
Postoperative Delirium and Postoperative Cognitive Dysfunction in Patients with Elective Hip or Knee Arthroplasty: A Narrative Review of the Literature

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. POD
3.1.1. Epidemiology
3.1.2. Risk Factors
3.1.3. History of Neuropsychiatric Conditions
3.1.4. Diagnosis
3.1.5. Pathophysiology and Biomarkers
3.1.6. Treatment
3.2. POCD
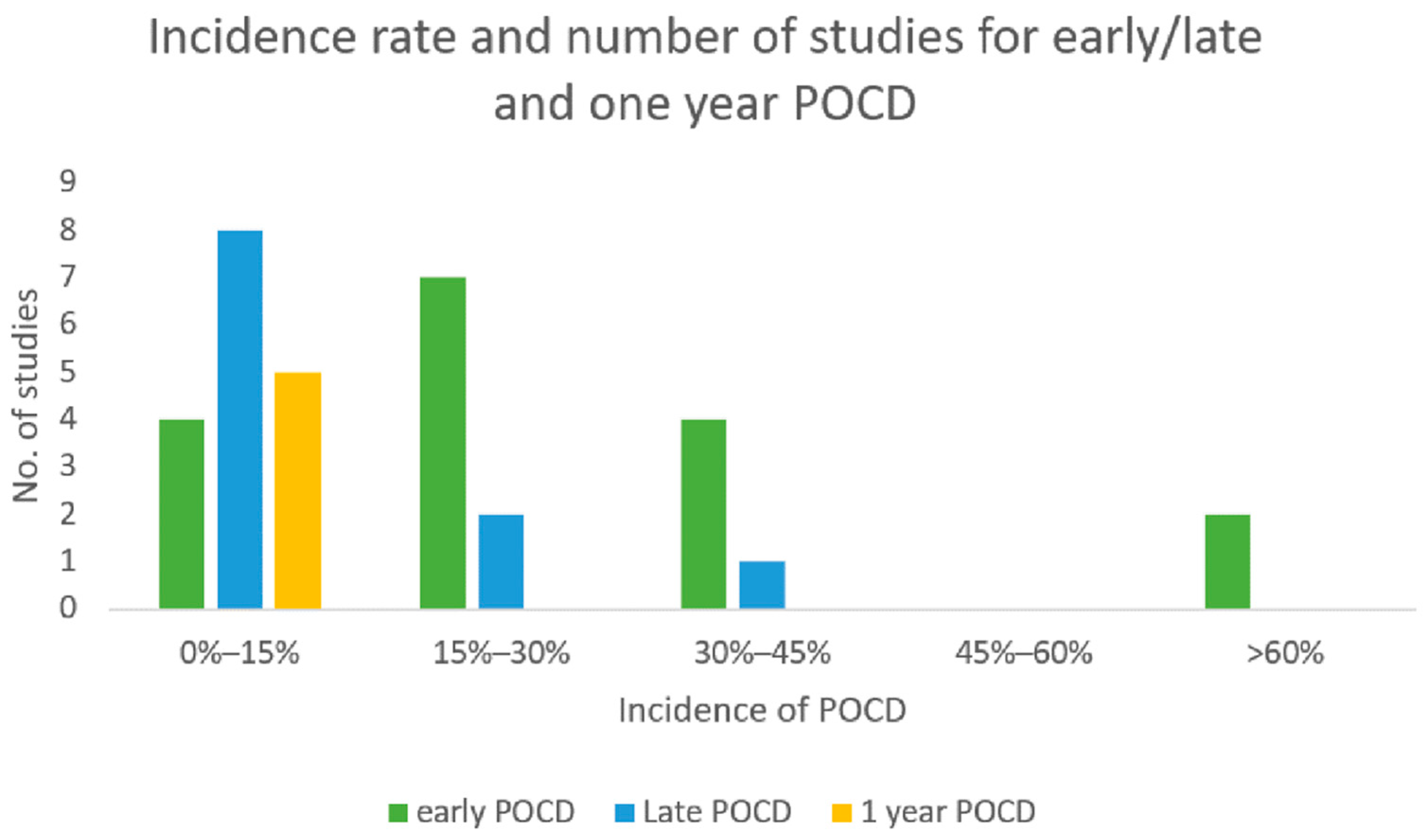
3.2.1. Epidemiology
3.2.2. Risk Factors
3.2.3. Diagnosis
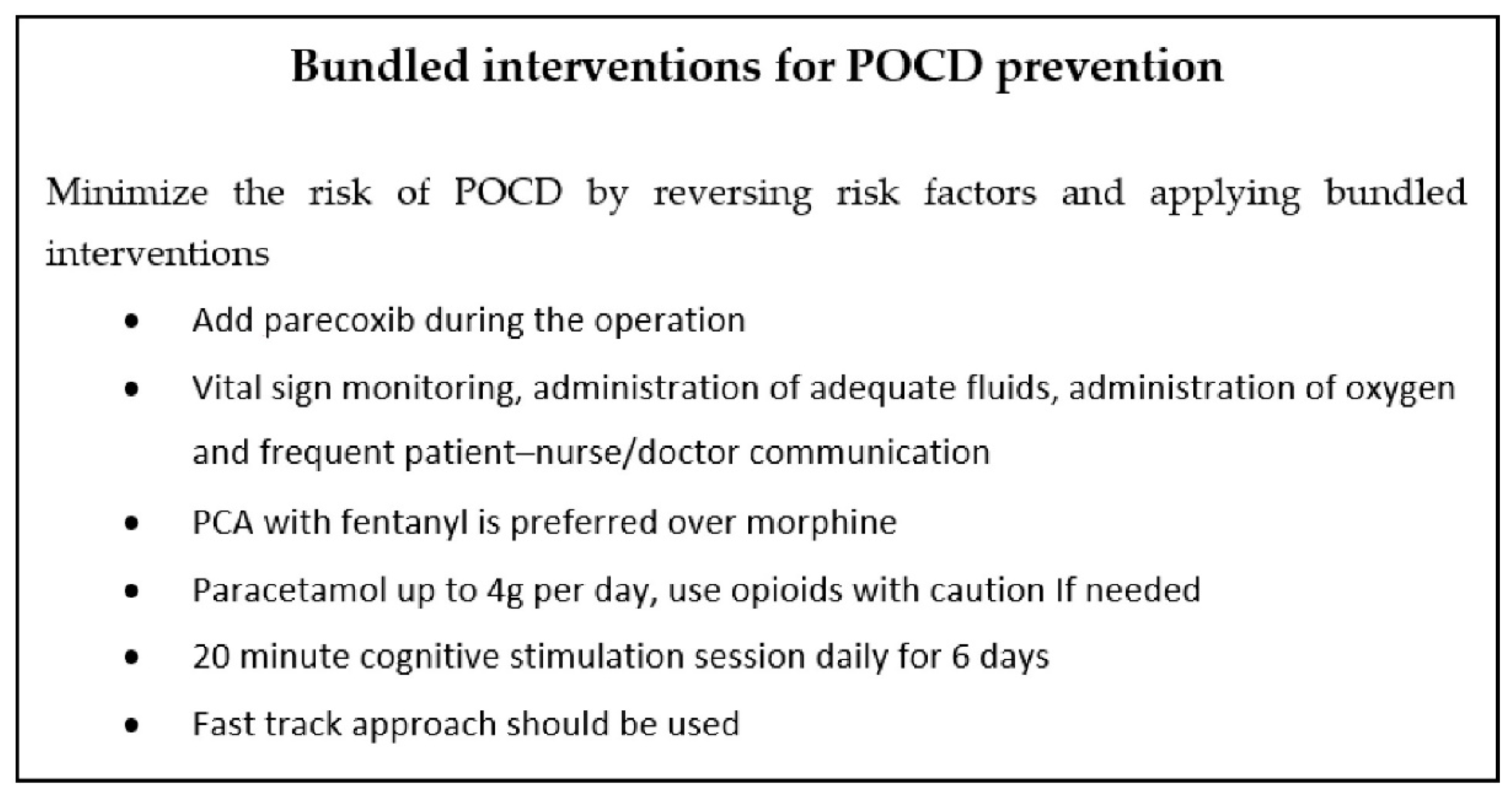
3.2.4. Treatment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferguson, R.J.; Palmer, A.J.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Maradit Kremers, H.; Larson, D.R.; Crowson, C.S.; Kremers, W.K.; Washington, R.E.; Steiner, C.A.; Jiranek, W.A.; Berry, D.J. Prevalence of Total Hip and Knee Replacement in the United States. J. Bone Jt. Surg.-Am. Vol. 2015, 97, 1386–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gai, N.; Lavi, R.; Jones, P.M.; Lee, H.; Naudie, D.; Bainbridge, D. The use of point-of-care ultrasound to diagnose patent foramen ovale in elective hip and knee arthroplasty patients and its association with postoperative delirium. Can. J. Anaesth. 2018, 65, 619–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viramontes, O.; Luan Erfe, B.M.; Erfe, J.M.; Brovman, E.Y.; Boehme, J.; Bader, A.M.; Urman, R.D. Cognitive impairment and postoperative outcomes in patients undergoing primary total hip arthroplasty: A systematic review. J. Clin. Anesth. 2019, 56, 65–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Räsänen, P.; Paavolainen, P.; Sintonen, H.; Koivisto, A.-M.; Blom, M.; Ryynänen, O.-P.; Roine, R.P. Effectiveness of hip or knee replacement surgery in terms of quality-adjusted life years and costs. Acta Orthop. 2007, 78, 108–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertsson, O.; Bizjajeva, S.; Fenstad, A.M.; Furnes, O.; Lidgren, L.; Mehnert, F.; Odgaard, A.; Pedersen, A.B.; Havelin, L.I. Knee arthroplasty in Denmark, Norway and Sweden: A pilot study from the Nordic Arthroplasty Register Association. Acta Orthop. 2010, 81, 82–89. [Google Scholar] [CrossRef]
- Aziz, K.T.; Best, M.J.; Naseer, Z.; Skolasky, R.L.; Ponnusamy, K.E.; Sterling, R.S.; Khanuja, H.S. The Association of Delirium with Perioperative Complications in Primary Elective Total Hip Arthroplasty. Clin. Orthop. Surg. 2018, 10, 286–291. [Google Scholar] [CrossRef]
- Petersen, P.B.; Jørgensen, C.C.; Kehlet, H. Lundbeck Foundation Centre for Fast-track Hip and Knee Replacement Collaborative Group Delirium after fast-track hip and knee arthroplasty—A cohort study of 6331 elderly patients. Acta Anaesthesiol. Scand. 2017, 61, 767–772. [Google Scholar] [CrossRef]
- Weinstein, S.M.; Poultsides, L.; Baaklini, L.R.; Mörwald, E.E.; Cozowicz, C.; Saleh, J.N.; Arrington, M.B.; Poeran, J.; Zubizarreta, N.; Memtsoudis, S.G. Postoperative delirium in total knee and hip arthroplasty patients: A study of perioperative modifiable risk factors. Br. J. Anaesth. 2018, 120, 999–1008. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Seok, S.; Kim, S.; Kim, K.; Lee, S.; Lee, K. The Risk Factors of Postoperative Delirium after Total Knee Arthroplasty. J. Knee Surg. 2017, 30, 600–605. [Google Scholar] [CrossRef]
