMed]
- Picciano, M.F. Nutrient composition of human milk. Pediatr. Clin. N. Am. 2001, 48, 53–67. [Google Scholar] [CrossRef]
- Guo, M. Human Milk Biochemistry and Infant Formula Manufacturing Technology, 2nd ed.; Elsevier: Cambridge, MA, USA, 2020; ISBN 9780081028988. [Google Scholar]
- Kim, S.Y.; Yi, D.Y. Components of human breast milk: From macronutrient to microbiome and microRNA. Clin. Exp. Pediatr. 2020, 63, 301–309. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Kang, S.; Jung, B.M.; Yi, H.; Jung, J.A.; Chang, N. Breast milk fatty acid composition and fatty acid intake of lactating mothers in South Korea. Br. J. Nutr. 2017, 117, 556–561. [Google Scholar] [CrossRef] [Green Version]
- Kiprop, V.J.; Girard, A.W.; Gogo, L.A.; Omwamba, M.N.; Mahungu, S.M. Determination of the Fatty Acid Profile of Breast Milk from Nursing Mothers in Bungoma County, Kenya. Food Nutr. Sci. 2016, 7, 661–670. [Google Scholar] [CrossRef] [Green Version]
- Koletzko, B.; Rodriguez-Palmero, M.; Demmelmair, H.; Fidler, N.; Jensen, R.; Sauerwald, T. Physiological aspects of human milk lipids. Early Hum. Dev. 2001, 65, S3–S18. [Google Scholar] [CrossRef]
- Visentainer, J.V.; Santos, O.O.; Maldaner, L.; Zappielo, C.; Neia, V.; Visentainer, L.; Pelissari, L.; Pizzo, J.; Rydlewski, A.; Silveira, R.; et al. Lipids and Fatty Acids in Human Milk: Benefits and Analysis. IntechOpen. 2018. Available online: https://www.intechopen.com/chapters/63140 (accessed on 10 July 2022). [CrossRef] [Green Version]
- German, B.; Dillard, C.J. Composition, Structure and Absorption of Milk Lipids: A Source of Energy, Fat-Soluble Nutrients and Bioactive Molecules. Crit. Rev. Food Sci. Nutr. 2006, 46, 57–92. [Google Scholar] [CrossRef]
- Koletzko, B.; Rodriguez-Palmero, M. Polyunsaturated fatty acids in human milk and their role in early infant development. J. Mammary Gland. Biol. Neoplasia 1999, 4, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Sinanoglou, V.J.; Cavouras, D.; Boutsikou, T.; Briana, D.D.; Lantzouraki, D.Z.; Paliatsiou, S.; Volaki, P.; Bratakos, S.; Malamitsi-Puchner, A.; Zoumpoulakis, P. Factors affecting human colostrum fatty acid profile: A case study. PLoS ONE 2017, 12, e0175817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefkowitz, W.; Lim, S.-Y.; Lin, Y.; Salem, N. Where does the developing brain obtain its docosahexaenoic acid? Relative contributions of dietary alpha linolenic acid, docosahexaenoic acid, and body stores in the developing rat. Pediatr. Res. 2005, 57, 157–165. [Google Scholar] [CrossRef] [Green Version]
- Gibson, R.A.; Muhlhausler, B.; Makrides, M. Conversion of linoleic acid and alpha-linolenic acid to long-chain polyunsaturated fatty acids (LCPUFAs), with a focus on pregnancy, lactation and the first 2 years of life. Matern. Child. Nutr. 2011, 7 (Suppl. 2), 17–26. [Google Scholar] [CrossRef]
- Calder, P.C. Functional roles of fatty acids and their effects on human health. J. Parenter. Enter. Nutr. 2015, 20, 18S–32S. [Google Scholar] [CrossRef]
- Tallima, H.; El Ridi, R. Arachidonic acid: Physiological roles and potential health benefits—A review. J. Adv. Res. 2018, 11, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Halimah, S.N.; Roosita, K.; Briawan, D.; Dewi, M. The Association Between Saturated Fatty Acids (SFAs) Level in Dietary and Blood During Pregnancy and SFAs Level in Breast Milk of Postpartum Mothers. IJSBAR 2021, 60, 93–104. [Google Scholar]
