
Abdominopelvic Actinomycosis—The Diagnostic and Therapeutic Challenge of the Most Misdiagnosed Disease

 ,
,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caplan, E.; Deputy, M.; Arul, D.; Wilson, J. Actinomycosis of the omentum with invasion of the abdominal wall, small bowel and transverse colon mimicking malignancy. BMJ Case Rep. 2019, 12, Bcr-2018-227728. [Google Scholar] [CrossRef]
- Yang, S.S.; Im, Y.C. Severe abdominopelvic actinomycosis with colon perforation and hepatic involvement mimicking advanced sigmoid colon cancer with hepatic metastasis: A case study. BMC Surg. 2018, 18, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andronic, D.; Lupascu, C.; Târcoveanu, E.; Georgescu, S.; Neacsu, C.; Ferariu, D.; Crumpei, F. Present trends in abdominal actinomycosis. Chirurgia 2009, 104, 439–446. [Google Scholar] [PubMed]
- Dayan, K.; Neufeld, D.; Zissin, R.; Bernheim, J.; Paran, H.; Schwartz, I.; Freund, U. Actinomycosis of the large bowel: Unusual presentations and their surgical treatment. Eur. J. Surg. 1996, 162, 657. [Google Scholar] [PubMed]
- Cintron, J.R.; Del Pino, A.; Duarte, B.; Wood, D. Abdominal actinomycosis. Dis. Colon Rectum 1996, 39, 105. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.K.; Turmezei, T.D.; Weston, V.C. Actinomycosis. BMJ 2011, 343, d6099. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Quarta, C.; Alovisi, M.; Crincoli, V.; Aiuto, R.; Crippa, R.; Angiero, F.; Laneve, E.; Sovereto, D.; De Lillo, A.; et al. Microbial Association with Genus Actinomyces in Primary and Secondary Endodontic Lesions, Review. Antibiotics 2020, 9, 433. [Google Scholar] [CrossRef]
- Sung, H.Y.; Lee, I.S.; Kim, S.I.; Jung, S.E.; Kim, S.W.; Kim, S.Y.; Chung, M.K.; Kim, W.C.; Oh, S.T.; Kang, W.K. Clinical features of abdominal actinomycosis: A 15-year experience of a single institute. J. Korean Med. Sci. 2011, 26, 932–937. [Google Scholar] [CrossRef]