- Jankowski, C.J.; Trenerry, M.R.; Cook, D.J.; Buenvenida, S.L.; Stevens, S.R.; Schroeder, D.R.; Warner, D.O. Cognitive and functional predictors and sequelae of postoperative delirium in elderly patients undergoing elective joInt. arthroplasty. Anesth. Analg. 2011, 112, 1186–1193. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Bin Abd Razak, H.R.; Yeo, S.J. Incidence of postoperative delirium in patients undergoing total knee arthroplasty-an Asian perspective. Ann. Transl. Med. 2017, 5, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, M.P.; Liang, M.H.; Daltroy, L.H.; Eaton, H.; Peteet, J.; Wright, E.; Albert, M. Delirium after elective orthopedic surgery: Risk factors and natural history. Int. J. Psychiatry Med. 1989, 19, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument: Methodological index for non-randomized studies. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 2nd ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Flink, B.J.; Rivelli, S.K.; Cox, E.A.; White, W.D.; Falcone, G.; Vail, T.P.; Young, C.C.; Bolognesi, M.P.; Krystal, A.D.; Trzepacz, P.T.; et al. Obstructive sleep apnea and incidence of postoperative delirium after elective knee replacement in the nondemented elderly. Anesthesiology 2012, 116, 788–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, K.A.; Kelly, S.E.; Stern, T.A.; Bode, R.H.; Price, L.L.; Hunter, D.J.; Gulczynski, D.; Bierbaum, B.E.; Sweeney, G.A.; Hoikala, K.A.; et al. Administration of olanzapine to prevent postoperative delirium in elderly joint-replacement patients: A randomized, controlled trial. Psychosomatics 2010, 51, 409–418. [Google Scholar] [CrossRef]
- Chung, K.S.; Lee, J.K.; Park, J.S.; Choi, C.H. Risk factors of delirium in patients undergoing total knee arthroplasty. Arch. Gerontol. Geriatr. 2015, 60, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Lowery, D.P.; Wesnes, K.; Ballard, C.G. Subtle attentional deficits in the absence of dementia are associated with an increased risk of post-operative delirium. Dement. Geriatr. Cogn. Disord. 2007, 23, 390–394. [Google Scholar] [CrossRef]
- Kudoh, A.; Takase, H.; Matsuno, S.; Katagai, H. A history of aggression is a risk factor for postoperative confusion in elderly male drinkers. J. Anesth. 2007, 21, 13–18. [Google Scholar] [CrossRef]
- Scott, J.E.; Mathias, J.L.; Kneebone, A.C. Incidence of delirium following total joInt. replacement in older adults: A meta-analysis. Gen. Hosp. Psychiatry 2015, 37, 223–229. [Google Scholar] [CrossRef]
- Sampson, E.L.; Raven, P.R.; Ndhlovu, P.N.; Vallance, A.; Garlick, N.; Watts, J.; Blanchard, M.R.; Bruce, A.; Blizard, R.; Ritchie, C.W. A randomized, double-blind, placebo-controlled trial of donepezil hydrochloride (Aricept) for reducing the incidence of postoperative delirium after elective total hip replacement. Int. J. Geriatr. Psychiatry 2007, 22, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Qi, J.; Liu, C.; Chen, L.; Chen, J. Postoperative Serum Albumin Decrease Independently Predicts Delirium in the Elderly Subjects after Total JoInt. Arthroplasty. Curr. Pharm. Des. 2020, 26, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Mu, D.-L.; Zhang, D.-Z.; Wang, D.-X.; Wang, G.; Li, C.-J.; Meng, Z.-T.; Li, Y.-W.; Liu, C.; Li, X.-Y. Parecoxib Supplementation to Morphine Analgesia Decreases Incidence of Delirium in Elderly Patients After Hip or Knee Replacement Surgery: A Randomized Controlled Trial. Anesth. Analg. 2017, 124, 1992–2000. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, E.L.; Mawhinney, T.; Beverland, D.; O’Brien, S.; McAuley, D.F.; Cairns, R.; Passmore, P.; McGuinness, B. Observational cohort study examining apolipoprotein E status and preoperative neuropsychological performance as predictors of post-operative delirium in an older elective arthroplasty population. Age Ageing 2017, 46, 779–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Y.-X.; Liu, F.-F.; Jia, M.; Yang, J.-J.; Shen, J.-C.; Zhu, G.-M.; Zhu, S.-H.; Li, W.-Y.; Yang, J.-J.; Ji, M.-H. Comparison of restrictive and liberal transfusion strategy on postoperative delirium in aged patients following total hip replacement: A preliminary study. Arch. Gerontol. Geriatr. 2014, 59, 181–185. [Google Scholar] [CrossRef]
