
Self-Rated Benefits of Auditory Performance after Bonebridge Implantation in Patients with Conductive or Mixed Hearing Loss, or Single-Sided Deafness



Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Surgery
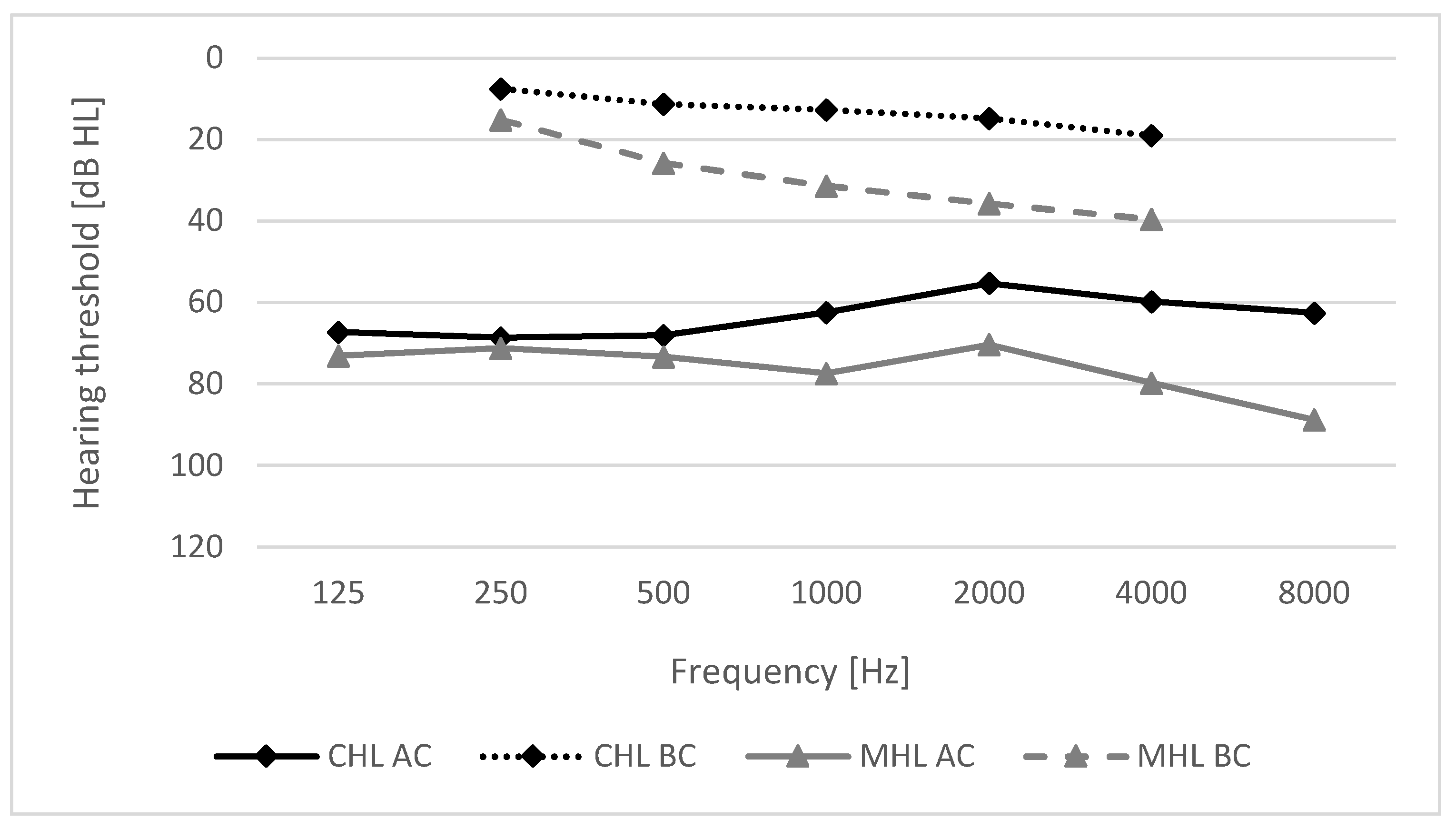
2.3. Pre-Operative Audiometric Assessment