- Lin, C.D.; Tai, H.C.; Wang, C.C.; Yu, C.T.; Chang, S.J.; Hsieh, C.H.; Shei-Dei Yang, S. Renal actinomycosis: An unusual cause of renal abscess. Urol. Sci. 2012, 23, 129–132. [Google Scholar] [CrossRef] [Green Version]
- Heo, S.H.; Shin, S.S.; Kim, J.W.; Lim, H.S.; Seon, H.J.; Jung, S.I.; Jeong, Y.Y.; Kang, H.K. Imaging of actinomycosis in various organs: A comprehensive review. Radiographics 2014, 34, 19–33. [Google Scholar] [CrossRef]
- Näf, F.; Enzler-Tschudy, A.; Kuster, S.P.; Uhlig, I.; Steffen, T. Abdominal actinomycosis mimicking a malignant neoplasm. Surg. Infect. 2014, 15, 462–463. [Google Scholar] [CrossRef] [Green Version]
- Filippou, D.; Psimitis, I.; Zizi, D.; Rizos, S. A rare case of ascending colon actinomycosis mimicking cancer. BMC Gastroenterol. 2005, 5, 1. [Google Scholar] [CrossRef] [Green Version]
- Ergül, Z.; Hoca, O.; Karahan, M.A.; Seker, D.; Hücümenoglu, S.; Ozakkoyunlu, S. A transverse colonic mass secondary to Actinomyces infection mimicking cancer. Turk. J. Gastroenterol. 2008, 19, 200–201. [Google Scholar]
- Privitera, A.; Milkhu, C.S.; Datta, V.; Rodriguez-Justo, M.; Windsor, A.; Cohen, C.R. Actinomycosis of the sigmoid colon: A case report. World J. Gastrointest. Surg. 2009, 1, 62–64. [Google Scholar] [CrossRef]
- Acquaro, P.; Tagliabue, F.; Confalonieri, G.; Faccioli, P.; Costa, M. Abdominal wall actinomycosis simulating a malignant neoplasm: Case report and review of the literature. World J. Gastrointest. Surg. 2010, 2, 247–250. [Google Scholar] [CrossRef]
- Petrie, B.A.; Schwartz, S.I.; Saltmarsh, G.F. Intra-abdominal actinomycosis in association with sigmoid diverticulitis. Am. Surg. 2014, 80, E157–E159. [Google Scholar] [CrossRef]
- Hsieh, Y.C.; Chang, Y.Y.; Lee, K.C. Colonic actinomycosis mimicking a fish bone-related granuloma. Clin. Gastroenterol. Hepatol. 2012, 10, e81–e82. [Google Scholar] [CrossRef]
- Vanoeteren, X.; Devreese, K.; De Munter, P. Abdominal actinomycosis: A rare complication after cholecystectomy. Acta Clin. Belg. 2014, 69, 152–156. [Google Scholar] [CrossRef]