- Cerejeira, J.; Batista, P.; Nogueira, V.; Vaz-Serra, A.; Mukaetova-Ladinska, E.B. The stress response to surgery and postoperative delirium: Evidence of hypothalamic-pituitary-adrenal axis hyperresponsiveness and decreased suppression of the GH/IGF-1 Axis. J. Geriatr. Psychiatry Neurol. 2013, 26, 185–194. [Google Scholar] [CrossRef]
- Cerejeira, J.; Nogueira, V.; Luís, P.; Vaz-Serra, A.; Mukaetova-Ladinska, E.B. The cholinergic system and inflammation: Common pathways in delirium pathophysiology. J. Am. Geriatr. Soc. 2012, 60, 669–675. [Google Scholar] [CrossRef]
- Krenk, L.; Rasmussen, L.S.; Hansen, T.B.; Bogø, S.; Søballe, K.; Kehlet, H. Delirium after fast-track hip and knee arthroplasty. Br. J. Anaesth. 2012, 108, 607–611. [Google Scholar] [CrossRef] [Green Version]
- Lowery, D.P.; Wesnes, K.; Brewster, N.; Ballard, C. Quantifying the association between computerised measures of attention and confusion assessment method defined delirium: A prospective study of older orthopaedic surgical patients, free of dementia. Int. J. Geriatr. Psychiatry 2008, 23, 1253–1260. [Google Scholar] [CrossRef]
- Priner, M.; Jourdain, M.; Bouche, G.; Merlet-Chicoine, I.; Chaumier, J.-A.; Paccalin, M. Usefulness of the short IQCODE for predicting postoperative delirium in elderly patients undergoing hip and knee replacement surgery. Gerontology 2008, 54, 116–119. [Google Scholar] [CrossRef]
- Freter, S.H.; Dunbar, M.J.; MacLeod, H.; Morrison, M.; MacKnight, C.; Rockwood, K. Predicting post-operative delirium in elective orthopaedic patients: The Delirium Elderly At-Risk (DEAR) instrument. Age Ageing 2005, 34, 169–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farlinger, C.; Clarke, H.; Wong, C.L. Perioperative pregabalin and delirium following total hip arthroplasty: A post hoc analysis of a double-blind randomized placebo-controlled trial. Can. J. Anaesth. 2018, 65, 1269–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radcliff, K.E.; Orozco, F.R.; Quinones, D.; Rhoades, D.; Sidhu, G.S.; Ong, A.C. Preoperative risk stratification reduces the incidence of perioperative complications after total knee arthroplasty. J. Arthroplast. 2012, 27, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Pulido, L.; Parvizi, J.; Macgibeny, M.; Sharkey, P.F.; Purtill, J.J.; Rothman, R.H.; Hozack, W.J. In hospital complications after total joInt. arthroplasty. J. Arthroplast. 2008, 23, 139–145. [Google Scholar] [CrossRef]
- Kinjo, S.; Lim, E.; Sands, L.P.; Bozic, K.J.; Leung, J.M. Does using a femoral nerve block for total knee replacement decrease postoperative delirium? BMC Anesth. 2012, 12, 4. [Google Scholar] [CrossRef] [Green Version]
- Fisher, B.W.; Flowerdew, G. A simple model for predicting postoperative delirium in older patients undergoing elective orthopedic surgery. J. Am. Geriatr. Soc. 1995, 43, 175–178. [Google Scholar] [CrossRef]
- Williams-Russo, P.; Urquhart, B.L.; Sharrock, N.E.; Charlson, M.E. Post-operative delirium: Predictors and prognosis in elderly orthopedic patients. J. Am. Geriatr. Soc. 1992, 40, 759–767. [Google Scholar] [CrossRef]
