
Ischemic Heart Disease and Liver Cirrhosis: Adding Insult to Injury

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Epidemiology, Clinical Presentation and Risk Factors
2.1. Epidemiology of CAD in LC
2.2. Clinical Presentation of CAD in LC
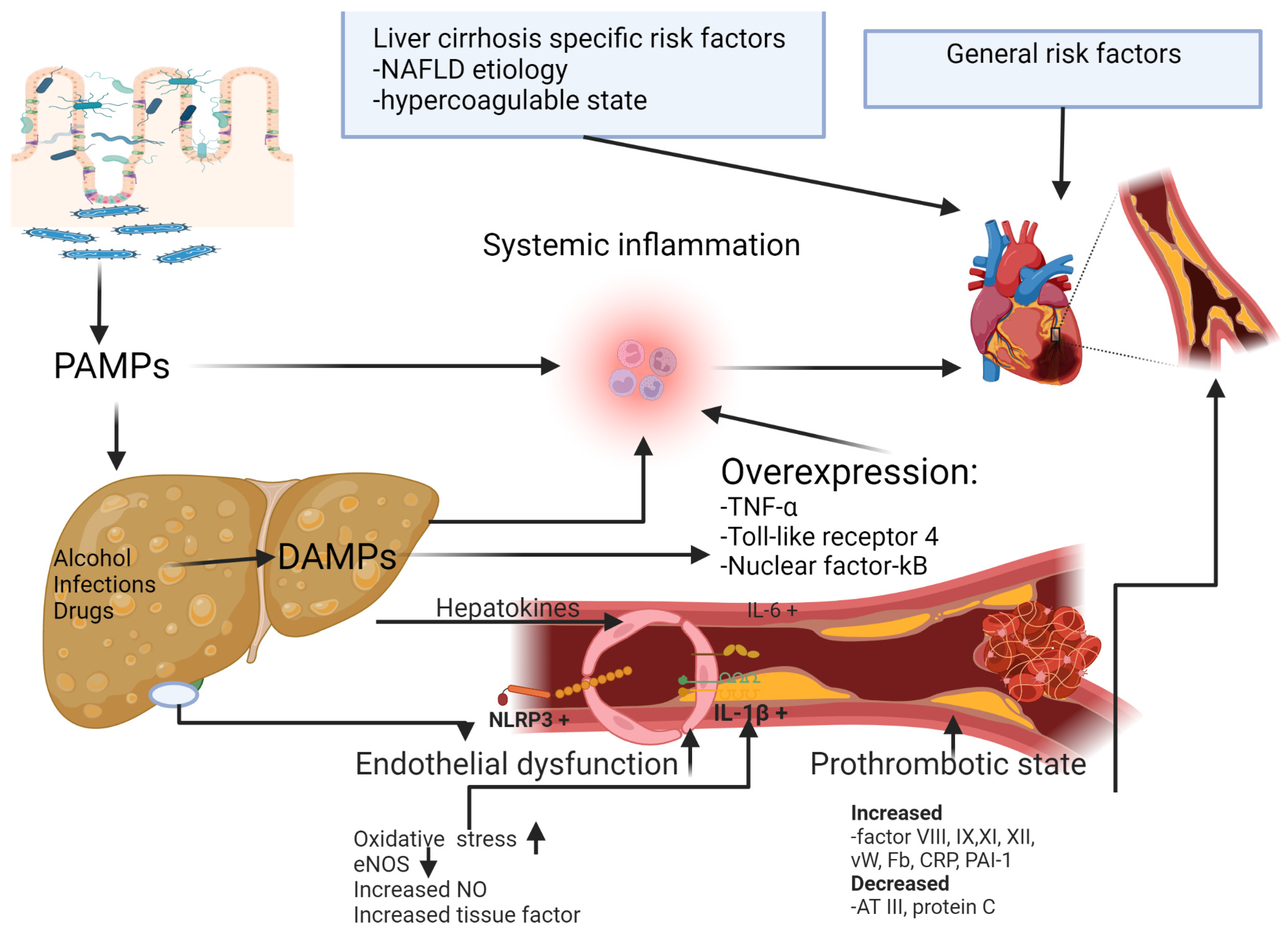
2.3. Risk Factors for CAD in LC
3. Etiology of Liver Cirrhosis and CAD
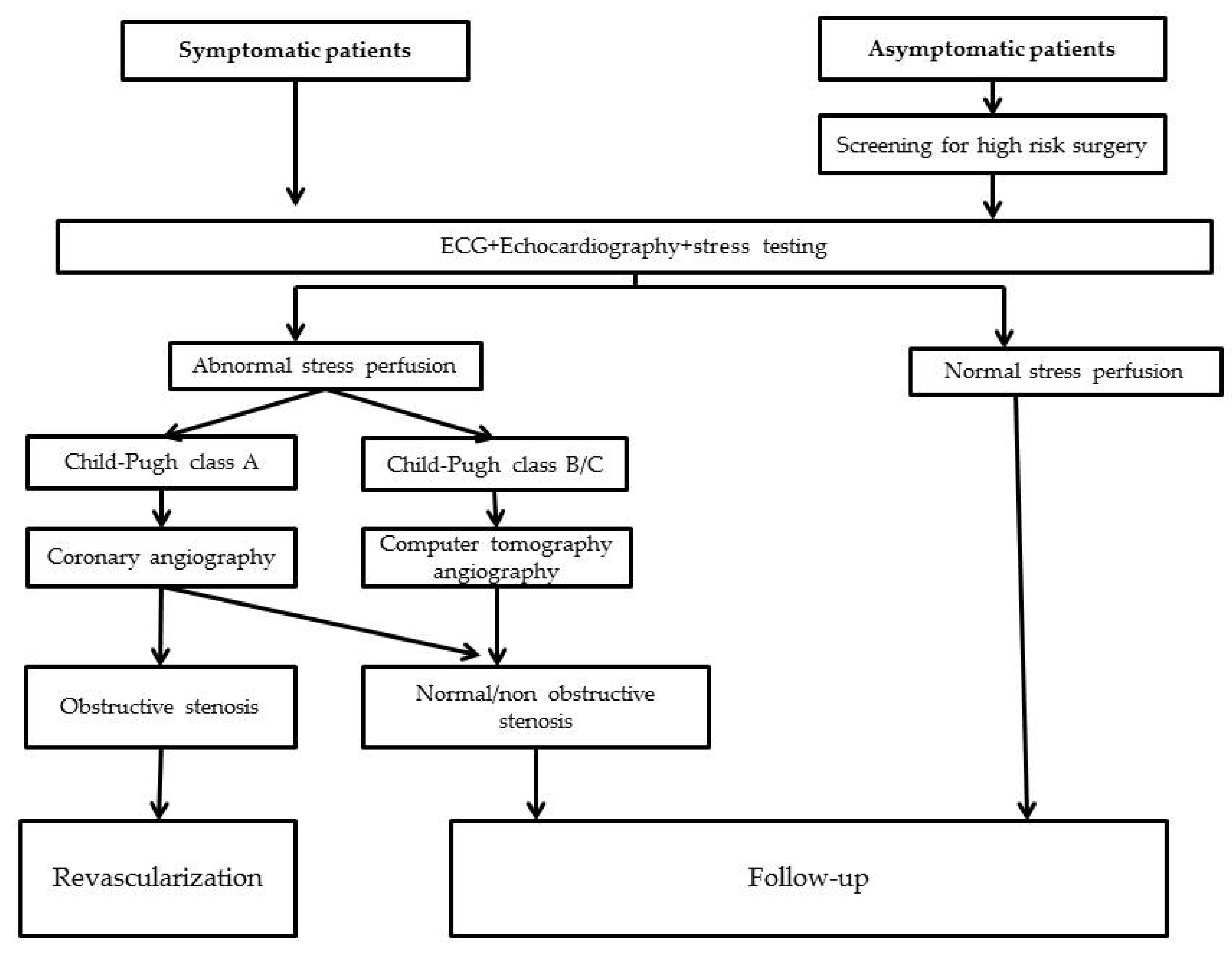
4. CAD Diagnosis in Liver Cirrhosis
5. Management of CAD in Liver Cirrhosis
5.1. Medical Therapy
5.2. Revascularization in Patients with CAD and Liver Cirrhosis
5.2.1. Percutaneous Coronary Intervention (PCI)
5.2.2. Coronary Artery Bypass Grafting (CABG)
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Vairappan, B. Endothelial dysfunction in cirrhosis: Role of inflammation and oxidative stress. World. J. Hepatol. 2015, 7, 443. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Jing, X.; Wu, C.; Zeng, Y.; Xie, Y.; Wang, M.; Chen, W.; Hu, X.; Zhou, Y.; Cai, X. Nonalcoholic Fatty Liver Disease-Associated Liver Fibrosis Is Linked with the Severity of Coronary Artery Disease Mediated by Systemic Inflammation. Dis. Markers 2021, 2021, 6591784. [Google Scholar] [CrossRef] [PubMed]
- El Hadi, H.; Di Vincenzo, A.; Vettor, R.; Rossato, M. Relationship between Heart Disease and Liver Disease: A Two-Way Street. Cells 2020, 9, 567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lluch, P.; Torondel, B.; Medina, P.; Segarra, G.; del Olmo, J.A.; Serra, M.A.; Rodrigo, J.M. Plasma concentrations of nitric oxide and asymmetric dimethylarginine in human alcoholic cirrhosis. J. Hepatol. 2004, 41, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Deanfield, J.E.; Halcox, J.P.; Rabelink, T.J. Endothelial Function and Dysfunction: Testing and Clinical Relevance. Circulation 2007, 115, 1285–1295. [Google Scholar] [CrossRef]
- Albillos, A.; Lario, M.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction: Distinctive features and clinical relevance. J. Hepatol. 2014, 61, 1385–1396. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Desert, R.; Das, S.; Song, Z.; Athavale, D.; Ge, X.; Nieto, N. Danger signals in liver injury and restoration of homeostasis. J. Hepatol. 2020, 73, 933–951. [Google Scholar] [CrossRef]
- Noda, Y.; Nomura, M.; Nakaya, Y.; Bando, S.; Ito, S. Relationship between liver cirrhosis and arteriosclerosis: Evaluation by pulse wave velocity, carotid arterial echotomography and autonomic nervous activity. Geriatr. Gerontol. Int. 2007, 7, 72–79. [Google Scholar] [CrossRef]
- Lin, S.-Y.; Lin, C.-L.; Lin, C.-C.; Wang, I.-K.; Hsu, W.-H.; Kao, C.-H. Risk of acute coronary syndrome and peripheral arterial disease in chronic liver disease and cirrhosis: A nationwide population-based study. Atherosclerosis 2018, 270, 154–159. [Google Scholar] [CrossRef]
- An, J.; Shim, J.H.; Kim, S.-O.; Lee, D.; Kim, K.M.; Lim, Y.-S.; Lee, H.C.; Chung, Y.-H.; Lee, Y.S. Prevalence and Prediction of Coronary Artery Disease in Patients With Liver Cirrhosis: A Registry-Based Matched Case–Control Study. Circulation 2014, 130, 1353–1362. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Li, N.; Sun, H.; Liang, C. The prevalence of coronary artery disease in patients with liver cirrhosis: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2018, 30, 118–120. [Google Scholar] [CrossRef]
- Patel, S.; Kiefer, T.L.; Ahmed, A.; Ali, Z.A.; Tremmel, J.A.; Lee, D.P.; Yeung, A.C.; Fearon, W.F. Comparison of the frequency of coronary artery disease in alcohol-related versus non-alcohol-related endstage liver disease. Am. J. Cardiol. 2011, 108, 1552–1555. [Google Scholar] [CrossRef]
- Patel, S.S.; Nabi, E.; Guzman, L.; Abbate, A.; Bhati, C.; Stravitz, R.T.; Reichman, T.; Matherly, S.C.; Driscoll, C.; Lee, H.; et al. Coronary artery disease in decompensated patients undergoing liver transplantation evaluation. Liver Transpl. 2018, 24, 333–342. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.; Siddiqui, M.B.; Chandrakumaran, A.; Rodriguez, V.A.; Faridnia, M.; Roman, J.H.; Zhang, E.; Patrone, M.V.; Kakiyama, G.; Walker, C.; et al. Progression to Cirrhosis Leads to Improvement in Atherogenic Milieu. Dig. Dis. Sci. 2021, 66, 263–272. [Google Scholar] [CrossRef]
- Azarbal, B.; Poommipanit, P.; Arbit, B.; Hage, A.; Patel, J.; Kittleson, M.; Kar, S.; Kaldas, F.M.; Busuttil, R.W. Feasibility and safety of percutaneous coronary intervention in patients with end-stage liver disease referred for liver transplantation. Liver Transpl. 2011, 17, 809–813. [Google Scholar] [CrossRef]
- Berzigotti, A.; Bonfiglioli, A.; Muscari, A.; Bianchi, G.; LiBassi, S.; Bernardi, M.; Zoli, M. Reduced prevalence of ischemic events and abnormal supraortic flow patterns in patients with liver cirrhosis. Liver Int. 2005, 25, 331–336. [Google Scholar] [CrossRef]
- McAvoy, N.C.; Kochar, N.; McKillop, G.; Newby, D.E.; Hayes, P.C. Prevalence of coronary artery calcification in patients undergoing assessment for orthotopic liver transplantation: Prevalence of Coronary Artery Calcification. Liver Transpl. 2008, 14, 1725–1731. [Google Scholar] [CrossRef]
- Gologorsky, E.; Pretto, E.A.; Fukazawa, K. Coronary artery disease and its risk factors in patients presenting for liver transplantation. J. Clin. Anesth. 2013, 25, 618–623. [Google Scholar] [CrossRef]
- Dangl, M.; Eisenberg, T.; Grant, J.K.; Vincent, L.; Colombo, R.; Sancassani, R.; Braghiroli, J.; Martin, P.; Vianna, R.; Nicolau-Raducu, R.; et al. A comprehensive review of coronary artery disease in patients with end-stage liver disease. Transpl. Rev. 2022, 36, 100709. [Google Scholar] [CrossRef]
- Tamarappoo, B.K.; Lin, A.; Commandeur, F.; McElhinney, P.A.; Cadet, S.; Goeller, M.; Razipour, A.; Chen, X.; Gransar, H.; Cantu, S.; et al. Machine learning integration of circulating and imaging biomarkers for explainable patient-specific prediction of cardiac events: A prospective study. Atherosclerosis 2021, 318, 76–82. [Google Scholar] [CrossRef]
- Huang, H.; Ho, H.; Chang, C.; Chuang, C.; Pun, C.K.; Lee, F.; Huang, Y.; Hou, M.; Hsu, S. Matrix metalloproteinase-9 inhibition or deletion attenuates portal hypertension in rodents. J. Cell. Mol. Med. 2021, 25, 10073–10087. [Google Scholar] [CrossRef]
- Balin, Ş.Ö.; Çabalak, M.; Tartar, A.S.; Kazancı, Ü.; Telo, S.; Demirdağ, K.; Akbulut, A. Pentraxin-3: A Novel Marker for Indicating Liver Fibrosis in Chronic Hepatitis B Patients? Turk. J. Gastroenterol. 2021, 32, 581–585. [Google Scholar] [CrossRef]
- Prystupa, A.; Kiciński, P.; Luchowska-Kocot, D.; Błażewicz, A.; Niedziałek, J.; Mizerski, G.; Jojczuk, M.; Ochal, A.; Sak, J.J.; Załuska, W. Association between Serum Selenium Concentrations and Levels of Proinflammatory and Profibrotic Cytokines-Interleukin-6 and Growth Differentiation Factor-15, in Patients with Alcoholic Liver Cirrhosis. Int. J. Environ. Res. Public Health 2017, 14, E437. [Google Scholar] [CrossRef]
- Graupera, I.; Solà, E.; Fabrellas, N.; Moreira, R.; Solé, C.; Huelin, P.; de la Prada, G.; Pose, E.; Ariza, X.; Risso, A.; et al. Urine Monocyte Chemoattractant Protein-1 Is an Independent Predictive Factor of Hospital Readmission and Survival in Cirrhosis. PLoS ONE 2016, 11, e0157371. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Kim, H.S.; Cho, Y.K.; Kim, E.H.; Lee, M.J.; Bae, I.Y.; Jung, C.H.; Park, J.-Y.; Kim, H.-K.; Lee, W.J. Association between noninvasive assessment of liver fibrosis and coronary artery calcification progression in patients with nonalcoholic fatty liver disease. Sci. Rep. 2020, 10, 18323. [Google Scholar] [CrossRef]
- Turan, Y. The Nonalcoholic Fatty Liver Disease Fibrosis Score Is Related to Epicardial Fat Thickness and Complexity of Coronary Artery Disease. Angiology 2020, 71, 77–82. [Google Scholar] [CrossRef]
- Kadayifci, A.; Tan, V.; Ursell, P.C.; Merriman, R.B.; Bass, N.M. Clinical and pathologic risk factors for atherosclerosis in cirrhosis: A comparison between NASH-related cirrhosis and cirrhosis due to other aetiologies. J. Hepatol. 2008, 49, 595–599. [Google Scholar] [CrossRef]
- Arslan, U.; Kocaoğlu, İ.; Balcı, M.; Duyuler, S.; Korkmaz, A. The association between impaired collateral circulation and non-alcoholic fatty liver in patients with severe coronary artery disease. J. Cardiol. 2012, 60, 210–214. [Google Scholar] [CrossRef] [Green Version]
- Ağaç, M.T.; Korkmaz, L.; Çavuşoğlu, G.; Karadeniz, A.G.; Ağaç, S.; Bektas, H.; Erkan, H.; Varol, M.O.; Vatan, M.B.; Acar, Z.; et al. Association Between Nonalcoholic Fatty Liver Disease and Coronary Artery Disease Complexity in Patients With Acute Coronary Syndrome: A Pilot Study. Angiology 2013, 64, 604–608. [Google Scholar] [CrossRef]
- Akabame, S.; Hamaguchi, M.; Tomiyasu, K.; Tanaka, M.; Kobayashi-Takenaka, Y.; Nakano, K.; Oda, Y.; Yoshikawa, T. Evaluation of Vulnerable Coronary Plaques and Non-Alcoholic Fatty Liver Disease (NAFLD) by 64-Detector Multislice Computed Tomography (MSCT). Circ. J. 2007, 72, 618–625. [Google Scholar] [CrossRef] [Green Version]
- Kazankov, K.; Munk, K.; Øvrehus, K.A.; Jensen, J.M.; Siggaard, C.B.; Grønbaek, H.; Nørgaard, B.L.; Vilstrup, H. High burden of coronary atherosclerosis in patients with cirrhosis. Eur. J. Clin. Invest. 2017, 47, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Friedrich-Rust, M.; Schoelzel, F.; Maier, S.; Seeger, F.; Rey, J.; Fichtlscherer, S.; Herrmann, E.; Zeuzem, S.; Bojunga, J. Severity of coronary artery disease is associated with non-alcoholic fatty liver dis-ease: A single-blinded prospective mono-center study. PLoS ONE 2017, 12, e0186720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.-C.; Yang, T.-W.; Wang, C.-C.; Wang, Y.-T.; Sung, W.-W.; Tseng, M.-H.; Lin, C.-C. Favorable clinical outcome of nonalcoholic liver cirrhosis patients with coronary artery disease: A population-based study. World J. Gastroenterol. 2018, 24, 3547–3555. [Google Scholar] [CrossRef] [PubMed]
- Chiriac, S.; Stanciu, C.; Girleanu, I.; Cojocariu, C.; Sfarti, C.; Singeap, A.-M.; Cuciureanu, T.; Huiban, L.; Muzica, C.M.; Zenovia, S.; et al. Nonalcoholic Fatty Liver Disease and Cardiovascular Diseases: The Heart of the Matter. Can. J. Gastroenterol. Hepatol. 2021, 2021, 6696857. [Google Scholar] [CrossRef]
- Kalaitzakis, E.; Rosengren, A.; Skommevik, T.; Björnsson, E. Coronary Artery Disease in Patients with Liver Cirrhosis. Dig. Dis. Sci. 2010, 55, 467–475. [Google Scholar] [CrossRef]
- Alyan, O.; Kacmaz, F.; Ozdemir, O.; Deveci, B.; Astan, R.; Celebi, A.S.; Ilkay, E. Hepatitis C Infection is Associated With Increased Coronary Artery Atherosclerosis Defined by Modified Reardon Severity Score System. Circ. J. 2008, 72, 1960–1965. [Google Scholar] [CrossRef] [Green Version]
- Dai, C.-Y.; Yeh, M.-L.; Huang, C.-F.; Hou, C.-H.; Hsieh, M.-Y.; Huang, J.-F.; Lin, I.-L.; Lin, Z.-Y.; Chen, S.-C.; Wang, L.-Y.; et al. Chronic hepatitis C infection is associated with insulin resistance and lipid profiles: Metabolic profiles and hepatitis C. J. Gastroenterol. Hepatol. 2015, 30, 879–884. [Google Scholar] [CrossRef]
- Cuciureanu, T.; Chiriac, S.; Chiorescu, M.; Gîrleanu, I.; Trifan, A. Chronic hepatitis C virus infection: A new modifiable cardio-metabolic risk factor? Clujul Med. 2017, 90, 251–255. [Google Scholar] [CrossRef] [Green Version]
- Barakat, A.A.E.-K.; Nasr, F.M.; Metwaly, A.A.; Morsy, S.; Eldamarawy, M. Atherosclerosis in chronic hepatitis C virus patients with and without liver cirrhosis. Egypt. Heart J. 2017, 69, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Adinolfi, L.E.; Rinaldi, L.; Nevola, R. Chronic hepatitis C, atherosclerosis and cardiovascular disease: What impact of direct-acting antiviral treatments? World J. Gastroenterol. 2018, 24, 4617–4621. [Google Scholar] [CrossRef]
- Roguljic, H.; Nincevic, V.; Bojanic, K.; Kuna, L.; Smolic, R.; Vcev, A.; Primorac, D.; Vceva, A.; Wu, G.Y.; Smolic, M. Impact of DAA Treatment on Cardiovascular Disease Risk in Chronic HCV Infection: An Update. Front. Pharmacol. 2021, 12, 678546. [Google Scholar] [CrossRef]
- Wang, C.; Zhao, P.; Liu, W. Risk of incident coronary artery disease in patients with primary biliary cirrhosis. Int. J. Clin. Exp. Med. 2014, 7, 2921–2924. [Google Scholar]
- Longo, M.; Crosignani, A.; Battezzati, P.M.; Giussani, S.C.; Invernizzi, P.; Zuin, M.; Podda, M. Hyperlipidaemic state and cardiovascular risk in primary biliary cirrhosis. Gut 2002, 51, 265–269. [Google Scholar] [CrossRef] [Green Version]
- Crippin, J.S.; Lindor, K.D.; Jorgensen, R.; Kottke, B.A.; Harrison, J.M.; Murtaugh, P.A.; Dickson, E.R. Hypercholesterolemia and atherosclerosis in primary biliary cirrhosis: What is the risk? Hepatology 1992, 15, 858–862. [Google Scholar] [CrossRef]
- Van Dam, G.M.; Gips, C.H. Primary Biliary Cirrhosis in The Netherlands: An Analysis of Associated Diseases, Cardiovascular Risk, and Malignancies on the Basis of Mortality Figures. Scand. J. Gastroenterol. 1997, 32, 77–83. [Google Scholar] [CrossRef]
- Ungprasert, P.; Wijarnpreecha, K.; Ahuja, W.; Spanuchart, I.; Thongprayoon, C. Coronary artery disease in primary biliary cirrhosis: A systematic review and meta-analysis of observational studies: CAD in PBC. Hepatol. Res. 2015, 45, 1055–1061. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Thygesen, K.; Mair, J.; Katus, H.; Plebani, M.; Venge, P.; Collinson, P.; Lindahl, B.; Giannitsis, E.; Hasin, Y.; Galvani, M.; et al. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur. Heart J. 2010, 31, 2197–2204. [Google Scholar] [CrossRef] [Green Version]
- Shimoni, Z.; Arbuzov, R.; Froom, P. Troponin Testing in Patients Without Chest Pain or Electrocardiographic Ischemic Changes. Am. J. Med. 2017, 130, 1205–1210. [Google Scholar] [CrossRef]
- Zardi, E.M.; Abbate, A.; Zardi, D.M.; Dobrina, A.; Margiotta, D.; Van Tassel, B.W.; Afeltra, A.; Sanyal, A.J. Cirrhotic Cardiomyopathy. J. Am. Coll. Cardiol. 2010, 56, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Wiese, S.; Mortensen, C.; Gøtze, J.P.; Christensen, E.; Andersen, O.; Bendtsen, F.; Møller, S. Cardiac and proinflammatory markers predict prognosis in cirrhosis. Liver Int. 2014, 34, e19–e30. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization. J. Am. Coll. Cardiol. 2022, 79, e21–e129. [Google Scholar] [CrossRef]
- Jacobs, E.; Singh, V.; Damluji, A.; Shah, N.R.; Warsch, J.L.; Ghanta, R.; Martin, P.; Alfonso, C.E.; Martinez, C.A.; Moscucci, M.; et al. Safety of transradial cardiac catheterization in patients with end-stage liver disease: Transradial catheterization in ESLD. Catheter. Cardiovasc. Interv. 2014, 83, 360–366. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver transplantation. J. Hepatol. 2016, 64, 433–485. [Google Scholar] [CrossRef]
- Martin, P.; DiMartini, A.; Feng, S.; Brown, R.; Fallon, M. Evaluation for liver transplantation in adults: 2013 practice guideline. Hepatology 2014, 59, 1144–1165. [Google Scholar] [CrossRef]
- Mori, T.; Nomura, M.; Hori, A.; Kondo, N.; Bando, S.; Ito, S. Mechanism of ST segment depression during exercise tests in patients with liver cirrhosis. J. Med. Invest. 2007, 54, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Harinstein, M.E.; Flaherty, J.D.; Ansari, A.H.; Robin, J.; Davidson, C.J.; Rossi, J.S.; Flamm, S.L.; Blei, A.T.; Bonow, R.O.; Abecassis, M.; et al. Predictive Value of Dobutamine Stress Echocardiography for Coronary Artery Disease Detection in Liver Transplant Candidates: DSE in Liver Transplant Candidates. Am. J. Transplant. 2008, 8, 1523–1528. [Google Scholar] [CrossRef]
- Doytchinova, A.T.; Feigenbaum, T.D.; Pondicherry-Harish, R.C.; Sepanski, P.; Green-Hess, D.; Feigenbaum, H.; Sawada, S.G. Diagnostic Performance of Dobutamine Stress Echocardiography in End-Stage Liver Disease. JACC Cardiovasc. Imaging 2019, 12, 2115–2122. [Google Scholar] [CrossRef]
- Bhatti, S.; Lizaola-Mayo, B.; Al-Shoha, M.; Garcia-Saenz-de-Sicilia, M.; Habash, F.; Ayoub, K.; Karr, M.; Ahmed, Z.; Borja-Cacho, D.; Duarte-Rojo, A. Use of Computed Tomography Coronary Calcium Score for Coronary Artery Disease Risk Stratification During Liver Transplant Evaluation. J. Clin. Exp. Hepatol. 2022, 12, 319–328. [Google Scholar] [CrossRef]
- Greenland, P.; Blaha, M.J.; Budoff, M.J.; Erbel, R.; Watson, K.E. Coronary Calcium Score and Cardiovascular Risk. J. Am. Coll. Cardiol. 2018, 72, 434–447. [Google Scholar] [CrossRef] [PubMed]
- Klem, I.; Heitner, J.F.; Shah, D.J.; Sketch, M.H.; Behar, V.; Weinsaft, J.; Cawley, P.; Parker, M.; Elliott, M.; Judd, R.M.; et al. Improved Detection of Coronary Artery Disease by Stress Perfusion Cardiovascular Magnetic Resonance With the Use of Delayed Enhancement Infarction Imaging. J. Am. Coll. Cardiol. 2006, 47, 1630–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Peuter, O.R.; Lussana, F.; Peters, R.J.G.; Büller, H.R.; Kamphuisen, P.W. A systematic review of selective and non-selective beta blockers for prevention of vascular events in patients with acute coronary syndrome or heart failure. Neth. J. Med. 2009, 67, 284–294. [Google Scholar] [PubMed]
- Krill, T.; Brown, G.; Weideman, R.A.; Cipher, D.J.; Spechler, S.J.; Brilakis, E.; Feagins, L.A. Patients with cirrhosis who have coronary artery disease treated with cardiac stents have high rates of gastrointestinal bleeding, but no increased mortality. Aliment. Pharmacol. Ther. 2017, 46, 183–192. [Google Scholar] [CrossRef]
- Trankle, C.R.; Vo, C.; Martin, E.; Puckett, L.; Siddiqui, M.S.; Brophy, D.F.; Stravitz, T.; Guzman, L.A. Clopidogrel Responsiveness in Patients With Decompensated Cirrhosis of the Liver Undergoing Pre-Transplant PCI. JACC Cardiovasc. Interv. 2020, 13, 661–663. [Google Scholar] [CrossRef]
- Ostojic, Z.; Ostojic, A.; Bulum, J.; Mrzljak, A. Safety and efficacy of dual antiplatelet therapy after percutaneous coronary interventions in patients with end-stage liver disease. World J. Cardiol. 2021, 13, 599–607. [Google Scholar] [CrossRef]
- Slugg, P.H.; Much, D.R.; Smith, W.B.; Vargas, R.; Nichola, P.; Necciari, J. Cirrhosis Does Not Affect the Pharmacokinetics and Pharmacodynamics of Clopidogrel. J. Clin. Pharmacol. 2000, 40, 396–401. [Google Scholar] [CrossRef]
- Wood, A.; Eghtesad, B.; Menon, K.V.N.; Fares, M.; Tong, M.Z.-Y.; Sharma, V.; Lopez, R.; Modaresi Esfeh, J. Safety and Outcomes of Combined Liver Transplantation and Cardiac Surgery in Cirrhosis. Ann. Thorac. Surg. 2021, 111, 62–68. [Google Scholar] [CrossRef]
- Zhang, M.; You, X.; Ke, M.; Jiao, Z.; Wu, H.; Huang, P.; Lin, C. Prediction of Ticagrelor and its Active Metabolite in Liver Cirrhosis Populations Using a Physiologically Based Pharmacokinetic Model Involving Pharmacodynamics. J. Pharm. Sci. 2019, 108, 2781–2790. [Google Scholar] [CrossRef]
- Ahmed, T.; Grigorian, A.Y.; Messerli, A.W. Management of Acute Coronary Syndrome in Patients with Liver Cirrhosis. Am. J. Cardiovasc. Drugs 2022, 22, 55–67. [Google Scholar] [CrossRef]
- Weinreich, M.; Mendoza, D.; Pettei, T.; Grayver, E. Eptifibatide and Cirrhosis: Rethinking GPIIb-IIIa Inhibitors for Acute Coronary Syndrome in the Setting of Liver Dysfunction. Cardiol. Res. 2014, 5, 191–194. [Google Scholar] [CrossRef] [Green Version]
- Russo, M.W.; Pierson, J.; Narang, T.; Montegudo, A.; Eskind, L.; Gulati, S. Coronary Artery Stents and Antiplatelet Therapy in Patients With Cirrhosis. J. Clin. Gastroenterol. 2012, 46, 339–344. [Google Scholar] [CrossRef]
- Lu, D.Y.; Saybolt, M.D.; Kiss, D.H.; Matthai, W.H.; Forde, K.A.; Giri, J.; Wilensky, R.L. One-Year Outcomes of Percutaneous Coronary Intervention in Patients with End-Stage Liver Disease. Clin. Med. Insights Cardiol. 2020, 14, 117954682090149. [Google Scholar] [CrossRef]
- Wu, V.C.-C.; Chen, S.-W.; Chou, A.-H.; Ting, P.-C.; Chang, C.-H.; Wu, M.; Hsieh, M.-J.; Wang, C.-Y.; Chang, S.-H.; Lin, M.-S.; et al. Dual antiplatelet therapy in patients with cirrhosis and acute myocardial infarction—A 13-year nationwide cohort study. PLoS ONE 2019, 14, e0223380. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, A.E.; Pollarsky, F.D.; Marino, M.; Cartier, M.; Vázquez, H.; Salgado, P.; Romero, G. Addition of statins to the standard treatment in patients with cirrhosis: Safety and efficacy. World J. Gastroenterol. 2021, 27, 4639–4652. [Google Scholar] [CrossRef]
- VanWagner, L.B. Asprin and statin use for management of atherosclerotic cardiovascular disease in liver transplant candidates: Are we missing the mark?: Vanwagner. Liver Transpl. 2018, 24, 865–867. [Google Scholar] [CrossRef]
- Patel, S.S.; Guzman, L.A.; Lin, F.-P.; Pence, T.; Reichman, T.; John, B.; Celi, F.S.; Liptrap, E.; Bhati, C.; Siddiqui, M.S. Utilization of aspirin and statin in management of coronary artery disease in patients with cirrhosis undergoing liver transplant evaluation. Liver Transpl. 2018, 24, 872–880. [Google Scholar] [CrossRef] [Green Version]
- Amir, O.; Hassan, Y.; Sarriff, A.; Awaisu, A.; Abd. Aziz, N.; Ismail, O. Incidence of risk factors for developing hyperkalemia when using ACE inhibitors in cardiovascular diseases. Pharm. World Sci. 2009, 31, 387–393. [Google Scholar] [CrossRef]
- Sacerdoti, D.; Bolognesi, M.; Merkel, C.; Angeli, P.; Gatta, A. Renal vasoconstriction in cirrhosis evaluated by duplex Doppler ultrasonography. Hepatology 1993, 17, 219–224. [Google Scholar]
- Franz, C.C.; Egger, S.; Born, C.; Rätz Bravo, A.E.; Krähenbühl, S. Potential drug-drug interactions and adverse drug reactions in patients with liver cirrhosis. Eur. J. Clin. Pharmacol. 2012, 68, 179–188. [Google Scholar] [CrossRef] [Green Version]
- Premkumar, M.; Rangegowda, D.; Vyas, T.; Khumuckham, J.S.; Shasthry, S.M.; Thomas, S.S.; Goyal, R.; Kumar, G.; Sarin, S.K. Carvedilol Combined With Ivabradine Improves Left Ventricular Diastolic Dysfunction, Clinical Progression, and Survival in Cirrhosis. J. Clin. Gastroenterol. 2020, 54, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Abougergi, M.S.; Karagozian, R.; Grace, N.D.; Saltzman, J.R.; Qamar, A.A. ST Elevation Myocardial Infarction Mortality Among Patients With Liver Cirrhosis: A Nationwide Analysis Across a Decade. J. Clin. Gastroenterol. 2015, 49, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Patel, N.J.; Rodriguez, A.P.; Shantha, G.; Arora, S.; Deshmukh, A.; Cohen, M.G.; Grines, C.; De Marchena, E.; Badheka, A.; et al. Percutaneous Coronary Intervention in Patients With End-Stage Liver Disease. Am. J. Cardiol. 2016, 117, 1729–1734. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, F.; Balla, S.; AlHajji, M.; Chaudhary, F.; Albeiruti, R.; Kawsara, A.; Alkhouli, M. Temporal trends in the utilization and outcomes of percutaneous coronary interventions in patients with liver cirrhosis. Catheter. Cardiovasc. Interv. 2020, 96, 802–810. [Google Scholar] [CrossRef]
- Marui, A.; Kimura, T.; Tanaka, S.; Miwa, S.; Yamazaki, K.; Minakata, K.; Nakata, T.; Ikeda, T.; Furukawa, Y.; Kita, T.; et al. Coronary Revascularization in Patients With Liver Cirrhosis. Ann. Thorac. Surg. 2011, 91, 1393–1399. [Google Scholar] [CrossRef]