2.4. Post-Operative Assessment
2.5. Statistical Analysis
2.6. Study Design
3. Results
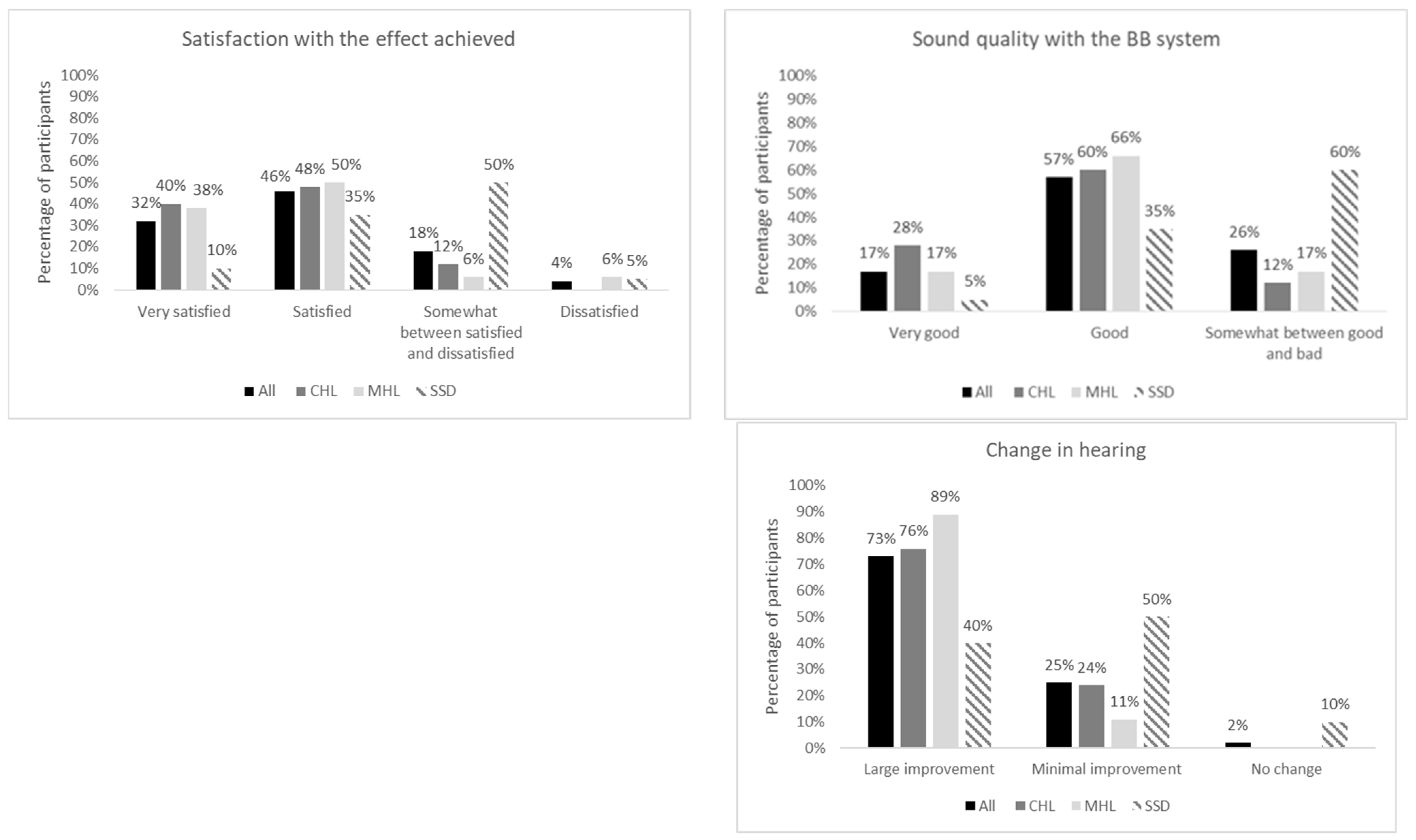
3.1. Subjective Assessment of Satisfaction—Results of the Structured Interview
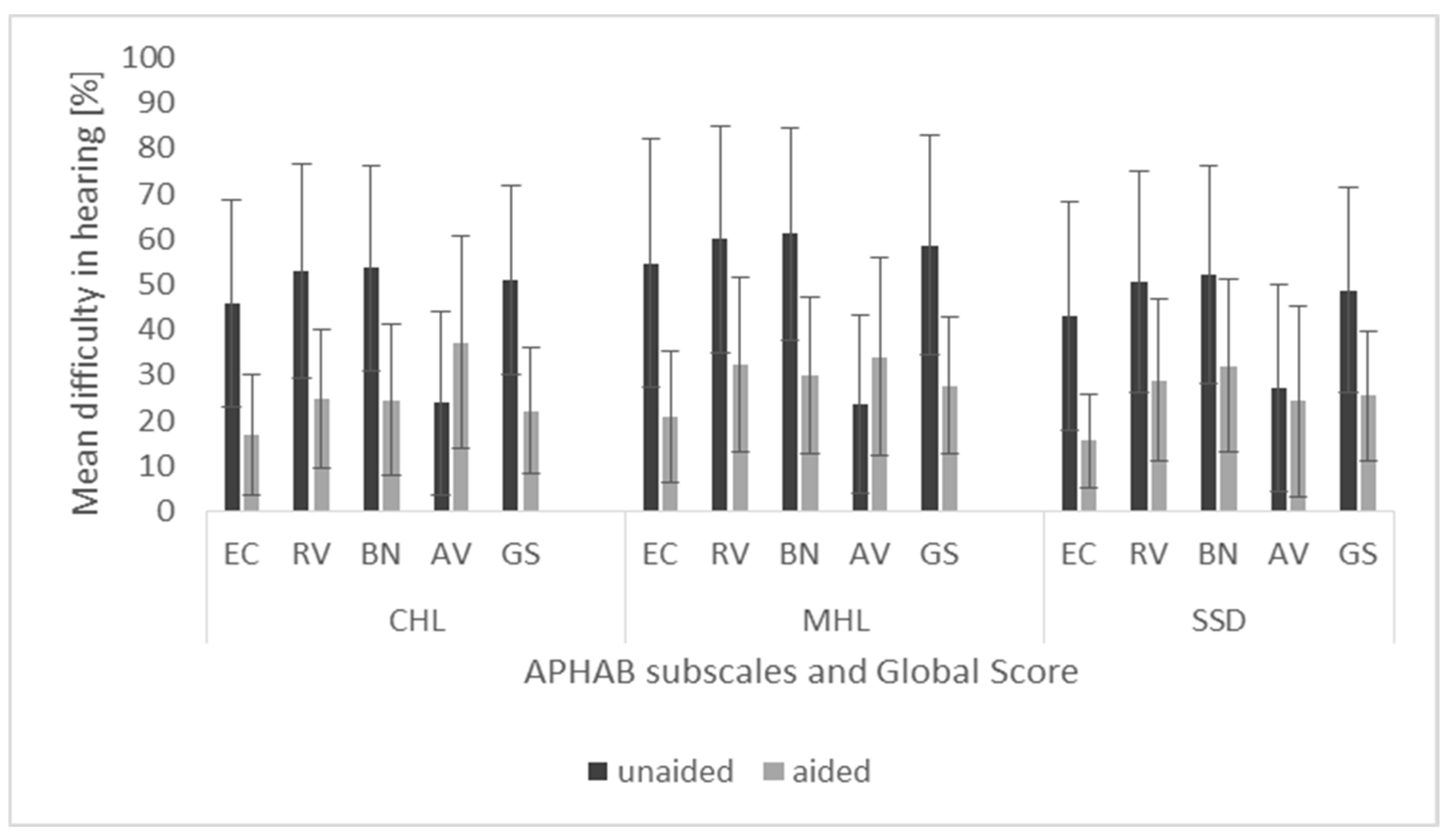
3.2. Limitation in Activity and Restriction in Participation—APHAB Outcomes
