
Pediatric Headache in Primary Care and Emergency Departments: Consensus with RAND/UCLA Method

 , ,
, , 
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Primary Care Pediatrician Evaluation
3.1.1. Recommendation 1 (Scenario 1)
- Age < 3 years
- Nocturnal or awakening headache
- Vomiting at night or in early morning
- Onset after physical effort, cough, Valsalva maneuver
- Cognitive decline or personality changes
- Altered state of consciousness
- History of seizures
- Recent onset (<2 months)
- Explosive onset
- Rapid worsening
- Fixed unilateral headache
- Association with projectile vomit, fever, general malaise
- Slow-down of weight for height development
- Change in headache pattern in children with known primary headache.
First and Second Survey Results Comparison
3.1.2. Recommendation 2 (Scenario 2)
- Macrocephaly in infants
- Meningeal signs
- Neurocutaneous markers
- Papilledema
- Abnormal eye movements, diplopia or nystagmus
- Asymmetry of strength or sensation
- Disturbance of gait or balance
- Asymmetry of osteotendinous reflexes
First and Second Survey Results Comparison
3.1.3. Recommendation 3 (Scenarios 3 and 4)
- Sudden onset of severe headache
- Headache exacerbated by lying down or coughing
- Focal neurological signs
- Dysautonomic signs (nausea, vomiting, paleness, sweating, etc.) preceding the headache
- Headache with temporal localization
- Precocious puberty
- Headache with occipital localization
- Chronic progressive headache
- A 14-year-old patient with a history of tension-type headache for two years with a sudden onset of severe headache
- A 15-year-old patient with a history of migraine and an episode partially responsive to paracetamol, associated with nausea and vomiting not present at night or in early morning
- An 8-year-old patient with headache and fever for two days with upper respiratory tract infection
- A 9-year-old patient with headache and high fever for four days with drowsiness and photophobia
- An 11-year-old patient with headache triggered or worsen by lying down or coughing
- A 14-year-old female patient with her third headache episode in five months preceded by aspecific visual disturbances of 15–30 min and strength deficit of the left arm
- A 17-year-old patient with known migraine, presenting with an episode lasting longer than 72 h and unresponsive to ibuprofen and paracetamol
- A 15-year-old patient with migraine without aura lasting more than 48 h and unresponsive to paracetamol
First and Second Survey Results Comparison
3.1.4. Recommendation 4 (Scenarios 5 and 6)
- Suggest a headache diary and refer the patient to a pediatric neurologist outpatient clinic;
- Suggest a headache diary and continue the follow-up, after OF evaluation;
- Prescribe an MRI with gadolinium;
- Prescribe a consultation to the pediatric neurologist;
- Prescribe a general ophthalmological evaluation; and
- Prescribe a cardiologist evaluation.
- Suggest ED referral; and
- Prescribe analgesic therapy and a pediatric neurology consultation.
First and Second Survey Results Comparison
3.2. Emergency Department Assessment
3.2.1. Recommendation 5 (Scenarios 1, 2, 3 and 4)
- Analgesic therapy and discharge in the case of reduction of symptoms
- An urgent pediatric neurologist consultation
- An urgent CT scan in the first instance
- Ocular fundus
- Urgent ophthalmologist examination
- Hospitalization for clinical observation and MRI examination
- Administration of analgesic therapy and discharge in the case of reduction of symptoms
- An urgent pediatric neurologist consultation
- An yourgent CT scan in the first instance
- Ophthalmologist consultation in the first instance
- Hospitalization for clinical observation and MRI examination
- Analgesic therapy and discharge in the case of reduction of symptoms
- An urgent pediatric neurologist consultation
- An urgent CT scan in the first instance
- Ophthalmologist examination in the first instance
- Admission for clinical observation and MRI examination
- Pain medication and clinical observation
- Performing OF
- Pain medication and discharge
- Pediatric neurologist elective consultation
- Pediatric neurologist urgent consultation
3.2.2. First and Second Survey Results Comparison
3.2.3. Recommendation 6 (Scenarios 5, 6, 7 and 8)
- Admission and observation
- Admission and observation in the case of fever or systemic symptoms
- Discharge with referral to pediatric neurologist clinic
- Discharge if symptoms subside during observation, with referral to pediatric neurology expert in the case of recurrence
- Pre-school age child
- Chronic-progressive course of headache
- Acute recurrent course of headache
- Association of weight loss
- Association of weight gain
- Familiarity with ischemic events during youth
- Association with upper respiratory tract infection/gastroenteritis
- Association with vomiting on awakening
- Negative first level imaging and persistence of pain
- Negative first level imaging and indication for further diagnostic investigation in urgency
- Indication for brain MRI in election for further investigation
- Patient diagnosed with migraine and with attack lasting for more than 72 h responding to iv therapy administered in the ED
- Seven-year-old patient with reported bilateral non-pulsating headache with negative neurological examination but pain intensity 6–7/10 VAS, partially responsive to analgesic therapy
- Seven-year-old patient with bilateral mild-to-moderate, non-pulsating headache and history of minor frontal head trauma 4 days before, in the absence of other neurological signs
- Headache in patient >5 years of age with negative neurological examination and failure to respond to acute therapy
- Headache in patient <5 years of age with negative neurological examination and failure to respond to acute drug therapy
- Headache at any age with positive neurological examination (focal signs, nystagmus, decreased visual acuity, lethargy, or irritability)
- Headache with positive physical examination for acute infectious disease
- Therapy-responsive headache associated with fever and upper airway infection, in patient >5 years of age
- Recent-onset headache, defined as being mild and responsive to therapy, in patients >5 years of age
- Recent-onset headache of high intensity
- Headache with persistent vomiting, even in the morning
- Headache with nocturnal awakenings
First and Second Survey Results Comparison
3.2.4. Recommendation 7 (Scenarios 9, 10 and 11)
- Performance of an urgent brain CT scan
- Admission and MRI examination
- Pediatric neurology expert assessment
- Clinical observation for 12–24 h
- Execution of blood tests to assess nutritional status and infections
- BMI calculation
- Blood pressure and ECG detection
- Perform urgent brain CT scan
- Perform deferred urgent MRI of the brain
- Perform cardiologic evaluation and echocardiogram
- Pediatric neurology expert assessment
- Perform OF and ophthalmologist consultation
- Perform blood tests, including coagulation
- Perform lumbar puncture
- Perform fundus oculi
- Perform brain CT scan
- If family history of migraine is present, consider deferred neuroimaging
First and Second Survey Results Comparison
3.3. Hospital Admission
3.3.1. Recommendation 8 (Scenarios 1 and 2)
- CT execution
- RMN execution
- Evaluation by the pediatric neurology expert
- 12–24 h of clinical observation
- Performing blood chemistry tests to assess nutritional status and ongoing infections
- BMI calculation
- BP and ECG detection
- Exclude encephalitis in the first instance by radiologic investigation
- Perform lumbar puncture
- Conduct child neuropsychiatric consultation to rule out psychoaffective/somatization disorders
- Perform viral serological investigations
- Observation to assess possible resolution within 24 h before continuing with the diagnostic procedure
- Electroencephalogram
First and Second Survey Results Comparison
3.3.2. Recommendation 9 (Scenarios 3 and 4)
- Perform urgent brain CT scan
- Perform deferred brain MRI
- Perform cerebrospinal fluid examination to exclude infectious processes
- Perform EEG to rule out occipital epilepsy
- If not associated with other symptoms, do not perform further investigations
- Ophthalmologist consultation
- When symptoms begin rapidly
- When there is mild confusion/sensory numbness that resolves after headache
- In the case of nausea and vomiting
- In the case of white/black, zigzag and/or central aura
- In the case of aura lasting <5 min
- In the case of sudden-onset colored circular aura
First and Second Survey Results Comparison
3.3.3. Recommendation 10 (Scenario 5)
- If posterior reversible encephalopathy (PRES) is suspected
- In the case of family history of coagulopathies or vascular malformations
- In the case of suspected idiopathic intracranial hypertension
- In the case of suspected familial hemiplegic migraine
- Routinely in the presence of any red flag
- In the case of post-traumatic headache
First and Second Survey Results Comparison
3.4. Acute Treatment
3.4.1. Recommendation 11 (Scenario 1)
- Paracetamol or ibuprofen
- Paracetamol, given its more rapid action as compared to ibuprofen
- Ibuprofen, given its more rapid action as compared to paracetamol
- Ibuprofen and triptans (almotriptan, eletriptan, rizatriptan, sumatriptan, zolmitriptan) in patients younger than 12 years old
First and Second Survey Results Comparison
3.4.2. Recommendation 12 (Scenario 2)
- The most commons symptoms (such as phonophobia, photophobia, nausea and vomiting) regress with analgesics
- The oral method of administration should be the favorite one for better efficacy
- In the case of phonophobia and photophobia, there is a satisfying response to ibuprofen, particularly if taken at the beginning of symptom onset
- In the case of nausea and vomiting, an antiemetic treatment should be associated
- In the case of nausea and vomiting, triptans grant a good response
- The treatment of nausea and vomiting should be avoided since they regress spontaneously and in a short time
First and Second Survey Results Comparison
3.4.3. Recommendation 13 (Scenario 3)
- All of the drugs of this class, approved in pediatrics, either oral or nasal, are equally effective
- Drugs given via nasal route should be preferred because they have shown a better relation between benefits and adverse effects in comparison to those given orally
- In the case of phono- or photophobia, there is no relevant improvement of symptoms
- They are used in combination with NSAID drugs
- They are used in combination with NSAID drugs in the case of an insufficient response to a single triptan
- In Italy, children older than 10 years are approved
- In Italy, children older than 12 years are approved
- It is possible to use the sumatriptan nasal spray, zolmitriptan nasal spray, and rizatriptan as tablets
- It is not possible to use them off-label in children younger than 12, even if under a specialist prescription
First and Second Survey Results Comparison
3.4.4. Recommendation 14 (Scenario 4)
- The use of ondansetron in pediatric age is indicated
- The use of dopamine agonists in pediatric age is indicated
- Their use is indicated in the case of acute headache of unknown diagnostic definition
First and Second Survey Results Comparison
3.4.5. Recommendation 15 (Scenario 5)
- Intravenous fluid hyperhydration should be started
- Metoclopramide can be efficient in treating both nausea and headache
- NSAID intravenous therapy should be attempted
- If the headache lasts more than 24 h, it is possible to use dihydroergotamine
- If the headache lasts more than 72 h, it is possible to use dihydroergotamine
- Perform a test dose (administer half dosage, adequate for weight and age);
- Perform a pregnancy test, when necessary;
- Treat with antiemetics 20 min before therapy (proclorperazine or metoclopramide for the first three doses, then, if still needed, it is suggested to use ondansetron, due to the high risk of extrapyramidal effects of dopamine antagonists).