- Valbø, A.; Rønning, E.J.; Aaberg, M. Actinomycosis as a complication of intrauterine device use. Tidsskr. Nor. Laegeforen. 2010, 130, 830–832. [Google Scholar] [CrossRef]
- Benhoff, D.F. Actinomycosis: Diagnostic & therapeutic considerations and a review of 32 cases. Can. J. Surg. 2008, 51, 155–158. [Google Scholar]
- Ha, Y.J.; An, J.H.; Shim, J.H.; Yu, E.S.; Kim, J.J.; Ha, T.Y.; Lee, H.C. A case of primary hepatic actinomycosis: An enigmatic inflammatory lesion of the liver. Clin. Mol. Hepatol. 2015, 21, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Willms, A.; Schaaf, S.; Güsgen, C.; Waldeck, S.; Schwab, R. Abdomina actinomycosis: A rare differential diagnosis to colon carcinoma and Morbus Crohn. Z. Gastroenterol. 2014, 52, 569–572. [Google Scholar] [PubMed]
- Pitot, D.; De Moor, V.; Demetter, P.; Place, S.; Gelin, M.; El Nakadi, I. Actinomycotic abscess of the anterior abdominal wall: A case report and literature review. Acta Chir Belg. 2008, 108, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Könönen, E.; Wade, W.G. Actinomyces and related organisms in human infections. Clin. Microbiol. Rev. 2015, 28, 419–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldwag, S.; Abbit, P.L.; Watts, B. Case reports: Percutaneous drainage of periappendiceal actinomycosis. Clin. Radiol. 1991, 44, 422–424. [Google Scholar] [CrossRef]
- Smego, R.A., Jr. Actinomycosis. In Infectious Diseases; Hoeprich, P.D., Jordan, M.C., Ronald, A.R., Eds.; Lippincott: New York, NY, USA, 1994; p. 493. [Google Scholar]
- Skoutelis, A.; Petrochilos, J.; Bassaris, H. Successful treatment of thoracic actinomycosis with ceftriaxone. Clin. Infect. Dis. 1994, 19, 161. [Google Scholar] [CrossRef] [PubMed]
- Zamani, F.; Sohrabi, M. Clinical, Endoscopic, and Histopathological Aspects of Sigmoid Actinomycosis; A Case Report and Literature Review. Middle East J. Dig. Dis. 2015, 7, 41–44. [Google Scholar]
- Akbulut, S.; Yagmur, Y.; Gumus, S.; Sogutcu, N.; Demircan, F. Actinomyces-induced inflammatory myofibroblastic tumor of the colon: A rare cause of an abdominal mass. Int. J. Surg. Case Rep. 2015, 9, 15–18. [Google Scholar] [CrossRef] [Green Version]
