
Comparison of Clinical Efficacy and Safety between 70–150 µm and 100–300 µm Doxorubicin Drug-Eluting Bead Transarterial Chemoembolization for Hepatocellular Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
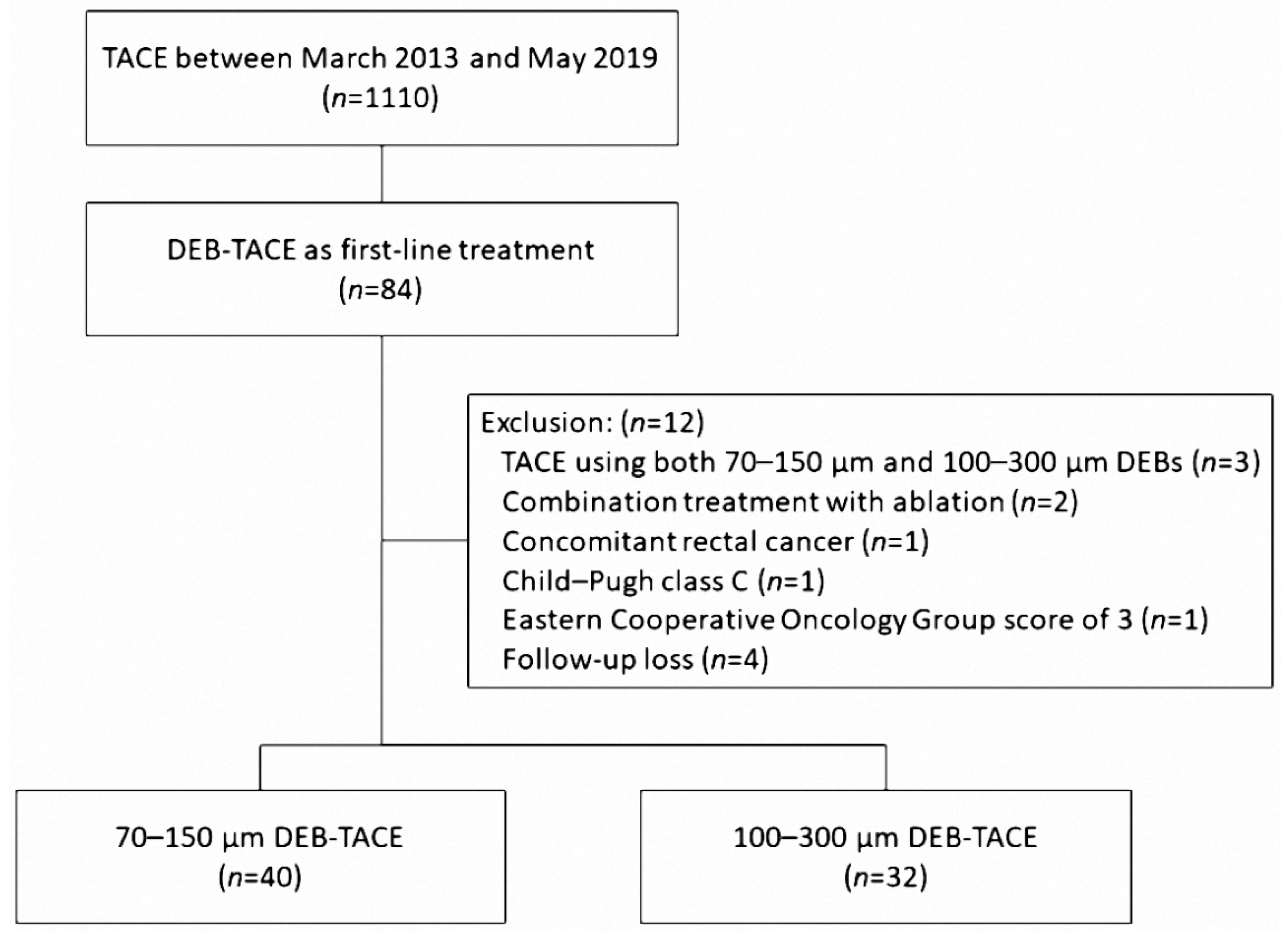
2.1. Patient Population
2.2. DEB-TACE Procedure
2.3. Follow-Up and Assessments
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Treatment Response
3.3. Safety Assessment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. Eur. J. Cancer 2012, 48, 599–641. [CrossRef] [PubMed]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [PubMed] [Green Version]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Xie, Z.B.; Wang, X.B.; Peng, Y.C.; Zhu, S.L.; Ma, L.; Xiang, B.D.; Gong, W.F.; Chen, J.; You, X.M.; Jiang, J.H.; et al. Systematic review comparing the safety and efficacy of conventional and drug-eluting bead transarterial chemoembolization for inoperable hepatocellular carcinoma. Hepatol. Res. 2015, 45, 190–200. [Google Scholar] [CrossRef]
- Varela, M.; Real, M.I.; Burrel, M.; Forner, A.; Sala, M.; Brunet, M.; Ayuso, C.; Castells, L.; Montañá, X.; Llovet, J.M.; et al. Chemoembolization of hepatocellular carcinoma with drug eluting beads: Efficacy and doxorubicin pharmacokinetics. J. Hepatol. 2007, 46, 474–481. [Google Scholar] [CrossRef]
- Sacco, R.; Bargellini, I.; Bertini, M.; Bozzi, E.; Romano, A.; Petruzzi, P.; Tumino, E.; Ginanni, B.; Federici, G.; Cioni, R.; et al. Conventional versus doxorubicin-eluting bead transarterial chemoembolization for hepatocellular carcinoma. J. Vasc. Interv. Radiol. JVIR 2011, 22, 1545–1552. [Google Scholar] [CrossRef]
- Golfieri, R.; Giampalma, E.; Renzulli, M.; Cioni, R.; Bargellini, I.; Bartolozzi, C.; Breatta, A.D.; Gandini, G.; Nani, R.; Gasparini, D.; et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br. J. Cancer 2014, 111, 255–264. [Google Scholar] [CrossRef] [Green Version]
- Lammer, J.; Malagari, K.; Vogl, T.; Pilleul, F.; Denys, A.; Watkinson, A.; Pitton, M.; Sergent, G.; Pfammatter, T.; Terraz, S.; et al. Prospective randomized study of doxorubicin-eluting-bead embolization in the treatment of hepatocellular carcinoma: Results of the PRECISION V study. Cardiovasc. Interv. Radiol. 2010, 33, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Prajapati, H.J.; Xing, M.; Spivey, J.R.; Hanish, S.I.; El-Rayes, B.F.; Kauh, J.S.; Chen, Z.; Kim, H.S. Survival, efficacy, and safety of small versus large doxorubicin drug-eluting beads TACE chemoembolization in patients with unresectable HCC. AJR. Am. J. Roentgenol. 2014, 203, W706–W714. [Google Scholar] [CrossRef]