First and Second Survey Results Comparison
3.5. Prophylaxis
3.5.1. Recommendation 16 (Scenario 1)
- Attacks are of high intensity with interference to quality of life, or they have a frequency of >4 days/month with 3–4 migraine attacks per month for at least 3 months
- Attacks respond only to acute polytherapy
- There is poor responsiveness to acute treatment with increased school absence or access to the ED
- In the case of medication-overuse headache
- Attacks of high intensity or that which follow one another with high frequency (more than four headache days per month and 3–4 migraine attacks per month for at least three months);
- Reduction of the patient’s quality of life;
First and Second Survey Results Comparison
3.5.2. Recommendation 17 (Scenario 2)
- Propranolol
- Amitriptyline alone
- Amitriptyline + cognitive-behavioral therapy
- Topiramate
- Valproate
- Triptans
- Among antiepileptics, topiramate at a dosage of 2–3 mg/Kg/day up to 100 mg/day was more effective than the placebo in reducing seizure frequency, and is the only drug indicated by the Food and Drug Administration for treatment of headache in adolescents aged 12–17 years [109,110]. However, it is no more effective than placebo in reducing headache attacks by at least 50% or in reducing disability [109,111]. Therefore, there is insufficient evidence for its efficacy in the prevention of pediatric headache. Its efficacy has been demonstrated in adults [112] but not in the pediatric population, for whom data in the literature are scarce. Nevertheless, topiramate may be indicated in male patients with certain forms of epilepsy associated with headache [113].
- Propranolol is a beta-blocker frequently used in pediatric populations, including for headache prevention, requiring adequate monitoring of blood pressure and heart rate [114,115]. Its dosage is 20–40 mg/day. The possible increase in blood concentrations of some triptans during prophylactic propranolol therapy is noteworthy [116]. In a systematic review, propranolol was found to have a better risk–benefit profile than topiramate, but there were no statistically significant differences in safety [117].
- Cinnarizine is an antihistamine and L-type calcium channel blocker. It is not recommended for co-administration with calcium antagonists in patients with current or previous depressive illness, arrhythmic heart disease, obesity, liver failure, pyramidal disorders and is contraindicated under 12 years of age. In the AHS guidelines, cinnarizine has been shown to be moderately effective compared to placebo in reducing the frequency and severity of migraine attacks, with low levels of evidence of efficacy in reducing migraine episodes by more than 50% compared to the placebo [28].
- Although some studies, such as the 2017 Childhood and Adolescent Migraine Prevention (CHAMP) Study [26,110], question the role of amitriptyline alone in headache prevention, the combination of amitriptyline (dosage: 1 mg/kg/day) and CBT has been shown to be effective in reducing the frequency of headache episodes and may be the first choice in patients whose headache causes a drastic reduction in quality of life or in adolescents with depression and anxiety disorders [118]. However, physicians should advise against the use of amitriptyline in patients with ongoing depression, as they are particularly at risk of developing suicidal ideation [28].
First and Second Survey Results Comparison
3.5.3. Recommendation 18 (Scenario 3)
- Topiramate
- Valproate
- Amitriptyline
- Propranolol
First and Second Survey Results Comparison
3.5.4. Recommendation 19 (Scenario 4)
- Start on low doses, gradually increasing the dosage over 3–4 weeks, even in the case of side effects if therapeutic benefit is achieved
- Start with low doses, gradually increasing the dosage over 3–4 weeks, discontinuing therapy in the case of side effects even if a therapeutic benefit is achievedTherapy should be continued for 12 weeks if a benefit is achieved
- Therapy should be continued for 6–12 months if there is a benefit.
First and Second Survey Results Comparison
3.5.5. Recommendation 20 (Scenario 5)
- A headache invalidity assessment should be carried out
- Take a careful personal and medication history
- Suggest the compilation of a headache diary
- Seek advice from the pediatric neurologist
- Recommend the use of opioids when pain is not controlled with NSAIDs/paracetamol
- Recommend use of nutraceuticals as needed
- Set up a prophylaxis with nutraceuticals lasting 2–3 months
First and Second Survey Results Comparison
3.5.6. Recommendation 21 (Scenario 6)
- Sleeping for a few hours in the afternoon
- Instructing children to go to bed and wake up at around the same time
- Regular mealtimes are recommended (usually three meals/day)
- It is recommended that children have a snack before going to bed
- Reduction of physical activity and sports is suggested
- Sleep hygiene: it is advisable to sleep an adequate number of hours per night and to maintain a routine sleep–wake rhythm. Insomnia, snoring, and frequent night waking can worsen the frequency of attacks.
- Physical activity: regular exercise in children has not been shown to be effective in preventing migraine, although studies in adult patients show the reverse. Physical activity of at least 30 min 3–5 times a week is recommended.
- Adequate water intake: increasing daily fluid intake has been shown to reduce the frequency and intensity of migraine attacks. Fluid intake varies according to age and level of physical activity, but includes 8–10 cups of non-caffeinated drinks per day.
- Regular food intake: fasting or skipping meals may act as a trigger for migraine. Children should have three meals/day.
- Identification of triggers: triggers should be identified as early as possible and avoided. Migraine occurs most often during school time, so the child’s school history should always be assessed in cases of frequent migraine in children. Caffeine and alcohol are known triggers for migraine and should be avoided. Some premonitory symptoms of migraine (fatigability, changes in mood, neck stiffness and increased sense of hunger) can often be misinterpreted as triggers [26,128].
First and Second Survey Results Comparison
3.5.7. Recommendation 22 (Scenarios 7 and 8)
- Recommend biofeedback
- Discontinue valproate or replace it with another prophylactic drug
- Recommend CBT
- Discourage competitive sporting activity
- Recommend reducing alcohol and caffeine intake
- Do not recommend oral contraception
- Discuss with the girl and her parents the teratogenicity of valproate, thus explaining the risk of possible pregnancy
- Change the drug used as preventive therapy
- Prescribe a gynecological examination and transvaginal ultrasound every six months
- Require periodic monitoring of blood valproic acid levels
- Behavioral-based therapy: according to Italian guidelines, this type of treatment can be considered as a first-choice approach or as a supplement to symptomatic and prophylactic drug treatment in pediatric patients, especially in the case of parental and/or young patient resistance to the use of drugs, presence of psychiatric comorbidity (anxiety disorders, mood disorders, social phobia, sleep disorders, etc.), presence of family issues, and ineffectiveness or inadequate response to previous treatments [57].
- Cognitive-behavioral therapy: CBT aims at teaching patients behavioral strategies to cope with pain, prevent migraine episodes through regular use of relaxation exercises, and assist patients with migraine-associated disabilities and comorbidities such as anxiety and depression. Its efficacy has been demonstrated especially in combination with amitriptyline in reducing headache-related disability, and the frequency of attacks by at least 50 percent of actual headache days [119]. According to the 2003 Italian guidelines, this type of treatment can be considered as a first choice in pediatric patients in whom headache causes significant disability or decreases their quality of life [24]. However, CBT alone may also be considered an effective first-choice therapy in certain patients, on pediatric neurologist advice [28]. Often, biofeedback (BFB) is included into CBT during the teaching of relaxation exercises, thus allowing patients to see the physiological changes that occur after relaxation exercises.
- BFB: This is a technique through which a subject receives information and can about its biological state and can change it. BFB thus creates an external link through which the subject can keep one or more physiological functions under control. BFB uses an electronic instrument to monitor these functions and sends information to the patient about its progress in the form of an acoustic or light signal. In this way, the patient can become aware of the progresses on these functions, which are usually considered independent of willpower, and can therefore learn to control it. According to some studays, patients undergoing BFB have experienced an improvement in migraine frequency and a decrease in attack duration and intensity [129]. Although this technique appears to be effective, it is not widely used due to several limitations: high cost, low availability, few dedicated staff, and low compliance of young patients.
First and Second Survey Results Comparison
3.6. Follow-Up
3.6.1. Recommendation 23 (Scenarios 1 and 2)
- Tell the patient to inform them any time a new migraine-related symptom appears
- Refer the patient to a child neurologist if she is taking topiramate or valproate as a prophylactic treatment to evaluate changes in therapy or to assess the teratogenic risk
- Recommend a gynecological evaluation if the patient wishes to start contraceptive oral therapy
- Periodically evaluate the patient’s health, especially if the migraine has a negative impact on mental health
- Persistence of headache symptoms during the first month of treatment
- Onset of anorexia
- Asthma exacerbation
First and Second Survey Results Comparison
3.6.2. Recommendation 24 (Scenario 3)
- Is indicated in every patient suffering from headache
- Is indicated in the case of metabolic syndrome
- Is indicated in the case of high BMI
- Is indicated when headache is associated with neurovegetative symptoms
- Must be associated with heart-rate monitoring
- Is mandatory in children <6 years old with headache
- Is indicated in patients taking propranolol
- Is indicated in patients on propranolol, if presenting with syncope
- Is indicated in patients taking amitriptyline
First and Second Survey Results Comparison
3.6.3. Recommendation 25 (Scenario 4)
- No more than 14 times/month for oral analgesics
- No more than 2 times/week for oral analgesics
- No more than 8–9 times/month for triptans
- No more than once a week for triptans
- Analgesics: no more than 14 times/month;
- Triptans, ergotamine, opioids: no more than nine times/month (opioids are cited with regard to ICHD-3, but their use is not recommended);
- Combinations of drugs: for less than a three-month period.
