
An Overview of Diabetic Foot Ulcers and Associated Problems with Special Emphasis on Treatments with Antimicrobials

 , , , and
, , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
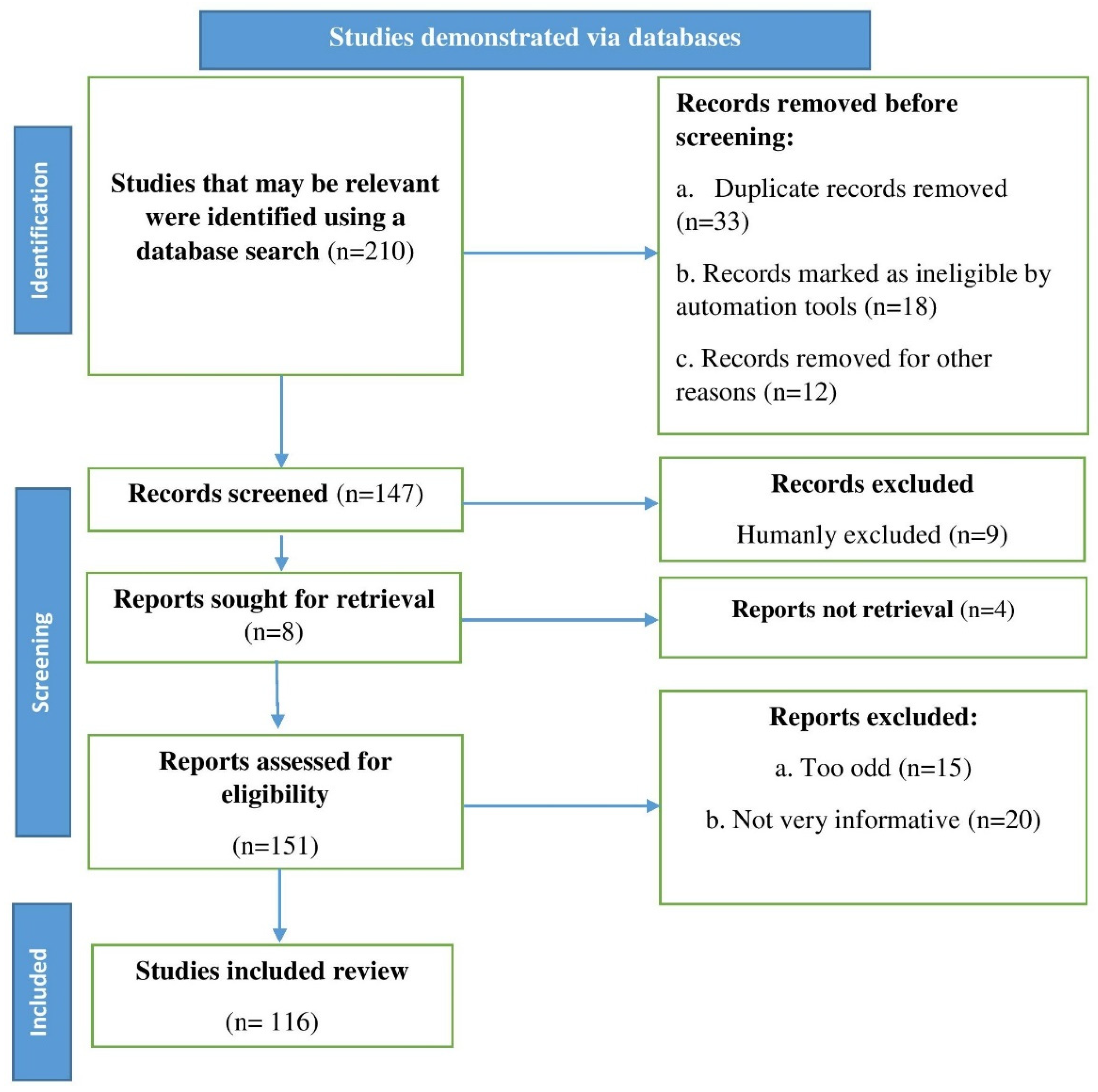
2. Methodology
3. Diabetic Foot Ulcers (DFUs)
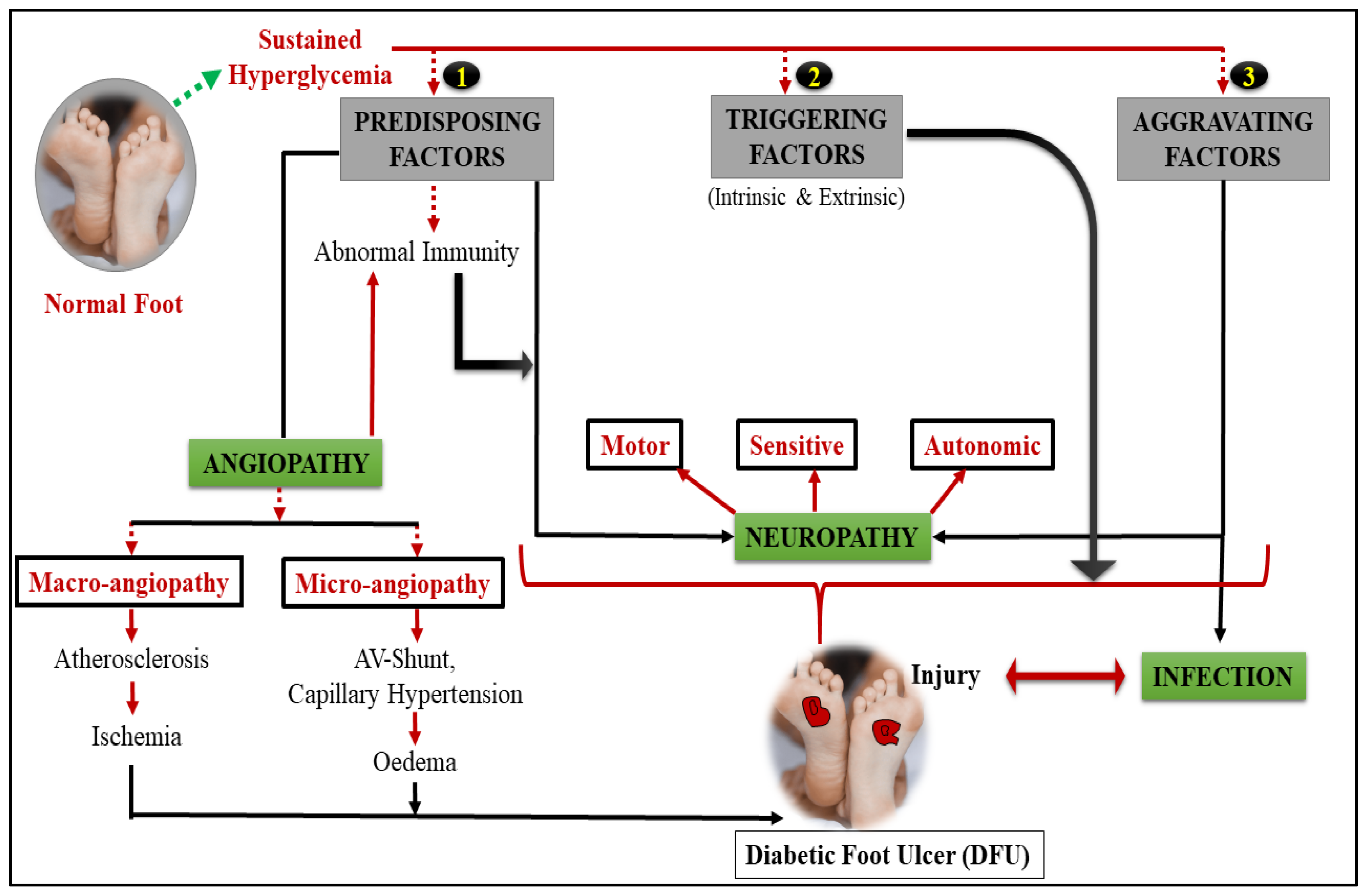
4. Pathophysiology of DFUs
4.1. Diabetic Neuropathy
4.2. DFUs Pathogenesis: Immunological Involvement
4.3. PAD
5. Infection of DFUs
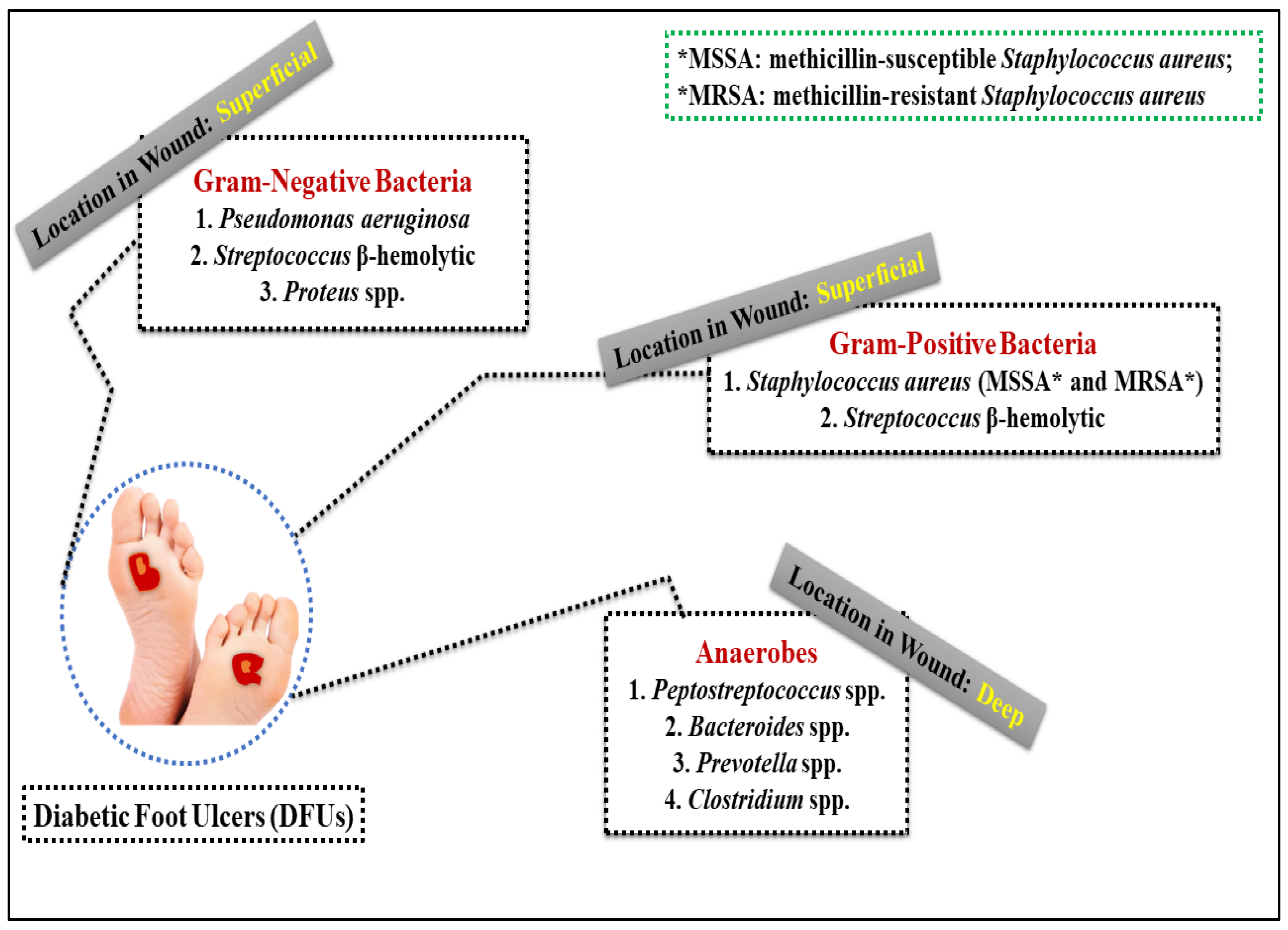
5.1. Bacterial Species of the DFUs
5.2. Existence of Biofilms and Its Production in DFUs
6. Multidrug-Resistant Bacteria in DFUs
7. Therapeutic Methods Used to Manage DFU Infections
7.1. Removal of the Bacterial Biofilm (Debridement)
7.2. Dressings
7.3. Types of Antibacterial Agents Used to Treat DFUs
7.4. Systemic Therapy with Antibiotics
8. Some Emerging Therapies in Brief for the Treatment of DFUs
9. Recent Upgrade in the Field of DFUs
10. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IDF | International Diabetes Federation |
| DFU | Diabetic foot ulcers |
| PAD | Peripheral arterial disease |
| ROS | Reactive oxygen species |
| NADPH | Nicotinamide adenine dinucleotide phosphate |
| DFIs | Diabetic foot infections |
| IDSA | Infectious Diseases Society of America |
| SIR | Systemic inflammatory reaction |
| CCO | Clostridial collagenase ointment |
| NPWT | Negative pressure wound therapy |
| LD | Laser Doppler |
| LTH | Local thermal hyperemia |
| PTCTD | Proximal tibial cortex transverse distraction |
| EPCs | Endothelial progenitor cells |
| BMSCs | Bone marrow-derived mesenchymal stem cells |
| PRP | Platelet-rich plasma |
| CDO | Continuous diffusion of oxygen |
| MWD | Moist wound dressing |
| XDR | Extensively drug-resistant bacteria |
| mTTT | Modified tibial transverse transport |
| AgNPs | Silver nanoparticles |
| TC | Turbinaria conoides |
| RCTs | Multicenter randomized controlled trials |
References
- Jiménez, P.G.; Martín-Carmona, J.; Hernández, E.L. Diabetes Mellitus. Medicine 2020, 13, 883–890. [Google Scholar] [CrossRef]
- Poretsky, L. (Ed.) Principles of Diabetes Mellitus; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010; ISBN 9780387098401. [Google Scholar]
- Aynalem, S.B.; Zeleke, A.J. Prevalence of Diabetes Mellitus and Its Risk Factors among Individuals Aged 15 Years and above in Mizan-Aman Town, Southwest Ethiopia, 2016: A Cross Sectional Study. Int. J. Endocrinol. 2018, 2018, 9317987. [Google Scholar] [CrossRef] [PubMed]
- Endris, T.; Worede, A.; Asmelash, D. Prevalence of Diabetes Mellitus, Prediabetes and Its Associated Factors in Dessie Town, Northeast Ethiopia: A Community-Based Study. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2799–2809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nugroho, P.S.; Tianingrum, N.A.; Sunarti, S.; Rachman, A.; Fahrurodzi, D.S.; Amiruddin, R. Predictor Risk of Diabetes Mellitus in Indonesia, Based on National Health Survey. Malays. J. Med. Health Sci. 2020, 16, 126–130. [Google Scholar]
- Hussain, Z.; Thu, H.E.; Shuid, A.N.; Katas, H.; Hussain, F. Recent Advances in Polymer-Based Wound Dressings for the Treatment of Diabetic Foot Ulcer: An Overview of State-of-the-Art. Curr. Drug Targets 2017, 19, 527–550. [Google Scholar] [CrossRef]
- Moura, L.I.F.; Dias, A.M.A.; Carvalho, E.; De Sousa, H.C. Recent Advances on the Development of Wound Dressings for Diabetic Foot Ulcer Treatment—A Review. Acta Biomater. 2013, 9, 7093–7114. [Google Scholar] [CrossRef] [Green Version]
- Li, W.W.; Li, V.W. Therapeutic Angiogenesis for Wound Healing. Wounds Compend. Clin. Res. Pract. 2003, 15, 2S–12S. [Google Scholar]