- Innis, S.M. Impact of maternal diet on human milk composition and neurological development of infants. Am. J. Clin. Nutr. 2014, 99, 734S–741S. [Google Scholar] [CrossRef] [Green Version]
- Khor, G.L.; Tan, S.S.; Stoutjesdijk, E.; Ng, K.W.T.; Khouw, I.; Bragt, M.; Schaafsma, A.; Dijck-Brouwer, D.A.J.; Muskiet, F.A.J. Temporal Changes in Breast Milk Fatty Acids Contents: A Case Study of Malay Breastfeeding Women. Nutrients 2021, 13, 101. [Google Scholar] [CrossRef]
- Lassek, W.D.; Gaulin, S.J. Linoleic and docosahexaenoic acids in human milk have opposite relationships with cognitive test performance in a sample of 28 countries. Prostagland. Leukot. Essent. Fatty Acids 2014, 91, 195–201. [Google Scholar] [CrossRef]
- Bernard, J.Y.; Armand, M.; Garcia, C.; Forhan, A.; Agostini, M.; Charles, M.-A.; Heude, B. The association between linoleic acid levels in colostrum and child cognition at 2 and 3 years in the EDEN cohort. Pediatr. Res. 2015, 77, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Bernard, J.Y.; Armand, M.; Peyre, H.; Garcia, C.; Forhan, A.; Agostini, M.; Charles, M.-A.; Heude, B. Breastfeeding, polyunsaturated fatty acid levels in colostrum and child intelligence quotient at age 5–6 years. J. Pediatr. 2017, 183, 43.e3–50.e3. [Google Scholar] [CrossRef] [PubMed]
- Hopperton, K.E.; Pitino, M.A.; Walton, K.; Kiss, A.; Unger, S.L.; O’Connor, D.L.; Bazinet, R.P. Docosahexaenoic acid and arachidonic acid levels are correlated in human milk: Implications for new European infant formula regulations. Lipids 2022, 57, 197–202. [Google Scholar] [CrossRef]
- Schipper, L.; Dijk, G.; Beek, E.M. Milk lipid composition and structure; The relevance for infant brain development. OCL 2020, 27, 5. [Google Scholar] [CrossRef] [Green Version]
- Hachey, D.L.; Silber, G.H.; Wong, W.W.; Garza, C. Human lactation II: Endogenous fatty acid synthesis by the mammary gland. Pediatr. Res. 1989, 25, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, R.; Bitman, J.; Carlson, S.; Couch, S.; Hamosh, M.; Newburg, D.S. Human milk lipids. In Handbook of Milk Composition; Jensen, R., Ed.; Academic Press: London, UK, 1995; pp. 495–573. ISBN 9780080533117. [Google Scholar]
- Thompson, B.J.; Smith, S. Biosynthesis of fatty acids by lactating human breast epithelial cells: An evaluation of the contribution to the overall composition of human milk fat. Pediatr. Res. 1985, 19, 139–143. [Google Scholar] [CrossRef] [Green Version]
- Nasser, R.; Stephen, A.M.; Goh, Y.K.; Clandinin, M.T. The effect of a controlled manipulation of maternal dietary fat intake on medium and long chain fatty acids in human breast milk in Saskatoon, Canada. Int. Breastfeed. J. 2010, 5, 3. [Google Scholar] [CrossRef] [Green Version]
- Gardner, A.S.; Rahman, I.A.; Lai, C.T.; Hepworth, A.; Trengove, N.; Hartmann, P.E.; Geddes, D.T. Changes in fatty acid composition of human milk in response to cold-like symptoms in the lactating mother and infant. Nutrients 2017, 9, 1034. [Google Scholar] [CrossRef]
- Innis, S.M. Human milk: Maternal dietary lipids and infant development. Proc. Nutr. Soc. 2007, 66, 397–404. [Google Scholar] [CrossRef]
- Guillocheau, E.; Legrand, P.; Rioux, V. Benefits of natural dietary trans fatty acids towards inflammation, obesity and type 2 diabetes: Defining the n-7 trans fatty acid family. OCL 2019, 26, 46. [Google Scholar] [CrossRef] [Green Version]
- Pipoyan, D.; Stepanyan, S.; Stepanyan, S.; Beglaryan, M.; Costantini, L.; Molinari, R.; Merendino, N. The Effect of Trans Fatty Acids on Human Health: Regulation and Consumption Patterns. Foods 2021, 10, 2452. [Google Scholar] [CrossRef]