First and Second Survey Results Comparison
4. Discussion
4.1. Primary Care Pediatrician Evaluation
4.2. Emergency Department Evaluation
4.3. Hospital Admission
4.4. Acute Treatment
4.5. Prophylaxis
4.6. Follow-Up
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dao, J.M.; Qubty, W. Headache Diagnosis in Children and Adolescents. Curr. Pain Headache Rep. 2018, 22, 17. [Google Scholar] [CrossRef]
- Abu-Arafeh, I.; Razak, S.; Sivaraman, B.; Graham, C. Prevalence of headache and migraine in children and adolescents: A systematic review of population-based studies. Dev. Med. Child Neurol. 2010, 52, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [CrossRef] [PubMed]
- Conicella, E.; Raucci, U.; Vanacore, N.; Vigevano, F.; Reale, A.; Pirozzi, N.; Valeriani, M. The child with headache in a pediatric emergency department. Headache 2008, 48, 1005–1011. [Google Scholar] [CrossRef]
- Kan, L.; Nagelberg, J.; Maytal, J. Headaches in a pediatric emergency department: Etiology, imaging, and treatment. Headache 2000, 40, 25–29. [Google Scholar] [CrossRef]
- León-Díaz, A.; González-Rabelino, G.; Alonso-Cerviño, M. Análisis etiológico de las cefaleas desde un servicio de emergencia pediátrica [Analysis of the aetiologies of headaches in a pediatric emergency service]. Rev. Neurol. 2004, 39, 217–221. [Google Scholar]
- Lateef, T.M.; Merikangas, K.R.; He, J.; Kalaydjian, A.; Khoromi, S.; Knight, E.; Nelson, K.B. Headache in a national sample of American children: Prevalence and comorbidity. J. Child Neurol. 2009, 24, 536–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D. The RAND/UCLA Adeguateness Method User’s Manual; The RAND Corporation: Santa Monica, CA, USA, 2001. [Google Scholar]
- Hicks, N.R. Some observations on attempts to measure appropriateness of care. BMJ 1994, 309, 730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphrey-Murto, S.; Varpio, L.; Gonsalves, C.; Wood, T.J. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med. Teach. 2017, 39, 14–19. [Google Scholar] [CrossRef]
- Ozge, A.; Termine, C.; Antonaci, F.; Natriashvili, S.; Guidetti, V.; Wöber-Bingöl, C. Overview of diagnosis and management of pediatric headache. Part I: Diagnosis. J. Headache Pain 2011, 12, 13–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toldo, I.; Sartori, S.; De Carlo, D.; Battistella, P.A. Headache in pediatric emergency department. Gior. Neuropsich. Età Evol. 2012, 32, 17–22. [Google Scholar]
- Lewis, D.W.; Ashwal, S.; Dahl, G.; Dorbad, D.; Hirtz, D.; Prensky, A.; Jarjour, I.; Quality Standards Subcommittee of the American Academy of Neurology; Practice Committee of the Child Neurology Society. Practice parameter: Evaluation of children and adolescents with recurrent headaches: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2002, 59, 490–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, M.; Strelzik, J.; Langdon, R.; DiSabella, M. Pediatric headache: Overview. Curr. Opin Pediatr. 2018, 30, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Blume, H.K. Pediatric headache: A review. Pediatr. Rev. 2012, 33, 562–576. [Google Scholar] [CrossRef]
- Barritt, A.; Miller, S.; Davagnanam, I.; Matharu, M. Rapid diagnosis vital in thunderclap headache. Practitioner 2016, 260, 23–28. [Google Scholar]
- Dilli, E. Thunderclap headache. Curr. Neurol. Neurosci. Rep. 2014, 14, 437. [Google Scholar] [CrossRef]
- Raucci, U.; Della Vecchia, N.; Ossella, C.; Paolino, M.C.; Villa, M.P.; Reale, A.; Parisi, P. Management of Childhood Headache in the Emergency Department. Review of the Literature. Front. Neurol. 2019, 10, 886. [Google Scholar] [CrossRef]
- Do, T.P.; Remmers, A.; Schytz, H.W.; Schankin, C.; Nelson, S.E.; Obermann, M.; Hansen, J.M.; Sinclair, A.J.; Gantenbein, A.R.; Schoonman, G.G. Red and orange flags for secondary headaches in clinical practice: SNNOOP10 list. Neurology 2019, 92, 134–144. [Google Scholar] [CrossRef]
- Parisi, P.; Belcastro, V.; Verrotti, A.; Striano, P.; Kasteleijn-Nolst Trenitè, D.G.A. “Ictal epileptic headache” and the revised International Headache Classification (ICHD-3) published in Cephalalgia 2018, vol. 38(1) 1-211: Not just a matter of definition! Epilepsy Behav. 2018, 87, 243–245. [Google Scholar] [CrossRef]
- Yayıcı Köken, Ö.; Danış, A.; Yüksel, D.; Aksoy, A.; Öztoprak, Ü.; Aksoy, E. Pediatric headache: Are the red flags misleading or prognostic? Brain Dev. 2021, 43, 372–379. [Google Scholar] [CrossRef]
- Wilne, S.; Collier, J.; Kennedy, C.; Koller, K.; Grundy, R.; Walker, D. Presentation of childhood CNS tumours: A systematic review and meta-analysis. Lancet Oncol. 2007, 8, 685–695. [Google Scholar] [CrossRef]
- Papetti, L.; Capuano, A.; Tarantino, S.; Vigevano, F.; Valeriani, M. Headache as an emergency in children and adolescents. Curr. Pain Headache Rep. 2015, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.; Couto-Silva, A.C.; Adan, L.; Trivin, C.; Sainte-Rose, C.; Zerah, M.; Valteau-Couanet, D.; Doz, F.; Chalumeau, M.; Brauner, R. Hypothalamic-pituitary lesions in pediatric patients: Endocrine symptoms often precede neuro-ophthalmic presenting symptoms. J. Pediatr. 2012, 161, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Tavoni, M.A.; Cardinali, C.; Fabiani, E.; Cardoni, G. La cefalea in età evolutiva: Approccio al Pronto Soccorso. Rivista di Emergenza e Urgenza Pediatrica (SIMEUP). Modulo Cefalee Età Evolutiva 2009, 2, 36–44. [Google Scholar]
- Segev-Becker, A.; Har-Gil, M.; Fainmesser, P.; Assia, E.L.; Watemberg, N. Yield and clinical efficacy of funduscopic examinations performed in the pediatric emergency room. Eur. J. Pediatr. 2014, 173, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, A.A. Pediatric and Adolescent Headache. Continuum (Minneap Minn). Headache 2018, 24, 1108–1136. [Google Scholar]
- Oskoui, M.; Pringsheim, T.; Holler-Managan, Y.; Potrebic, S.; Billinghurst, L.; Gloss, D.; Hershey, A.D.; Licking, N.; Sowell, M.; Victorio, M.C.; et al. Practice guideline update summary: Acute treatment of migraine in children and adolescents: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 2019, 93, 487–499. [Google Scholar] [CrossRef] [Green Version]
- Mazzotta, G.; Gallai, V.; Sarchielli, P.; Prudenzano, M.P.; Puca, F.M.; Moscato, D.; Ad Hoc Committe. Linee Guida Per La Diagnosi E La Terapia Della Cefalea Giovanile. Available online: https://www.sinpia.eu/wp-content/uploads/2019/02/2002_2.pdf (accessed on 19 September 2021).
- Kröner-Herwig, B.; Heinrich, M.; Morris, L. Headache in German children and adolescents: A population-based epidemiological study. Cephalalgia 2007, 27, 519–527. [Google Scholar] [CrossRef]
- Eliasen, M.; Jørgensen, T.; Schröder, A.; Dantoft, T.M.; Fink, P.; Poulsen, C.H.; Johansen, N.B.; Eplov, L.F.; Skovbjerg, S.; Kreiner, S. Somatic symptom profiles in the general population: A latent class analysis in a Danish population-based health survey. Clin. Epidemiol. 2017, 9, 421–433. [Google Scholar] [CrossRef] [Green Version]
- Toldo, I.; Pinello, L.; Suppiej, A.; Ermani, M.; Cermakova, I.; Zanin, E.; Sartori, S.; Battistella, P.A. Nonorganic (psychogenic) visual loss in children: A retrospective series. J. Neuroophthalmol. 2010, 30, 26–30. [Google Scholar] [CrossRef]
- Regier, D.A.; Kuhl, E.A.; Kupfer, D.J. The DSM-5: Classification and criteria changes. World Psychiatry 2013, 12, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Munday, S.; Rao, A. Always on my mind: Headache in children. Emerg. Med. Australas. 2016, 28, 376–378. [Google Scholar] [CrossRef]
- Tepecik Böyükbaş, İ.; Çıtak Kurt, A.N.; Tural Hesapçıoğlu, S.; Uğurlu, M. Relationship between headache and Internet addiction in children. Turk. J. Med. Sci. 2019, 49, 1292–1297. [Google Scholar] [CrossRef]
- Özge, A.; Faedda, N.; Abu-Arafeh, I.; Gelfand, A.A.; Goadsby, P.J.; Cuvellier, J.C.; Valeriani, M.; Sergeev, A.; Barlow, K.; Uludüz, D.; et al. Experts’ opinion about the primary headache diagnostic criteria of the ICHD-3rd edition beta in children and adolescents. J. Headache Pain 2017, 18, 109. [Google Scholar] [CrossRef] [Green Version]
- Winder, M.M.; Marietta, J.; Kerr, L.M.; Puchalski, M.D.; Zhang, C.; Ware, A.L.; Cowley, C.G. Reducing Unnecessary Diagnostic Testing in Pediatric Syncope: A Quality Improvement Initiative. Pediatr. Cardiol. 2021, 42, 942–950. [Google Scholar] [CrossRef] [PubMed]
- Millet, A.; Evain, J.N.; Desrumaux, A.; Francony, G.; Bouzat, P.; Mortamet, G. Clinical applications of transcranial Doppler in non-trauma critically ill children: A scoping review. Child’s Nerv. Syst. 2021, 37, 2759–2768. [Google Scholar] [CrossRef] [PubMed]
- Roser, T.; Bonfert, M.; Ebinger, F.; Blankenburg, M.; Ertl-Wagner, B.; Heinen, F. Primary versus secondary headache in children: A frequent diagnostic challenge in clinical routine. Neuropediatrics 2013, 44, 34–39. [Google Scholar] [PubMed]