3.3. Relationship between APHAB and Hearing Impairment in the Contralateral Ear
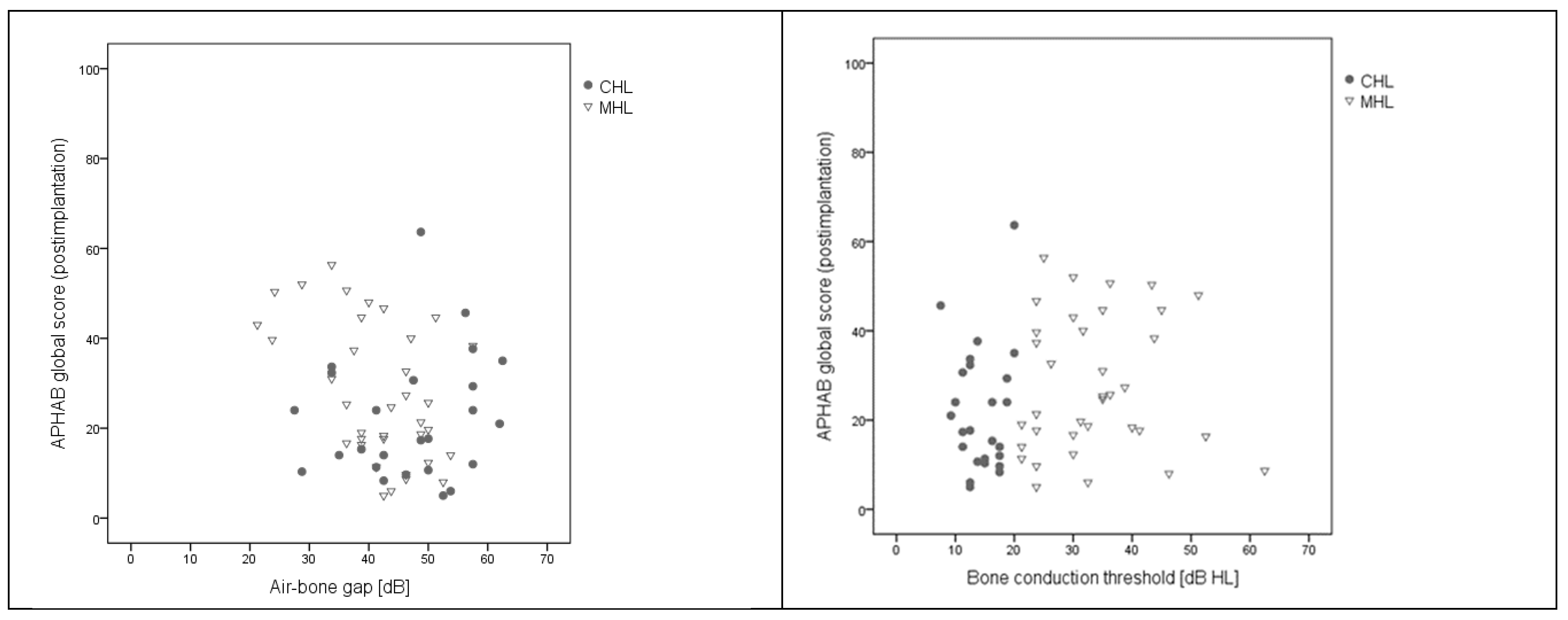
3.4. Relationships between APHAB Score, Air-Bone Gap, and Bone Conduction Threshold in the Implanted Ear
3.5. Relationships between APHAB Score, Duration of BB Use, and Time per Day of Processor Use
4. Discussion
4.1. Conductive and Mixed Hearing Loss
4.2. Single-Sided Deafness
4.3. Limitations
4.4. Summary
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Report on Hearing. Available online: https://www.who.int/publications/i/item/world-report-on-hearing (accessed on 25 November 2021).
