
Boron Neutron Capture Therapy (BNCT) Mediated by Maleimide-Functionalized Closo-Dodecaborate Albumin Conjugates (MID:BSA) for Oral Cancer: Biodistribution Studies and In Vivo BNCT in the Hamster Cheek Pouch Oral Cancer Model

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. MID:BSA Preparation and Biodistribution Studies
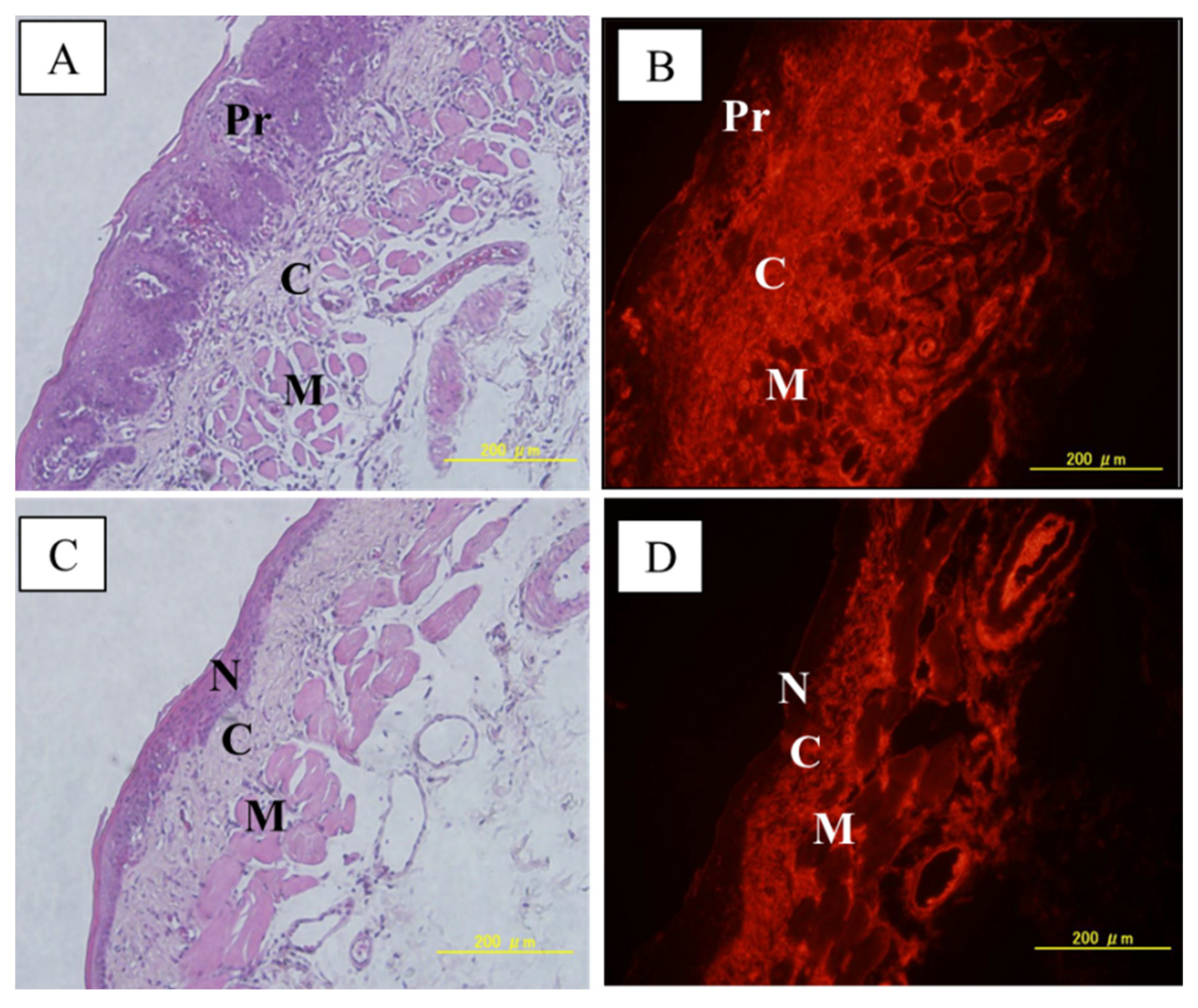
2.2. Preliminary MID:BSA Immunostaining Studies
2.3. In Vivo BNCT Studies
2.4. Statistical Analysis
3. Results

{kind=link}
{kind=link}
| MID:BSA 15 mg B/kg 12 h-Protocol | MID:BSA 15 mg B/kg 19 h-Protocol | |||
|---|---|---|---|---|
| Tissue | n | ppm ± SD | n | ppm ± SD |
| Tumor | 15 tumors | 32.4 ± 9.0 | 27 tumors | 31.7 ± 11.1 |
| Precancerous tissue | 4 animals | 15.7 ± 3.0 | 8 animals | 24.3 ± 11.3 |
| Normal | 4 animals | 5.5 ± 1.3 | 8 animals | 6.8 ± 1.5 |
| Liver | 4 animals | 27.4 ± 5.3 | 8 animals | 30.4 ± 12.7 |
| Kidney | 4 animals | 25.2 ± 3.9 | 8 animals | 27.5 ± 7.6 |
| Spleen | 4 animals | 14.0 ± 3.7 | 4 animals | 17.7 ± 3.8 |
| Blood | 4 animals | 41.9 ± 6.8 | 8 animals | 23.2 ± 9.0 |
| Tumor/precancerous tissue | 2.1 ± 0.6 | 1.3 ± 0.6 | ||
| Tumor/normal tissue | 6.1 ± 0.9 | 4.7 ± 1.4 | ||
| Tumor/blood | 0.8 ± 0.1 | 1.6 ± 1.1 | ||
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
List of Abbreviations
| BNCT | Boron Neutron Capture Therapy |
| BPA | Boronophenylalanine |
| GB-10 | Decahydrodecaborate |
| MID | Maleimide-functionalized closo-dodecaborate |
| EPR | Enhanced Permeability and Retention effect |
| BSA | Bovine serum albumin |
| HPV | Human papillomavirus |
| LET | Linear Energy Transfer |
| DMBA | 7,12-dimethylbenz[a]anthracene |
| CICUAL-CNEA | Argentine National Atomic Energy Commission Animal Care and Use Committee |
| PBS | Phosphate-buffered saline |
| TTBS | Tween-Tris-buffered saline (TTBS) |
| NR | No (tumor) Response |
| OR | Overall (tumor) Response |
| PR | Partial (tumor) Response |
| CR | Complete (tumor) Response |
| NUMF | non unusual features |
| SPARC | Secreted Protein, Acidic, and Rich in Cysteine |
| IFP | Interstitial fluid pressure |
References
- Schüttrumpf, L.; Marschner, S.; Scheu, K.; Hess, J.; Rietzler, S.; Walch, A.; Baumeister, P.; Kirchner, T.; Ganswindt, U.; Zitzelsberger, H.; et al. Definitive chemoradiotherapy in patients with squamous cell cancers of the head and neck-results from an unselected cohort of the clinical cooperation group “Personalized Radiotherapy in Head and Neck Cancer”. Radiat. Oncol. 2020, 15, 7. [Google Scholar] [CrossRef]
- Alves, C.G.B.; Treister, N.S.; Ribeiro, A.C.P.; Brandão, T.B.; Tonaki, J.O.; Lopes, M.A.; Rivera, C.; Santos-Silva, A.R. Strategies for communicating oral and oropharyngeal cancer diagnosis: Why talk about it? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 347–356. [Google Scholar] [CrossRef]
- Atwell, D.; Elks, J.; Cahill, K.; Hearn, N.; Vignarajah, D.; Lagopoulos, J.; Min, M. A Review of Modern Radiation Therapy Dose Escalation in Locally Advanced Head and Neck Cancer. Clin. Oncol. (R. Coll. Radiol.) 2020, 32, 330–341. [Google Scholar] [CrossRef] [PubMed]
- Machiels, J.P.; Lambrecht, M.; Hanin, F.X.; Duprez, T.; Gregoire, V.; Schmitz, S.; Hamoir, M. Advances in the management of squamous cell carcinoma of the head and neck. F1000Prime Rep. 2014, 6, 44. [Google Scholar] [CrossRef]
- Koudougou, C.; Bertin, H.; Lecaplain, B.; Badran, Z.; Longis, J.; Corre, P.; Hoornaert, A. Postimplantation radiation therapy in head and neck cancer patients: Literature review. Head Neck. 2020, 42, 794–802. [Google Scholar] [CrossRef]
- Cinausero, M.; Aprile, G.; Ermacora, P.; Basile, D.; Vitale, M.G.; Fanotto, V.; Parisi, G.; Calvetti, L.; Sonis, S.T. New frontiers in the pathobiology and treatment of cancer regimen-related mucosal injury. Front. Pharmacol. 2017, 8, 354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monti Hughes, A.; Goldfinger, J.A.; Santa Cruz, I.S.; Pozzi, E.C.; Thorp, S.; Curotto, P.; Garabalino, M.A.; Itoiz, M.E.; Palmieri, M.A.; Ramos, P.; et al. Different oral cancer scenarios to personalize targeted therapy: Boron Neutron Capture Therapy translational studies. Ther. Deliv. 2019, 10, 353–362. [Google Scholar] [CrossRef]
- Shu, Z.; Li, P.; Yu, B.; Huang, S.; Chen, Y. The effectiveness of probiotics in prevention and treatment of cancer therapy-induced oral mucositis: A systematic review and meta-analysis. Oral Oncol. 2020, 102, 104559. [Google Scholar] [CrossRef]
- Coderre, J.A.; Morris, G.M.; Kalef-Ezra, J.; Micca, P.L.; Ma, R.; Youngs, K.; Gordon, C.R. The effects of boron neutron capture irradiation on oral mucosa: Evaluation using a rat tongue model. Radiat. Res. 1999, 152, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Trivillin, V.A.; Heber, E.M.; Nigg, D.W.; Itoiz, M.E.; Calzetta, O.; Blaumann, H.; Longhino, J.; Schwint, A.E. Therapeutic success of boron neutron capture therapy (BNCT) mediated by a chemically nonselective boron agent in an experimental model of oral cancer: A new paradigm in BNCT radiobiology. Radiat. Res. 2006, 166, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Schwint, A.E.; Trivillin, V.A. ‘Close-to-ideal’ tumor boron targeting for boron neutron capture therapy is possible with ‘less-than-ideal’ boron carriers approved for use in humans. Ther. Deliv. 2015, 6, 269–272. [Google Scholar] [CrossRef]
- Farhood, B.; Samadian, H.; Ghorbani, M.; Zakariaee, S.S.; Knaup, C. Physical, dosimetric and clinical aspects and delivery systems in neutron capture therapy. Rep. Pract. Oncol. Radiother. 2018, 23, 462–473. [Google Scholar] [CrossRef]
- Menendez, P.R.; Roth, B.M.; Pereira, M.D.; Casal, M.R.; González, S.J.; Feld, D.B.; Santa Cruz, G.A.; Kessler, J.; Longhino, J.; Blaumann, H.; et al. BNCT for skin melanoma in extremities: Updated Argentine clinical results. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S50–S53. [Google Scholar] [CrossRef]
- Kankaanranta, L.; Seppala, T.; Koivunoro, H.; Saarilahti, K.; Atula, T.; Collan, J.; Salli, E.; Kortesniemi, M.; Uusi-Simola, J.; Välimäki, P.; et al. Boron neutron capture therapy in the treatment of locally recurred head-and-neck cancer: Final analysis of a Phase I/II trial. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e67–e75. [Google Scholar] [CrossRef]
- Lim, D.; Quah, D.S.; Leech, M.; Marignol, L. Clinical potential of boron neutron capture therapy for locally recurrent inoperable previously irradiated head and neck cancer. Appl. Radiat. Isot. 2015, 106, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Hiratsuka, J.; Kamitani, N.; Tanaka, R.; Yoden, E.; Tokiya, R.; Suzuki, M.; Barth, R.F.; Ono, K. Boron neutron capture therapy for vulvar melanoma and genital extramammary Paget’s disease with curative responses. Cancer Commun. 2018, 38, 38. [Google Scholar] [CrossRef] [Green Version]
- Shiba, H.; Takeuchi, K.; Hiramatsu, R.; Furuse, M.; Nonoguchi, N.; Kawabata, S.; Kuroiwa, T.; Kondo, N.; Sakurai, Y.; Suzuki, M.; et al. Boron Neutron Capture Therapy Combined with Early Successive Bevacizumab Treatments for Recurrent Malignant Gliomas—A Pilot Study. Neurol. Med. Chir. (Tokyo) 2018, 58, 487–494. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.W.; Liu, Y.H.; Chou, F.I.; Jiang, S.H. Clinical trials for treating recurrent head and neck cancer with boron neutron capture therapy using the Tsing-Hua Open Pool Reactor. Cancer Commun. 2018, 38, 37. [Google Scholar] [CrossRef] [Green Version]
- Hirose, K.; Konno, A.; Hiratsuka, J.; Yoshimoto, S.; Kato, T.; Ono, K.; Otsuki, N.; Hatazawa, J.; Tanaka, H.; Takayama, K.; et al. Boron neutron capture therapy using cyclotron-based epithermal neutron source and borofalan (10B) for recurrent or locally advanced head and neck cancer (JHN002): An open-label phase II trial. Radiother. Oncol. 2021, 155, 182–187. [Google Scholar] [CrossRef]
- Nagini, S.; Kowshik, J. The hamster buccal pouch model of oral carcinogenesis. Methods Mol. Biol. 2016, 1422, 341–350. [Google Scholar] [CrossRef]
- Sangild, P.T.; Shen, R.L.; Pontoppidan, P.; Rathe, M. Animal models of chemotherapy-induced mucositis: Translational relevance and challenges. Am. J. Physiol. Gastrointest. Liver Physiol. 2018, 314, G231–G246. [Google Scholar] [CrossRef]
- Yapijakis, C.; Kalogera, S.; Papakosta, V.; Vassiliou, S. The Hamster Model of Sequential Oral Carcinogenesis: An Update. In Vivo 2019, 33, 1751–1755. [Google Scholar] [CrossRef] [Green Version]
- Monti-Hughes, A.; Aromando, R.F.; Perez, M.A.; Schwint, A.E.; Itoiz, M.E. The hamster cheek pouch model for field cancerization studies. Periodontol. 2000 2015, 67, 292–311. [Google Scholar] [CrossRef]
- Salley, J.J. Experimental carcinogenesis in the cheek pouch of the Syrian hamster. J. Dent. Res. 1954, 33, 253–262. [Google Scholar] [CrossRef]
- Morris, L. Factors influencing experimental carcinogenesis in the hamster cheek pouch. J. Dent Res. 1961, 40, 3–15. [Google Scholar] [CrossRef]
- Kreimann, E.L.; Itoiz, M.E.; Longhino, J.; Blaumann, H.; Calzetta, O.; Schwint, A.E. Boron neutron capture therapy for the treatment of oral cancer in the hamster cheek pouch model. Cancer Res. 2001, 61, 8638–8642. [Google Scholar]
- Pozzi, E.; Nigg, D.W.; Miller, M.; Thorp, S.I.; Heber, E.M.; Zarza, L.; Estryk, G.; Monti Hughes, A.; Molinari, A.J.; Garabalino, M.; et al. Dosimetry and radiobiology at the new RA-3 reactor boron neutron capture therapy (BNCT) facility: Application to the treatment of experimental oral cancer. Appl Radiat Isot. 2009, 67 (Suppl. 7–8), S309–S312. [Google Scholar] [CrossRef]
- Monti Hughes, A.; Pozzi, E.C.; Heber, E.M.; Thorp, S.; Miller, M.; Itoiz, M.E.; Aromando, R.F.; Molinari, A.J.; Garabalino, M.A.; Nigg, D.W.; et al. Boron Neutron Capture Therapy (BNCT) in an oral precancer model: Therapeutic benefits and potential toxicity of a double application of BNCT with a six-week interval. Oral Oncol. 2011, 47, 1017–1022. [Google Scholar] [CrossRef]
- Heber, E.M.; Hawthorne, M.F.; Kueffer, P.J.; Garabalino, M.A.; Thorp, S.I.; Pozzi, E.C.; Monti Hughes, A.; Maitz, C.A.; Jalisatgi, S.S.; Nigg, D.W.; et al. Therapeutic efficacy of boron neutron capture therapy mediated by boron-rich liposomes for oral cancer in the hamster cheek pouch model. Proc. Natl. Acad. Sci. USA 2014, 111, 16077–16081. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, H.; Kikuchi, S.; Kawai, K.; Ishii, S.; Sato, S. Closo-Dodecaborate-conjugated human serum albumins: Preparation and in vivo selective boron delivery to tumor. Pure Appl. Chem. 2018, 90, 745–753. [Google Scholar] [CrossRef] [Green Version]
- Elsadek, B.; Kratz, F. Impact of albumin on drug delivery—New applications on the horizon. J. Control Release 2012, 157, 4–28. [Google Scholar] [CrossRef]
- Ziaaddini, V.; Saeidifar, M.; EslamiMoghadam, M.; Saberi, M.; Mozafari, M. Improvement of efficacy and decrement cytotoxicity of oxaliplatin anticancer drug using bovine serum albumin nanoparticles: Synthesis, characterisation and release behaviour. IET Nanobiotechnol. 2020, 14, 105–111. [Google Scholar] [CrossRef]
- Kamphorst, J.J.; Nofal, M.; Commisso, C.; Hackett, S.R.; Lu, W.; Grabocka, E.; Vander Heiden, M.G.; Miller, G.; Drebin, J.A.; Bar-Sagi, D.; et al. Human pancreatic cancer tumors are nutrient poor and tumor cells actively scavenge extracellular protein. Cancer Res. 2015, 75, 544–553. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, S.; Kanoh, D.; Sato, S.; Sakurai, Y.; Suzuki, M.; Nakamura, H. Maleimide-functionalized closo-dodecaborate albumin conjugates (MID-AC): Unique ligation at cysteine and lysine residues enables efficient boron delivery to tumor for neutron capture therapy. J. Control Rel. 2016, 237, 160–167. [Google Scholar] [CrossRef]
- Kashiwagi, H.; Kawabata, S.; Yoshimura, K.; Fukuo, Y.; Kanemitsu, T.; Takeuchi, K.; Hiramatsu, R.; Nishimura, K.; Kawai, K.; Takata, T.; et al. Boron neutron capture therapy using dodecaborated albumin conjugates with maleimide is effective in a rat glioma model. Investig. New Drugs 2022, 40, 255–264. [Google Scholar] [CrossRef]
- Santa Cruz, I.S.; Garabalino, M.A.; Trivillin, V.A.; Itoiz, M.E.; Pozzi, E.C.C.; Thorp, S.; Curotto, P.; Guidobono, J.S.; Heber, E.M.; Nigg, D.W.; et al. Optimization of the classical oral cancerization protocol in hamster to study oral cancer therapy. Oral Dis. 2020, 26, 1175–1184. [Google Scholar] [CrossRef]
- Garabalino, M.A.; Olaiz, N.; Portu, A.; Saint Martin, G.; Thorp, S.I.; Pozzi, E.C.C.; Curotto, P.; Itoiz, M.E.; Monti Hughes, A.; Colombo, L.L.; et al. Electroporation optimizes the uptake of boron-10 by tumor for boron neutron capture therapy (BNCT) mediated by GB-10: A boron biodistribution study in the hamster cheek pouch oral cancer model. Radiat. Environ. Biophys. 2019, 58, 455–467. [Google Scholar] [CrossRef]
- Sonis, S.T.; Peterson, R.L.; Edwards, L.J.; Lucey, C.A.; Wang, L.; Mason, L.; Login, G.; Ymamkawa, M.; Moses, G.; Bouchard, P.; et al. Defining mechanisms of action of interleukin-11 on the progression of radiation induced oral mucositis in hamsters. Oral Oncol. 2000, 36, 373–381. [Google Scholar] [CrossRef]
- López-Castaño, F.; Oñate-Sánchez, R.E.; Roldán-Chicano, R.; Cabrerizo-Merino, M.C. Measurement of secondary mucositis to ´oncohematologic treatment by means of different scale. Med. Oral Patol. Oral Cir. Bucal 2015, 10, 412–421. [Google Scholar]
- Molinari, A.J.; Pozzi, E.C.; Monti Hughes, A.; Heber, E.M.; Garabalino, M.A.; Thorp, S.I.; Miller, M.; Itoiz, M.E.; Aromando, R.F.; Nigg, D.W.; et al. “Sequential” boron neutron capture therapy (BNCT): A novel approach to BNCT for the treatment of oral cancer in the hamster cheek pouch model. Radiat. Res. 2011, 175, 463–472. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing. 2021. Available online: https://www.r-project.org/ (accessed on 30 June 2021).
- Zuur, A.F.; Ieno, E.N.; Walker, N.J.; Saveliev, A.A.; Smith, G.M. Mixed Effects Models and Extension in Ecology with R; Springer Science + Business Media, LLC: New York, NY, USA, 2009. [Google Scholar]
- Williamson, T.; Eliasziw, M.; Fick, G.H. Log-binomial models: Exploring failed convergence. Emerg. Themes Epidemiol. 2013, 10, 14. [Google Scholar] [CrossRef] [Green Version]
- Garabalino, M.A.; Monti Hughes, A.; Molinari, A.J.; Heber, E.M.; Pozzi, E.C.; Cardoso, J.E.; Colombo, L.L.; Nievas, S.; Nigg, D.W.; Aromando, R.F.; et al. Boron neutron capture therapy (BNCT) for the treatment of liver metastases: Biodistribution studies of boron compounds in an experimental model. Radiat. Environ. Biophys. 2011, 50, 199–207. [Google Scholar] [CrossRef]
- Available online: https://www.fda.gov/media/70406/download (accessed on 20 August 2021).
- Heber, E.M.; Aromando, R.F.; Trivillin, V.A.; Itoiz, M.E.; Nigg, D.W.; Kreimann, E.L.; Schwint, A.E. Therapeutic effect of boron neutron capture therapy (BNCT) on field cancerized tissue: Inhibition of DNA synthesis and lag in the development of second primary tumors in precancerous tissue around treated tumors in DMBA-induced carcinogenesis in the hamster cheek pouch oral cancer model. Arch. Oral Biol. 2007, 52, 273–279. [Google Scholar] [CrossRef]
- Monti Hughes, A.; Heber, E.M.; Pozzi, E.; Nigg, D.W.; Calzetta, O.; Blaumann, H.; Longhino, J.; Nievas, S.I.; Aromando, R.F.; Itoiz, M.E.; et al. Boron neutron capture therapy (BNCT) inhibits tumor development from precancerous tissue: An experimental study that supports a potential new application of BNCT. Appl. Radiat. Isot. 2009, 67 (Suppl. 7–8), S313–S317. [Google Scholar] [CrossRef]
- Aromando, R.F.; Raimondi, A.R.; Pérez, M.A.; Trivillin, V.A.; Schwint, A.E.; Itoiz, M.E. Angiogenesis in Potentially Malignant Lesions and Carcinomas during Experimental Oral Carcinogenesis: A Preliminary Study in the Hamster Cheek Pouch. Anticancer Res. 2014, 34, 6381–6388. [Google Scholar]
- Aquino, G.; Sabatino, R.; Cantile, M.; Aversa, C.; Ionna, F.; Botti, G.; La Mantia, E.; Collina, F.; Malzone, G.; Pannone, G.; et al. Expression analysis of SPARC/osteonectin in oral squamous cell carcinoma patients: From saliva to surgical specimen. Biomed. Res. Int. 2013, 2013, 736438. [Google Scholar] [CrossRef]
- Chen, D.; Yang, K.; Mei, J.; Zhang, G.; Lv, X.; Xiang, L. Screening the pathogenic genes and pathways related to DMBA (7,12-dimethylbenz[a]anthracene)-induced transformation of hamster oral mucosa from precancerous lesions to squamous cell carcinoma. Oncol. Lett. 2011, 2, 637–642. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Choi, Y.; Chang, H.; Um, W.; Ryu, J.H.; Kwon, I.C. Alliance with EPR Effect: Combined Strategies to Improve the EPR Effect in the Tumor Microenvironment. Theranostics 2019, 9, 8073–8090. [Google Scholar] [CrossRef]
- Golombek, S.K.; May, J.N.; Theek, B.; Appold, L.; Drude, N.; Kiessling, F.; Lammers, T. Tumor targeting via EPR: Strategies to enhance patient responses. Adv. Drug Deliv. Rev. 2018, 130, 17–38. [Google Scholar] [CrossRef]
- Fang, J.; Nakamura, H.; Maeda, H. The EPR effect: Unique features of tumor blood vessels for drug delivery, factors involved, and limitations and augmentation of the effect. Adv. Drug Deliv. Rev. 2011, 63, 136–151. [Google Scholar] [CrossRef]
- Dhaliwal, A.; Zheng, G. Improving accessibility of EPR-insensitive tumor phenotypes using EPR-adaptive strategies: Designing a new perspective in nanomedicine delivery. Theranostics 2019, 9, 8091–8108. [Google Scholar] [CrossRef] [PubMed]
- Monti Hughes, A.; Pozzi, E.C.; Thorp, S.; Garabalino, M.A.; Farías, R.O.; González, S.J.; Heber, E.M.; Itoiz, M.E.; Aromando, R.F.; Molinari, A.J.; et al. Boron neutron capture therapy for oral precancer: Proof of principle in an experimental animal model. Oral Dis. 2013, 19, 789–795. [Google Scholar] [CrossRef] [PubMed]


| Dose Components | Fast Neutrons * | Gamma Photons * | Induced Protons * | Total Dose Without Boron Irradiation Component ** | Boron Irradiation Component | Boron Dose/ppm Boron Concentration | Total Absorbed Dose |
|---|---|---|---|---|---|---|---|
| MID:BSA/BNCT 15 mg/kg 19 h post-injection-4.8 Gy absorbed dose to precancerous tissue | |||||||
| Tumor | - | 0.44 ± 0.04 Gy | 0.60 ± 0.13 Gy | 1.05 ± 0.14 Gy | 4.9 ± 2.0 Gy | 0.16 ± 0.08 Gy | 6.0 ± 2.0 Gy |
| Precancerous tissue | - | 0.44 ± 0.04 Gy | 0.60 ± 0.13 Gy | 1.05 ± 0.14 Gy | 3.8 ± 1.9 Gy | 0.16 ± 0.11 Gy | 4.8 ± 1.9 Gy |
| Normal tissue | - | 0.44 ± 0.04 Gy | 0.60 ± 0.13 Gy | 1.05 ± 0.14 Gy | 1.1 ± 0.3 Gy | 0.16 ± 0.06 Gy | 2.1 ± 0.4 Gy |
| MID:BSA/BNCT 15 mg/kg 19 h post-injection-6.0 Gy absorbed dose to precancerous tissue | |||||||
| Tumor | - | 0.55 ± 0.06 Gy | 0.74 ± 0.16 Gy | 1.30 ± 0.17 Gy | 6.1 ± 2.5 Gy | 0.19 ± 0.10 Gy | 7.4 ± 2.5 Gy |
| Precancerous tissue | - | 0.55 ± 0.06 Gy | 0.74 ± 0.16 Gy | 1.30 ± 0.17 Gy | 4.7 ± 2.4 Gy | 0.19 ± 0.13 Gy | 6.0 ± 2.4 Gy |
| Normal tissue | - | 0.55 ± 0.06 Gy | 0.74 ± 0.16 Gy | 1.30 ± 0.17 Gy | 1.3 ± 0.4 Gy | 0.19 ± 0.07 Gy | 2.6 ± 0.4 Gy |
| MID:BSA/BNCT 15 mg/kg 19 h post-injection-7.5 Gy absorbed dose to precancerous tissue | |||||||
| Tumor | - | 0.67 ± 0.07 Gy | 0.93 ± 0.20 Gy | 1.60 ± 0.21 Gy | 7.7 ± 3.1 Gy | 0.24 ± 0.13 Gy | 9.3 ± 3.2 Gy |
| Precancerous tissue | - | 0.67 ± 0.07 Gy | 0.93 ± 0.20 Gy | 1.60 ± 0.21 Gy | 5.9 ± 3.0 Gy | 0.24 ± 0.17 Gy | 7.5 ± 3.0 Gy |
| Normal tissue | - | 0.67 ± 0.07 Gy | 0.93 ± 0.20 Gy | 1.60 ± 0.21 Gy | 1.6 ± 0.5 Gy | 0.24 ± 0.09 Gy | 3.2 ± 0.5 Gy |
| 7 Days | 14 Days | 21 Days | 28 Days | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | %OR | %CR | n | %OR | %CR | n | %OR | %CR | n | %OR | %CR | |
| CONTROL | 51 | 24 | 2 | 51 | 22 | 8 | 45 | 18 | 7 | 34 | 21 | 9 |
| (A) 4.8 Gy | 35 | 54 | 9 | 35 | 66 | 14 | 27 | 56 | 19 | 27 | 59 | 19 |
| (B) 6.0 Gy | 21 | 100 | 10 | 21 | 81 | 14 | 21 | 76 | 14 | 16 | 82 | 18 |
| (C) 7.5 Gy | 27 | 78 | 19 | 27 | 78 | 15 | 27 | 70 | 22 | 27 | 67 | 19 |
| R ≥ 50% | 7 Days | 14 Days | 21 Days | 28 Days | ||||
|---|---|---|---|---|---|---|---|---|
| n | %R | n | %R | n | %R | n | %R | |
| (A) 4.8 Gy | 16 | 44 | 18 | 39 | 10 | 70 | 11 | 55 |
| (B) 6.0 Gy | 19 | 53 | 14 | 79 | 13 | 92 | 11 | 64 |
| (C) 7.5 Gy | 16 | 31 | 17 | 82 | 13 | 85 | 13 | 92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monti Hughes, A.; Goldfinger, J.A.; Palmieri, M.A.; Ramos, P.; Santa Cruz, I.S.; De Leo, L.; Garabalino, M.A.; Thorp, S.I.; Curotto, P.; Pozzi, E.C.C.; et al. Boron Neutron Capture Therapy (BNCT) Mediated by Maleimide-Functionalized Closo-Dodecaborate Albumin Conjugates (MID:BSA) for Oral Cancer: Biodistribution Studies and In Vivo BNCT in the Hamster Cheek Pouch Oral Cancer Model. Life 2022, 12, 1082. https://doi.org/10.3390/life12071082
Monti Hughes A, Goldfinger JA, Palmieri MA, Ramos P, Santa Cruz IS, De Leo L, Garabalino MA, Thorp SI, Curotto P, Pozzi ECC, et al. Boron Neutron Capture Therapy (BNCT) Mediated by Maleimide-Functionalized Closo-Dodecaborate Albumin Conjugates (MID:BSA) for Oral Cancer: Biodistribution Studies and In Vivo BNCT in the Hamster Cheek Pouch Oral Cancer Model. Life. 2022; 12(7):1082. https://doi.org/10.3390/life12071082
Chicago/Turabian StyleMonti Hughes, Andrea, Jessica A. Goldfinger, Mónica A. Palmieri, Paula Ramos, Iara S. Santa Cruz, Luciana De Leo, Marcela A. Garabalino, Silvia I. Thorp, Paula Curotto, Emiliano C. C. Pozzi, and et al. 2022. "Boron Neutron Capture Therapy (BNCT) Mediated by Maleimide-Functionalized Closo-Dodecaborate Albumin Conjugates (MID:BSA) for Oral Cancer: Biodistribution Studies and In Vivo BNCT in the Hamster Cheek Pouch Oral Cancer Model" Life 12, no. 7: 1082. https://doi.org/10.3390/life12071082