- Massano, D.; Julliand, S.; Kanagarajah, L.; Gautier, M.; Vizeneux, A.; Elmaleh, M.; Alison, M.; Lejay, E.; Romanello, S.; Teisseyre, L.; et al. Headache with focal neurologic signs in children at the emergency department. J. Pediatr. 2014, 165, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, H.J.; Huang, J.L.; Hsia, S.H.; Lin, J.J.; Huang, I.A.; Wu, C.T. Headache in the pediatric emergency service: A medical center experience. Pediatr. Neonatol. 2014, 55, 208–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, R.; Versace, A.; Lauria, B.; Grasso, G.; Castagno, E.; Ricceri, F.; Pagliero, R.; Urbino, A.F. Headache in the pediatric emergency department: A 5-year retrospective study. Cephalalgia 2018, 38, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.J.; Zauel, D.W.; Schlaeger, T.F.; Meyer, S.M. Bilateral juxtapapillary subretinal neovascularization and pseudopapilledema in a three-year-old child. J. Pediatr. Ophthalmol. Strabismus. 1978, 15, 296–299. [Google Scholar] [CrossRef]
- Chang, M.Y.; Pineles, S.L. Optic disk drusen in children. Surv. Ophthalmol. 2016, 61, 745–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abegão Pinto, L.; Vandewalle, E.; Marques-Neves, C.; Stalmans, I. Visual field loss in optic disc drusen patients correlates with central retinal artery blood velocity patterns. Acta Ophthalmol. 2014, 92, e286–e291. [Google Scholar] [CrossRef]
- Asensio-Sánchez, V.M.; Trujillo-Guzmán, L. SD-OCT to distinguish papilledema from pseudopapilledema. Arch. Soc. Esp. Oftalmol. 2015, 90, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Albakr, A.; Hamad, M.H.; Alwadei, A.H.; Bashiri, F.A.; Hassan, H.H.; Idris, H.; Hassan, S.; Muayqil, T.; Altweijri, I.; Salih, M.A. Idiopathic intracranial hypertension in children: Diagnostic and management approach. Sudan J. Pediatr. 2016, 16, 67–76. [Google Scholar]
- Gaier, E.D.; Heidary, G. Pediatric Idiopathic Intracranial Hypertension. Semin. Neurol. 2019, 39, 704–710. [Google Scholar] [CrossRef]
- Mollan, S.P.; Mitchell, J.L.; Sinclair, A.J. Tip of the iceberg in idiopathic intracranial hypertension. Pract. Neurol. 2019, 19, 178–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Digre, K.B.; Nakamoto, B.K.; Warner, J.E.; Langeberg, W.J.; Baggaley, S.K.; Katz, B.J. A comparison of idiopathic intracranial hypertension with and without papilledema. Headache 2009, 49, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Faz, G.; Butler, I.J.; Koenig, M.K. Incidence of papilledema and obesity in children diagnosed with idiopathic “benign” intracranial hypertension: Case series and review. J. Child Neurol. 2010, 25, 1389–1392. [Google Scholar] [CrossRef]
- Blanco-Baudrit, D.A.; Blanco-Baudrit, L.F.; Yock-Corrales, A. Pediatric headache in the emergency department. Pediatr. Neonatal. Nurs. Open J. 2016, 2, 99–103. [Google Scholar] [CrossRef]
- Bonadio, W. Pediatric lumbar puncture and cerebrospinal fluid analysis. J. Emerg. Med. 2014, 46, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, M.; Baglioni, V. Management of Neurological Emergencies in Children: An Updated Overview. Neuropediatrics 2021, 52, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Lateef, T.M.; Grewal, M.; McClintock, W.; Chamberlain, J.; Kaulas, H.; Nelson, K.B. Headache in young children in the emergency department: Use of computed tomography. Pediatrics 2009, 124, e12–e17. [Google Scholar] [CrossRef] [Green Version]
- Tsze, D.S.; Ochs, J.B.; Gonzalez, A.E.; Dayan, P.S. Red flag findings in children with headaches: Prevalence and association with emergency department neuroimaging. Cephalalgia 2019, 39, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Schytz, H.W.; Amin, F.M.; Jensen, R.H.; Carlsen, L.; Maarbjerg, S.; Lund, N.; Aegidius, K.; Thomsen, L.L.; Bach, F.W.; Beier, D.; et al. Reference programme: Diagnosis and treatment of headache disorders and facial pain. Danish Headache Society, 3rd edition. J. Headache Pain 2021, 22, 22. [Google Scholar] [CrossRef] [PubMed]
- Sarchielli, P.; Granella, F.; Prudenzano, M.P.; Pini, L.A.; Guidetti, V.; Bono, G.; Pinessi, L.; Alessandri, M.; Antonaci, F.; Fanciullacci, M.; et al. Italian guidelines for primary headaches: 2012 revised version. J. Headache Pain 2012, 13, S31–S70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carville, S.; Padhi, S.; Reason, T.; Underwood, M. Guideline Development Group. Diagnosis and management of headaches in young people and adults: Summary of NICE guidance. BMJ 2012, 345, e5765. [Google Scholar] [CrossRef] [PubMed]
- Parisi, P.; Vanacore, N.; Belcastro, V.; Carotenuto, M.; Del Giudice, E.; Mariani, R.; Papetti, L.; Pavone, P.; Savasta, S.; Striano, P.; et al. “Pediatric Headache Commission” of Società Italiana di Neurologia Pediatrica (SINP). Clinical guidelines in pediatric headache: Evaluation of quality using the AGREE II instrument. J. Headache Pain 2014, 15, 57. [Google Scholar] [CrossRef] [Green Version]
- Goldman, R.D.; Cheng, S.; Cochrane, D.D. Improving diagnosis of pediatric central nervous system tumours: Aiming for early detection. CMAJ 2017, 189, E459–E463. [Google Scholar] [CrossRef] [Green Version]
- Braun, K.P.; Rafay, M.F.; Uiterwaal, C.S.; Pontigon, A.M.; DeVeber, G. Mode of onset predicts etiological diagnosis of arterial ischemic stroke in children. Stroke 2007, 38, 298–302. [Google Scholar] [CrossRef]
- Ferraù, L.; Giammello, F.; Fazio, M.C.; Grillo, F.; Vinci, S.L.; Toscano, A.; Musolino, R.F.; Dell’Aera, C. Management of Teenage Stroke in the Acute Setting: Two Case Reports. SN Compr. Clin. Med. 2021, 3, 2660–2664. [Google Scholar] [CrossRef]
- Atkinson, D.S., Jr. Computed tomography of pediatric stroke. Semin. Ultrasound CT MR 2006, 27, 207–218. [Google Scholar] [CrossRef]
- Gadian, D.G.; Calamante, F.; Kirkham, F.J.; Bynevelt, M.; Johnson, C.L.; Porter, D.A.; Chong, W.K.; Prengler, M.; Connelly, A. Diffusion and Perfusion Magnetic Resonace Imaging in childhood stroke. J. Child Neurol. 2000, 15, 279–283. [Google Scholar] [CrossRef]
- Alfonzo, M.J.; Bechtel, K.; Babineau, S. Management of headache in the pediatric emergency department. Pediatr. Emerg. Med. Pract. 2013, 10, 1–25. [Google Scholar]
- Fitch, M.T.; van de Beek, D. Emergency diagnosis and treatment of adult meningitis. Lancet Infect. Dis. 2007, 7, 191–200. [Google Scholar] [CrossRef]
- Expert Panel on Pediatric Imaging; Hayes, L.L.; Palasis, S.; Bartel, T.B.; Booth, T.N.; Iyer, R.S.; Jones, J.Y.; Kadom, N.; Milla, S.S.; Myseros, J.S.; et al. ACR Appropriateness Criteria® Headache-Child. J. Am. Coll. Radiol. 2018, 15, S78–S90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nievelstein, R.A.; van Dam, I.M.; van der Molen, A.J. Multidetector CT in children: Current concepts and dose reduction strategies. Pediatr. Radiol. 2010, 40, 1324–1344. [Google Scholar] [CrossRef] [Green Version]
- Odle, T.G. Dose Reduction Techniques in Pediatric Computed Tomography. Radiol. Technol. 2019, 91, 161CT–180CT. [Google Scholar]
- Kirchmann, M.; Thomsen, L.L.; Olesen, J. Basilar-type migraine: Clinical, epidemiologic, and genetic features. Neurology 2006, 66, 880–886. [Google Scholar] [CrossRef] [PubMed]
- Hung, R.M.; MacGregor, D.L. Management of pediatric migraine: Current concepts and controversies. Indian J. Pediatr. 2008, 75, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.K.; Shinnar, S. Nonconvulsive status epilepticus. Emerg. Med. Clin. N. Am. 2011, 29, 65–72. [Google Scholar] [CrossRef]
- Ferrari-Marinho, T.; Macedo, E.F.; Costa Neves, R.S.; Costa, L.V.; Tudesco, I.S.; Carvalho, K.C.; Carrete, H.; Caboclo, L.O.; Yacubian, E.M.; Hamad, A.P. Gastaut type idiopathic childhood occipital epilepsy. Epileptic Disord. 2013, 15, 80–83. [Google Scholar] [CrossRef]
- Parisi, P.; Villa, M.P.; Pelliccia, A.; Rollo, V.C.; Chiarelli, F.; Verrotti, A. Panayiotopoulos syndrome: Diagnosis and management. Neurol. Sci. 2007, 28, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Adame, N.; Hedlund, G.; Byington, C.L. Sinogenic intracranial empyema in children. Pediatrics 2005, 116, e461–e467. [Google Scholar] [CrossRef] [Green Version]
- Alehan, F.K. Value of neuroimaging in the evaluation of neurologically normal children with recurrent headache. J. Child Neurol. 2002, 17, 807–809. [Google Scholar] [CrossRef] [PubMed]
- McDonald, R.J.; McDonald, J.S.; Kallmes, D.F.; Jentoft, M.E.; Murray, D.L.; Thielen, K.R.; Williamson, E.E.; Eckel, L.J. Intracranial gadolinium deposition after contrastenhanced MR imaging. Radiology 2015, 275, 772–782. [Google Scholar] [CrossRef] [Green Version]
- McDonald, J.S.; McDonald, R.J.; Jentoft, M.E.; Paolini, M.A.; Murray, D.L.; Kallmes, D.F.; Eckel, L.J. Intracranial gadolinium deposition following gadodiamide-enhanced magnetic resonance imaging in pediatric patients: A case-control study. JAMA Pediatr. 2017, 171, 705–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loder, E.; Weizenbaum, E.; Frishberg, B.; Silberstein, S. American Headache Society Choosing Wisely Task Force. Choosing wisely in headache medicine: The American Headache Society’s list of five things physicians and patients should question. Headache 2013, 53, 1651–1659. [Google Scholar] [CrossRef]