- Aumeistere, L.; Beluško, A.; Ciproviča, I.; Zavadska, D. Trans Fatty Acids in Human Milk in Latvia: Association with Dietary Habits during the Lactation Period. Nutrients 2021, 13, 2967. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Rifas-Shiman, S.L.; Rimm, E.B.; Oken, E.; Gillman, M.W. Maternal trans fatty acid intake and fetal growth. Am. J. Clin. Nutr. 2011, 94, 1241–1247. [Google Scholar] [CrossRef]
- Koletzko, B. Human milk lipids. Ann. Nutr. Metab. 2016, 69 (Suppl. 2), 28–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lien, E.L.; Boyle, F.G.; Yuhas, R.; Tomarelli, R.M.; Quinlan, P. The effect of triglyceride positional distribution on fatty acid absorption in rats. J. Pediatr. Gastroenterol. Nutr. 1997, 25, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Peleg-Raibstein, D. Understanding the Link Between Maternal Overnutrition, Cardio-Metabolic Dysfunction and Cognitive Aging. Front. Neurosci. 2021, 15, 645569. [Google Scholar] [CrossRef]
- Matsyura, O.; Besh, L.; Borysiuk, O.; Gutor, T.; Malska, A.; Kovalska, O.; Besh, O.; Sorokopud, O.; Vari, S.G. Food Hypersensitivity in Children Aged 0–3 Years of the Lviv Region in Ukraine: A Cross-Sectional Study. Front. Pediatr. 2022, 9, 800331. [Google Scholar] [CrossRef]
- Rodriguez, M.; Koletzko, B.; Kunz, C.; Jensen, R. Nutritional and Biochemical Properties of Human Milk, Part II. Lipids, Micronutrients and Active factors. Clin. Perinatol. 1999, 26, 335–359. [Google Scholar] [CrossRef]
- Smit, E.N.; Martini, I.A.; Mulder, H.; Boersma, E.R.; Muskiet, F.A.J. Estimated biological variation of the mature human milk fatty acid composition. Prostaglandins Leukot. Essent. Fat. Acids 2002, 66, 549–555. [Google Scholar] [CrossRef]
- Mitoulas, L.R.; Gurrin, L.C.; Doherty, D.A.; Sherriff, J.L.; Hartmann, P.E. Infant Intake of Fatty Acids from Human Milk over the First Year of Lactation. Br. J. Nutr. 2003, 90, 979–986. [Google Scholar] [CrossRef] [Green Version]
- Amaral, Y.; Silva, L.; Soares, F.; Marano, D.; Nehab, S.; Abranches, A.; Costa, A.C.; Moreira, M.E. What are the Maternal Factors that Potentially Intervenes in the Nutritional Composition of Human Milk? Nutrients 2021, 13, 1587. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Liu, X.; Wang, L. The investigation of fatty acid composition of breast milk and its relationship with dietary fatty acid intake in 5 regions of China. Medicine 2019, 98, 24. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Gestational Diabetes Mellitus. Diabetes Care 2003, 26, S103–S105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, T.A.; Xiang, A.; Kjos, S.L.; Watanabe, R. What is gestational diabetes? Diabetes Care 2007, 30, S105–S111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalano, P.M.; Kirwan, J.P.; Haugel-de Mouzon, S.; King, J. Gestational diabetes and insulin resistance: Role in short- and long-term implications for mother and fetus. J. Nutr. 2003, 133, 1674S–1683S. [Google Scholar] [CrossRef]
- Wijendran, V.; Bendel, R.B.; Couch, S.; Philipson, E.H.; Cheruku, S.; Lammi-Keefe, C.J. Fetal erythrocyte phospholipid polyunsaturated fatty acids are altered in pregnancy complicated with gestational diabetes mellitus. Lipids 2000, 35, 927–931. [Google Scholar] [CrossRef]
- Jackson, M.B.; Lammi-Keefe, C.J.; Jensen, R.G.; Couch, S.C.; Ferris, A.M. Total lipid and fatty acid composition of milk from women with and without insulin-dependent diabetes mellitus. Am. J. Clin. Nutr. 1994, 60, 353–361. [Google Scholar] [CrossRef]
- Peila, C.; Gazzolo, D.; Bertino, E.; Cresi, F.; Coscia, A. Influence of Diabetes during Pregnancy on Human Milk Composition. Nutrients 2020, 12, 185. [Google Scholar] [CrossRef] [Green Version]
- Muuse, B.G.; Werdmuller, G.A.; Geerts, J.P.; De Knegt, R.J. Fatty acid profile of Dutch butterfat. Neth. Milk Dairy J. 1986, 40, 189–201. [Google Scholar]
- Ramiro-Cortijo, D.; Singh, P.; Liu, Y.; Medina-Morales, E.; Yakah, W.; Freedman, S.D.; Martin, C.R. Breast Milk Lipids and Fatty Acids in Regulating Neonatal Intestinal Development and Protecting against Intestinal Injury. Nutrients 2020, 12, 534. [Google Scholar] [CrossRef] [Green Version]
- Giuffrida, F.; Fleith, M.; Goyer, A.; Samuel, T.M.; Elmelegy-Masserey, I.; Fontannaz, P.; Cruz-Hernandez, C.; Thakkar, S.K.; Monnard, C.; De Castro, C.A.; et al. Human milk fatty acid composition and its association with maternal blood and adipose tissue fatty acid content in a cohort of women from Europe. Eur. J. Nutr. 2022, 61, 2167–2182. [Google Scholar] [CrossRef] [PubMed]
- Demmelmair, H.; Koletzko, B. Detailed knowledge of maternal and infant factors and human milk composition could inform recommendations for optimal composition. Acta Paediatr. 2022, 111, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, J.; Macedo Da Costa, T.H.; Ito, M.K. Influences of maternal dietary intake and suckling on breast milk lipid and fatty acid composition in low-income women from Brasilia. Braz. Early Hum. Dev. 2005, 81, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Fidler, N.; Koletzko, B. The fatty acid composition of human colostrum. Eur. J. Nutr. 2000, 39, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Bitman, J.; Hamosh, M.; Hamosh, P. Milk composition and volume during the onset of lactation in a diabetic mother. Am. J. Clin. Nutr. 1989, 50, 1364–1369. [Google Scholar] [CrossRef] [Green Version]
- Roopashree, P.G.; Shetty, S.S.; Kumari, N.S. Effect of medium chain fatty acid in human health and disease. J. Funct. Foods 2021, 87, 104724. [Google Scholar] [CrossRef]
- Floris, L.M.; Stahl, B.; Abrahamse-Berkeveld, M.; Teller, I.C. Human milk fatty acid profile across lactational stages after term and preterm delivery: A pooled data analysis. Prostagland Leukot. Essent. Fatty Acids 2020, 156, 102023. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Hernández, S.; Esteban-Muñoz, A.; Giménez-Martínez, R.; Aguilar-Cordero, M.J.; Miralles-Buraglia, B.; Olalla-Herrera, M. A Comparison of Changes in the Fatty Acid Profile of Human Milk of Spanish Lactating Women during the First Month of Lactation Using Gas Chromatography-Mass Spectrometry. A Comparison with Infant Formulas. Nutrients 2019, 11, 3055. [Google Scholar] [CrossRef] [Green Version]
- Garaulet, M.; Hernandez-Morante, J.J.; Tebar, F.J.; Zamora, S. Relation between degree of obesity and site-specific adipose tissue fatty acid composition in a Mediterranean population. Nutrition 2011, 27, 170–176. [Google Scholar] [CrossRef]
- de la Garza Puentes, A.; Martí Alemany, A.; Chisaguano, A.M.; Montes Goyanes, R.; Castellote, A.I.; Torres-Espínola, F.J.; García-Valdés, L.; Escudero-Marín, M.; Segura, M.T.; Campoy, C.; et al. The Effect of Maternal Obesity on Breast Milk Fatty Acids and Its Association with Infant Growth and Cognition—The PREOBE Follow-Up. Nutrients 2019, 11, 2154. [Google Scholar] [CrossRef] [Green Version]
- López-López, A.; López-Sabater, M.; Campoy-Folgoso, C.; Rivero-Urgell, M.; Castellote-Bargalló, A. Fatty acid and sn-2 fatty acid composition in human milk from Granada (Spain) and in infant formulas. Eur. J. Clin. Nutr. 2002, 56, 1242–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyall, S.C.; Michael-Titus, A.T. Neurological benefits of omega-3 fatty acids. Neuromolecular Med. 2008, 10, 219–235. [Google Scholar] [CrossRef] [PubMed]
- Garbagnati, F.; Cairella, G.; De Martino, A.; Multari, M.; Scognamiglio, U.; Venturiero, V.; Paolucci, S. Is antioxidant and n-3 supplementation able to improve functional status in poststroke patients? Results from the Nutristroke Trial. Cerebrovasc. Dis. 2009, 27, 375–383. [Google Scholar] [CrossRef]
- Bromfield, E.; Dworetzky, B.; Hurwitz, S.; Eluri, Z.; Lane, L.; Replansky, S.; Mostofsky, D. A randomized trial of polyunsaturated fatty acids for refractory epilepsy. Epilepsy Behav. 2008, 12, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Wijendran, V.; Brenna, J.T.; Wang, D.H.; Zhu, W.; Meng, D.; Ganguli, K.; Kothapalli, K.S.; Requena, P.; Innis, S.; Walker, W.A. Long-chain polyunsaturated fatty acids attenuate the IL-1beta-induced proinflammatory response in human fetal intestinal epithelial cells. Pediatr. Res. 2015, 78, 626–633. [Google Scholar] [CrossRef] [Green Version]
- Whiting, C.V.; Bland, P.W.; Tarlton, J.F. Dietary n-3 polyunsaturated fatty acids reduce disease and colonic proinflammatory cytokines in a mouse model of colitis. Inflamm. Bowel Dis. 2005, 11, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, K.; Hoppu, U.; Hamalainen, M.; Linderborg, K.; Moilanen, E.; Isolauri, E. Breast milk fatty acids may link innate and adaptive immune regulation: Analysis of soluble CD14, prostaglandin E2, and fatty acids. Pediatr. Res. 2006, 59, 723–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbige, L.S. Fatty acids, the immune response, and autoimmunity: A question of n−6 essentiality and the balance between n-6 and n-3. Lipids 2003, 38, 323–341. [Google Scholar] [CrossRef]
- Isesele, P.; Enstad, S.; Huong, P.; Thomas, R.; Wagner, C.L.; Sen, S.; Cheema, S.K. Breast Milk from Non-Obese Women with a High Omega-6 to Omega-3 Fatty Acid Ratio, but Not from Women with Obesity, Increases Lipogenic Gene Expression in 3T3-L1 Preadipocytes, Suggesting Adipocyte Dysfunction. Biomedicines 2022, 10, 1129. [Google Scholar] [CrossRef]
- Sprecher, H. Metabolism of highly unsaturated n-3 and n-6 fatty acids. Biochim. Biophys. Acta Mol. Cell Biol. Lipids 2000, 1486, 219–231. [Google Scholar] [CrossRef]
- Saito, E.; Okada, T.; Abe, Y.; Odaka, M.; Kuromori, Y.; Iwata, F.; Hara, M.; Mugishima, H.; Kitamura, Y. Abdominal adiposity is associated with fatty acid desaturase activity in boys: Implications for C-reactive protein and insulin resistance. Prostaglandins Leukot. Essent. Fat. Acids 2013, 88, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Wolters, M.; Schlenz, H.; Börnhorst, C.; Risé, P.; Galli, C.; Moreno, L.A.; Pala, V.; Siani, A.; Veidebaum, T.; Tornaritis, M. Desaturase activity is associated with weight status and metabolic risk markers in young children. J. Clin. Endocrinol. Metab. 