- Kudoh, A.; Takase, H.; Takahira, Y.; Takazawa, T. Postoperative confusion increases in elderly long-term benzodiazepine users. Anesth. Analg. 2004, 99, 1674–1678. [Google Scholar] [CrossRef]
- Williams-Russo, P.; Sharrock, N.E.; Mattis, S.; Szatrowski, T.P.; Charlson, M.E. Cognitive effects after epidural vs. general anesthesia in older adults. A randomized trial. JAMA 1995, 274, 44–50. [Google Scholar] [CrossRef]
- Rade, M.C.; Yadeau, J.T.; Ford, C.; Reid, M.C. Postoperative delirium in elderly patients after elective hip or knee arthroplasty performed under regional anesthesia. HSS J. 2011, 7, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Culley, D.J.; Flaherty, D.; Fahey, M.C.; Rudolph, J.L.; Javedan, H.; Huang, C.-C.; Wright, J.; Bader, A.M.; Hyman, B.T.; Blacker, D.; et al. Poor Performance on a Preoperative Cognitive Screening Test Predicts Postoperative Complications in Older Orthopedic Surgical Patients. Anesthesiology 2017, 127, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Puustinen, J.; Luostarinen, L.; Luostarinen, M.; Pulliainen, V.; Huhtala, H.; Soini, M.; Suhonen, J. The Use of MoCA and Other Cognitive Tests in Evaluation of Cognitive Impairment in Elderly Patients Undergoing Arthroplasty. Geriatr. Orthop. Surg. Rehabil. 2016, 7, 183–187. [Google Scholar] [CrossRef]
- Xie, Z.; Swain, C.A.; Ward, S.A.P.; Zheng, H.; Dong, Y.; Sunder, N.; Burke, D.W.; Escobar, D.; Zhang, Y.; Marcantonio, E.R. Preoperative cerebrospinal fluid β-Amyloid/Tau ratio and postoperative delirium. Ann. Clin. Transl. Neurol. 2014, 1, 319–328. [Google Scholar] [CrossRef]
- Xie, H.; Huang, D.; Zhang, S.; Hu, X.; Guo, J.; Wang, Z.; Zhou, G. Relationships between adiponectin and matrix metalloproteinase-9 (MMP-9) serum levels and postoperative cognitive dysfunction in elderly patients after general anesthesia. Aging Clin. Exp. Res. 2016, 28, 1075–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dighe, K.; Clarke, H.; McCartney, C.J.; Wong, C.L. Perioperative gabapentin and delirium following total knee arthroplasty: A post-hoc analysis of a double-blind randomized placebo-controlled trial. Can. J. Anaesth. 2014, 61, 1136–1137. [Google Scholar] [CrossRef]
- Cunningham, E.L.; McGuinness, B.; McAuley, D.F.; Toombs, J.; Mawhinney, T.; O’Brien, S.; Beverland, D.; Schott, J.M.; Lunn, M.P.; Zetterberg, H.; et al. CSF Beta-amyloid 1-42 Concentration Predicts Delirium Following Elective Arthroplasty Surgery in an Observational Cohort Study. Ann. Surg. 2019, 269, 1200–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duque, A.F.; Post, Z.D.; Orozco, F.R.; Lutz, R.W.; Ong, A.C. A Proactive Approach to High Risk Delirium Patients Undergoing Total JoInt. Arthroplasty. J. Arthroplast. 2018, 33, 1171–1176. [Google Scholar] [CrossRef]
- Petre, B.M.; Roxbury, C.R.; McCallum, J.R.; Defontes, K.W.; Belkoff, S.M.; Mears, S.C. Pain reporting, opiate dosing, and the adverse effects of opiates after hip or knee replacement in patients 60 years old or older. Geriatr. Orthop. Surg. Rehabil. 2012, 3, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Bellelli, G.; Speciale, S.; Trabucchi, M. Predictors of delirium during in-hospital rehabilitation in elderly patients after hip arthroplasty. Age Ageing 2005, 34, 532. [Google Scholar] [CrossRef]
- Jain, F.A.; Brooks, J.O.; Larsen, K.A.; Kelly, S.E.; Bode, R.H.; Sweeney, G.A.; Stern, T.A. Individual risk profiles for postoperative delirium after joInt. replacement surgery. Psychosomatics 2011, 52, 410–416. [Google Scholar] [CrossRef]