- McDonald, R.J.; McDonald, J.S.; Kallmes, D.F.; Jentoft, M.E.; Paolini, M.A.; Murray, D.L.; Williamson, E.E.; Eckel, L.J. Gadolinium deposition in human brain tissues after contrast-enhanced MR imaging in adult patients without intracranial abnormalities. Radiology 2017, 285, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Radbruch, A.; Haase, R.; Kieslich, P.J.; Weberling, L.D.; Kickingereder, P.; Wick, W.; Schlemmer, H.P.; Bendszus, M. No signal intensity increase in the dentate nucleus on unenhanced T1-weighted MR images after more than 20 serial injections of macrocyclic gadolinium-based contrast agents. Radiology 2017, 282, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Kacperski, J.; Kabbouche, M.A.; O’Brien, H.L.; Weberding, J.L. The optimal management of headaches in children and adolescents. Ther. Adv. Neurol. Disord. 2016, 9, 53–68. [Google Scholar] [CrossRef] [Green Version]
- Hämäläinen, M.L.; Hoppu, K.; Valkeila, E.; Santavuori, P. Ibuprofen or acetaminophen for the acute treatment of migraine in children: A double-blind, randomized, placebo-controlled, crossover study. Neurology 1997, 48, 103–107. [Google Scholar] [CrossRef]
- Faber, A.J.; Lagman-Bartolome, A.M.; Rajapakse, T. Drugs for the acute treatment of migraine in children and adolescents. Pediatr. Child Health 2017, 22, 454–458. [Google Scholar] [CrossRef]
- Richer, L.; Billinghurst, L.; Linsdell, M.A.; Russell, K.; Vandermeer, B.; Crumley, E.T.; Durec, T.; Klassen, T.P.; Hartling, L. Drugs for the acute treatment of migraine in children and adolescents. Cochrane Database Syst. Rev. 2016, 4, CD005220. [Google Scholar]
- Pavithra, V.; Mishra, D.; Behera, S.; Juneja, M. Paracetamol versus Ibuprofen for the Acute Treatment of Migraine Headache in Children: A Blinded Randomized Controlled Trial. Indian J. Pediatr. 2020, 87, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Hershey, A.D. Current approaches to the diagnosis and management of pediatric migraine. Lancet Neurol. 2010, 9, 190–204. [Google Scholar] [CrossRef]
- Winner, P.; Rothner, A.D.; Wooten, J.D.; Webster, C.; Ames, M. Sumatriptan nasal spray in adolescent migraineurs: A randomized, double-blind, placebo-controlled, acute study. Headache 2006, 46, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Winner, P.; Rothner, A.D.; Saper, J.; Nett, R.; Asgharnejad, M.; Laurenza, A.; Austin, R.; Peykamian, M. A randomized, double-blind, placebo-controlled study of sumatriptan nasal spray in the treatment of acute migraine in adolescents. Pediatrics 2000, 106, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Fraser, I.P.; Han, L.; Han, T.H.; Li, C.C.; Hreniuk, D.; Stoch, S.A.; Wagner, J.A.; Linder, S.; Winner, P. Pharmacokinetics and tolerability of rizatriptan in pediatric migraineurs in a randomized study. Headache 2012, 52, 625–635. [Google Scholar] [CrossRef]
- Linder, S.L.; Mathew, N.T.; Cady, R.K.; Finlayson, G.; Ishkanian, G.; Lewis, D.W. Efficacy and tolerability of almotriptan in adolescents: A randomized, double-blind, placebo-controlled trial. Headache 2008, 48, 1326–1336. [Google Scholar] [CrossRef] [PubMed]
- Whitehouse, W.P.; Agrawal, S. Management of children and young people with headache. Arch. Dis. Child Educ. Pract. Ed. 2017, 102, 58–65. [Google Scholar] [CrossRef] [Green Version]
- Romano, C.; Dipasquale, V.; Scarpignato, C. Antiemetic Drug Use in Children: What the Clinician Needs to Know. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 466–471. [Google Scholar] [CrossRef]
- Gui, S.; Patel, N.; Issenman, R.; Kam, A.J. Acute Management of Pediatric Cyclic Vomiting Syndrome: A Systematic Review. J. Pediatr. 2019, 214, 158–164.e4. [Google Scholar] [CrossRef] [PubMed]
- Talai, A.; Heilbrunn, B. Ondansetron for Acute Migraine in the Pediatric Emergency Department. Pediatr. Neurol. 2020, 103, 52–56. [Google Scholar] [CrossRef]
- Brousseau, D.C.; Duffy, S.J.; Anderson, A.C.; Linakis, J.G. Treatment of pediatric migraine headaches: A randomized, double-blind trial of prochlorperazine versus ketorolac. Ann. Emerg. Med. 2004, 43, 256–262. [Google Scholar] [CrossRef]
- Sheridan, D.C.; Laurie, A.; Pacheco, S.; Fu, R.; Hansen, M.L.; Ma, O.J.; Meckler, G.D. Relative Effectiveness of Dopamine Antagonists for Pediatric Migraine in the Emergency Department. Pediatr. Emerg. Care 2018, 34, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Menniti-Ippolito, F.; Traversa, G.; Da Cas, R.; Rossi, R.; Renna, S.; Barabino, P.; Saggiomo, G.; Vetrano, F.; Sagliocca, L. Extrapyramidal reactions in children treated with metoclopramide. Ital. J. Pediatr. 2004, 30, 49–52. [Google Scholar]
- Slater, S.K.; Powers, S.W.; O’Brien, H.L. Migraine in children: Presentation, disability and response to treatment. Curr. Opin. Pediatr. 2018, 30, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Linder, S.L. Treatment of childhood headache with dihydroergotamine mesylate. Headache 1994, 34, 578–580. [Google Scholar] [CrossRef]
- Kabbouche, M.A.; Powers, S.W.; Segers, A.; LeCates, S.; Manning, P.; Biederman, S.; Vaughan, P.; Burdine, D.; Hershey, A.D. Inpatient treatment of status migraine with dihydroergotamine in children and adolescents. Headache 2009, 49, 106–109. [Google Scholar] [CrossRef]
- Hämäläinen, M.L.; Hoppu, K.; Santavuori, P.R. Oral dihydroergotamine for therapy-resistant migraine attacks in children. Pediatr. Neurol. 1997, 16, 114–117. [Google Scholar] [CrossRef]
- Hershey, A.D.; Powers, S.W.; Vockell, A.L.; LeCates, S.; Kabbouche, M.A.; Maynard, M.K. PedMIDAS: Development of a questionnaire to assess disability of migraines in children. Neurology 2001, 57, 2034–2039. [Google Scholar] [CrossRef] [PubMed]
- El-Chammas, K.; Keyes, J.; Thompson, N.; Vijayakumar, J.; Becher, D.; Jackson, J.L. Pharmacologic treatment of pediatric headaches: A meta-analysis. JAMA Pediatr. 2013, 167, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Newton, R.W. Childhood headache. Arch. Dis. Child Educ. Pract. Ed. 2008, 93, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.J.; Jensen, R.; Katsarava, Z.; Linde, M.; MacGregor, E.A.; Osipova, V.; Paemeleire, K.; Olesen, J.; Peters, M.; Martelletti, P. Aids to management of headache disorders in primary care (2nd edition): On behalf of the European Headache Federation and Lifting The Burden: The Global Campaign against Headache. J. Headache Pain 2019, 20, 57. [Google Scholar] [CrossRef]
- VanderPluym, J.; Gautreaux, J.; Burch, R.; Whitaker, E.; Roberts, J.; Turner, D.P.; Gelfand, A.A. Evidence Regarding 134 Headache in Children and Adolescents: Protocol for a Systematic Review. Headache 2020, 60, 171–177. [Google Scholar] [CrossRef]
- Lewis, D.; Winner, P.; Saper, J.; Ness, S.; Polverejan, E.; Wang, S.; Kurland, C.L.; Nye, J.; Yuen, E.; Eerdekens, M.; et al. Randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of topiramate for migraine prevention in pediatric subjects 12 to 17 years of age. Pediatrics 2009, 123, 924–934. [Google Scholar] [CrossRef]
- Powers, S.W.; Coffey, C.S.; Chamberlin, L.A.; Ecklund, D.J.; Klingner, E.A.; Yankey, J.W.; Korbee, L.L.; Porter, L.L.; Hershey, A.D.; CHAMP Investigators. Trial of Amitriptyline, Topiramate, and Placebo for Pediatric Migraine. N. Engl. J. Med. 2017, 376, 115–124. [Google Scholar] [CrossRef] [Green Version]
- Lakshmi, C.V.; Singhi, P.; Malhi, P.; Ray, M. Topiramate in the prophylaxis of pediatric migraine: A double-blind placebo-controlled trial. J. Child Neurol. 2007, 22, 829–835. [Google Scholar] [CrossRef]
- Freitag, F.G.; Collins, S.D.; Carlson, H.A.; Goldstein, J.; Saper, J.; Silberstein, S.; Mathew, N.; Winner, P.K.; Deaton, R.; Sommerville, K. Depakote ER Migraine Study Group. A randomized trial of divalproex sodium extended-release tablets in migraine prophylaxis. Neurology 2002, 58, 1652–1659. [Google Scholar] [CrossRef]
- Linde, M.; Mulleners, W.M.; Chronicle, E.P.; McCrory, D.C. Valproate (valproic acid or sodium valproate or a combination of the two) for the prophylaxis of episodic migraine in adults. Cochrane Database Syst. Rev. 2013, 6, CD010611. [Google Scholar] [CrossRef] [Green Version]
- Bidabadi, E.; Mashouf, M. A randomized trial of propranolol versus sodium valproate for the prophylaxis of migraine in pediatric patients. Pediatr. Drugs 2010, 12, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Olness, K.; MacDonald, J.T.; Uden, D.L. Comparison of self-hypnosis and propranolol in the treatment of juvenile classic migraine. Pediatrics 1987, 79, 593–597. [Google Scholar] [CrossRef]
- Marathe, P.H.; Greene, D.S.; Kollia, G.D.; Barbhaiya, R.H. A pharmacokinetic interaction study of avitriptan and propranolol. Clin. Pharmacol. Ther. 1998, 63, 367–378. [Google Scholar] [CrossRef]
- Locher, C.; Kossowsky, J.; Koechlin, H.; Lam, T.L.; Barthel, J.; Berde, C.B.; Gaab, J.; Schwarzer, G.; Linde, K.; Meissner, K. Efficacy, Safety, and Acceptability of Pharmacologic Treatments for Pediatric Migraine Prophylaxis: A Systematic Review and Network Meta-analysis. JAMA Pediatr. 2020, 174, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.W.; Kashikar-Zuck, S.M.; Allen, J.R.; LeCates, S.L.; Slater, S.K.; Zafar, M.; Kabbouche, M.A.; O’Brien, H.L.; Shenk, C.E.; Rausch, J.R.; et al. Cognitive behavioral therapy plus amitriptyline for chronic migraine in children and adolescents: A randomized clinical trial. JAMA 2013, 310, 2622–2630. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Latorre, M.A.; Roig, M. Natural history of migraine in childhood. Cephalalgia 2000, 20, 573–579. [Google Scholar] [CrossRef]