- Cox, R.M. Assessment of Subjective Outcome of Hearing Aid Fitting: Getting the Client’s Point of View. Int. J. Audiol. 2003, 42 (Suppl. 1), S90–96. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.M.; Alexander, G.C. The Abbreviated Profile of Hearing Aid Benefit. Ear Hear 1995, 16, 176–186. [Google Scholar] [CrossRef]
- Magele, A.; Schoerg, P.; Stanek, B.; Gradl, B.; Sprinzl, G.M. Active Transcutaneous Bone Conduction Hearing Implants: Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0221484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, R.M.; Alexander, G.C. Measuring Satisfaction with Amplification in Daily Life: The SADL Scale. Ear Hear 1999, 20, 306–320. [Google Scholar] [CrossRef] [Green Version]
- Król, B.; Cywka, K.B.; Skarżyńska, M.B.; Skarżyński, P.H. Implantation of the Bonebridge BCI 602 after Mastoid Obliteration with S53P4 Bioactive Glass: A Safe Method of Treating Difficult Anatomical Conditions-Preliminary Results. Life 2021, 11, 374. [Google Scholar] [CrossRef] [PubMed]
- Król, B.; Cywka, K.B.; Skarżyńska, M.B.; Skarżyński, P.H. Mastoid Obliteration with S53P4 Bioactive Glass after Canal Wall down Mastoidectomy: Preliminary Results. Am. J. Otolaryngol. 2021, 42, 102895. [Google Scholar] [CrossRef]
- Król, B.; Porowski, M.; Cywka, K.B.; Skarżyńska, M.B.; Skarżyński, P.H. Mastoid Obliteration with S53P4 Bioactive Glass Can Make Bonebridge Implantation Feasible: A Case Report. Am. J. Case Rep. 2020, 21, e925914. [Google Scholar] [CrossRef]
- Riss, D.; Arnoldner, C.; Baumgartner, W.-D.; Blineder, M.; Flak, S.; Bachner, A.; Gstoettner, W.; Hamzavi, J.-S. Indication Criteria and Outcomes with the Bonebridge Transcutaneous Bone-Conduction Implant. Laryngoscope 2014, 124, 2802–2806. [Google Scholar] [CrossRef]
- Sprinzl, G.; Lenarz, T.; Ernst, A.; Hagen, R.; Wolf-Magele, A.; Mojallal, H.; Todt, I.; Mlynski, R.; Wolframm, M.D. First European Multicenter Results with a New Transcutaneous Bone Conduction Hearing Implant System: Short-Term Safety and Efficacy. Otol. Neurotol. 2013, 34, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Sprinzl, G.M.; Wolf-Magele, A. The Bonebridge Bone Conduction Hearing Implant: Indication Criteria, Surgery and a Systematic Review of the Literature. Clin. Otolaryngol. 2016, 41, 131–143. [Google Scholar] [CrossRef]
- Dillon, M.T.; Buss, E.; Rooth, M.A.; King, E.R.; Deres, E.J.; Buchman, C.A.; Pillsbury, H.C.; Brown, K.D. Effect of Cochlear Implantation on Quality of Life in Adults with Unilateral Hearing Loss. Audiol. Neurootol. 2017, 22, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Schmerber, S.; Deguine, O.; Marx, M.; Van de Heyning, P.; Sterkers, O.; Isabelle, M.; Garin, P.; Godey, B.; Vincent, C.; Venail, F.; et al. Safety and Effectiveness of the Bonebridge Transcutaneous Active Direct-Drive Bone-Conduction Hearing Implant at 1-Year Device Use. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1835–1851. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Chen, P.; Zhao, C.; Liu, Y.; Gao, M.; Huang, Z.; Zhao, S. Audiological and Subjective Outcomes of 100 Implanted Transcutaneous Bone Conduction Devices and Preoperative Bone Conduction Hearing Aids in Patients with Bilateral Microtia-Atresia. Acta Oto-Laryngologica 2020, 140, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Ihler, F.; Volbers, L.; Blum, J.; Matthias, C.; Canis, M. Preliminary Functional Results and Quality of Life after Implantation of a New Bone Conduction Hearing Device in Patients with Conductive and Mixed Hearing Loss. Otol Neurotol. 2014, 35, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Monini, S.; Bianchi, A.; Talamonti, R.; Atturo, F.; Filippi, C.; Barbara, M. Patient Satisfaction after Auditory Implant Surgery: Ten-Year Experience from a Single Implanting Unit Center. Acta Otolaryngol. 2017, 137, 389–397. [Google Scholar] [CrossRef]
- Skarżyński, P.H.; Ratuszniak, A.; Król, B.; Kozieł, M.; Osińska, K.; Cywka, K.B.; Sztabnicka, A.; Skarżyński, H. The Bonebridge in Adults with Mixed and Conductive Hearing Loss: Audiological and Quality of Life Outcomes. Audiol. Neurootol. 2019, 24, 90–99. [Google Scholar] [CrossRef]
- Ratuszniak, A.; Skarzynski, P.H.; Gos, E.; Skarzynski, H. The Bonebridge Implant in Older Children and Adolescents with Mixed or Conductive Hearing Loss: Audiological Outcomes. Int. J. Pediatr. Otorhinolaryngol. 2019, 118, 97–102. [Google Scholar] [CrossRef]
- Ren, R.; Zhao, S.; Wang, D.; Li, Y.; Ma, X.; Li, Y.; Fu, X.; Chen, P.; Dou, J. Audiological Effectiveness of Bonebridge Implantation for Bilateral Congenital Malformation of the External and Middle Ear. Eur. