
Human Milk Macronutrients and Bioactive Molecules and Development of Regional Fat Depots in Western Australian Infants during the First 12 Months of Lactation

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
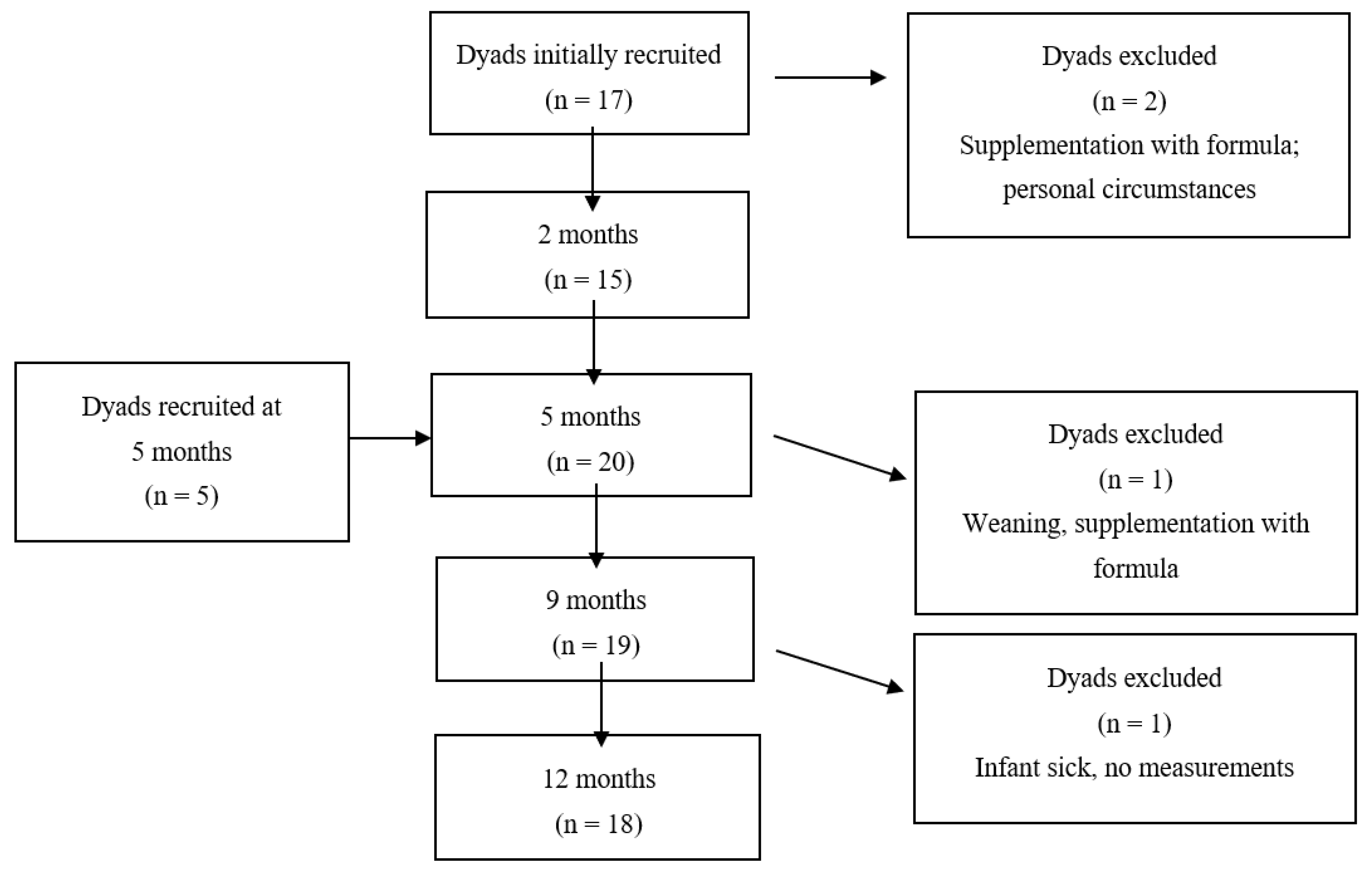
2.1. Participants and Design
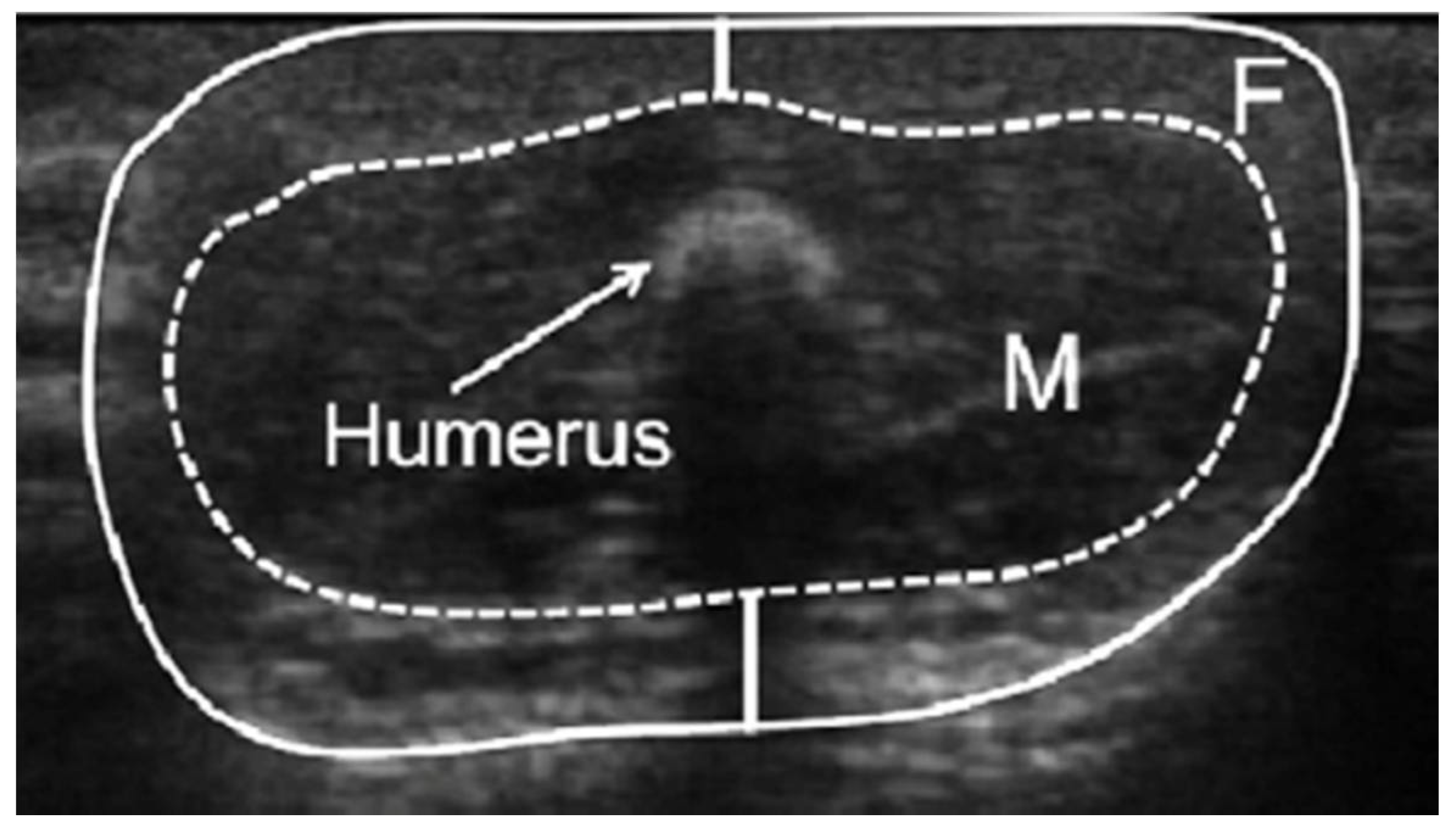
2.2. Measurements of Infant Limb Fat and Lean Areas
2.3. Assessment of Maternal Body Composition
2.4. Analysis of Human Milk Components
2.5. Statistical Analyses
3. Results
3.1. Participants
3.2. Infant Limb Fat and Lean Areas across the First 12 Months of Age
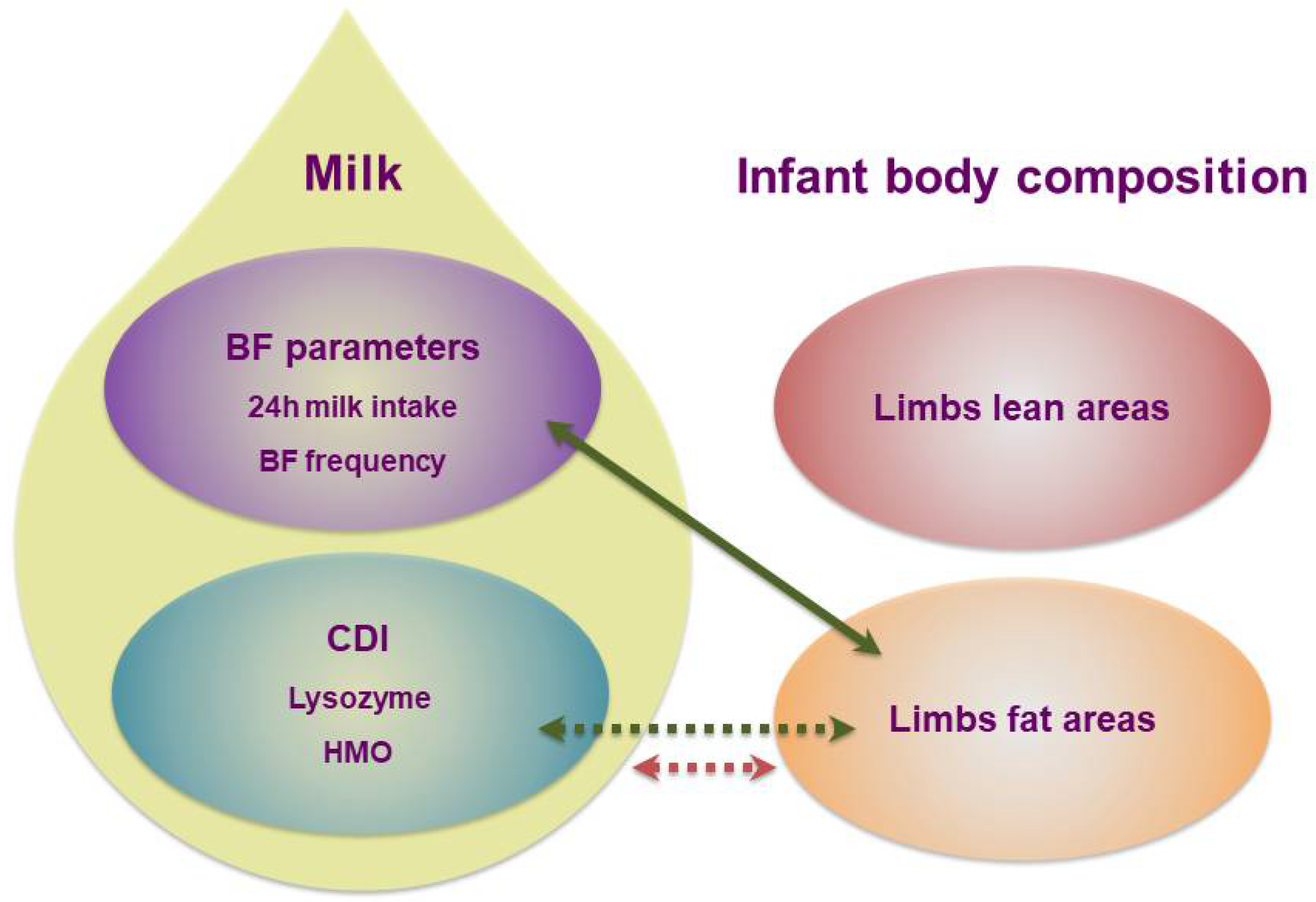
3.3. Human Milk Components and Infant Limb Fat and Lean Areas
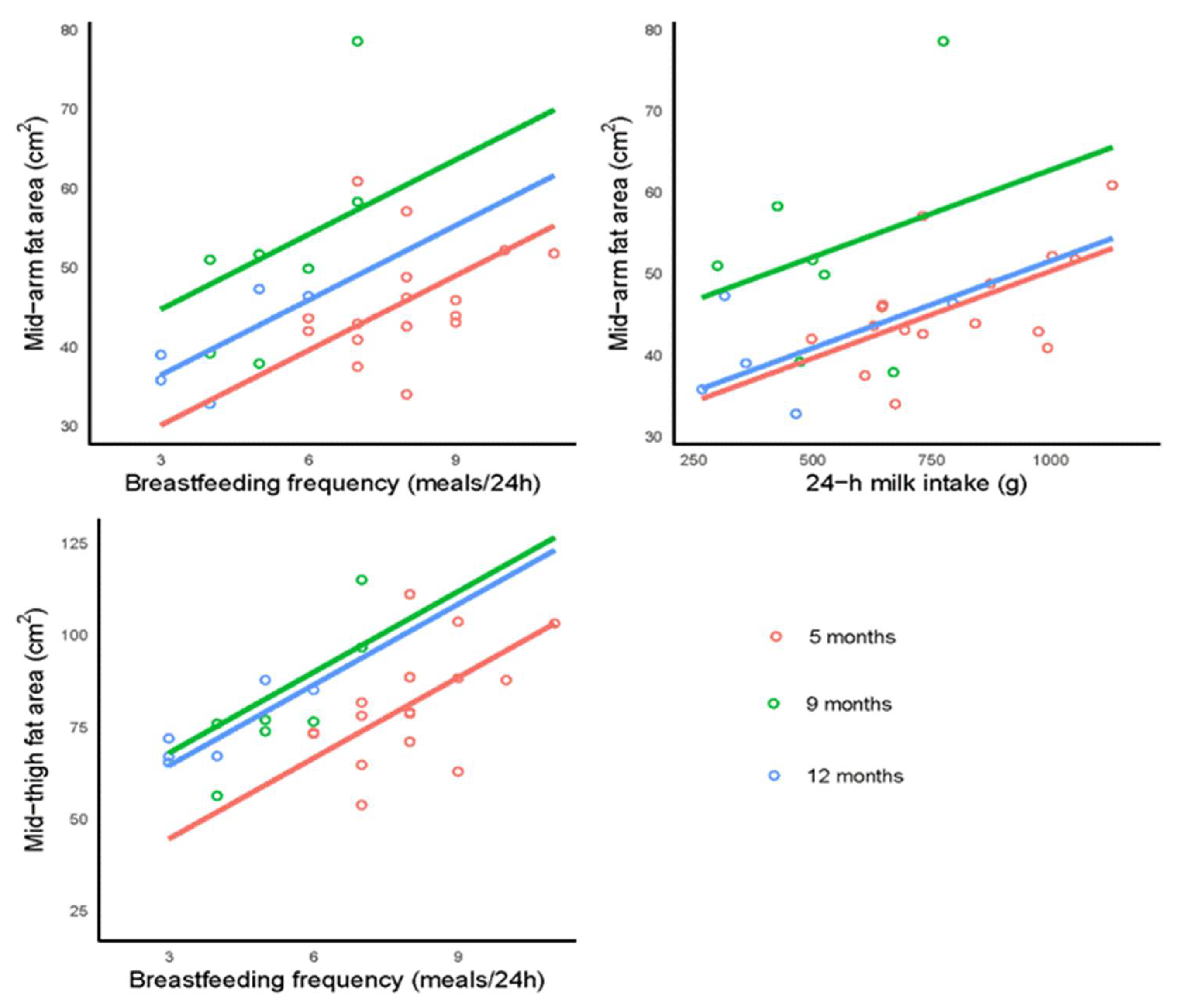
3.4. Breastfeeding Parameters and Infant Limb Fat and Lean Areas
3.5. Maternal Body Composition and Infant Limb Fat and Lean Areas
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Leunissen, R.W.; Kerkhof, G.F.; Stijnen, T.; Hok-ken-Koelega, A. Timing and tempo of first-year rapid growth in relation to cardiovascular and metabolic risk profile in early adulthood. JAMA 2009, 301, 2234–2242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butte, N.; Wong, W.; Hopkinson, J.; Smith, E.; Ellis, K. Infant feeding mode affects early growth and body composition. Pediatrics 2000, 16, 1355–1366. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.G.; Martin, J.M. Does breastfeeding protect against childhood obesity? Moving beyond observational evidence. Curr. Obes. Rep. 2015, 4, 207–216. [Google Scholar] [CrossRef] [PubMed]
- De Lucia Rolfe, E.; Modi, N.; Uthaya, S.; Hughes, I.A.; Dunger, D.B.; Acerini, C.; Stolk, R.P.; Ong, K.K. Ultrasound estimates of visceral and subcutaneous-abdominal adipose tissues in infancy. J. Obes. 2013, 2013, 951954. [Google Scholar] [CrossRef] [PubMed]
- Gridneva, Z.; Rea, A.; Lai, C.T.; Tie, W.J.; Kugananthan, S.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Development of visceral and subcutaneous-abdominal adipose tissue in breastfed infants during first year of lactation. Nutrients 2021, 13, 3294. [Google Scholar] [CrossRef]
- Golan, R.; Shelef, I.; Rudich, A.; Gepner, Y.; Shemesh, E.; Chassidim, Y.; Harman-Boehm, I.; Henkin, Y.; Schwarzfuchs, D.; Ben Avraham, S.; et al. Abdominal superficial subcutaneous fat: A putative distinct protective fat subdepot in type 2 diabetes. Diabetes Care 2012, 35, 640–647. [Google Scholar] [CrossRef] [Green Version]
- Neville, M.C.; Allen, J.C.; Archer, P.C.; Casey, C.E.; Seacat, J.; Keller, R.P.; Lutes, V.; Rasbach, J.; Neifert, M. Studies in human lactation: Milk volume and nutrient composition during weaning and lactogenesis. Am. J. Clin. Nutr. 1991, 54, 81–92. [Google Scholar] [CrossRef]
- Gridneva, Z.; George, A.D.; Suwaydi, M.A.; Sindi, A.S.; Ma, J.; Stinson, L.F.; Geddes, D.T. Environmental determinants of human milk composition in relation to health outcomes. Acta Paediatr. 2022. [Google Scholar] [CrossRef]
- Vanderwall, C.; Clark, R.R.; Eickhoff, J.; Carrel, A.L. BMI is a poor predictor of adiposity in young overweight and obese children. BMC Pediatr. 2017, 17, 135. [Google Scholar] [CrossRef] [Green Version]
- Toro-Ramos, T.; Paley, C.; Pi-Sunyer, F.X.; Gallagher, D. Body composition during fetal development and infancy through the age of 5 years. Eur. J. Clin. Nutr. 2015, 69, 1279–1289. [Google Scholar] [CrossRef] [Green Version]
- Ward, L.; Poston, L.; Godfrey, K.; Koletzko, B. Assessing early growth and adiposity: Report from an Early Nutrition Academy workshop. Ann. Nutr. Metab. 2013, 63, 120–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLeod, G.; Geddes, D.; Nathan, E.; Sherriff, J.; Simmer, K.; Hartmann, P. Feasibility of using ultrasound to measure preterm body composition and to assess macronutrient influences on tissue accretion rates. Early Hum. Dev. 2013, 89, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Arthur, P.; Hartmann, P.; Smith, M. Measurement of the milk intake of breast-fed infants. J. Pediatr. Gastroenterol. Nutr. 1987, 6, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Kent, J.C.; Mitoulas, L.R.; Cregan, M.D.; Ramsay, D.T.; Doherty, D.A.; Hartmann, P.E. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics 2006, 117, e387–e395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larciprete, G.; Valensise, H.; Pierro, G.; Vasapollo, B.; Casalino, B.; Arduini, D.; Jarvis, S.; Cirese, E. Intrauterine growth restriction and fetal body composition. Ultrasound Obstet. Gynecol. 2005, 26, 258–262. [Google Scholar] [CrossRef]
- Gridneva, Z.; Rea, A.; Hepworth, A.R.; Ward, L.C.; Lai, C.T.; Hartmann, P.E.; Geddes, D.T. Relationships between breastfeeding patterns and maternal and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Kugananthan, S.; Gridneva, Z.; Lai, C.T.; Hepworth, A.R.; Mark, P.J.; Kakulas, F.; Geddes, D.T. Associations between maternal body composition and appetite hormones and macronutrients in human milk. Nutrients 2017, 9, 252. [Google Scholar] [CrossRef]
- Van Itallie, T.B.; Yang, M.U.; Heymsfield, S.B.; Funk, R.C.; Boileau, R.A. Height-normalized indices of the body’s fat-free mass and fat mass: Potentially useful indicators of nutritional status. Am. J. Clin. Nutr. 1990, 52, 953–959. [Google Scholar] [CrossRef] [Green Version]
- Kugananthan, S.; Lai, C.T.; Gridneva, Z.; Mark, P.J.; Geddes, D.T.; Kakulas, F. Leptin levels are higher in whole compared to skim human milk, supporting a cellular contribution. Nutrients 2016, 8, 711. [Google Scholar] [CrossRef]
- Gridneva, Z.; Kugananthan, S.; Rea, A.; Lai, C.T.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Human milk adiponectin and leptin and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 1125. [Google Scholar] [CrossRef] [Green Version]
- Gridneva, Z.; Tie, W.J.; Rea, A.; Lai, C.T.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Human milk casein and whey protein and infant body composition over the first 12 months of lactation. Nutrients 2018, 10, 1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gridneva, Z.; Rea, A.; Tie, W.J.; Lai, C.T.; Kugananthan, S.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Carbohydrates in human milk and body composition of term infants during the first 12 months of lactation. Nutrients 2019, 11, 1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gridneva, Z.; Lai, C.T.; Rea, A.; Tie, W.J.; Ward, L.C.; Murray, K.; Hartmann, P.E.; Geddes, D.T. Human milk immunomodulatory proteins are related to development of infant body composition during the first year of lactation. Pediatr. Res. 2020, 89, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Keller, R.; Neville, M. Determination of total protein in human milk: Comparison of methods. Clin. Chem. 1986, 32, 120–123. [Google Scholar] [CrossRef]