- Valdés-Peregrina, E.N.; Bonifaz, A.; Arteaga-Sarmiento, J.F.; Hernández- González, M. Primary intestinal actinomycosis in ilium and colon. A case report and review of the literature. Rev. Esp. Patol. 2018, 51, 253–256. [Google Scholar]
- Valour, F.; Sénéchal, A.; Dupieux, C.; Karsenty, J.; Lustig, S.; Breton, P.; Gleizal, A.; Boussel, L.; Laurent, F.; Braun, E.; et al. Actinomycosis: Etiology, clinical features, diagnosis, treatment, and management. Infect. Drug Resist. 2014, 7, 183–197. [Google Scholar]
- Smith, A.J.; Hall, V.; Thakker, B.; Gemmell, C.G. Antimicrobial susceptibility testing of Actinomyces species with 12 antimicrobial agents. J. Antimicrob. Chemother. 2005, 56, 407–409. [Google Scholar] [CrossRef] [Green Version]
- Yegüez, J.F.; Martinez, S.A.; Sands, L.R.; Hellinger, M.D. Pelvic actinomycosis presenting as malignant large bowel obstruction: A case report and a review of the literature. Am. Surg. 2000, 66, 85–90. [Google Scholar]
- Cirafici, L.; Worreth, M.; Froehlich, F. L’actinomycose abdominopelvienne. Présentation d’un cas et revue de la littérature [Pelvic and abdominal actinomycosis. Case report and review of the literature]. Rev. Med. Suisse Romande 2002, 122, 535–537. (In French) [Google Scholar]
- Chelli, D.; Hassini, A.; Aloui, F.; Sfar, E.; Zouaoui, B.; Chelli, H.; Chanoufi, B. Actinomycose pelvienne Expérience tunisienne: À propos de 5 cas [Pelvic actinomycosis in Tunisia: Five cases]. Sante 2008, 18, 77–82. [Google Scholar]
- Lim, K.T.; Moon, S.J.; Kwon, J.S.; Son, Y.W.; Choi, H.Y.; Choi, Y.Y.; Pyo, J.Y.; Park, Y.W.; Moon, H.S. Urachal Actinomycosis Mimicking a Urachal Tumor. Korean J. Urol. 2010, 51, 438–440. [Google Scholar] [CrossRef]
- Marret, H.; Wagner, N.; Ouldamer, L.; Jacquet, A.; Body, G. Actinomycose pelvienne: Est-ce prévisible? [Pelvic actinomycosis: Just think of it]. Gynecol. Obstet. Fertil. 2010, 38, 307–312. [Google Scholar] [CrossRef]
- Jabi, R.; Ramdani, H.; Elmir, S.; Elmejjati, F.; Serji, B.; El Harroudi, T.; Bouziane, M. Pseudotumoral Actinomycosis Mimicking Malignant Colic Disease: A Case Report and Literature Review. Visc. Med. 2020, 36, 333–337. [Google Scholar] [CrossRef]
- Asiri, B.I.; Alshehri, A.A.; Alqahtani, A.S.; Albishi, A.M.; Assiri, Y.I.; Asmiri, E.A. Caecum actinomycosis with acute abdomen: A case report. J. Taibah Univ. Med. Sci. 2020, 15, 148–152. [Google Scholar] [CrossRef]
- Kim, S.; Kang, S.I.; Kim, S.; Jang, M.H.; Kim, J.H. Abdominopelvic Actinomycosis Mimicking Peritoneal Carcinomatosis: A Case Report. Ann. Coloproctol. 2020, 36, 417–420. [Google Scholar] [CrossRef] [Green Version]
- Pamathy, G.; Jayarajah, U.; Gamlaksha, D.S.; Constantine, R.; Banagala, A.S. Abdominal actinomycosis mimicking a transverse colon malignancy: A case report and review of the literature. J. Med. Case Rep. 2021, 15, 224. [Google Scholar] [CrossRef]
- Clarrett, D.; Ray, J.M.; Taylor, J.R. Abdominal Actinomycosis Abscess Presenting as an Isolated Gastrointestinal Pseudotumor. ACG Case Rep. J. 2021, 8, e00672. [Google Scholar] [CrossRef]
- Tarzi, M.; Douedari, A.; Aldakhil, R.; Danial, A.K.; Al-Haj, A. Case report: Actinomycosis of the abdominal wall. J. Surg. Case Rep. 2021, 2021, rjab171. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 43.36 ± 19.14 years (18–64 years) |
| Gender | 9 male/19 female patients |
| Predisposing factors | N (cases) (%) |
| Long-term IUDs | 13/28 (46.4%) |
| Diabetes | 5/28 (17.8%) |
| Foreign bodies | |
| Toothpick | 1/28 (3.5%) |
| Gallstones lost in the peritoneum | 1/28 (3.5%) |
| Stenting of the bile duct | 1/28 (3.5%) |
| Immunosuppression | 3/28 (10.7%) |
| Diverticulitis | 3/28 (10.7%) |
| Oral diseases associated | 5/28 (17.8%) |
| Gastroesophageal reflux associated | 9/28 (32.1%) |
| No predisposing factors | 1/28 (3.5%) |
| Clinical features | N (cases) (%) |
| Distended abdomen with tenderness | 11/28 (39.2%) |
| Tumor palpable | 4/28 (14.2%) |