- Esposito, M.; Ruberto, M.; Pascotto, A.; Carotenuto, M. Nutraceutical preparations in childhood migraine prophylaxis: Effects on headache outcomes including disability and behaviour. Neurol. Sci. 2012, 33, 1365–1368. [Google Scholar] [CrossRef]
- Gross, E.C.; Lisicki, M.; Fischer, D.; Sándor, P.S.; Schoenen, J. The metabolic face of migraine—From pathophysiology to treatment. Nat. Rev. Neurol. 2019, 15, 627–643. [Google Scholar] [CrossRef]
- Orr, S.L.; Venkateswaran, S. Nutraceuticals in the prophylaxis of pediatric migraine: Evidence-based review and recommendations. Cephalalgia 2014, 34, 568–583. [Google Scholar] [CrossRef]
- Maier, J.A.; Pickering, G.; Giacomoni, E.; Cazzaniga, A.; Pellegrino, P. Headaches and Magnesium: Mechanisms, Bioavailability, Therapeutic Efficacy and Potential Advantage of Magnesium Pidolate. Nutrients 2020, 12, 2660. [Google Scholar] [CrossRef]
- Grazzi, L.; Andrasik, F.; Usai, S.; Bussone, G. Magnesium as a preventive treatment for pediatric episodic tension-type headache: Results at 1-year follow-up. Neurol. Sci. 2007, 28, 148–150. [Google Scholar] [CrossRef]
- Bruni, O.; Alonso-Alconada, D.; Besag, F.; Biran, V.; Braam, W.; Cortese, S.; Moavero, R.; Parisi, P.; Smits, M.; Van der Heijden, K.; et al. Current role of melatonin in pediatric neurology: Clinical recommendations. Eur. J. Pediatr. Neurol. 2015, 19, 122–133. [Google Scholar] [CrossRef]
- Gelfand, A.A.; Goadsby, P.J. The Role of Melatonin in the Treatment of Primary Headache Disorders. Headache 2016, 56, 1257–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arruda, J.; Yeh, A.M. Integrative Approach to Pediatric Nausea. Pediatr. Ann. 2019, 48, e236–e242. [Google Scholar] [CrossRef]
- Kroon Van Diest, A.M.; Ernst, M.M.; Slater, S.; Powers, S.W. Similarities and Differences Between Migraine in Children and Adults: Presentation, Disability, and Response to Treatment. Curr. Pain Headache Rep. 2017, 21, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrasik, F.; Grazzi, L.; Sansone, E.; D’Amico, D.; Raggi, A.; Grignani, E. Non-pharmacological Approaches for Headaches in Young Age: An Updated Review. Front. Neurol. 2018, 9, 1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomson, T.; Marson, A.; Boon, P.; Canevini, M.P.; Covanis, A.; Gaily, E.; Kälviäinen, R.; Trinka, E. Valproate in the treatment of epilepsy in girls and women of childbearing potential. Epilepsia 2015, 56, 1006–1019. [Google Scholar] [CrossRef]
- Vatzaki, E.; Straus, S.; Dogne, J.M.; Garcia Burgos, J.; Girard, T.; Martelletti, P. Latest clinical recommendations on valproate use for migraine prophylaxis in women of childbearing age: Overview from European Medicines Agency and European Headache Federation. J. Headache Pain 2018, 19, 68. [Google Scholar] [CrossRef]
- Crawford, P. Interactions between antiepileptic drugs and hormonal contraception. CNS Drugs 2002, 16, 263–272. [Google Scholar] [CrossRef]
- Evans, R.W.; Rizzoli, P.; Loder, E.; Bana, D. Beta-blockers for migraine. Headache 2008, 48, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.J.; Jürgens, T.P. Antidepressants in long-term migraine prevention. Drugs 2009, 69, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, A.A.; Goadsby, P.J. Medication overuse in children and adolescents. Curr. Pain Headache Rep. 2014, 18, 428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alstadhaug, K.B.; Ofte, H.K.; Kristoffersen, E.S. Preventing and treating medication overuse headache. Pain Rep. 2017, 2, e612. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Median | Disagreement | Classification |
|---|---|---|
| 7–9 | No | Appropriate with agreement |
| 7–9 | Yes | Appropriate but with disagreement |
| 4–6 | Not applicable | Uncertain |
| 1–3 | Not applicable | Inappropriate |
| Headache Characteristics |
| Onset modalities (sudden onset, progressive) |
| Duration |
| Location (frontal, temporal, occipital, parietal) |
| Quality of pain (pulsating, severe) |
| Intensity |
| Premonitory symptoms |
| Aura |
| Association with vegetative symptoms (dizziness, sweating, etc.) |
| Association with neurological symptoms (ictal episodes, walking impairment, speech impairment, diplopia, etc.) |
| Triggering factors (stress, sleep deprivation, coughing, Valsalva maneuver) |
| Alleviating factors (rest, staying in the dark) |
| Efficacy of analgesic therapy |
| Proximate pathological history |
| Recent trauma |
| Fever |
| Remote pathological history |
| Primary headache |
| Neurocutaneous disorders (e.g., neurofibromatosis) |
| Congenital heart disease |
| Immunodeficiency |
| Neoplasms |
| Coagulopathies |
| Peritoneal ventricular shunts |
| Family history |
| Primary headache |
| Neurocutaneous disorders |
| Congenital heart disease |
| Immunodeficiencies |
| Coagulopathies |
| Primary headache |
| Neurocutaneous disorders |
| Headache Characteristics |
| Pain that wakes the child from sleep or occurs on waking |
| Worsening of headache in recumbency and/or during straining, coughing, and/or other forms of Valsalva maneuver, physical activity |
| Sudden severe headache, thunderclap headache |
| Recurrent localized headache |
| Occipital headache |
| Inadequate response to therapy |
| Changes in headache characteristics (both chronic or acute): intensity, frequency, pattern |
| Chronic progressive headache |
| Clinical and medical history |
| Incomplete medical and clinical history |
| Age < 5 y/o |
| Recent head trauma (<12 h if severe, >12 h if mild) |
| High-risk population (sickle cell anemia, coagulopathy, immunodeficiency, former or present tumor, cardiac diseases with right-left shunt, hydrocephalus or ventricular shunt, type 1 neurofibromatosis, tuberous sclerosis, familiar genetic syndromes) |
| Changes in mood, behavior, or personality * |
| Polyuria, polydipsia |
| Morning/fasting nausea and/or vomiting |
| Growth anomalies (head circumference increase, short stature or growth reduction, precocious/delayed puberty) |
| Neck/rachis symptoms |
| Systemic disease symptoms (weight loss, night sweats, fever, joint pain) |
| Clinical data from physical examination |
| Reduced general condition |
| Neurological signs and symptoms (persistent nausea and/or vomiting, impaired mental state, ataxia, asymmetric, weakness, focal deficits) |
| Motor signs and symptoms (regression of psychomotor development, focal deficits, gait abnormalities, impaired coordination, impaired swallowing) |
| Visual disorders (papilledema, retinal hemorrhage, pathological pupillary response, diplopia, nystagmus or abnormal ocular movements, visual field defects, visual acuity defect reduction unrelated to abnormal ocular refraction) |
| Incompliant child (impossibility to perform physical examination) |
| Neck stiffness or other meningeal signs |
| Trauma |
| Cranial vascular murmur |
| Neurocutaneous markers |
| Macrocephaly |
| Acute Headache | Recurrent Acute Headache |
| Upper respiratory tract infections with or without fever | Migraine Tension headache |
| Acute sinusitis | Cluster headache |
| Pharyngitis | Hypertension |
| Viral or bacterial meningitis | Hyperhyroidism |
| Migraine (first episode) | Pheocromocytoma |
| Drug abuse | Drugs |
| Poisoning | |
| Medications (steroids, oral contraceptives) | |
| Ventricular-peritoneal shunt malfunction | |
| Brain tumor | |
| Subarachnoid haemorrhage | |
| Intracranic haemorrhage | |
| Hydrocephalus | |
| Venous sinuses thrombosis | |
| Chronic progressive headache | Non progressive chronic headache |
| Brain tumor | Chronic migraine |
| Communicating or obstructive hydrocephalus | Tension-type headache |
| Pseudotumor cerebri | Cluster headache |
| Cerebral abscess Subdural chronic hematoma | |
| Aneurysms and vascular malformations Drugs | |
| Poisoning | |
| Daily persistent new onset headache | |
| Primary acute headache and chronic headache association | |
| General and Vital Signs Assessment |
| General condition (complexion, hydration status) |
| Skin temperature |
| Cardiorespiratory activity |
| Blood pressure |
| Auxological parameters: weight, height, head circumference |
| Physical examination |
| Skin: search for skin discolorations |
| Examination of algogenic structures of the head and neck: sinuses, temporomandibular joints, identification of trigger points, pain points or muscle contractures |
| Palpation of the thyroid gland |
| Assessment of nuchal stiffness |
| Pubertal state |
| Systematic neurological examination |
| Mental and psychic status (drowsiness, irritability), alertness, responsiveness, speech |
| Asymmetries and side marks |
| Ocular system: pupillary reflexes, extrinsic ocular motility with nystagmus and diplopia search, visual field |
| Fundus oculi |
| Cranial nerves: facial symmetry, strength and sensitivity of facial districts, signs of focal pathology |
| Marching, balance, coordination, basic gait planting |
| Strength and sensitivity |
| Osteotendinous reflexes (in the infant, archaic reflexes) |
| Primary Headache | Secondary Headache | |
|---|---|---|
| Duration of disease | Chronic, >6 months | Acute-subacute |
| Temporal pattern | Recurring or daily | Progressive |
| Localization | Frontal, temporal | Occipital |
| Features | Pulsating, squeezing | Gravitating |
| Intensity | Mild to severe | Generally severe |
| Time of the day | Indifferent | Upon awakening in the morning |
| Episode duration | Hours to days | Continuous |
| Neurological objectivity | Normal | Impaired |
| Emetic symptomatology | Nausea > vomit | Vomit > nausea |
| Visual symptoms | Visual aura | Diplopia |
| Phonophobia and photophobia | Possible | Absent |
| Drug | Dose | Age Indications | Notes |
|---|---|---|---|
| ALMOTRIPTAN | 6.25–12.5 mg tabs | ≥12 years old | Efficacy on phonophobia and photophobia |
| RIZATRIPTAN | 5–10 mg OSF | ≥5 years old | Reduce dose in the case of simultaneous use of propranolol |
| SUMATRIPTAN | 5–20 mg NS | ≥12 years old | Efficacy on phonophobia and photophobia |
| ZOLMITRIPTAN | 5 mg NS | ≥5 years old | Efficacy at lower doses compared to other triptans |
| Drug | Dose | Notes |
|---|---|---|
| TRIPTAN + IBUPROFEN | Multiple formulations available | |
| SUMATRIPTAN + NAPROXEN | 10/60 mg Tabs 30/180 mg Tabs 85/500 mg Tabs | Efficacy regarding phono- and photophobia Efficacy demonstrated even at the lowest dose Minimum age 12 years |
| Drug | Dose | Notes |
|---|---|---|
| ONDANSETRON | OS, repeatable every 8 h: If <15 kg: 0.2 mg/kg If 15–30 kg: 4 mg If >30 kg: 4–8 mg | Sedation Dystonias |
| PROCHLORPERAZINE | OS: If 10–13 kg: 2.5 mg every 12–24 ore If 13–18 kg: 2.5 mg every 8–12 ore (maximum 10 mg/day) If 18–40 kg: 2.5 mg every 8 h or 5 mg every 12 h IV: 0.1–0.15 mg/kg/dose | Sedation Dystonias |
| PROMETHAZINE | OS, R: 0.25–1 mg every 4–6 h | Sedation Dystonias |
| Drug | Dose | Maximum Dose |
|---|---|---|
| INTRAVENOUS HYDRATION + PROCHLORPERAZINE + IV KETOROLAC | 0.15 mg/kg 0.5 mg/kg | 10 mg 30 mg |
| SUMATRIPTAN | 3–6 mg NS | 20 mg in 24 h |
| METOCLOPRAMIDE | 0.2 mg/kg IV | 10 mg |
| DIHYDROERGOTAMINE (DHE) | 0.5 mg in 3 min IV |
| Drug | Dose | Maximum Dose | Notes |
|---|---|---|---|
| AMITRIPTYLINE (PLUS CBT) | Initial dose: 0.25–0.50 mg/kg/day To be increased in the case of ineffectiveness Maintenance: 1 mg/kg/day | 75 mg/day | Side effects: suicidal ideation. For patients aged 12 years and older with depression or anxiety disorders. |
| TOPIRAMATE | Initial dose: 1–2 mg/kg/day (in younger than 12 years); 2.5 mg/kg/day (in aged 12 years and olders) for a week | 100 mg/day | Side effects: teratogenicity (caution in women of childbearing age). |
| VALPROATE | Initial dose: 10–15 mg/kg/day in 2 doses | 30 mg/kg/day | Side effects: teratogenicity (caution in women of childbearing age). |
| CINNARIZINE | 1.5 mg/kg/day if weight <30 kg 50 mg/day if weight >30 kg | Contraindicated in patients younger than 12 years. | |
| FLUNARIZINE | 3–5 mg/day in a single daily dose | 10 mg/day | Side effects: weight gain, sedation. Contraindicated in patients younger than 12 years. |
| NIMODIPINE | 10–20 mg/day in 3 doses | 150 mg/day | Side effects: mild gastrointestinal disturbances. Contraindicated in patients younger than 12 years. |
| PROPRANOLOL | Initial dose: 1 mg/kg/day in 3 doses Maintenance: 20–40 mg/day in 3 doses | 3 mg/kg/day | Use with caution in asthmatic, depressed or diabetic patients. |
| Nutraceutical | Dose | Notes |
|---|---|---|
| 5-HYDROXYTRYPTOPHAN | 5 mg/kg/day | Side effects: nausea, abdominal pain, drowsiness |
| MAGNESIUM | 1.5–4.5 g/day | Side effects: flatulence, diarrhea. Contraindications: severe renal failure |
| RIBOFLAVIN | 25–400 mg/day | Side effects: yellowish urine, gastro-intestinal symptoms |
| MELATONIN | 3 mg/day before night sleep | High doses may cause daytime drowsiness, impaired physical and mental performance, suppressed body temperature and elevated blood prolactin levels |
| Primary Care Pediatrician Evaluation |
| Recommendation 1: In the case of acute headache in a pediatric patient, the PCP should identify the red flags that require urgent diagnostic and therapeutic procedures by an adequate history collection, in order to distinguish primary from secondary forms. |
| Recommendation 2: Assessment of vital signs, general physical examination, and a complete neurological examination should always be performed in a child with headache, as this can identify warning signs suggestive of secondary headache. In particular, the presence of high-risk red flags suggestive of severe conditions such as infectious processes, vascular lesions or intracranial expansions should be excluded. The neurological examination should include: assessment of level of consciousness, meningeal signs, visual, gait and co-ordination disturbances, speech and hearing disorders, focal neurological deficits such as localized strength or sensory deficits, cranial nerve deficits. The OF is a useful non-invasive examination that a pediatrician can perform if sufficiently experienced. In doubtful cases, an ophthalmologist evaluation for fundoscopy with pupil dilation is recommended. |
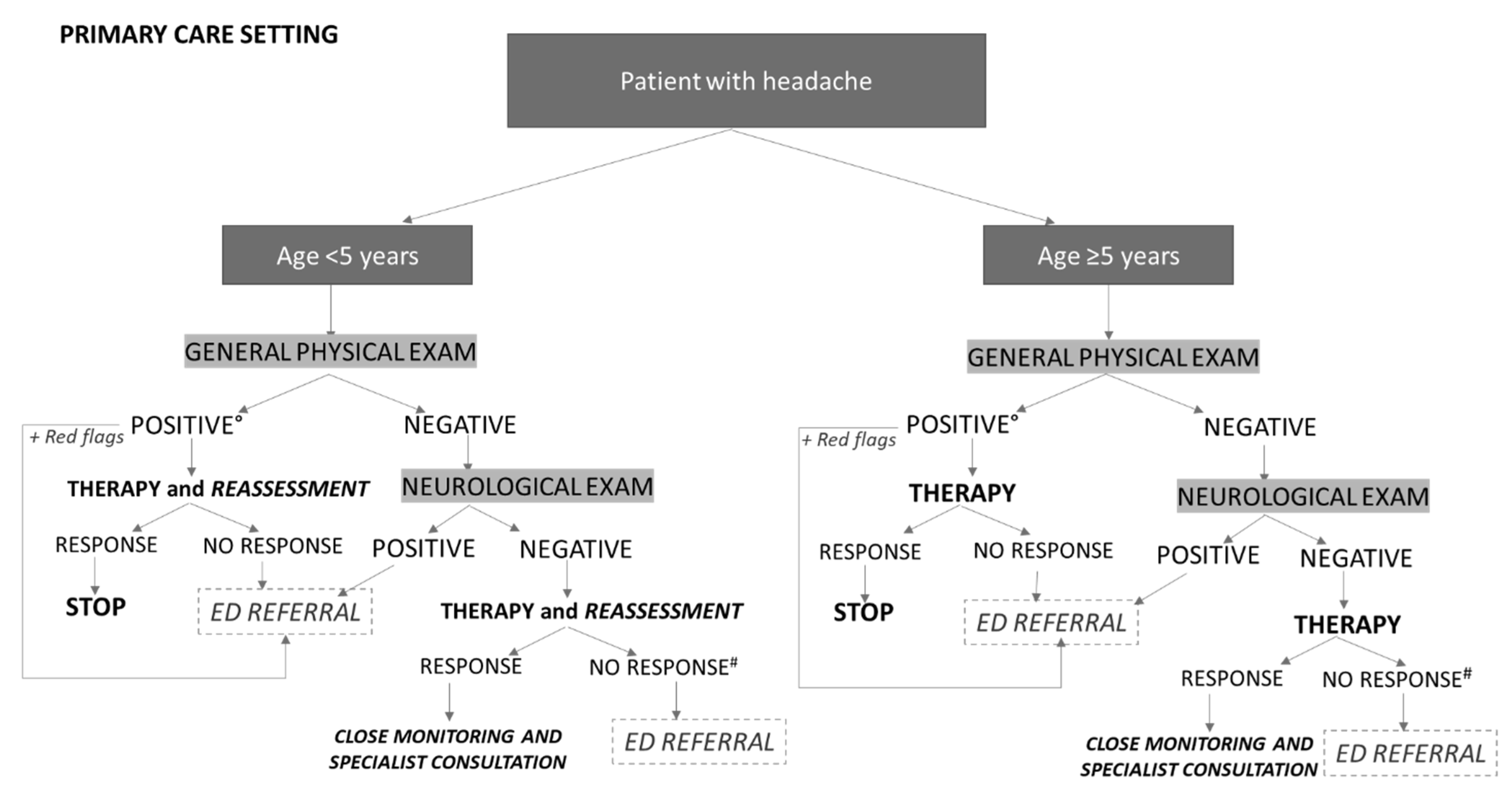
| Recommendation 3: The role of the PCP is to detect potentially dangerous or life-threatening conditions that require an immediate emergency setting medical evaluation. In the case of neurological alterations at physical examination, or in the presence of other warning signs, the patient should be immediately addressed to the ED. In the case of a general physical examination suggestive of secondary and non-life-threatening conditions, the underlying causes should be treated and an initial analgesic therapy approach should be performed under close monitoring, especially in preschool patients. An ED referral is recommended only in the case of general worsening, therapy failure, appearance of warning signs/symptoms, or positive neurological examination. |
| Recommendation 4: In the case of normal general and neurological examination, without red flags, after investigating the patient’s environmental context and presence of trigger factors, the PCP may recommend acute antalgic therapy, the use of a headache diary, and plan a clinical re-evaluation to assess symptoms evolution and response to therapy. Referral to the pediatric neurologist is recommended in the following cases: children under 5 years of age, lack of or insufficient response to therapy, worsening of symptoms, or in general, for a specialist diagnostic definition. |
| Emergency department evaluation |
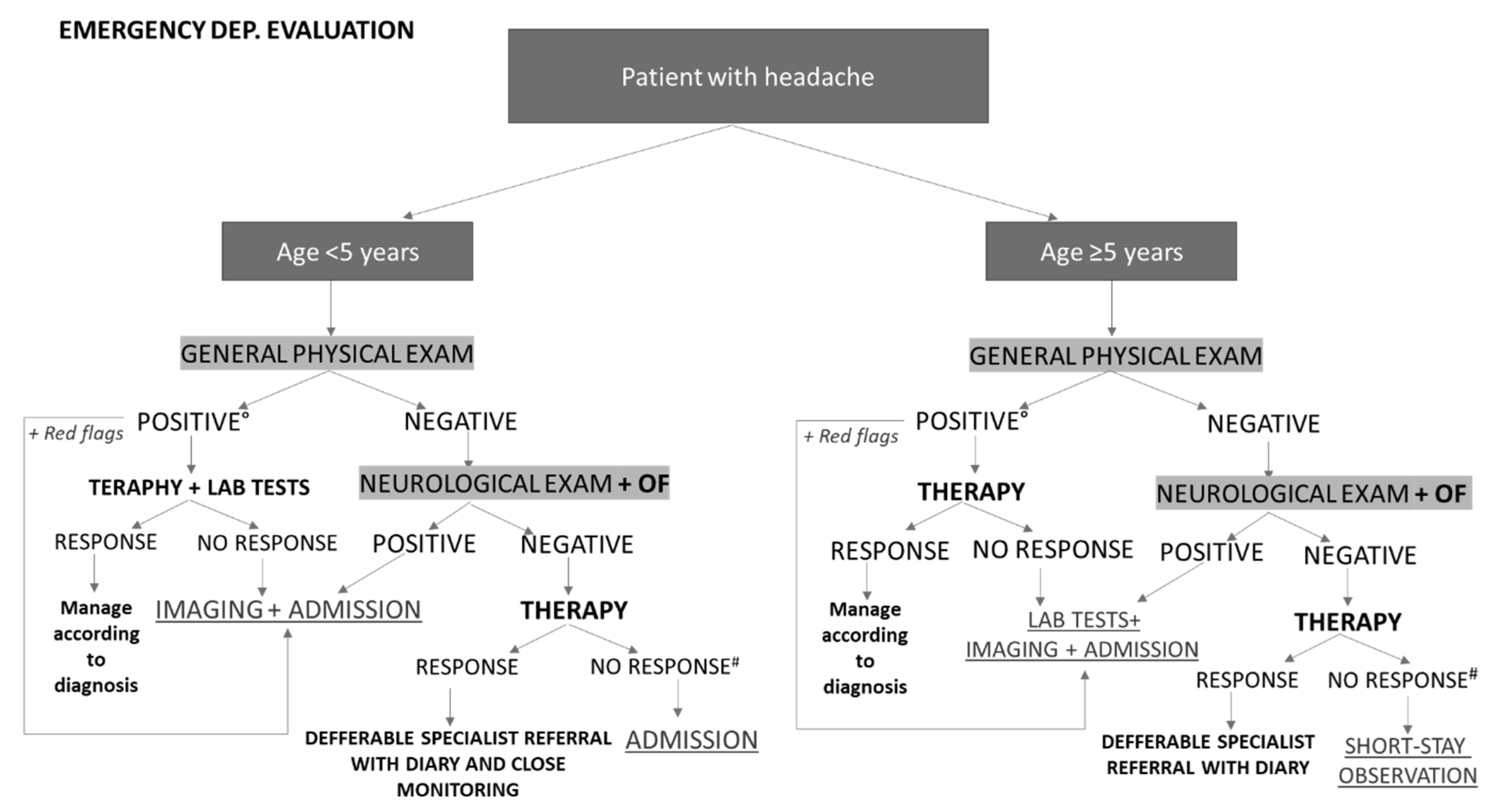
| Recommendation 5: During triage, patients not requiring urgent care should be distinguished from those with red flags suggestive of life-threatening disease. In ED, laboratory tests are indicated in the case of a positive general physical examination for secondary forms or when a benign form (e.g., infectious) is suspected, in order to define etiological therapy. Ophthalmologic consultation should be considered whenever a visual symptom is identified and is not clearly correlated with primary headache or in all cases that require an ocular fundus in cycloplegia. Urgent consultation with a pediatric neurologist is indicated, whenever possible, in cases presenting neurological signs or symptoms; it may be deferred to an elective consultation in cases of headache symptoms suggestive of primary or secondary non-life-threatening forms that can be treated with symptomatic therapy. |
| Recommendation 6: Hospitalization is indicated for patients who, irrespective of age, present with a positive general physical examination for benign secondary forms whose causes require further diagnostic and therapeutic investigation and/or alterations on neurological examination and/or fundus oculi indicative of papilledema and/or red flags. In preschool patients (<5 years old), it may be appropriate to hospitalize even forms with negative neurological and general examination but absent response to symptomatic therapy. A short observation regimen may be planned for similar cases in school-aged patients (>5 years). |
| Recommendation 7: CT scan without contrast medium is the test of choice in the emergency setting, due to its rapidity of execution and its easier accessibility in the ED, without the need for patient sedation. In the case of suspected stroke, brain MRI should be performed within one hour of patient arrival in the ED. |
| Hospital admission |
| Recommendation 8: During hospitalization, a close monitoring of parameters and clinical conditions is appropriate to assess response to therapy and possible appearance of “red flags” for secondary headaches. The choice of diagnostic investigations depends on clinical suspicion and is supported by the evaluation of the pediatric neurologist. In the case of a positive general examination, it is recommended to perform microbiological and specific instrumental examinations to exclude infections. The appearance of neurological warning signs during hospitalization is an indication to perform urgent neuroimaging to exclude life-threatening conditions. |
| Recommendation 9: In the differential diagnosis between primary headache and epilepsy, it is useful to consider some characteristic clinical features and to consult a pediatric neurologist who may request an EEG. |
| Recommendation 10: Red flags identified through the collection of anamnestic data, general and neurological physical examination, should direct to in-depth examinations through neuroimaging. In an inpatient setting, MRI is preferred in the suspicion of lesions of the saddle, craniocervical junction, posterior fossa, white matter abnormalities, congenital malformations and infectious processes, as it is more sensitive than CT and safer in terms of radiation protection. For the evaluation of ischemic events or vascular malformations, it is recommended to consider in addition to the standard sequences also CT angiography or MRA depending on availability and level of urgency. |
| Acute treatment |
| Recommendation 11: In the management of acute headache attack in pediatric patient with no definite diagnosis, ibuprofen is a first-line therapy for his rapidity of action. As an alternative, it is possible to use paracetamol, the efficacy of which is similar to that of ibuprofen, despite lower rapidity. The preferred route of administration is the oral one, using buccal formulations. |
| Recommendation 12: In the case of acute attack in a patient with diagnosis of migraine, in order to treat associated symptoms (phonophobia, photophobia, nausea and vomiting), physicians should explain to the patient that they regress with analgesics taken at the beginning or when pain is still low to moderate. The oral way of administration is the advisable one, in buccal formulations. It is possible to associate an antiemetic treatment in order to promote oral therapy; if nausea and vomiting make the oral route difficult, it may be necessary to refer the patient to the nearest ED to gain a venous access and administer fluids, analgesic and antiemetic therapy. |
| Recommendation 13: Triptans are indicated in adolescents with migraine, possibly in association to ibuprofen in the case of insufficient response to monotherapy. Triptans approved in pediatric age are four: almotriptan, sumatriptan, zolmitriptan, for children older than 12 years, and rizatriptan, for children older than 6 years. Off-label use for younger ages is possible under pediatric neurologist prescription. Their use is restricted to acute pain not responding sufficiently to treatment with non-steroidal anti-inflammatory drugs and/or paracetamol and they should be taken when pain is still low to moderate for a rapid and safe response, even though they may be still effective in cases of pain from moderate to severe. They are available in oral and nasal formulations. Both way of administration showed a similar efficacy, even though the oral one is better tolerated. |
| Recommendation 14: Even though analgesic treatment alone is shown to control associated symptoms, the administration of antiemetic drugs can be considered with a double effect of limiting nausea and vomiting, often associated with headache, and promote oral administration of analgesics, when necessary. The main drugs approved in these conditions are ondansetron, serotonin receptors antagonist, used in hospital, and dopamine antagonists such as promethazine and proclorperazine. |
| Recommendation 15: In children presenting with acute migraine attack, not responding to first line treatment, or status migrainosus, a venous access should be established to start intravenous hyperhydration and intravenous paracetamol or NSAIDs (ibuprofen or ketorolac) therapy. Metoclopramide is a dopamine antagonist alternative to first line analgesics, that showed efficacy in treating both vomiting and pain. In the case of status migrainosus, the therapy consists in intravenous administration of dihydroergotamine at high (0.5–1 mg/kg every 8 h) or low (0.1–0.2 mg/kg every 8 h) dose. |
| Prophylaxis |
| Recommendation 16: The indications for preventive therapy in pediatric headache are: attacks of high intensity or occurring with high frequency (more than 4 days/month with 3–4 headache attacks/month for at least three months), reduction in patient’s quality of life, poor responsiveness to acute treatment with disability. The decision to undertake preventive therapy is a responsibility of the pediatric neurology specialist. Prophylaxis may also prevent adverse events of drug abuse, such as medication overuse headache. |
| Recommendation 17: The current guidelines only provide the use of topiramate, propranolol, amitriptyline + CBT and cinnarizine for the prophylactic treatment of migraine, for which the analysis of the evidence has given satisfactory results in terms of efficacy. |
| Recommendation 18: To date, efficacy data of the main drugs used for headache prophylaxis are controversial. The choice of the appropriate drug is based on comorbidities, adverse effects and parents’ and patient’s preferences. |
| Recommendation 19: Preventive drug therapy should be started at the lowest possible doses. Doses should then be gradually increased over 3–4 weeks until therapeutic benefit develops, the maximum administered dose is reached, or significant side effects occur. Treatment should be continued for 7–8 weeks at the correct effective dose to achieve real benefit. If migraine episodes decrease in frequency and intensity, therapy should be continued for approximately 6–12 months. |
| Recommendation 20: The use of nutraceuticals in the preventive treatment of headache remains debated. In clinical practice, nutraceuticals are not contraindicated in mild primary headaches or in support of drug therapy, considering their good tolerability and safety. |
| Recommendation 21: Physicians should explain to patients and families that lifestyle and certain behavioral factors can influence the frequency of headache and should educate patients and their families to identify and change factors that act as triggers for headache. |
| Recommendation 22: The use of complementary therapies for headache prevention is a possible alternative to pharmacological prophylaxis. In certain patients, on the advice of the specialist, it may be considered an effective first-line therapy. Complementary therapies may also be useful in situations of poor patient and parental compliance, poor tolerance and/or presence of contraindications to drug therapy. |
| Follow-up |
| Recommendation 23: A specialist re-assessment should be recommended every time a patient taking prophylactic therapy shows significant adverse reactions, inadequate tolerance to the drug or rapid changes in the headache pattern during the first months. |
| Recommendation 24: Physical examination of a patient with headache must include heart rate and blood pressure assessment. Evidence from the literature do not give precise indications on blood pressure monitoring in patients with headache but it is considered mandatory in patients assuming beta blockers, calcium channel blockers and amitriptyline. |
| Recommendation 25: Medication overuse headache is a concrete risk in the pediatric age. The PCP must monitor acute treatment in patients with headache. Assumption of NSAIDs for more than 14 days/month, triptans/ergotamine for more than 9 days/months, combined drugs for more than 3 months are criteria for a specialist re-evaluation and start of a preventive therapy. |
| Primary Care Physicians | Hospital Physicians | Pediatric Neurologists |
|---|---|---|
| Evaluate non-critical patients with headache | Detect red-flags requiring urgent imaging and hospital admission | Specialist management of primary and secondary headache patients |
| Detect red-flags requiring immediate emergency setting medical evaluation | Detect underling conditions requiring specific treatments | Support primary care and hospital physicians for diagnosis and treatment |
| Treat non-life-threatening headache and underlining conditions | Treat and observe patients not-responding to oral acute therapy | Follow-up |
| Monitor specific cases and require specialist consultations when indicated | Request specialist consultation when indicated |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prezioso, G.; Suppiej, A.; Alberghini, V.; Bergonzini, P.; Capra, M.E.; Corsini, I.; De Fanti, A.; Fiumana, E.; Fornaro, M.; Marangio, L.; et al. Pediatric Headache in Primary Care and Emergency Departments: Consensus with RAND/UCLA Method. Life 2022, 12, 142. https://doi.org/10.3390/life12020142
Prezioso G, Suppiej A, Alberghini V, Bergonzini P, Capra ME, Corsini I, De Fanti A, Fiumana E, Fornaro M, Marangio L, et al. Pediatric Headache in Primary Care and Emergency Departments: Consensus with RAND/UCLA Method. Life. 2022; 12(2):142. https://doi.org/10.3390/life12020142
Chicago/Turabian StylePrezioso, Giovanni, Agnese Suppiej, Valentina Alberghini, Patrizia Bergonzini, Maria Elena Capra, Ilaria Corsini, Alessandro De Fanti, Elisa Fiumana, Martina Fornaro, Lucia Marangio, and et al. 2022. "Pediatric Headache in Primary Care and Emergency Departments: Consensus with RAND/UCLA Method" Life 12, no. 2: 142. https://doi.org/10.3390/life12020142