- Nandi, S.; Harvey, W.F.; Saillant, J.; Kazakin, A.; Talmo, C.; Bono, J. Pharmacologic risk factors for post-operative delirium in total joInt. arthroplasty patients: A case-control study. J. Arthroplast. 2014, 29, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Yen, T.E.; Allen, J.C.; Rivelli, S.K.; Patterson, S.C.; Metcalf, M.R.; Flink, B.J.; Mirrakhimov, A.E.; Lagoo, S.A.; Vail, T.P.; Young, C.C.; et al. Association between Serum IGF-I levels and Postoperative Delirium in Elderly Subjects Undergoing Elective Knee Arthroplasty. Sci. Rep. 2016, 6, 20736. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.M.; Parvizi, J.; Hanssen, A.D.; Gay, P.C. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement: A case-control study. Mayo Clin. Proc. 2001, 76, 897–905. [Google Scholar] [CrossRef]
- Wang, J.; Li, Z.; Yu, Y.; Li, B.; Shao, G.; Wang, Q. Risk factors contributing to postoperative delirium in geriatric patients postorthopedic surgery: Postoperative delirium. Asia-Pac. Psychiatry 2015, 7, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Simpson, C.J.; Kellett, J.M. The relationship between pre-operative anxiety and post-operative delirium. J. Psychosom. Res. 1987, 31, 491–497. [Google Scholar] [CrossRef]
- Gholson, J.J.; Bedard, N.A.; Dowdle, S.B.; Brown, T.S.; Gao, Y.; Callaghan, J.J. Total JoInt. Arthroplasty in Patients With Schizophrenia: How Much Does It Increase the Risk of Complications? J. Arthroplast. 2018, 33, 2082–2086. [Google Scholar] [CrossRef]
- Price, C.C.; Levy, S.-A.; Tanner, J.; Garvan, C.; Ward, J.; Akbar, F.; Bowers, D.; Rice, M.; Okun, M. Orthopedic Surgery and Post-Operative Cognitive Decline in Idiopathic Parkinson’s Disease: Considerations from a Pilot Study. J. Parkinsons Dis. 2015, 5, 893–905. [Google Scholar] [CrossRef] [Green Version]
- Newman, J.M.; Sodhi, N.; Dalton, S.E.; Khlopas, A.; Newman, R.P.; Higuera, C.A.; Mont, M.A. Does Parkinson Disease Increase the Risk of Perioperative Complications After Total Hip Arthroplasty? A Nationwide Database Study. J. Arthroplast. 2018, 33, S162–S166. [Google Scholar] [CrossRef]
- Van Meenen, L.C.C.; van Meenen, D.M.P.; de Rooij, S.E.; ter Riet, G. Risk prediction models for postoperative delirium: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2014, 62, 2383–2390. [Google Scholar] [CrossRef]
- Inouye, S.K.; van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Steiner, L.A. Postoperative delirium. Part 1: Pathophysiology and risk factors. Eur. J. Anaesthesiol. 2011, 28, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shen, X. Postoperative delirium in the elderly: The potential neuropathogenesis. Aging Clin. Exp. Res. 2018, 30, 1287–1295. [Google Scholar] [CrossRef] [PubMed]
- Cerejeira, J.; Batista, P.; Nogueira, V.; Firmino, H.; Vaz-Serra, A.; Mukaetova-Ladinska, E.B. Low preoperative plasma cholinesterase activity as a risk marker of postoperative delirium in elderly patients. Age Ageing 2011, 40, 621–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krenk, L.; Kehlet, H.; Bæk Hansen, T.; Solgaard, S.; Soballe, K.; Rasmussen, L.S. Cognitive dysfunction after fast-track hip and knee replacement. Anesth. Analg. 2014, 118, 1034–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, M.-H.; Yuan, H.-M.; Zhang, G.-F.; Li, X.-M.; Dong, L.; Li, W.-Y.; Zhou, Z.-Q.; Yang, J.-J. Changes in plasma and cerebrospinal fluid biomarkers in aged patients with early postoperative cognitive dysfunction following total hip-replacement surgery. J. Anesth. 2013, 27, 236–242. [Google Scholar] [CrossRef]
- Patel, R.V.; Stygall, J.; Harrington, J.; Newman, S.P.; Haddad, F.S. Cerebral microembolization during primary total hip arthroplasty and neuropsychologic outcome: A pilot study. Clin. Orthop. Relat. Res. 2010, 468, 1621–1629. [Google Scholar] [CrossRef] [Green Version]
- Cavallari, M.; Dai, W.; Guttmann, C.R.G.; Meier, D.S.; Ngo, L.H.; Hshieh, T.T.; Callahan, A.E.; Fong, T.G.; Schmitt, E.; Dickerson, B.C.; et al. Neural substrates of vulnerability to postsurgical delirium as revealed by presurgical diffusion MRI. Brain 2016, 139, 1282–1294. [Google Scholar] [CrossRef] [Green Version]
- Krenk, L.; Rasmussen, L.S.; Kehlet, H. Delirium in the fast-track surgery setting. Best Pr. Res. Clin. Anaesthesiol. 2012, 26, 345–353. [Google Scholar] [CrossRef]
- Herrick, I.A.; Ganapathy, S.; Komar, W.; Kirkby, J.; Moote, C.A.; Dobkowski, W.; Eliasziw, M. Postoperative cognitive impairment in the elderly. Choice of patient-controlled analgesia opioid. Anaesthesia 1996, 51, 356–360. [Google Scholar] [CrossRef]
- Duggleby, W.; Lander, J. Cognitive status and postoperative pain: Older adults. J. Pain Symptom Manag. 1994, 9, 19–27. [Google Scholar] [CrossRef]
- Guay, J.; Johnson, R.L.; Kopp, S. Nerve blocks or no nerve blocks for pain control after elective hip replacement (arthroplasty) surgery in adults. Cochrane Database Syst. Rev. 2017, 10, CD011608. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, H.; Mohan, H.; Hare, C.O.; Reynolds, J.V.; Kenny, R.A. Mind Over Matter? The Hidden Epidemic of Cognitive Dysfunction in the Older Surgical Patient. Ann. Surg. 2017, 265, 677–691. [Google Scholar] [CrossRef] [PubMed]
- Moller, J.T.; Cluitmans, P.; Rasmussen, L.S.; Houx, P.; Rasmussen, H.; Canet, J.; Rabbitt, P.; Jolles, J.; Larsen, K.; Hanning, C.D.; et al. Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet 1998, 351, 857–861. [Google Scholar] [CrossRef]
- Evered, L.; Silbert, B.; Scott, D.A.; Ames, D.; Maruff, P.; Blennow, K. Cerebrospinal Fluid Biomarker for Alzheimer Disease Predicts Postoperative Cognitive Dysfunction. Anesthesiology 2016, 124, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Silbert, B.; Evered, L.; Scott, D.A.; McMahon, S.; Choong, P.; Ames, D.; Maruff, P.; Jamrozik, K. Preexisting cognitive impairment is associated with postoperative cognitive dysfunction after hip joInt. replacement surgery. Anesthesiology 2015, 122, 1224–1234. [Google Scholar] [CrossRef] [PubMed]
- Li, W.-X.; Luo, R.-Y.; Chen, C.; Li, X.; Ao, J.-S.; Liu, Y.; Yin, Y.-Q. Effects of propofol, dexmedetomidine, and midazolam on postoperative cognitive dysfunction in elderly patients: A randomized controlled preliminary trial. Chin. Med. J. 2019, 132, 437–445. [Google Scholar] [CrossRef]
- Konishi, Y.; Evered, L.A.; Scott, D.A.; Silbert, B.S. Postoperative cognitive dysfunction after sevoflurane or propofol general anaesthesia in combination with spinal anaesthesia for hip arthroplasty. Anaesth. Intensive Care 2018, 46, 596–600. [Google Scholar] [CrossRef] [Green Version]
- Koch, S.; Forteza, A.; Lavernia, C.; Romano, J.G.; Campo-Bustillo, I.; Campo, N.; Gold, S. Cerebral fat microembolism and cognitive decline after hip and knee replacement. Stroke 2007, 38, 1079–1081. [Google Scholar] [CrossRef]
- Rodriguez, R.A.; Tellier, A.; Grabowski, J.; Fazekas, A.; Turek, M.; Miller, D.; Wherrett, C.; Villeneuve, P.J.; Giachino, A. Cognitive dysfunction after total knee arthroplasty: Effects of intraoperative cerebral embolization and postoperative complications. J. Arthroplast. 2005, 20, 763–771. [Google Scholar] [CrossRef]
- Rasmussen, L.S.; Schmehl, W.; Jakobsson, J. Comparison of xenon with propofol for supplementary general anaesthesia for knee replacement: A randomized study. Br. J. Anaesth. 2006, 97, 154–159. [Google Scholar] [CrossRef] [Green Version]
- Deo, H.; West, G.; Butcher, C.; Lewis, P. The prevalence of cognitive dysfunction after conventional and computer-assisted total knee replacement. Knee 2011, 18, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Evered, L.; Scott, D.A.; Silbert, B.; Maruff, P. Postoperative cognitive dysfunction is independent of type of surgery and anesthetic. Anesth. Analg. 2011, 112, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.; Zhang, F.; Xue, Q.; Yu, B. Accuracy of regional cerebral oxygen saturation in predicting postoperative cognitive dysfunction after total hip arthroplasty: Regional cerebral oxygen saturation predicts POCD. J. Arthroplast. 2013, 28, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Ni, C.; Xu, T.; Li, N.; Tian, Y.; Han, Y.; Xue, Q.; Li, M.; Guo, X. Cerebral oxygen saturation after multiple perioperative influential factors predicts the occurrence of postoperative cognitive dysfunction. BMC Anesth. 2015, 15, 156. [Google Scholar] [CrossRef] [Green Version]
- Postler, A.; Neidel, J.; Günther, K.-P.; Kirschner, S. Incidence of early postoperative cognitive dysfunction and other adverse events in elderly patients undergoing elective total hip replacement (THR). Arch. Gerontol. Geriatr. 2011, 53, 328–333. [Google Scholar] [CrossRef]
- Salazar, F.; Doñate, M.; Boget, T.; Bogdanovich, A.; Basora, M.; Torres, F.; Fàbregas, N. Intraoperative warming and post-operative cognitive dysfunction after total knee replacement. Acta Anaesthesiol. Scand. 2011, 55, 216–222. [Google Scholar] [CrossRef]
- Zhu, S.-H.; Ji, M.-H.; Gao, D.-P.; Li, W.-Y.; Yang, J.-J. Association between perioperative blood transfusion and early postoperative cognitive dysfunction in aged patients following total hip replacement surgery. UPS J. Med. Sci. 2014, 119, 262–267. [Google Scholar] [CrossRef]
- Yan, L.; Liu, Q.; Zhu, Y.; Zhou, M.; Wang, H.; Qin, X.; Wang, L. Association of Preexisting Neurocognitive Impairments and Perioperative Neurocognitive Disorders for Hip JoInt. Replacement Surgery: A Prospective Cohort Study. Med. Sci. Monit. 2019, 25, 4617–4626. [Google Scholar] [CrossRef]
- Scarmeas, N.; Stern, Y. Cognitive Reserve and Lifestyle. J. Clin. Exp. Neuropsychol. 2003, 25, 625–633. [Google Scholar] [CrossRef]
- Scott, J.E.; Mathias, J.L.; Kneebone, A.C.; Krishnan, J. Postoperative cognitive dysfunction and its relationship to cognitive reserve in elderly total joInt. replacement patients. J. Clin. Exp. Neuropsychol. 2017, 39, 459–472. [Google Scholar] [CrossRef]
- Hou, R.; Wang, H.; Chen, L.; Qiu, Y.; Li, S. POCD in patients receiving total knee replacement under deep vs. light anesthesia: A randomized controlled trial. Brain Behav. 2018, 8, e00910. [Google Scholar] [CrossRef]
- Jones, M.J.; Piggott, S.E.; Vaughan, R.S.; Bayer, A.J.; Newcombe, R.G.; Twining, T.C.; Pathy, J.; Rosen, M. Cognitive and functional competence after anaesthesia in patients aged over 60: Controlled trial of general and regional anaesthesia for elective hip or knee replacement. BMJ 1990, 300, 1683–1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macfarlane, A.J.R.; Prasad, G.A.; Chan, V.W.S.; Brull, R. Does regional anesthesia improve outcome after total knee arthroplasty? Clin. Orthop. Relat. Res. 2009, 467, 2379–2402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, D.; Bowes, J.B.; Brown, M.W. Changes in memory following general or spinal anaesthesia for hip arthroplasty. Anaesthesia 1988, 43, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Nielson, W.R.; Gelb, A.W.; Casey, J.E.; Penny, F.J.; Merchant, R.N.; Manninen, P.H. Long-term cognitive and social sequelae of general versus regional anesthesia during arthroplasty in the elderly. Anesthesiology 1990, 73, 1103–1109. [Google Scholar] [CrossRef]
- Hizel, L.P.; Warner, E.D.; Wiggins, M.E.; Tanner, J.J.; Parvataneni, H.; Davis, R.; Penney, D.L.; Libon, D.J.; Tighe, P.; Garvan, C.W.; et al. Clock Drawing Performance Slows for Older Adults After Total Knee Replacement Surgery. Anesth. Analg. 2019, 129, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Salazar, F.; Doñate, M.; Boget, T.; Bogdanovich, A.; Basora, M.; Torres, F.; Gracia, I.; Fàbregas, N. Relationship between intraoperative regional cerebral oxygen saturation trends and cognitive decline after total knee replacement: A post-hoc analysis. BMC Anesth. 2014, 14, 58. [Google Scholar] [CrossRef] [Green Version]
- Gray, A.C.; Torrens, L.; Howie, C.; Christie, J.; Robinson, C.M. Cognitive function and cerebral emboli after primary hip arthroplasty. HIP Int. 2008, 18, 40–45. [Google Scholar] [CrossRef]
- Cheng, C.-M.; Chiu, M.-J.; Wang, J.-H.; Liu, H.-C.; Shyu, Y.-I.L.; Huang, G.-H.; Chen, C.C.-H. Cognitive stimulation during hospitalization improves global cognition of older Taiwanese undergoing elective total knee and hip replacement surgery. J. Adv. Nurs. 2012, 68, 1322–1329. [Google Scholar] [CrossRef]
- Zhu, Y.-Z.; Yao, R.; Zhang, Z.; Xu, H.; Wang, L.-W. Parecoxib prevents early postoperative cognitive dysfunction in elderly patients undergoing total knee arthroplasty: A double-blind, randomized clinical consort study. Medicine 2016, 95, e4082. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Incidence Rate of POD | No. of Studies |
|---|---|
| 0–5% | 7 |
| 5–10% | 3 |
| 10–15% | 11 |
| 15–20% | 2 |
| 20–25% | 5 |
| 25–30% | 3 |
| >30% | 4 |
| Risk factors | Diagnosis of POD | Treatment |
|---|---|---|
| CAM4  criteria: criteria:
| Risk stratification and implementation of a multiple component prevention protocol for high risk patients |
| Risk Factors | Diagnosis | Treatment |
|---|---|---|
| Comparing the preoperative and postoperative scores of different neurocognitive tests | Minimize the risk of POCD development by reversing risk factors and applying interventions
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitsis, P.; Zisimou, T.; Gkiatas, I.; Kostas-Agnantis, I.; Gelalis, I.; Korompilias, A.; Pakos, E. Postoperative Delirium and Postoperative Cognitive Dysfunction in Patients with Elective Hip or Knee Arthroplasty: A Narrative Review of the Literature. Life 2022, 12, 314. https://doi.org/10.3390/life12020314
Kitsis P, Zisimou T, Gkiatas I, Kostas-Agnantis I, Gelalis I, Korompilias A, Pakos E. Postoperative Delirium and Postoperative Cognitive Dysfunction in Patients with Elective Hip or Knee Arthroplasty: A Narrative Review of the Literature. Life. 2022; 12(2):314. https://doi.org/10.3390/life12020314
Chicago/Turabian StyleKitsis, Petros, Theopisti Zisimou, Ioannis Gkiatas, Ioannis Kostas-Agnantis, Ioannis Gelalis, Anastasios Korompilias, and Emilios Pakos. 2022. "Postoperative Delirium and Postoperative Cognitive Dysfunction in Patients with Elective Hip or Knee Arthroplasty: A Narrative Review of the Literature" Life 12, no. 2: 314. https://doi.org/10.3390/life12020314