- Kunz, C.; Lonnerdal, B. Human milk proteins: Separation of whey proteins and their analysis by polyacrylamide gel electrophoresis, fast protein liquid chromatography (FPLC) gel filtration, and anion-exchange chromatography. Am. J. Clin. Nutr. 1989, 49, 464–470. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Casadio, Y.; Lai, C.; Prime, D.; Hepworth, A.; Trengove, N.; Hartmann, P. Investigation of short-term variations in casein and whey proteins in breast milk of term mothers. Hepatol. Nutr. 2012, 55, 136–141. [Google Scholar] [CrossRef]
- Mitoulas, L.R.; Kent, J.C.; Cox, D.B.; Owens, R.A.; Sherriff, J.L.; Hartmann, P.E. Variation in fat, lactose and protein in human milk over 24 h and throughout the first year of lactation. Br. J. Nutr. 2002, 88, 29–37. [Google Scholar] [CrossRef]
- Euber, J.; Brunner, J. Determination of lactose in milk products by high-performance liquid chromatography. J. Dairy Sci. 1979, 62, 685–690. [Google Scholar] [CrossRef]
- Albalasmeh, A.; Berhe, A.; Ghezzehei, T. A new method for rapid determination of carbohydrate and total carbon concentrations using UV spectrophotometry. Carbohydr. Polym. 2013, 97, 253–261. [Google Scholar] [CrossRef]
- Selsted, M.; Martinez, R. A simple and ultrasensitive enzymatic assay for the quantitative determination of lysozyme in the picogram range. Anal. Biochem. 1980, 109, 67–70. [Google Scholar] [CrossRef]
- Zhang, G.; Lai, C.T.; Hartmann, P.; Oddy, W.H.; Kusel, M.M.H.; Sly, P.D.; Holt, P.G. Anti-infective proteins in breast milk and asthma-associated phenotypes during early childhood. Pediatr. Allergy Immunol. 2014, 25, 544–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tijssen, P. Practice and theory of immunoessays. In Laboratory Techniques in Biochemistry and Molecular Biology; Burdon, R.H., van Knippenberg, P.H., Eds.; Elsevier: Amsterdam, The Netherlands, 1985. [Google Scholar]
- Diggle, P.J.; Heagerty, P.J.; Liang, K.-Y.; Zeger, S.L. Analysis of Longitudinal Data; Oxford University Press Inc.: Oxford, NY, USA, 2002. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curran-Everett, D. Multiple comparisons: Philosophies and illustrations. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, R1–R8. [Google Scholar] [CrossRef] [PubMed]
- Kuzawa, C.W. Adipose tissue in human infancy and childhood: An evolutionary perspective. Am. J. Phys. Anthr. 1998, 107 (Suppl. 27), 177–209. [Google Scholar] [CrossRef]
- Fomon, S.; Haschke, F.; Ziegler, E.; Nelson, S. Body composition of reference children from birth to age 10 years. Am. J. Clin. Nutr. 1982, 35, 1169–1175. [Google Scholar] [CrossRef]
- Cunnane, S.C.; Crawford, M.A. Survival of the fattest: Fat babies were the key to evolution of the large human brain. Comp. Biochem. Physiol. Part A Mol. Integr. Physiol. 2003, 136, 17–26. [Google Scholar] [CrossRef]
- Adam, P.A.J.; Raiha, N.; Rahiala, E.-L.; Kekomaki, M. Oxidation of glucose and d-β-hydroxybuyrate by the early human fetal brain. Acta Paediatr. Scand. 1975, 64, 17–24. [Google Scholar] [CrossRef]
- Carberry, A.; Golditz, P.; Lingwood, B. Body composition from birth to 4.5 months in infants born to non-obese women. Pediatr. Res. 2010, 68, 84–88. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Cano, A.M.; Mier-Cabrera, J.; Allegre-Dávalos, A.L.; Muñoz-Manrique, C.; Perichart-Perera, O. Higher fat mass and fat mass accretion during the first six months of life in exclusively breastfed infants. Pediatr. Res. 2019, 87, 588–594. [Google Scholar] [CrossRef]
- Breij, L.M.; Abrahamse-Berkeveld, M.; Acton, D.; De Lucia Rolfe, E.; Ong, K.K.; Hokken-Koelega, A.C.S. Impact of early infant growth, duration of breastfeeding and maternal factors on total body fat mass and visceral fat at 3 and 6 months of age. Ann. Nutr. Metab. 2017, 71, 203–210. [Google Scholar] [CrossRef]
- Singh, A.S.; Mulder, C.; Twisk, J.W.R.; Van Mechelen, W.; Chinapaw, M.J.M. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Corvalán, C.; Gregory, C.O.; Ramirez-Zea, M.; Martorell, R.; Stein, A.D. Size at birth, infant, early and later childhood growth and adult body composition: A prospective study in a stunted population. Int. J. Epidemiol. 2007, 36, 550–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, A.; Magnuson, A.; Foster, M. Detrimental and protective fat: Body fat distribution and its relation to metabolic disease. Horm. Mol. Biol. Clinl. Investig. 2014, 17, 13–27. [Google Scholar] [CrossRef]
- Snijder, M.B.; Visser, M.; Dekker, J.M.; Goodpaster, B.H.; Harris, T.B.; Kritchevsky, S.B.; De Rekeneire, N.; Kanaya, A.M.; Newman, A.B.; Tylavsky, F.A.; et al. Low subcutaneous thigh fat is a risk factor for unfavourable glucose and lipid levels, independently of high abdominal fat. The Health ABC Study. Diabetologia 2005, 48, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Lee, Y.H.; Lee, B.W.; Kang, E.S.; Lee, I.K.; Cha, B.S. Anatomic fat depots and cardiovascular risk: A focus on the leg fat using nationwide surveys (KNHANES 2008–2011). Cardiovasc. Diabetol. 2017, 16, 54. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Hu, E.A.; Wu, H.; Malik, V.; Sun, Q. Associations of leg fat accumulation with adiposity-related biological factors and risk of metabolic syndrome. Obesity 2013, 21, 824–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snijder, M.B.; Dekker, J.M.; Visser, M.; Bouter, L.M.; Stehouwer, C.D.; Yudkin, J.S.; Heine, R.J.; Nijpels, G.; Seidell, J.C.; Hoorn Study. Trunk fat and leg fat have independent and opposite associations with fasting and postload glucose levels: The Hoorn study. Diabetes Care 2004, 27, 372–377. [Google Scholar] [CrossRef] [Green Version]
- Larsson, M.; Lind, M.V.; Lharnkjær, A.; Due, A.P.; Blom, I.C.; Wells, J.; Lai, C.T.; Mølgaard, C.; Geddes, D.T.; Michaelsen, K.F. Excessive weight gain followed by catch-down in exclusively breastfed infants: An exploratory study. Nutrients 2018, 10, 1290. [Google Scholar] [CrossRef] [Green Version]
- Perrella, S.L.; Geddes, D.T. A case report of a breastfed infant’s excessive weight gains over 14 months. J. Hum. Lact. 2016, 32, 364–368. [Google Scholar] [CrossRef]