- Singh, M.R.; Saraf, S.; Vyas, A.; Jain, V.; Singh, D. Innovative Approaches in Wound Healing: Trajectory and Advances. Artif. Cells Nanomed. Biotechnol. 2013, 41, 202–212. [Google Scholar] [CrossRef]
- Singh, N.; Armstrong, D.G.; Lipsky, B.A. Preventing Foot Ulcers in Patients with Diabetes. J. Am. Med. Assoc. 2005, 293, 217–228. [Google Scholar] [CrossRef]
- Ruke, M.G.; Savai, J. Diabetic Foot Infection, Biofilm & New Management Strategy. Diabetes Res. Open Access 2019, 1, 7–22. [Google Scholar] [CrossRef]
- Yazdanpanah, L. Literature Review on the Management of Diabetic Foot Ulcer. World J. Diabetes 2015, 6, 37. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Lu, J.; Jing, Y.; Tang, S.; Zhu, D.; Bi, Y. Global Epidemiology of Diabetic Foot Ulceration: A Systematic Review and Meta-Analysis. Ann. Med. 2017, 49, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Jeffcoate, W.J.; Vileikyte, L.; Boyko, E.J.; Armstrong, D.G.; Boulton, A.J.M. Current Challenges and Opportunities in the Prevention and Management of Diabetic Foot Ulcers. Diabetes Care 2018, 41, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Oyibo, S.O.; Jude, E.B.; Tarawneh, I.; Nguyen, H.C.; Harkless, L.B.; Boulton, A.J.M. A Comparison of Two Diabetic Foot Ulcer Classification Systems: The Wagner and the University of Texas Wound Classification Systems. Diabetes Care 2001, 24, 84–88. [Google Scholar] [CrossRef] [Green Version]
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF Diabetes Atlas: Global Estimates of the Prevalence of Diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef]
- Eldor, R.; Raz, I.; Ben Yehuda, A.; Boulton, A.J.M. New and Experimental Approaches to Treatment of Diabetic Foot Ulcers: A Comprehensive Review of Emerging Treatment Strategies. Diabet. Med. 2004, 21, 1161–1173. [Google Scholar] [CrossRef]
- Alavi, A.; Sibbald, R.G.; Mayer, D.; Goodman, L.; Botros, M.; Armstrong, D.G.; Woo, K.; Boeni, T.; Ayello, E.A.; Kirsner, R.S. Diabetic Foot Ulcers: Part II. Management. J. Am. Acad. Dermatol. 2014, 70, 21.e1–21.e24. [Google Scholar] [CrossRef]
- Management, E.; McCulloch, J.M.; Kloth, L.C. Wound Healing: Evidence-Based Management; FA Davis: Philadelphia, PA, USA, 2010. [Google Scholar]
- Muhammad Ibrahim, A. Diabetic Foot Ulcer: Synopsis of the Epidemiology and Pathophysiology. Int. J. Diabetes Endocrinol. 2018, 3, 23. [Google Scholar] [CrossRef] [Green Version]
- Rosyid, F.N. Etiology, Pathophysiology, Diagnosis and Management of Diabetics’ Foot Ulcer. Int. J. Res. Med. Sci. 2017, 5, 4206. [Google Scholar] [CrossRef] [Green Version]
- Syafril, S. Pathophysiology Diabetic Foot Ulcer. In Proceedings of the IOP Conference Series: Earth and Environmental Science, Medan, Indonesia, 15–18 November 2017; Volume 125. [Google Scholar]
- Alavi, A.; Sibbald, R.G.; Mayer, D.; Goodman, L.; Botros, M.; Armstrong, D.G.; Woo, K.; Boeni, T.; Ayello, E.A.; Kirsner, R.S. Diabetic Foot Ulcers: Part I. Pathophysiology and Prevention. J. Am. Acad. Dermatol. 2014, 70, 1.e1–1.e18. [Google Scholar] [CrossRef]
- Aumiller, W.D.; Dollahite, H.A. Pathogenesis and Management of Diabetic Foot Ulcers. J. Am. Acad. Physician Assist. 2015, 28, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Alsanawi, Y.; Alismail, H.; AlabdRabalnabi, M.; Alturki, H.; Alsuhaibani, A.; Mahbub, M.; Junayd, A.; Alamri, A.; Jawahraji, M.; Aldaghmani, M. Pathogenesis and Management of Diabetic Foot Ulcers. Int. J. Community Med. Public Health 2018, 5, 4953. [Google Scholar] [CrossRef]
- Frykberg, R.G. Diabetic Foot Ulcers: Pathogenesis and Management. Am. Fam. Physician 2002, 66, 1655–1662. [Google Scholar] [PubMed]
- Megallaa, M.H.; Ismail, A.A.; Zeitoun, M.H.; Khalifa, M.S. Association of Diabetic Foot Ulcers with Chronic Vascular Diabetic Complications in Patients with Type 2 Diabetes. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1287–1292. [Google Scholar] [CrossRef]
- Esteghamati, A.; Aflatoonian, M.; Rad, M.V.; Mazaheri, T.; Mousavizadeh, M.; Nakhjavani, M.; Noshad, S. Association of Osteoprotegerin with Peripheral Artery Disease in Patients with Type 2 Diabetes. Arch. Cardiovasc. Dis. 2015, 108, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Muthiah, A.; Kandasamy, R.S.N.; Madasamy, A. A Study on Diabetic Foot and Its Association with Peripheral Artery Disease. Int. Surg. J. 2017, 4, 1217. [Google Scholar] [CrossRef]
- Schaper, N.C. Diabetic Foot Ulcer Classification System for Research Purposes: A Progress Report on Criteria for Including Patients in Research Studies. Diabetes Metab. Res. Rev. 2004, 20, S90–S95. [Google Scholar] [CrossRef]
- Loesche, M.; Gardner, S.E.; Kalan, L.; Horwinski, J.; Zheng, Q.; Hodkinson, B.P.; Tyldsley, A.S.; Franciscus, C.L.; Hillis, S.L.; Mehta, S.; et al. Temporal Stability in Chronic Wound Microbiota Is Associated with Poor Healing. J. Investig. Dermatol. 2017, 137, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Andrea Nelson, E.; Backhouse, M.R.; Bhogal, M.S.; Wright-Hughes, A.; Lipsky, B.A.; Nixon, J.; Brown, S.; Gray, J. Concordance in Diabetic Foot Ulcer Infection. BMJ Open 2013, 3, e002370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, A.; Wright-Hughes, A.; Backhouse, M.R.; Lipsky, B.A.; Nixon, J.; Bhogal, M.S.; Reynolds, C.; Brown, S. CODIFI (Concordance in Diabetic Foot Ulcer Infection): A Cross-Sectional Study of Wound Swab versus Tissue Sampling in Infected Diabetic Foot Ulcers in England. BMJ Open 2018, 8, e019437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jouhar, L.; Jaafar, R.F.; Nasreddine, R.; Itani, O.; Haddad, F.; Rizk, N.; Hoballah, J.J. Microbiological Profile and Antimicrobial Resistance among Diabetic Foot Infections in Lebanon. Int. Wound J. 2020, 17, 1764–1773. [Google Scholar] [CrossRef] [PubMed]
- Jneid, J.; Lavigne, J.P.; La Scola, B.; Cassir, N. The Diabetic Foot Microbiota: A Review. Hum. Microbiome J. 2017, 5–6, 1–6. [Google Scholar] [CrossRef]
- Pereira, S.G.; Moura, J.; Carvalho, E.; Empadinhas, N. Microbiota of Chronic Diabetic Wounds: Ecology, Impact, and Potential for Innovative Treatment Strategies. Front. Microbiol. 2017, 8, 1791. [Google Scholar] [CrossRef]
- Martínez-De Jesús, F.R.; Ramos-De La Medina, A.; Remes-Troche, J.M.; Armstrong, D.G.; Wu, S.C.; Lázaro Martínez, J.L.; Beneit-Montesinos, J.V. Efficacy and Safety of Neutral PH Superoxidised Solution in Severe Diabetic Foot Infections. Int. Wound J. 2007, 4, 353–362. [Google Scholar] [CrossRef]
- Liu, P.Y.; Shi, Z.Y.; Sheu, W.H.H. Diagnosis and Treatment of Diabetic Foot Infections. J. Intern. Med. Taiwan 2012, 23, 431–441. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.O.; Henry, M. Update in Diagnosis and Treatment of Diabetic Foot Infections. Phys. Med. Rehabil. Clin. N. Am. 2009, 20, 611–625. [Google Scholar] [CrossRef]
- Murali, T.S.; Kavitha, S.; Spoorthi, J.; Bhat, D.V.; Prasad, A.S.B.; Upton, Z.; Ramachandra, L.; Acharya, R.V.; Satyamoorthy, K. Characteristics of Microbial Drug Resistance and Its Correlates in Chronic Diabetic Foot Ulcer Infections. J. Med. Microbiol. 2014, 63, 1377–1385. [Google Scholar] [CrossRef]
- Jain, S.; Barman, R. Bacteriological Profile of Diabetic Foot Ulcer with Special Reference to Drug-Resistant Strains in a Tertiary Care Center in North-East India. Indian J. Endocrinol. Metab. 2017, 21, 688–694. [Google Scholar] [CrossRef]
- Karmaker, M.; Sanyal, S.K.; Sultana, M.; Hossain, M.A. Association of Bacteria in Diabetic and Non-Diabetic Foot Infection—An Investigation in Patients from Bangladesh. J. Infect. Public Health 2016, 9, 267–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.; Collier, A.; Townsend, E.M.; O’Donnell, L.E.; Bal, A.M.; Butcher, J.; MacKay, W.G.; Ramage, G.; Williams, C. One Step Closer to Understanding the Role of Bacteria in Diabetic Foot Ulcers: Characterising the Microbiome of Ulcers. BMC Microbiol. 2016, 16, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pouget, C.; Dunyach-Remy, C.; Pantel, A.; Schuldiner, S.; Sotto, A.; Lavigne, J.P. Biofilms in Diabetic Foot Ulcers: Significance and Clinical Relevance. Microorganisms 2020, 8, 1580. [Google Scholar] [CrossRef] [PubMed]
- Donlan, R.M. Biofilms: Microbial Life on Surfaces. Emerg. Infect. Dis. 2002, 8, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Gupta, Y.; Agrawal, R.; Khare, P.; Jain, S.K. Biofilms—A Microbial Life Perspective: A Critical Review. Crit. Rev. Ther. Drug Carr. Syst. 2007, 24, 393–443. [Google Scholar] [CrossRef] [PubMed]
- Miere, F.; Teușdea, A.C.; Laslo, V.; Cavalu, S.; Fritea, L.; Dobjanschi, L.; Zdrinca, M.; Zdrinca, M.; Ganea, M.; Pașc, P.; et al. Evaluation of In Vitro Wound-Healing Potential, Antioxidant Capacity, and Antimicrobial Activity of Stellaria media (L.) Vill. Appl. Sci. 2021, 11, 11526. [Google Scholar] [CrossRef]
- Santos, R.; Veiga, A.S.; Tavares, L.; Castanho, M.; Oliveira, M. Bacterial Biofilms in Diabetic Foot Ulcers: Potential Alternative Therapeutics. In Microbial Biofilms—Importance and Applications; IntechOpen: London, UK, 2016. [Google Scholar]
- Messad, N.; Prajsnar, T.K.; Lina, G.; O’Callaghan, D.; Foster, S.J.; Renshaw, S.A.; Skaar, E.P.; Bes, M.; Dunyach-Remy, C.; Vandenesch, F.; et al. Existence of a Colonizing Staphylococcus Aureus Strain Isolated in Diabetic Foot Ulcers. Diabetes 2015, 64, 2991–2995. [Google Scholar] [CrossRef] [Green Version]
- Cavalu, S.; Simon, V. Proteins adsorption to orthopaedic biomaterials: Vibrational spectroscopy evidence. J. Optoelectron. Adv. Mater. 2007, 9, 3297–3302. [Google Scholar]
- Srivastava, P.; Sivashanmugam, K. Combinatorial Drug Therapy for Controlling Pseudomonas Aeruginosa and Its Association with Chronic Condition of Diabetic Foot Ulcer. Int. J. Low. Extrem. Wounds 2020, 19, 7–20. [Google Scholar] [CrossRef]
- Johani, K.; Malone, M.; Jensen, S.; Gosbell, I.; Dickson, H.; Hu, H.; Vickery, K. Microscopy Visualisation Confirms Multi-Species Biofilms Are Ubiquitous in Diabetic Foot Ulcers. Int. Wound J. 2017, 14, 1160–1169. [Google Scholar] [CrossRef]
- Shahi, S.K.; Kumar, A. Isolation and Genetic Analysis of Multidrug Resistant Bacteria from Diabetic Foot Ulcers. Front. Microbiol. 2016, 6, 1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, X.; Jin, P.; Chu, Y.; Feng, S.; Wang, P. Clinical Characteristics and Risk Factors of Diabetic Foot Ulcer with Multidrug-Resistant Organism Infection. Int. J. Low. Extrem. Wounds 2014, 13, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Zubair, M.; Malik, A.; Ahmad, J. Clinico-Bacteriology and Risk Factors for the Diabetic Foot Infection with Multidrug Resistant Microorganisms in North India. Biol. Med. 2010, 2, 22–34. [Google Scholar] [CrossRef]
- Xie, X.; Bao, Y.; Ni, L.; Liu, D.; Niu, S.; Lin, H.; Li, H.; Duan, C.; Yan, L.; Huang, S.; et al. Bacterial Profile and Antibiotic Resistance in Patients with Diabetic Foot Ulcer in Guangzhou, Southern China: Focus on the Differences among Different Wagner’s Grades, IDSA/IWGDF Grades, and Ulcer Types. Int. J. Endocrinol. 2017, 2017, 8694903. [Google Scholar] [CrossRef]
- Adeyemo, A.T.; Kolawole, B.; Rotimi, V.O.; Aboderin, A.O. Multicentre Study of the Burden of Multidrug-Resistant Bacteria in the Aetiology of Infected Diabetic Foot Ulcers. Afr. J. Lab. Med. 2021, 10, 1261. [Google Scholar] [CrossRef] [PubMed]
- Matta-Gutiérrez, G.; García-Morales, E.; García-Álvarez, Y.; Álvaro-Afonso, F.J.; Molines-Barroso, R.J.; Lázaro-Martínez, J.L. The Influence of Multidrug-Resistant Bacteria on Clinical Outcomes of Diabetic Foot Ulcers: A Systematic Review. J. Clin. Med. 2021, 10, 1948. [Google Scholar] [CrossRef]
- Apelqvist, J.; Larsson, J. What Is the Most Effective Way to Reduce Incidence of Amputation in the Diabetic Foot? Diabetes Metab. Res. Rev. 2000, 16, S75–S83. [Google Scholar] [CrossRef]
- Balows, A. Molecular Medical Microbiology. Diagn. Microbiol. Infect. Dis. 2002, 43, 173–174. [Google Scholar] [CrossRef]
- Tayeb, K.A. Managing Infection: A Holistic Approach. J. Wound Care 2015, 24, 20–30. [Google Scholar] [CrossRef]
- Attinger, C.; Wolcott, R. Clinically Addressing Biofilm in Chronic Wounds. Adv. Wound Care 2012, 1, 127–132. [Google Scholar] [CrossRef] [Green Version]
- Kataoka, Y.; Kunimitsu, M.; Nakagami, G.; Koudounas, S.; Weller, C.D.; Sanada, H. Effectiveness of Ultrasonic Debridement on Reduction of Bacteria and Biofilm in Patients with Chronic Wounds: A Scoping Review. Int. Wound J. 2021, 18, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Yarets, Y. Effective Biofilm Removal and Changes in Bacterial Biofilm Building Capacity after Wound Debridement with Low-Frequency Ultrasound as Part of Wound Bed Preparation before Skin Grafting. Chronic Wound Care Manag. Res. 2017, 4, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Dhar, Y.; Han, Y. Current Developments in Biofilm Treatments: Wound and Implant Infections. Eng. Regen. 2020, 1, 64–75. [Google Scholar] [CrossRef]
- Wolcott, R. Disrupting the Biofilm Matrix Improves Wound Healing Outcomes. J. Wound Care 2015, 24, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Dreyfus, J.; Delhougne, G.; James, R.; Gayle, J.; Waycaster, C. Clostridial Collagenase Ointment and Medicinal Honey Utilization for Pressure Ulcers in US Hospitals. J. Med. Econ. 2018, 21, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Waycaster, C.; Carter, M.J.; Gilligan, A.M.; Mearns, E.S.; Fife, C.E.; Milne, C.T. Comparative Cost and Clinical Effectiveness of Clostridial Collagenase Ointment for Chronic Dermal Ulcers. J. Comp. Eff. Res. 2018, 7, 149–165. [Google Scholar] [CrossRef] [Green Version]
- Lázaro-Martínez, J.L.; Álvaro-Afonso, F.J.; Sevillano-Fernández, D.; Molines-Barroso, R.J.; García-Álvarez, Y.; García-Morales, E. Clinical and Antimicrobial Efficacy of a Silver Foam Dressing with Silicone Adhesive in Diabetic Foot Ulcers with Mild Infection. Int. J. Low. Extrem. Wounds 2019, 18, 269–278. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Bolatai, A.; Wu, N. Application Progress of Nano Silver Dressing in the Treatment of Diabetic Foot. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 4145–4154. [Google Scholar] [CrossRef]
- Huang, C.; Wang, R.; Yan, Z. Silver Dressing in the Treatment of Diabetic Foot: A Protocol for Systematic Review and Meta-Analysis. Medicine 2021, 100, e24876. [Google Scholar] [CrossRef]
- Cavalu, S.; Roiu, G.; Pop, O.; Heredea, D.A.P.; Costea, T.O.; Costea, C.F. Nano-Scale Modifications of Amniotic Membrane Induced by UV and Antibiotic Treatment: Histological, AFM and FTIR Spectroscopy Evidence. Materials 2021, 14, 863. [Google Scholar] [CrossRef]
- Zhang, X.; Sun, D.; Jiang, G.C. Comparative Efficacy of Nine Different Dressings in Healing Diabetic Foot Ulcer: A Bayesian Network Analysis. J. Diabetes 2019, 11, 418–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dumville, J.C.; Deshpande, S.; O’Meara, S.; Speak, K. Hydrocolloid Dressings for Healing Diabetic Foot Ulcers. Cochrane Database Syst. Rev. 2013, 2013, CD009099. [Google Scholar] [CrossRef]
- Kwon, K.T.; Armstrong, D.G. Microbiology and Antimicrobial Therapy for Diabetic Foot Infections. Infect. Chemother. 2018, 50, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Haldar, J.; Mukherjee, P.; Mukhopadhyay, S.; Maiti, P.K. Isolation of Bacteria from Diabetic Foot Ulcers with Special Reference to Anaerobe Isolation by Simple Two-Step Combustion Technique in Candle Jar. Indian J. Med. Res. 2017, 145, 97–101. [Google Scholar] [CrossRef] [Green Version]
- Lipsky, B.A.; Armstrong, D.G.; Citron, D.M.; Tice, A.D.; Morgenstern, D.E.; Abramson, M.A. Ertapenem versus Piperacillin/Tazobactam for Diabetic Foot Infections (SIDESTEP): Prospective, Randomised, Controlled, Double-Blinded, Multicentre Trial. Lancet 2005, 366, 1695–1703. [Google Scholar] [CrossRef]
- Roberts, A.D.; Simon, G.L. Diabetic Foot Infections: The Role of Microbiology and Antibiotic Treatment. Semin. Vasc. Surg. 2012, 25, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Karri, V.V.S.R.; Kuppusamy, G.; Talluri, S.V.; Yamjala, K.; Mannemala, S.S.; Malayandi, R. Current and Emerging Therapies in the Management of Diabetic Foot Ulcers. Curr. Med. Res. Opin. 2016, 32, 519–542. [Google Scholar] [CrossRef]
- Ahmed, A.; Getti, G.; Boateng, J. Ciprofloxacin-Loaded Calcium Alginate Wafers Prepared by Freeze-Drying Technique for Potential Healing of Chronic Diabetic Foot Ulcers. Drug Deliv. Transl. Res. 2018, 8, 1751–1768. [Google Scholar] [CrossRef]
- Yingsakmongkol, N. Clinical Outcomes of WF10 Adjunct to Standard Treatment of Diabetic Foot Ulcers. J. Wound Care 2013, 22, 130–136. [Google Scholar] [CrossRef]
- Gasca-Lozano, L.E.; Lucano-Landeros, S.; Ruiz-Mercado, H.; Salazar-Montes, A.; Sandoval-Rodríguez, A.; Garcia-Bañuelos, J.; Santos-Garcia, A.; Davila-Rodriguez, J.R.; Navarro-Partida, J.; Bojórquez-Sepúlveda, H.; et al. Pirfenidone Accelerates Wound Healing in Chronic Diabetic Foot Ulcers: A Randomized, Double-Blind Controlled Trial. J. Diabetes Res. 2017, 2017, 3159798. [Google Scholar] [CrossRef]
- Ram, M.; Singh, V.; Kumawat, S.; Kumar, D.; Lingaraju, M.C.; Uttam Singh, T.; Rahal, A.; Kumar Tandan, S.; Kumar, D. Deferoxamine Modulates Cytokines and Growth Factors to Accelerate Cutaneous Wound Healing in Diabetic Rats. Eur. J. Pharmacol. 2015, 764, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Maderal, A.D.; Vivas, A.C.; Eaglstein, W.H.; Kirsner, R.S. The FDA and Designing Clinical Trials for Chronic Cutaneous Ulcers. Semin. Cell Dev. Biol. 2012, 23, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Tecilazich, F.; Dinh, T.L.; Veves, A. Emerging Drugs for the Treatment of Diabetic Ulcers. Expert Opin. Emerg. Drugs 2013, 18, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Richmond, N.A.; Vivas, A.C.; Kirsner, R.S. Topical and Biologic Therapies for Diabetic Foot Ulcers. Med. Clin. N. Am. 2013, 97, 883–898. [Google Scholar] [CrossRef] [PubMed]
- Kirsner, R.S.; Warriner, R.; Michela, M.; Stasik, L.; Freeman, K. Advanced Biological Therapies for Diabetic Foot Ulcers. Arch. Dermatol. 2010, 146, 857–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, L.; Setia, O.; Aurshina, A.; Liu, S.; Hu, H.; Isaji, T.; Liu, H.; Wang, T.; Ono, S.; Guo, X.; et al. Stem Cell Therapy for Diabetic Foot Ulcers: A Review of Preclinical and Clinical Research. Stem Cell Res. Ther. 2018, 9, 188. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Gang, X.; Sun, C.; Wang, G. Mesenchymal Stem Cells Improve Healing of Diabetic Foot Ulcer. J. Diabetes Res. 2017, 2017, 9328347. [Google Scholar] [CrossRef]
- Davani, F.; Alishahi, M.; Sabzi, M.; Khorram, M.; Arastehfar, A.; Zomorodian, K. Dual Drug Delivery of Vancomycin and Imipenem/Cilastatin by Coaxial Nanofibers for Treatment of Diabetic Foot Ulcer Infections. Mater. Sci. Eng. C 2021, 123, 111975. [Google Scholar] [CrossRef]
- Agbi, K.E.; Carvalho, M.; Phan, H.; Tuma, C. Case Report: Diabetic Foot Ulcer Infection Treated with Topical Compounded Medications. Int. J. Pharm. Compd. 2017, 21, 22–27. [Google Scholar]
- Shi, E.; Shofler, D. Maggot Debridement Therapy: A Systematic Review. Br. J. Community Nurs. 2014, 19, S6–S13. [Google Scholar] [CrossRef]
- Naik, G.; Harding, K. Maggot Debridement Therapy: The Current Perspectives. Chronic Wound Care Manag. Res. 2017, 4, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, M.A.R.Q.; Ferraz, J.B.; Junior, M.A.A.; Moura, A.D.; da Costa, M.E.S.M.; Costa, F.J.M.D.; Neto, V.F.A.; Neto, R.M.; Gama, R.A. Use of Maggot Therapy for Treating a Diabetic Foot Ulcer Colonized by Multidrug Resistant Bacteria in Brazil. Indian J. Med. Res. Suppl. 2015, 141, 340–342. [Google Scholar] [CrossRef]
- Parizad, N.; Hajimohammadi, K.; Goli, R. Surgical Debridement, Maggot Therapy, Negative Pressure Wound Therapy, and Silver Foam Dressing Revive Hope for Patients with Diabetic Foot Ulcer: A Case Report. Int. J. Surg. Case Rep. 2021, 82, 105931. [Google Scholar] [CrossRef]
- Maranna, H.; Lal, P.; Mishra, A.; Bains, L.; Sawant, G.; Bhatia, R.; Kumar, P.; Beg, M.Y. Negative Pressure Wound Therapy in Grade 1 and 2 Diabetic Foot Ulcers: A Randomized Controlled Study. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Finžgar, M.; Frangež, H.B.; Cankar, K.; Frangež, I. Transcutaneous Application of the Gaseous CO2 for Improvement of the Microvascular Function in Patients with Diabetic Foot Ulcers. Microvasc. Res. 2021, 133, 104100. [Google Scholar] [CrossRef]
- Fang, J.; Xu, J.; Zhang, Y.; Chen, H.; Ma, Z.; Huang, Z.; Hu, J. Stromal Cell-Derived Factor-1 May Play Pivotal Role in Distraction-Stimulated Neovascularization of Diabetic Foot Ulcer. Med. Hypotheses 2021, 149, 110548. [Google Scholar] [CrossRef] [PubMed]
- Ratiu, C.; Brocks, M.; Costea, T.; Moldovan, L.; Cavalu, S. PRGF-Modified Collagen Membranes for Guided Bone Regeneration: Spectroscopic, Microscopic and Nano-Mechanical Investigations. Appl. Sci. 2019, 9, 1035. [Google Scholar] [CrossRef] [Green Version]
- Shao, S.; Pan, R.; Chen, Y. Autologous Platelet-Rich Plasma for Diabetic Foot Ulcer. Trends Endocrinol. Metab. 2020, 31, 885–890. [Google Scholar] [CrossRef]
- Uzun, E.; Güney, A.; Gönen, Z.B.; Özkul, Y.; Kafadar, İ.H.; Günay, M.; Mutlu, M. Intralesional Allogeneic Adipose-Derived Stem Cells Application in Chronic Diabetic Foot Ulcer: Phase I/2 Safety Study. Foot Ankle Surg. 2020, 27, 636–642. [Google Scholar] [CrossRef]
- He, S.; Liang, C.; Yi, C.; Wu, M. Therapeutic Effect of Continuous Diffusion of Oxygen Therapy Combined with Traditional Moist Wound Dressing Therapy in the Treatment of Diabetic Foot Ulcers. Diabetes Res. Clin. Pract. 2021, 174, 108743. [Google Scholar] [CrossRef]
- Terabe, Y.; Kaneko, N.; Nakabayashi, K.; Matsui, A.; Ando, H. Long-Term Efficient Management of Diabetic Foot Ulcer Using Simultaneous Foot Ulcer Closure and Surgical off-Loading. JPRAS Open 2021, 30, 1–5. [Google Scholar] [CrossRef]
- Srivastava, P.; Sivashanmugam, K. Efficacy of Sub-MIC Level of Meropenem and Ciprofloxacin against Extensive Drug-Resistant (XDR) Pseudomonas Aeruginosa Isolates of Diabetic Foot Ulcer Patients. Infect. Genet. Evol. 2021, 92, 104824. [Google Scholar] [CrossRef] [PubMed]
- Elsadek, N.E.; Nagah, A.; Ibrahim, T.M.; Chopra, H.; Ghonaim, G.A.; Emam, S.E.; Cavalu, S.; Attia, M.S. Electrospun Nanofibers Revisited: An Update on the Emerging Applications in Nanomedicine. Materials 2022, 15, 1934. [Google Scholar] [CrossRef] [PubMed]
- Fadol, E.M.; Suliman, H.M.; Osman, B.; Abdalla, S.A.; Osman, W.J.A.; Mohamed, E.M.; Abdoon, I.H. Therapeutic Outcomes Evaluation of Adjuvant Hyperbaric Oxygen Therapy for Non-Healing Diabetic Foot Ulcers among Sudanese Patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 102173. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Ding, X.; Jing, Z.; Lu, H.; Yang, K.; Wang, Y.; Xu, H. Modified Tibial Transverse Transport Technique for the Treatment of Ischemic Diabetic Foot Ulcer in Patients with Type 2 Diabetes. J. Orthop. Transl. 2021, 29, 100–105. [Google Scholar] [CrossRef]
- Suresh, T.C.; Poonguzhali, T.V.; Anuradha, V.; Ramesh, B.; Suresh, G. Aqueous Extract of Turbinaria conoides (J.Agardh) Kutzing Mediated Fabrication of Silver Nanoparticles Used against Bacteria Associated with Diabetic Foot Ulcer. Mater. Today Proc. 2021, 43, 3038–3043. [Google Scholar] [CrossRef]
- Dixon, D.; Edmonds, M. Managing Diabetic Foot Ulcers: Pharmacotherapy for Wound Healing. Drugs 2021, 81, 29–56. [Google Scholar] [CrossRef]
- Pasca, P.M.; Cavalu, S. The Influence of Propolis Nanoparticles on Dermal Fibroblasts Migration: Premises for Development of Propolis-Based Collagen Dermal Patches. Dig. J. Nanomater. Biostruct. 2021, 16, 929–938. [Google Scholar]
- Cavalu, S.; Fritea, L.; Brocks, M.; Barbaro, K.; Murvai, G.; Costea, T.O.; Antoniac, I.; Verona, C.; Romani, M.; Latini, A.; et al. Novel Hybrid Composites Based on PVA/SeTiO2 Nanoparticles and Natural Hydroxyapatite for Orthopedic Applications: Correlations between Structural, Morphological and Biocompatibility Properties. Materials 2020, 13, 2077. [Google Scholar] [CrossRef]
- Alavi, M.; Nokhodchi, A. Antimicrobial and Wound Treatment Aspects of Micro- and Nanoformulations of Carboxymethyl, Dialdehyde, and TEMPO-Oxidized Derivatives of Cellulose: Recent Advances. Macromol. Biosci. 2020, 20, 1900362. [Google Scholar] [CrossRef]
- Anwar, K.; Hussein, D.; Salih, J. Antimicrobial Susceptibility Testing and Phenotypic Detection of MRSA Isolated from Diabetic Foot Infection. Int. J. Gen. Med. 2020, 13, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Alhubail, A.; Sewify, M.; Messenger, G.; Masoetsa, R.; Hussain, I.; Nair, S.; Tiss, A. Microbiological Profile of Diabetic Foot Ulcers in Kuwait. PLoS ONE 2020, 15, e0244306. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baig, M.S.; Banu, A.; Zehravi, M.; Rana, R.; Burle, S.S.; Khan, S.L.; Islam, F.; Siddiqui, F.A.; Massoud, E.E.S.; Rahman, M.H.; et al. An Overview of Diabetic Foot Ulcers and Associated Problems with Special Emphasis on Treatments with Antimicrobials. Life 2022, 12, 1054. https://doi.org/10.3390/life12071054
Baig MS, Banu A, Zehravi M, Rana R, Burle SS, Khan SL, Islam F, Siddiqui FA, Massoud EES, Rahman MH, et al. An Overview of Diabetic Foot Ulcers and Associated Problems with Special Emphasis on Treatments with Antimicrobials. Life. 2022; 12(7):1054. https://doi.org/10.3390/life12071054
Chicago/Turabian StyleBaig, Mirza Shahed, Ahmadi Banu, Mehrukh Zehravi, Ritesh Rana, Sushil S. Burle, Sharuk L. Khan, Fahadul Islam, Falak A. Siddiqui, Ehab El Sayed Massoud, Md. Habibur Rahman, and et al. 2022. "An Overview of Diabetic Foot Ulcers and Associated Problems with Special Emphasis on Treatments with Antimicrobials" Life 12, no. 7: 1054. https://doi.org/10.3390/life12071054