| Deep organ adhesion | 12/28 (42,3%) |
| Abdominal pain | 18/28 (76,9%) |
| Fever | 17/28 (61,5%) |
| Weight loss | 14/28 (50%) |
| Anemia | 13/28 (46.4%) |
| Leukocytosis | 23/28 (82.14%) |
| The mean duration of symptoms | |
| Chronic or subacute symptoms | 2.8 ± 2.4 month (1–14 months) |
| Emergency | 11.7 ± 9.2 days (7–21 days) |
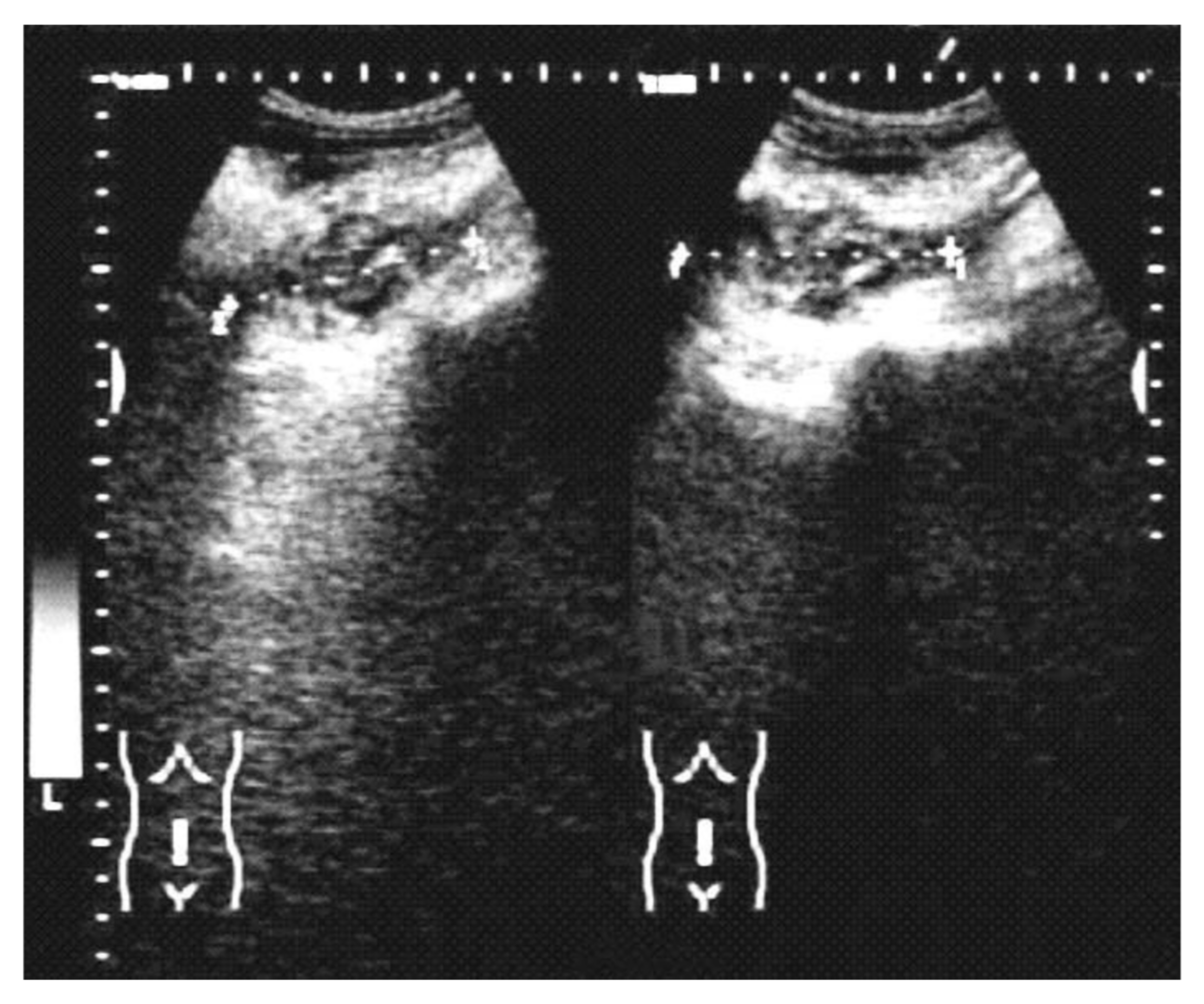
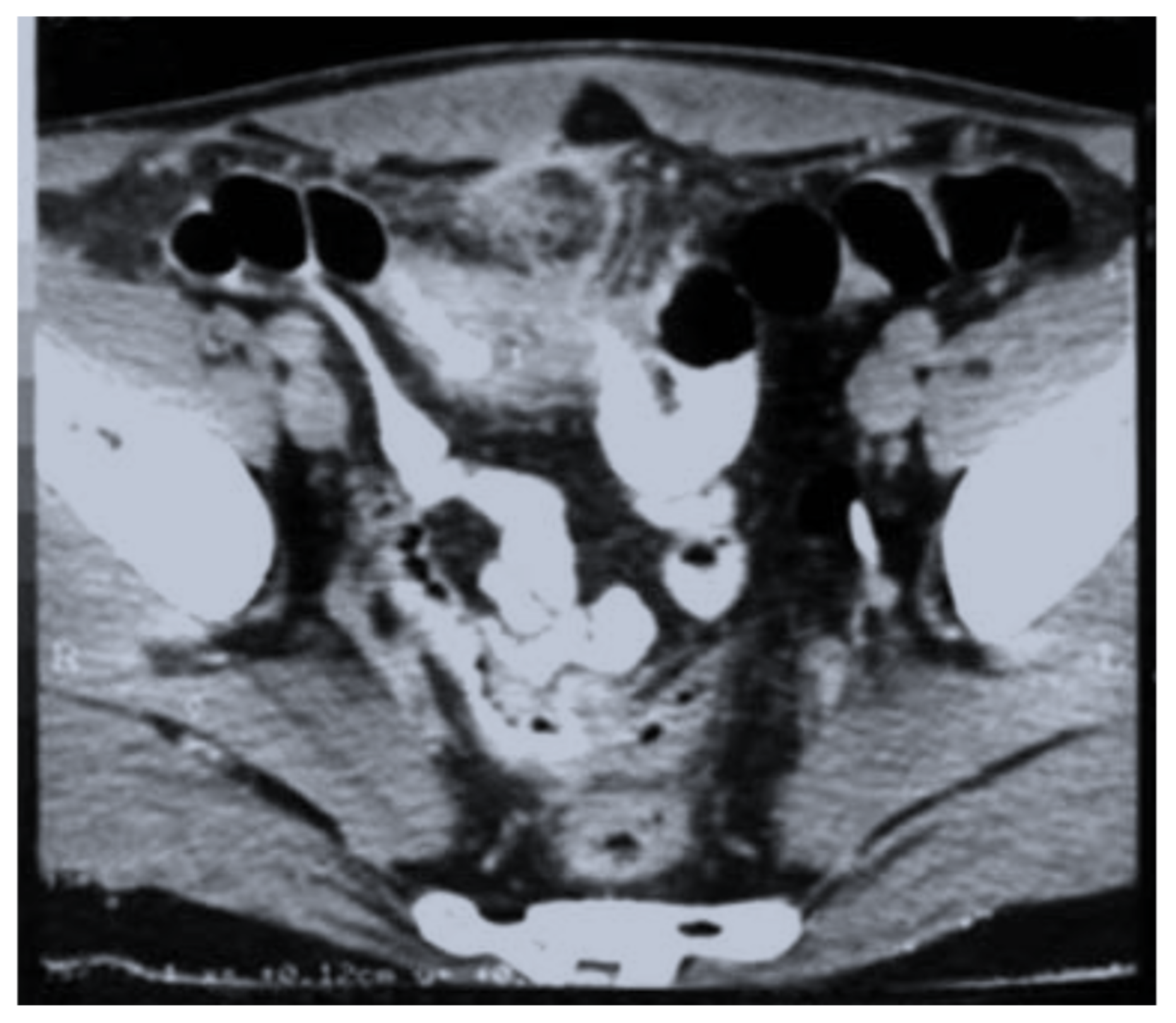
| Imaging (US, CT) characteristic | N (cases) (%) |
| Intraperitoneal collections | 11/28 (39.2%) |
| A heterogeneous mass involving the colon | 6/28 (21.4%) |
| Omental mass | 3/28 (10.7%) |
| Inflammatory mass involving the ovaries | 6/28 (21.4%) |
| Right liver abscesses | 2/28 (7.1%) |
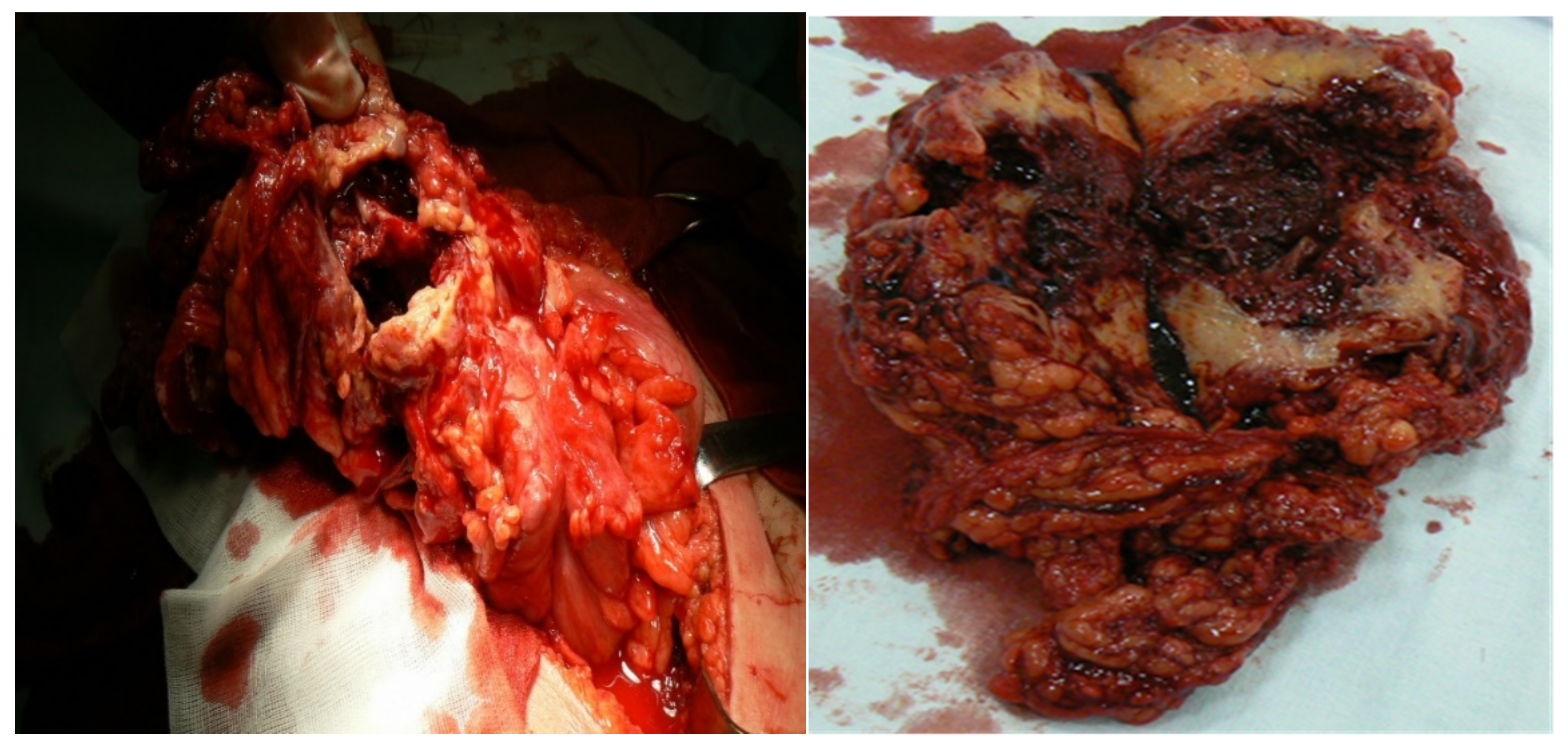
| Treatment | N (cases) (%) |
| Open approach | 6/28 (21.4%) |
| Right hemicolectomy | 3/6 (50%) |
| Segmental colectomy | 2/6 (33.3%) |
| Drainage of peritoneal abscess | 1/6 (17.6%) |
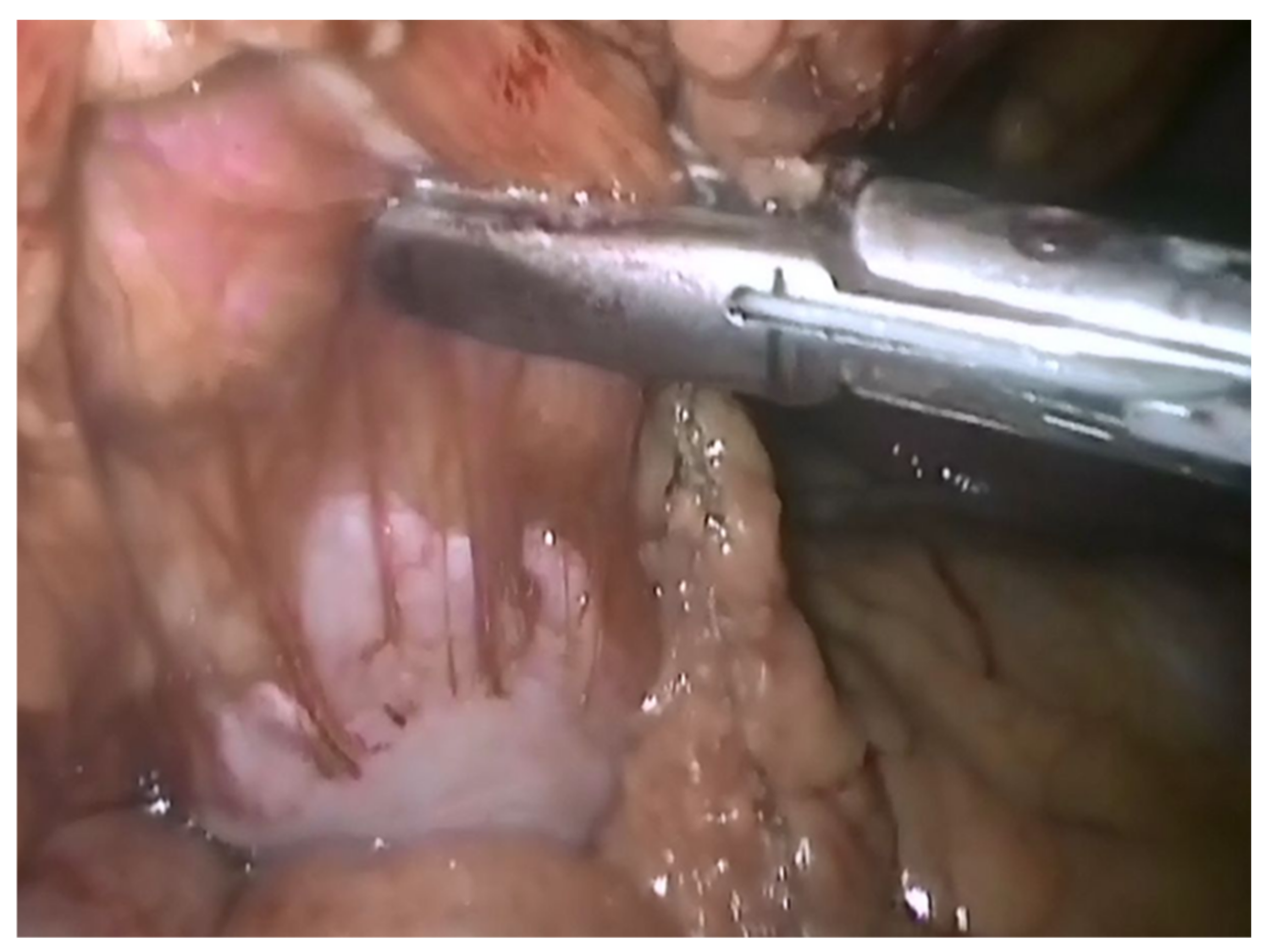
| Laparoscopic approach | 21/28 (21.4%) |
| Omental laparoscopic resection | 3/21 (14.2%) |
| Right hemicolectomy | 1/21 (4.7%) |
| Bilateral salpingo-oophorectomy | 6/21 (28.5%) |
| Drainage of peritoneal abscess | 11/21 (5.2%) |
| Drainage and biopsy of the liver abscess | 1/21 (4.7%) |
| Radiologic percutaneous approach of the liver abscess | 1/28 (3.5%) |
| Postoperative treatment—intravenous penicillin for 4–6 weeks (12 to 20 million units daily in divided doses every four to six hours) + amoxicillin oral | 6.5 months ± 4.6 months (3 weeks–12 months) |
| Recurrences | 3/28 (10.7%) |
| Author/Year | Total Cases | Involved Sites | Mean Age | Gender, M/F | Predisposing Factors | Leukocytosis | Presumptive Diagnosis | Final Diagnosis | Treatment |
|---|---|---|---|---|---|---|---|---|---|
| Yegüez JF et al., 2000 [33] | 1 | Rectosigmoid and cecum | 49 | F | − | − | Tumor of colon | Histologic diagnosis of surgical specimen | Resection and colostomy + actinomycosis medication |