- Artym, J.; Zimecki, M. Milk-derived proteins and peptides in clinical trials. Postepy. Hig. Med. Dosw. 2013, 67, 800–816. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Lo, L.; Forsberg, L.; Maier, R. Helicobacter pylori peptidoglycan modifications confer lysozyme resistance and contribute to survival in the host. mBio 2012, 3, e00409–e00412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montagne, P.; Cuilliere, M.L.; Mole, C.; Bene, M.C.; Faure, G. Changes in lactoferrin and lysozyme levels in human milk during the first twelve weeks of lactation. Adv. Exp. Med. Biol. 2001, 501, 241–247. [Google Scholar] [PubMed]
- Bode, L. The functional biology of human milk oligosaccharides. Early Hum. Dev. 2015, 91, 619–622. [Google Scholar] [CrossRef] [PubMed]
- Alderete, T.A.; Autran, C.; Brekke, B.E.; Knight, R.; Bode, L.; Goran, M.; Fields, D. Associations between human milk oligosaccharides and infant body composition in the first 6 mo of life. Am. J. Clin. Nutr. 2015, 102, 1381–1388. [Google Scholar] [CrossRef]
- Koleva, P.T.; Bridgman, S.L.; Kozyrskyj, A.L. The infant gut microbiome: Evidence for obesity risk and dietary intervention. Nutrients 2015, 7, 2237–2260. [Google Scholar] [CrossRef] [Green Version]
- Bode, L. Human milk oligosaccharides: Every baby needs a sugar mama. Glycobiology 2012, 22, 1147–1162. [Google Scholar] [CrossRef] [Green Version]
- Braun, O.H.; Sandkuhler, H. Relationships between lysozyme concentration of human milk, bacteriologic content, and weight gain of premature infants. J. Pediatr. Gastroenterol. Nutr. 1985, 4, 583–586. [Google Scholar] [CrossRef]
- Bol’shakova, A.M.; Shcherbakova, E.G.; Ivanova, S.D.; Medvedeva, M.M.; Zhuravleva, T.P. Lysozyme in the feeding of premature infants with mixed pathology. Antibiotiki 1984, 29, 784–790. [Google Scholar]
- Saben, J.; Sims, C.; Abraham, A.; Bode, L.; Andres, A. Human milk oligosaccharide concentrations and infant intakes are associated with maternal overweight and obesity and predict infant growth. Nutrients 2021, 13, 446. [Google Scholar] [CrossRef]
- Woo, J.; Guerrero, M.; Altaye, M.; Ruiz-Palacios, G.; Martin, L.; Dubert-Ferrandon, A.; Newburg, D.; Morrow, A. Human milk adiponectin is associated with growth in two independent cohorts. Breastfeed Med. 2009, 4, 101–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.Y.; Zhang, Z.J.; Yao, W.; Morrow, A.; Peng, Y.M. Variation of maternal milk adiponectin and its correlation with infant growth. Zhonghua Er Ke Za Zhi 2011, 49, 338–343. [Google Scholar] [PubMed]
- de Fluiter, K.; Kerkhof, G.F.; van Beijsterveldt, I.; Breij, L.M.; de Heijning, B.; Abrahamse-Berkeveld, M.; Hokken-Koelega, A. Longitudinal human milk macronutrients, body composition and infant appetite during early life. Clin. Nutr. 2021, 40, 3401–3408. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Heinig, M.J.; Nommsen, L.A.; Lonnerdal, B. Maternal versus infant factors related to breast milk intake and residual milk volume: The DARLING study. Pediatrics 1991, 87, 829–837. [Google Scholar] [CrossRef]
- Gridneva, Z.; Kugananthan, S.; Hepworth, A.R.; Tie, W.J.; Lai, C.T.; Ward, L.C.; Hartmann, P.E.; Geddes, D.T. Effect of human milk appetite hormones, macronutrients, and infant characteristics on gastric emptying and breastfeeding patterns of term fully breastfed infants. Nutrients 2017, 9, 15. [Google Scholar] [CrossRef]
- Galpin, L.; Thakwalakwa, C.; Phuka, J.; Ashorn, P.; Maleta, K.; Wong, W.W.; Manary, M.J. Breast milk intake is not reduced more by the introduction of energy dense complementary food than by typical infant porridge. J. Nutr. 2007, 137, 1828–1833. [Google Scholar] [CrossRef] [Green Version]
- Cheema, A.S.; Stinson, L.F.; Rea, A.; Lai, C.T.; Payne, M.S.; Murray, K.; Geddes, D.T.; Gridneva, Z. Human milk lactose, insulin, and glucose relative to infant body composition during exclusive breastfeeding. Nutrients 2021, 13, 3724. [Google Scholar] [CrossRef]
- Tahir, M.J.; Haapala, J.L.; Foster, L.P.; Duncan, K.M.; Teague, A.M.; Kharbanda, E.O.; McGovern, P.M.; Whitaker, K.M.; Rasmussen, K.M.; Fields, D.A.; et al. Higher maternal diet quality during pregnancy and lactation is associated with lower infant weight-for-length, body fat percent, and fat mass in early postnatal life. Nutrients 2019, 11, 632. [Google Scholar] [CrossRef] [Green Version]
- Leghi, G.E.; Netting, M.J.; Middleton, P.F.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. The impact of maternal obesity on human milk macronutrient composition: A systematic review. Nutrients 2020, 12, 934. [Google Scholar] [CrossRef] [Green Version]
- Leghi, G.E.; Netting, M.J.; Lai, C.T.; Narayanan, A.; Dymock, M.; Rea, A.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, B.S. Reduction in maternal energy intake during lactation decreased maternal body weight and concentrations of leptin, insulin and adiponectin in human milk without affecting milk production, milk macronutrient composition or infant growth. Nutrients 2021, 13, 1892. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | 2 Months | 5 Months | 9 Months | 12 Months |
|---|---|---|---|---|
| Mean ± SD (Min–Max) | Mean ± SD (Min–Max) | Mean ± SD (Min–Max) | Mean ± SD (Min–Max) | |
| Mothers | (n = 14) | (n = 20) | (n = 18) | (n = 18) |
| Weight (kg) | 78.8 ± 19.3 a | 70.1 ± 17.8 | 63.0 ± 10.0 | 64.2 ± 17.3 |
| (57.5–116.2) | (53.7–115.3) | (50.4–121.9) | (51.4–121.9) | |
| BMI (kg/m2) | 27.2 ± 5.5 | 24.8 ± 5.0 | 22.7 ± 3.9 | 23.9 ± 5.9 |
| (20.4–35.5) | (19.0–35.2) | (17.9–37.2) | (18.2–37.2) | |
| Infants | (n = 15) | (n = 20) | (n = 19) | (n = 18) |
| Sex (M/F) | 9 M/6 F | 10 M/10 F | 10 M/9 F | 9 M/9 F |
| Age (months) | 2.04 ± 0.14 | 5.16 ± 0.22 | 9.22 ± 0.27 | 12.26 ± 0.28 |
| (1.87–2.33) | (4.77–5.47) | (8.83–9.77) | (11.63–12.67) | |
| Length (cm) | 58.1 ± 1.9 | 64.8 ± 2.3 | 71.7 ± 1.9 | 73.6 ± 3.2 |
| (54.2–60.0) | (60.5–69.5) | (66.0–74.0) | (69.0–78.5) | |
| Weight (kg) | 5.63 ± 0.66 | 7.43 ± 1.13 | 8.84 ± 0.98 | 9.65 ± 0.62 |
| (4.42–7.40) | (5.81–9.51) | (6.68–10.10) | (7.17–11.09) | |
| BMI (kg/m2) | 16.6 ± 1.2 | 17.6 ± 1.9 | 17.7 ± 1.7 | 17.8 ± 0.9 |
| (14.5–18.1) | (14.9–20.4) | (14.2–20.2) | (13.7–19.2) | |
| Infant limbs measurements | (n = 13) | (n = 19) | (n = 18) | (n = 12) |
| Mid-arm lean area (cm2) | 106.6 ± 11.8 | 116.6 ± 10.4 | 125.2 ± 12.7 | 127.3 ± 6.9 |
| (82.4–120.8) | (98.1–134.3) | (106.4–156.4) | (118.5–142.5) | |
| Mid-arm fat area (cm2) | 41.6 ± 6.6 | 47.2 ± 7.5 | 49.6 ± 9.3 | 40.5 ± 6.7 |
| (31.4–53.0) | (34.0–62.3) | (37.9–78.6) | (31.4–50.0) | |
| Mid-thigh lean area (cm2) | 148.3 ± 21.6 | 179.2 ± 22.5 | 197.0 ± 24.9 | 195.3 ± 29.0 |
| (110.5–184.6) | (138.2–214.2) | (170.8–270.8) | (117.9–237.7) | |
| Mid-thigh fat area (cm2) | 61.8 ± 12.5 | 81.0 ± 16.5 | 76.9 ± 24.4 | 71.2 ± 15.5 |
| (41.3–85.5) | (52.4–112.2) | (22.0–121.2) | (41.3–91.6) | |
| Breastfeeding parameters | ||||
| 24-h MI (g) | (n = 17) b | (n = 8) | (n = 8) | |
| 819 ± 205 | 478 ± 154 | 451 ± 216 | ||
| (498–1185) | (300–775) | (255–795) | ||
| BFF (meals/24 h) | (n = 17) b | (n = 8) | (n = 9) | |
| 8.1 ± 1.4 | 5.4 ± 1.3 | 4.4 ± 2.1 | ||
| (6–11) | (4–7) | (2–8) | ||
| Months after Birth | |||||||
|---|---|---|---|---|---|---|---|
| Infant Characteristic | Between 5 and 2 Months | Between 9 and 2 Months | Between 12 and 2 Months | Between 9 and 5 Months | Between 12 and 5 Months | Between 12 and 9 | Overall p-Value |
| (n = 13) | (n = 13) | (n = 12) | (n = 18) | (n = 12) | (n = 12) | (n = 18) | |
| Mid-arm lean area (cm2) | 10.93 ± 3.17 b (0.003) c | 19.19 ± 3.22 (<0.001) | 22.73 ± 3.75 (<0.001) | 8.26 ± 2.86 (0.020) | 11.80 ± 3.40 (0.003) | 3.54 ± 3.42 (0.73) | <0.001 |
| Mid-arm fat area (cm2) | 5.76 ± 2.45 (0.087) | 8.00 ± 2.49 (0.007) | −2.09 ± 2.88 (0.89) | 2.24 ± 2.22 (0.74) | −7.84 ± 2.62 (0.015) | −10.08 ± 2.64 (<0.001) | <0.001 |
| Mid-thigh lean area (cm2) | 30.34 ± 8.04 (0.001) | 48.06 ± 8.15 (<0.001) | 46.95 ± 8.93 (<0.001) | 17.72 ± 7.29 (0.071) | 16.61 ± 8.08 (0.17) | −1.12 ± 8.15 (1.00) | <0.001 |
| Mid-thigh fat area (cm2) | 16.96 ± 5.88 (0.020) | 12.71 ± 5.97 (0.14) | 6.48 ± 6.57 (0.76) | −4.25 ± 5.33 (0.86) | −10.48 ± 5.92 (0.29) | −6.23 ± 5.97 (0.72) | 0.035 |
| Predictor | 2 Months | 5 Months | 9 Months | 12 Months | p-Values | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | |
| Daily intakes of milk components | |||||||||||
| (n = 13) | (n = 17) | (n = 7) | (n = 5) | (n = 17) | |||||||
| Mid-arm lean area (cm2), significant at <0.005 d | |||||||||||
| Leptin (ng/day) | 105 (10.3) | 0.01 (0.02) a | 133 (6.82) | −0.05 (0.02) | 106 (14.3) | 0.08 (0.05) | 128 (9.58) | −0.004 (0.04) | 0.32 | 0.019 | 0.046 b |
| Mid-arm fat area (cm2), significant at <0.009 | |||||||||||
| Lysozyme (g/day) | 38.2 (2.79) | 40 (23.2) | 31.2 (9.09) | 189 (125) | 21.9 (9.95) | 484 (151) | 48.4 (5.99) | −98.1 (58.4) | 0.064 | <0.001 | 0.001 |
| HMO (g/day) | 42.8 (4.05) | −0.13 (0.25) | 39.3 (4.16) | 0.54 (0.30) | 18.1 (10.7) | 2.79 (0.84) | 39.1 (4.58) | 0.12 (0.18) | 0.28 | 0.002 | 0.004 |
| Mid-thigh lean area (cm2), significant at <0.005 | |||||||||||
| Leptin (ng/day) | 179 (13.7) | −0.06 (0.03) | 202 (10.5) | −0.06 (0.03) | 215 (10.1) | −0.06 (0.03) | 215 (9.63) | −0.06 (0.03) | 0.025 c | 0.001 | 0.16 |
| Concentrations of milk components | |||||||||||
| (n = 13) | (n = 19) | (n = 18) | (n = 9) | (n = 19) | |||||||
| Mid-arm lean area (cm2), significant at <0.005 | |||||||||||
| Lactoferrin (g/L) | 119 (6.27) | −26.4 (10.9) | 122 (6.9) | −12.1 (15.5) | 115 (6.21) | 15.7 (9.51) | 119 (12.1) | 13.8 (17.1) | 0.73 | <0.001 | 0.029 |
| Lactose (g/L) | 185 (32) | −1.18 (0.47) | 88.9 (33.9) | 0.42 (0.52) | 85.7 (30.1) | 0.60 (0.46) | 151 (42.1) | −0.33 (0.63) | 0.73 | <0.001 | 0.040 |