- Padia, S.A.; Shivaram, G.; Bastawrous, S.; Bhargava, P.; Vo, N.J.; Vaidya, S.; Valji, K.; Harris, W.P.; Hippe, D.S.; Kogut, M.J. Safety and efficacy of drug-eluting bead chemoembolization for hepatocellular carcinoma: Comparison of small-versus medium-size particles. J. Vasc. Interv. Radiol. JVIR 2013, 24, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Liapi, E.; Vossen, J.A.; Buijs, M.; Ventura, V.P.; Georgiades, C.; Hong, K.; Kamel, I.; Torbenson, M.S.; Geschwind, J.F. Distribution of iron oxide-containing Embosphere particles after transcatheter arterial embolization in an animal model of liver cancer: Evaluation with MR imaging and implication for therapy. J. Vasc. Interv. Radiol. JVIR 2008, 19, 1490–1496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliberti, C.; Carandina, R.; Lonardi, S.; Dadduzio, V.; Vitale, A.; Gringeri, E.; Zanus, G.; Cillo, U. Transarterial Chemoembolization with Small Drug-Eluting Beads in Patients with Hepatocellular Carcinoma: Experience from a Cohort of 421 Patients at an Italian Center. J. Vasc. Interv. Radiol. JVIR 2017, 28, 1495–1502. [Google Scholar] [CrossRef] [PubMed]
- Deipolyi, A.R.; Oklu, R.; Al-Ansari, S.; Zhu, A.X.; Goyal, L.; Ganguli, S. Safety and efficacy of 70–150 μm and 100–300 μm drug-eluting bead transarterial chemoembolization for hepatocellular carcinoma. J. Vasc. Interv. Radiol. JVIR 2015, 26, 516–522. [Google Scholar] [CrossRef]
- Huo, Y.R.; Xiang, H.; Chan, M.V.; Chan, C. Survival, tumour response and safety of 70–150 μm versus 100–300 μm doxorubicin drug-eluting beads in transarterial chemoembolisation for hepatocellular carcinoma. J. Med. Imaging Radiat. Oncol. 2019, 63, 802–811. [Google Scholar] [CrossRef]
- Venkat, S.R.; Shah, M.B.; Barbery, K.J.; Checkver, A.; Abrahams, B.; Kang, K.; Narayanan, G. Comparison of 70–150 μm (M1) versus 100-300 μm doxorubicin drug-eluting beads in transarterial chemoembolization for hepatocellular carcinoma. J. Vasc. Interv. Radiol. 2015, 26, S68. [Google Scholar] [CrossRef]
- Heckman, A.; DeFoe, A.; Donovan, T.; Vargo, C. Does size matter? A comparison of 70–150 μm (M1) versus 100–300 μm drug-eluting beads in transarterial chemoembolization for hepatic malignancy. J. Vasc. Interv. Radiol. 2016, 27, S84–S85. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.; Yoon, J.; Kim, Y.; Oh, D.; Kim, S.J.; Ahn, J.; Suh, G.Y.; Nam, S.J.; Mitchell, S.A. Linguistic Validation of the US National Cancer Institute’s Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events in Korean. J. Glob. Oncol. 2019, 5, 1–10. [Google Scholar] [CrossRef]