2015, 100, 3760–3769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vernon, R. Endocrine control of metabolic adaptation during lactation. Proc. Nutr. Soc. 1989, 48, 23–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.; Tsai, M.Y.; Sun, Q.; Hinkle, S.N.; Rawal, S.; Mendola, P.; Ferrara, A.; Albert, P.S.; Zhang, C. A prospective and longitudinal study of plasma phospholipid saturated fatty acid profile in relation to cardiometabolic biomarkers and the risk of gestational diabetes. Am. J. Clin. Nutr. 2018, 107, 1017–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covaciu, F.D.; Feher, I.; Molnar, C.; Floare-Avram, V.; Dehelean, A. Characterization of the Fatty Acid and Elemental Composition of Human Milk with Chemometric Processing to Determine the Nutritional Value. Anal. Lett. 2022, 55. [Google Scholar] [CrossRef]
- Lowensohn, R.I.; Stadler, D.D.; Naze, C. Current Concepts of Maternal Nutrition. Obstet. Gynecol. Surv. 2016, 71, 413–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Normal BMI * | Normal BMI * with GD | Obese | Obese with GD | |
|---|---|---|---|---|
| Number of involved mothers | 24 | 15 | 15 | 15 |
| Maternal age (years) | 27.1 ± 1.2 | 27.8 ± 1.3 | 26.3 ± 1.2 | 30.7 ± 1.8 |
| Gestational age (weeks) | 39.5 ± 0.6 | 38.2 ± 0.2 | 37.8 ± 0.2 | 39.6 ± 0.4 |
| Maternal BMI at delivery | 23.4 ± 0.3 a | 23.1 ± 0.4 a | 31.5 ± 0.6 b | 32.5 ± 0.5 c |
| Sex of neonate | ||||
| Female | 11 | 8 | 10 c | 4 d |
| Male | 13 | 7 | 5 d | 11 c |
| Delivery | ||||
| Natural | 16 | 8 | 14 | 11 |
| Cesarean section | 8 | 7 | 1 | 4 |
| Maternal education level | ||||
| Primary school | 1 | 1 | 2 | 2 |
| High school | 10 | 12 | 7 | 9 |
| College and above | 13 | 3 | 6 | 4 |
| Fatty Acid | Normal BMI (n = 15) | Normal BMI+GD (n = 15) | Obese (n = 14) | Obese+GD (n = 14) |
|---|---|---|---|---|
| C6:0 | 1.66 ± 1.71 a | 0.17 ± 0.42 b | 0.24 ± 0.46 c | 0.11 ± 0.27 d |
| C8:0 | 0.22 ± 0.53 | 0.04 ± 0.09 | 0.01 ± 0.04 | 0.07 ± 0.11 |
| C10:0 | 1.05 ± 0.62 | 0.84 ± 0.21 | 0.79 ± 0.22 | 0.78 ± 0.30 |
| C12:0 | 5.75 ± 2.20 b | 5.25 ± 1.99 b | 5.04 ± 1.30 b | 3.57 ± 2.00 a |
| C14:0 | 7.74 ± 2.54 b | 7.14 ± 3.44 b | 4.13 ± 3.82 a | 4.58 ± 4.70 a |
| C16:0 | 25.80 ± 2.21 a | 28.64 ± 2.78 b | 27.85 ± 2.75 b | 29.09 ± 3.45 b |
| C18:0 | 5.28 ± 0.55 | 5.31 ± 1.70 | 4.57 ± 1.66 | 4.86 ± 1.42 |
| C20:0 | 0.13 ± 0.05 | 0.08 ± 0.05 | 0.17 ± 0.16 | 0.13 ± 0.09 |
| C21:0 | 0.41 ± 1.04 | 0.01 ± 0.03 | 0.02 ± 0.03 | 0.05 ± 0.11 |
| C24:0 | 0.33 ± 0.69 | 0.06 ± 0.13 | nd | nd |
| ∑SFA | 48.37 ± 1.63 | 47.53 ± 2.17 | 42.82 ± 3.12 | 43.24 ± 2.48 |
| Predicted Group Membership | ||||
|---|---|---|---|---|
| Normal BMI | Obese | |||
| Original | Count | Normal BMI | 29 | 1 |
| Obese | 0 | 28 | ||
| % | Normal BMI | 96.7 | 3.3 | |
| Obese | 0.0 | 100.0 | ||
| Cross-validated | Count | Normal BMI | 25 | 5 |
| Obese | 1 | 27 | ||
| % | Normal BMI | 83.3 | 16.7 | |
| Obese | 3.6 | 96.4 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simon Sarkadi, L.; Zhang, M.; Muránszky, G.; Vass, R.A.; Matsyura, O.; Benes, E.; Vari, S.G. Fatty Acid Composition of Milk from Mothers with Normal Weight, Obesity, or Gestational Diabetes. Life 2022, 12, 1093. https://doi.org/10.3390/life12071093
Simon Sarkadi L, Zhang M, Muránszky G, Vass RA, Matsyura O, Benes E, Vari SG. Fatty Acid Composition of Milk from Mothers with Normal Weight, Obesity, or Gestational Diabetes. Life. 2022; 12(7):1093. https://doi.org/10.3390/life12071093
Chicago/Turabian StyleSimon Sarkadi, Livia, Miaomiao Zhang, Géza Muránszky, Réka Anna Vass, Oksana Matsyura, Eszter Benes, and Sandor G. Vari. 2022. "Fatty Acid Composition of Milk from Mothers with Normal Weight, Obesity, or Gestational Diabetes" Life 12, no. 7: 1093. https://doi.org/10.3390/life12071093