| sIgA (g/L) | 126 (7.93) | −36.4 (13.5) | 105 (6.82) | 22.6 (12.5) | 118 (7.3) | 11 (11.2) | 120 (11.8) | 11.2 (16.3) | 0.89 | <0.001 | 0.007 |
| Mid-arm fat area (cm2), significant at <0.005 | |||||||||||
| sIgA (g/L) | 34.7 (5.99) | 12.9 (10.2) | 46.6 (5.14) | 1.91 (9.47) | 63.8 (5.49) | −22.7 (8.46) | 43.4 (8.87) | −7.11 (12.3) | 0.38 | <0.001 | 0.041 |
| Mid-thigh lean area (cm2), significant at <0.005 | |||||||||||
| Whey protein (g/L) | 206 (28.1) | −8.78 (4.14) | 254 (32.1) | −13.6 (5.78) | 164 (20.8) | 5.41 (3.3) | 230 (27.7) | −4.35 (3.86) | 0.15 | <0.001 | 0.008 |
| Lactoferrin (g/L) | 167 (13.7) | −36.2 (24.1) | 211 (14.9) | −75.5 (33.7) | 180 (13.4) | 28 (20.7) | 207 (21.2) | −10.8 (31.7) | 0.35 | <0.001 | 0.040 |
| Mid-thigh fat area (cm2), significant at <0.005 | |||||||||||
| Adiponectin (ng/mL) | 78.8 (10.8) | −1.31 (0.92) | 99.4 (10.7) | −1.84 (1.04) | 143 (20.6) | −7.72 (2.31) | 71.9 (15.4) | −0.144 (1.34) | 0.039 | 0.023 | 0.028 |
| Total protein (g/L) | 159 (34.3) | −8.65 (3.14) | 975 (14.5) | 0.58 (1.2) | 111 (24.1) | −3.14 (2.28) | 72.5 (21.6) | −0.352 (1.79) | 0.32 | 0.009 | 0.030 |
| Casein (g/L) | 54.6 (23.2) | 9.61 (18.5) | 84.4 (10.5) | −1.45 (5.71) | 116 (13.8) | −32.2 (10.9) | 88.3 (19.2) | −13.7 (13) | 0.19 | 0.004 | 0.039 |
| Predictor | 2–5 Months | 9 Months | 12 Months | p-Values | |||||
|---|---|---|---|---|---|---|---|---|---|
| Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Intercept (SE) | Slope (SE) | Predictor | Infant Age (Months) | Interaction | |
| (n = 14) | (n = 7) | (n = 5) | (n = 14) | ||||||
| Mid-arm fat area (cm2), significant at <0.05 c | |||||||||
| BFF (meals/24 h) d | 20.7 (9.88) a | 3.15 (1.21) | 35.3 (7.23) | 3.15 (1.21) | 27 (6.22) | 3.15 (1.21) | 0.008 b | 0.002 | 0.065 |
| 24 h MI (g) d | 28.9 (7.65) | 0.021 (0.009) | 41.4 (5.64) | 0.021 (0.009) | 30.2 (5.33) | 0.021 (0.009) | 0.024 | 0.002 | 0.37 |
| Mid-thigh fat area (cm2), significant at <0.05 | |||||||||
| BFF (meals/24 h) | 22.6 (14.7) | 7.33 (1.78) | 46 (10.4) | 7.33 (1.78) | 42.5 (8.6) | 7.33 (1.78) | <0.001 | 0.002 | 0.29 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gridneva, Z.; Rea, A.; Lai, C.T.; Tie, W.J.; Kugananthan, S.; Warden, A.H.; Perrella, S.L.; Murray, K.; Geddes, D.T. Human Milk Macronutrients and Bioactive Molecules and Development of Regional Fat Depots in Western Australian Infants during the First 12 Months of Lactation. Life 2022, 12, 493. https://doi.org/10.3390/life12040493
Gridneva Z, Rea A, Lai CT, Tie WJ, Kugananthan S, Warden AH, Perrella SL, Murray K, Geddes DT. Human Milk Macronutrients and Bioactive Molecules and Development of Regional Fat Depots in Western Australian Infants during the First 12 Months of Lactation. Life. 2022; 12(4):493. https://doi.org/10.3390/life12040493
Chicago/Turabian StyleGridneva, Zoya, Alethea Rea, Ching Tat Lai, Wan Jun Tie, Sambavi Kugananthan, Ashleigh H. Warden, Sharon L. Perrella, Kevin Murray, and Donna T. Geddes. 2022. "Human Milk Macronutrients and Bioactive Molecules and Development of Regional Fat Depots in Western Australian Infants during the First 12 Months of Lactation" Life 12, no. 4: 493. https://doi.org/10.3390/life12040493