| Cirafici L et al., 2002 [34] | 1 | Left colon | 56 | F | IUD | + | Tumor occlusive of colon | Histologic diagnosis of surgical specimen | Colostomy + actinomycosis medication |
| Chelli D et al., 2008 [35] | 5 | Pelvic inflammatory disease | 39.2 | F | IUD | + | Pelvic inflammatory disease | Culture of the microorganisms | Drainage + actinomycosis medication |
| Privitera A et al., 2009 [14] | 1 | Left colon | 67 | M | + | Abscessed tumors of the sigmoid colon | Histologic diagnosis of surgical specimen | Hartmann’s procedure + actinomycosis medication | |
| Lim KT et al., 2010 [36] | 1 | Abdominal wall mass that extended from the dome of the bladder | 26 | M | − | + | Urachal tumor | Histologic Diagnosis of Surgical Specimen | Partial cystectomy with abdominal wall mass excision + actinomycosis medication |
| Marret H et al., 2010 [37] | 11 | Ovary, colon, pelvic inflammatory disease | F | IUD | + | Pelvic inflammatory disease, ovarian cancer, bowel obstruction, acute peritonitis | Culture of the microorganisms, histologic diagnosis of surgical specimen | Total abdominal hysterectomy; salphingo-oophorectomy + actinomycosis medication | |
| Sung HY et al., 2011 [8] | 23 | Appendix (n = 5), ovarian mass (n = 5), abdominal wall mass (n = 4), colonic mass (n = 4), small bowel mass (n = 2), uterus mass (n = 2), and liver | 47.8 | 5 M/18 F | IUD, total abdominal hysterectomy, Caesarean section, a fish bone-induced rectal perforation polypectomy-induced microperforation, peritoneal dialysis, cholecystectomy with T-tube drainage | + | Acute appendicitis (n = 10), pelvic inflammatory disease (n = 8), and acute tubo-ovarian abscess (n = 4), ovarian cancer, or colon cancer | Histologic diagnosis of surgical specimen | Right hemicolectomy; left hemicolectomy; total abdominal hysterectomy; salphingo-oophorectomy + actinomycosis medication |
| Jabi R et al., 2020 [38] | 1 | Left colon | 48 | M | − | + | Tumor of the left colon | Histologic diagnosis of surgical specimen | Left segmental colectomy with latero-lateral mechanical anastomosis + actinomycosis medication |
| Asiri BI et al., 2020 [39] | 1 | Appendix | 38 | M | − | + | Acute appendicitis and cecum tumor | Histologic diagnosis of surgical specimen | Appendectomy and laparoscope-assisted ileocaecal resection with ileocolic anastomosis + actinomycosis medication |
| Kim S et al., 2020 [40] | 1 | Peritoneal and pelvic masses | 47 | F | IUD | − | Peritoneal carcinomatosis | Histologic diagnosis of surgical specimen | Peritoneal biopsy + actinomycosis medication |
| Pamathy G et al., 2021 [41] | 1 | Transverse and descending colon | 40 | F | IUD | + | Transverse and descending colon malignancy | Histologic diagnosis of surgical specimen | Left hemicolectomy |
| Clarrett D et al., 2021 [42] | 1 | Transverse colon, abdominal wall | 66 | M | − | − | Transverse colon malignancy | Histologic diagnosis of surgical specimen | Surgical resection of the right upper abdominal wall mass en bloc with right hemicolectomy |
| Tarzi M et al., 2021 [43] | 1 | Abdominal wall | 59 | M | Type 2 diabetes | − | Abdominal wall tumor | Histologic diagnosis of surgical specimen | Surgical excisional biopsy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vasilescu, A.M.; Târcoveanu, E.; Lupascu, C.; Blaj, M.; Lupascu Ursulescu, C.; Bradea, C. Abdominopelvic Actinomycosis—The Diagnostic and Therapeutic Challenge of the Most Misdiagnosed Disease. Life 2022, 12, 447. https://doi.org/10.3390/life12030447
Vasilescu AM, Târcoveanu E, Lupascu C, Blaj M, Lupascu Ursulescu C, Bradea C. Abdominopelvic Actinomycosis—The Diagnostic and Therapeutic Challenge of the Most Misdiagnosed Disease. Life. 2022; 12(3):447. https://doi.org/10.3390/life12030447
Chicago/Turabian StyleVasilescu, Alin Mihai, Eugen Târcoveanu, Cristian Lupascu, Mihaela Blaj, Corina Lupascu Ursulescu, and Costel Bradea. 2022. "Abdominopelvic Actinomycosis—The Diagnostic and Therapeutic Challenge of the Most Misdiagnosed Disease" Life 12, no. 3: 447. https://doi.org/10.3390/life12030447