- Lee, M.; Chung, J.W.; Lee, K.H.; Won, J.Y.; Chun, H.J.; Lee, H.C.; Kim, J.H.; Lee, I.J.; Hur, S.; Kim, H.C.; et al. Korean Multicenter Registry of Transcatheter Arterial Chemoembolization with Drug-Eluting Embolic Agents for Nodular Hepatocellular Carcinomas: Six-Month Outcome Analysis. J. Vasc. Interv. Radiol. JVIR 2017, 28, 502–512. [Google Scholar] [CrossRef]
- Aal, A.K.A.; Moawad, S.; Lune, P.V.; El Khudari, H.; Hanaoka, M.M.; Abouldahab, N.; Gunn, A.J.; White, J.; Shoreibah, M.; Li, Y.; et al. Survival Outcomes of Very Small Drug-Eluting Beads Used in Chemoembolization of Unresectable Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. JVIR 2019, 30, 1325–1334.e1322. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Ou, H.Y.; Yu, C.Y.; Huang, T.L.; Tsang, L.L.; Cheng, Y.F. Drug-eluting bead transarterial chemoembolization for hepatocellular carcinoma: Does size really matter? Diagn. Interv. Radiol. 2020, 26, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Richter, G.; Radeleff, B.; Stroszczynski, C.; Pereira, P.; Helmberger, T.; Barakat, M.; Huppert, P. Safety and Feasibility of Chemoembolization with Doxorubicin-Loaded Small Calibrated Microspheres in Patients with Hepatocellular Carcinoma: Results of the MIRACLE I Prospective Multicenter Study. Cardiovasc. Interv. Radiol. 2018, 41, 587–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vesselle, G.; Quirier-Leleu, C.; Velasco, S.; Charier, F.; Silvain, C.; Boucebci, S.; Ingrand, P.; Tasu, J.P. Predictive factors for complete response of chemoembolization with drug-eluting beads (DEB-TACE) for hepatocellular carcinoma. Eur. Radiol. 2016, 26, 1640–1648. [Google Scholar] [CrossRef] [PubMed]
- Odisio, B.C.; Ashton, A.; Yan, Y.; Wei, W.; Kaseb, A.; Wallace, M.J.; Vauthey, J.N.; Gupta, S.; Tam, A.L. Transarterial hepatic chemoembolization with 70-150 µm drug-eluting beads: Assessment of clinical safety and liver toxicity profile. J. Vasc. Interv. Radiol. JVIR 2015, 26, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Namur, J.; Wassef, M.; Millot, J.M.; Lewis, A.L.; Manfait, M.; Laurent, A. Drug-eluting beads for liver embolization: Concentration of doxorubicin in tissue and in beads in a pig model. J. Vasc. Interv. Radiol. JVIR 2010, 21, 259–267. [Google Scholar] [CrossRef]
- Malagari, K.; Iezzi, R.; Goldberg, S.N.; Bilbao, J.I.; Sami, A.; Akhan, O.; Giuliante, F.; Pompili, M.; Crocetti, L.; Valentini, V.; et al. The ten commandments of chemoembolization: Expert discussion and report from Mediterranean Interventional Oncology (MIOLive) congress 2017. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 372–381. [Google Scholar] [CrossRef]
- Chang, W.C.; Hsu, H.H.; Chiu, S.H.; Huang, W.Y.; Lo, C.H.; Lin, H.H.; Huang, P.C.; Shih, Y.L.; Wan, Y.L. Transcatheter Arterial Chemoembolization with Drug-Eluting Beads for the Treatment of Hepatocellular Carcinoma: Recommended Selection for Small-Caliber (<100 μm) Beads. J. Hepatocell. Carcinoma 2021, 8, 937–949. [Google Scholar] [CrossRef]
- Urbano, J.; Echevarria-Uraga, J.J.; Ciampi-Dopazo, J.J.; Sánchez-Corral, J.A.; Cobos Alonso, J.; Anton-Ladislao, A.; Peña-Baranda, B.; Nacarino-Mejias, V.; González-Costero, R.; Muñoz Ruiz-Canela, J.J.; et al. Multicentre prospective study of drug-eluting bead chemoembolisation safety using tightly calibrated small microspheres in non-resectable hepatocellular carcinoma. Eur. J. Radiol. 2020, 126, 108966. [Google Scholar] [CrossRef]
- Ballı, H.T.; Aikimbaev, K. Super-selective transarterial chemoembolization of hepatocellular carcinoma with doxorubicin-eluting beads sized 40–75 microns: Assessment of efficacy and safety. Diagn. Interv. Radiol. 2020, 26, 482–487. [Google Scholar] [CrossRef]
- Nouri, Y.M.; Kim, J.H.; Yoon, H.K.; Ko, H.K.; Shin, J.H.; Gwon, D.I. Update on Transarterial Chemoembolization with Drug-Eluting Microspheres for Hepatocellular Carcinoma. Korean J. Radiol. 2019, 20, 34–49. [Google Scholar] [CrossRef] [PubMed]
- Dreher, M.R.; Sharma, K.V.; Woods, D.L.; Reddy, G.; Tang, Y.; Pritchard, W.F.; Chiesa, O.A.; Karanian, J.W.; Esparza, J.A.; Donahue, D.; et al. Radiopaque drug-eluting beads for transcatheter embolotherapy: Experimental study of drug penetration and coverage in swine. J. Vasc. Interv. Radiol. JVIR 2012, 23, 257–264.e254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gholamrezanezhad, A.; Mirpour, S.; Geschwind, J.F.; Rao, P.; Loffroy, R.; Pellerin, O.; Liapi, E.A. Evaluation of 70-150-μm doxorubicin-eluting beads for transcatheter arterial chemoembolization in the rabbit liver VX2 tumour model. Eur. Radiol. 2016, 26, 3474–3482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, A.L.; Dreher, M.R.; O’Byrne, V.; Grey, D.; Caine, M.; Dunn, A.; Tang, Y.; Hall, B.; Fowers, K.D.; Johnson, C.G.; et al. DC BeadM1™: Towards an optimal transcatheter hepatic tumour therapy. J. Mater. Sci. Mater. Med. 2016, 27, 13. [Google Scholar] [CrossRef] [PubMed]
- Namur, J.; Citron, S.J.; Sellers, M.T.; Dupuis, M.H.; Wassef, M.; Manfait, M.; Laurent, A. Embolization of hepatocellular carcinoma with drug-eluting beads: Doxorubicin tissue concentration and distribution in patient liver explants. J. Hepatol. 2011, 55, 1332–1338. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | 70–150 μm | 100–300 μm | p Value |
|---|---|---|---|
| Numbers of patients | 40 | 32 | |
| Age | 65.8 ± 11.2 | 62.2 ± 9.5 | 0.153 |
| Male | 28 (70.0%) | 24 (75.0%) | 0.638 |
| Etiology | 0.850 | ||
| Hepatitis B | 23 (57.5%) | 20 (62.5%) | |
| Hepatitis C | 6 (15.0%) | 6 (18.8%) | |
| Alcohol | 5 (12.5%) | 3 (9.4%) | |
| Other | 6 (15.0%) | 6 (18.8%) | |
| Child–Pugh score | 0.436 | ||
| A | 33 (82.5%) | 24 (75.0%) | |
| B | 7 (17.5%) | 8 (25.0%) | |
| BCLC stage | 0.965 | ||
| 0 | 6 (15.0%) | 6 (18.8%) | |
| A | 28 (70.0%) | 21 (65.6%) | |
| B | 5 (12.5%) | 4 (12.5%) | |
| C | 1 (2.5%) | 1 (3.1%) | |
| Alfa-fetoprotein (AFP) | 0.289 | ||
| ≤20 ng/mL | 20 (50.0%) | 20 (62.5%) | |
| >20 ng/mL | 20 (50.0%) | 12 (37.5%) | |
| Aspartate aminotransferase (AST) | 0.267 | ||
| ≤45 U/L | 24 (60.0%) | 15 (46.9%) | |
| >45 U/L | 16 (40.0%) | 17 (53.1%) | |
| Alanine aminotransferase (ALT) | 0.173 | ||
| ≤40 U/L | 34 (85.0%) | 23 (71.9%) | |
| >40 U/L | 6 (15.0%) | 9 (28.1%) | |
| Albumin | 0.658 | ||
| ≤4 g/dL | 27 (67.5%) | 20 (62.5%) | |
| >4 g/dL | 13 (32.5%) | 12 (37.5%) | |
| Total bilirubin | 0.097 | ||
| ≤1.2 mg/dL | 31 (77.5%) | 19 (59.4%) | |
| >1.2 mg/dL | 9 (22.5%) | 13 (40.6%) | |
| Prothrombin time | 0.155 | ||
| ≤1.2 INR | 23 (57.5%) | 13 (40.6%) | |
| >1.2 INR | 17 (42.5%) | 19 (59.4%) |
| Characteristic | 70–150 μm | 100–300 μm | p Value |
|---|---|---|---|
| Numbers of patients | 40 | 32 | |
| Tumor distribution | 0.624 | ||
| Single | 26 (65.0%) | 19 (59.4%) | |
| Multiple | 14 (35.0%) | 13 (40.6%) | |
| Tumor location | 0.453 | ||
| Unilobar | 37 (92.5%) | 27 (84.4%) | |
| Bilobar | 3 (7.5%) | 5 (15.6%) | |
| Maximum tumor diameter (cm) | 3.57 ± 2.2 | 2.99 ± 1.47 | 0.185 |
| Sum of tumor diameters (cm) | 4.45 ± 3.26 | 3.91 ± 2.4 | 0.437 |
| Dose of doxorubicin (mg) | 28.8 ± 14.2 | 23.2 ± 12.5 | 0.083 |
| Selective catheterization | 0.123 | ||
| Segmental | 14 (35.0%) | 17 (53.1%) | |
| Subsegmental | 26 (65.0%) | 15 (46.9%) | |
| Additional bland embolization | 3 (7.5%) | 2 (6.3%) | 1.000 |
| Response | 70–150 μm (n = 40) | 100–300 μm (n = 32) | p Value |
|---|---|---|---|
| Complete response | 19 (47.5%) | 11 (34.4%) | 0.262 |
| Partial response | 15 (37.5%) | 15 (46.9%) | 0.423 |
| Objective response | 34 (85.0%) | 26 (81.3%) | 0.671 |
| Stable disease | 4 (10.0%) | 5 (15.6%) | 0.498 |
| Progressive disease | 2 (5.0%) | 1 (3.1%) | 1.000 |
| Characteristics | Complete Response n = 30 | No Complete Response n = 42 | p Value |
|---|---|---|---|
| Tumor distribution | 0.267 | ||
| Single | 21 (70%) | 24 (57.1%) | |
| Multiple | 9 (30%) | 18 (42.9%) | |
| Tumor location | 0.128 | ||
| Unilobar | 29 (96.7%) | 35 (83.3%) | |
| Bilobar | 1 (3.3%) | 7 (16.7%) | |
| Maximum tumor diameter (cm) | 2.68 ± 1.46 | 3.77 ± 2.09 | 0.011 |
| Sum of tumor diameters (cm) | 3.17 ± 1.79 | 4.96 ± 3.31 | 0.004 |
| AFP | 0.873 | ||
| ≤20 ng/mL | 17 (56.7%) | 23 (54.8%) | |
| >20 ng/mL | 13 (43.3%) | 19 (45.2%) | |
| Child–Pugh score | 0.185 | ||
| A | 26 (86.7%) | 31 (73.8%) | |
| B | 4 (13.3%) | 11 (26.2%) | |
| BCLC stage | 0.131 | ||
| 0 | 8 (26.7%) | 4 (9.5%) | |
| A | 20 (66.7%) | 29 (69%) | |
| B | 2 (6.7%) | 7 (16.7%) | |
| C | 0 (0%) | 2 (4.8%) | |
| Dose of doxorubicin (mg) | 24.2 ± 11.2 | 27.8 ± 15.1 | 0.251 |
| Selective catheterization | 0.658 | ||
| Segmental | 12 (40%) | 19 (45.2%) | |
| Subsegmental | 18 (60%) | 23 (54.8%) | |
| Additional bland embolization | 2 (6.7%) | 3 (7.1%) | 1 |
| Adverse Events | 70–150 μm (n = 40) | 100–300 μm (n = 32) | p Value |
|---|---|---|---|
| Abdominal pain | 17 (42.5%) | 14 (43.8%) | 0.981 |
| Grade 1/2/3 | 8/9/0 | 7/7/0 | |
| Vomiting | 3 (7.5%) | 2 (6.3%) | 1.000 |
| Grade 1/2/3 | 3/0/0 | 2/0/0 | |
| Fever | 21 (52.5%) | 11 (34.4%) | 0.124 |
| Grade 1/2/3 | 21/0/0 | 11/0/0 | |
| Prolonged hospitalization (≥7 days) | 4 (10.0%) | 1 (3.1%) | 0.373 |
| Increased Child–Pugh score after 1 month | 1 (2.5%) | 5 (15.6%) | 0.082 |
| A5→A6 | 1 | 2 | |
| B7→B9 | 0 | 2 | |
| B8→B9 | 0 | 1 |
| Variable | 70–150 μm (n = 40) | 100–300 μm (n = 32) | p Value |
|---|---|---|---|
| AST | 37 (14.5–74.5) | 32 (6–65) | 0.389 |
| ALT | 28 (3.5–55.5) | 16 (3–39) | 0.316 |
| Albumin | −0.3 (−0.6–−0.1) | −0.3 (−0.5–0.0) | 0.419 |
| Total bilirubin | 0.54 (0.28–0.69) | 0.56 (0.30–0.81) | 0.586 |
| Prothrombin time | 0.12 (0.06–0.21) | 0.10 (0.04–0.18) | 0.234 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, J.W.; Hong, H.P.; Kim, M.S.; Shin, B.S.; Kwon, H.-J.; Kim, B.I.; Sohn, W. Comparison of Clinical Efficacy and Safety between 70–150 µm and 100–300 µm Doxorubicin Drug-Eluting Bead Transarterial Chemoembolization for Hepatocellular Carcinoma. Life 2022, 12, 297. https://doi.org/10.3390/life12020297
Yi JW, Hong HP, Kim MS, Shin BS, Kwon H-J, Kim BI, Sohn W. Comparison of Clinical Efficacy and Safety between 70–150 µm and 100–300 µm Doxorubicin Drug-Eluting Bead Transarterial Chemoembolization for Hepatocellular Carcinoma. Life. 2022; 12(2):297. https://doi.org/10.3390/life12020297
Chicago/Turabian StyleYi, Jung Woo, Hyun Pyo Hong, Myung Sub Kim, Byung Seok Shin, Heon-Ju Kwon, Byung Ik Kim, and Won Sohn. 2022. "Comparison of Clinical Efficacy and Safety between 70–150 µm and 100–300 µm Doxorubicin Drug-Eluting Bead Transarterial Chemoembolization for Hepatocellular Carcinoma" Life 12, no. 2: 297. https://doi.org/10.3390/life12020297