- Lu, D.Y.; Steitieh, D.; Feldman, D.N.; Cheung, J.W.; Wong, S.C.; Halazun, H.; Halazun, K.J.; Amin, N.; Wang, J.; Chae, J.; et al. Impact Of Cirrhosis On 90-Day Outcomes After Percutaneous Coronary Intervention (from A Nationwide Database). Am. J. Cardiol. 2020, 125, 1295–1304. [Google Scholar] [CrossRef]
- Urban, P.; Meredith, I.T.; Abizaid, A.; Pocock, S.J.; Carrié, D.; Naber, C.; Lipiecki, J.; Richardt, G.; Iñiguez, A.; Brunel, P.; et al. Polymer-free Drug-Coated Coronary Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2015, 373, 2038–2047. [Google Scholar] [CrossRef] [Green Version]
- Windecker, S.; Latib, A.; Kedhi, E.; Kirtane, A.J.; Kandzari, D.E.; Mehran, R.; Price, M.J.; Abizaid, A.; Simon, D.I.; Worthley, S.G.; et al. Polymer-based or Polymer-free Stents in Patients at High Bleeding Risk. N. Engl. J. Med. 2020, 382, 1208–1218. [Google Scholar] [CrossRef]
- Murata, M.; Kato, T.S.; Kuwaki, K.; Yamamoto, T.; Dohi, S.; Amano, A. Preoperative hepatic dysfunction could predict postoperative mortality and morbidity in patients undergoing cardiac surgery: Utilization of the MELD scoring system. Int. J. Cardiol. 2016, 203, 682–689. [Google Scholar] [CrossRef]
- Shaheen, A.A.M.; Kaplan, G.G.; Hubbard, J.N.; Myers, R.P. Morbidity and mortality following coronary artery bypass graft surgery in patients with cirrhosis: A population-based study. Liver Int. 2009, 29, 1141–1151. [Google Scholar] [CrossRef]
- Singh, V.; Savani, G.T.; Mendirichaga, R.; Jonnalagadda, A.K.; Cohen, M.G.; Palacios, I.F. Frequency of Complications Including Death from Coronary Artery Bypass Grafting in Patients With Hepatic Cirrhosis. Am. J. Cardiol. 2018, 122, 1853–1861. [Google Scholar] [CrossRef]
- Imam, A.; Karatas, C.; Mecit, N.; Kalayoglu, M.; Kanmaz, T. Cardiac Intervention Before Liver Transplantation. Transplant. Proc. 2021, 53, 1622–1625. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| General Population Risk Factors |
|---|
| Age > 50 years |
| Smoking |
| Dyslipidemia |
| Arterial hypertension |
| Diabetes mellitus |
| Family history of CAD |
| Personal history of CAD |
| Male sex |
| Liver-Cirrhosis-Specific Risk Factors |
| NAFLD etiology |
| Decompensated liver cirrhosis and hypercoagulable state |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gîrleanu, I.; Trifan, A.; Huiban, L.; Muzîca, C.; Petrea, O.C.; Sîngeap, A.M.; Cojocariu, C.; Chiriac, S.; Cuciureanu, T.; Costache, I.I.; et al. Ischemic Heart Disease and Liver Cirrhosis: Adding Insult to Injury. Life 2022, 12, 1036. https://doi.org/10.3390/life12071036
Gîrleanu I, Trifan A, Huiban L, Muzîca C, Petrea OC, Sîngeap AM, Cojocariu C, Chiriac S, Cuciureanu T, Costache II, et al. Ischemic Heart Disease and Liver Cirrhosis: Adding Insult to Injury. Life. 2022; 12(7):1036. https://doi.org/10.3390/life12071036
Chicago/Turabian StyleGîrleanu, Irina, Anca Trifan, Laura Huiban, Cristina Muzîca, Oana Cristina Petrea, Ana Maria Sîngeap, Camelia Cojocariu, Stefan Chiriac, Tudor Cuciureanu, Irina Iuliana Costache, and et al. 2022. "Ischemic Heart Disease and Liver Cirrhosis: Adding Insult to Injury" Life 12, no. 7: 1036. https://doi.org/10.3390/life12071036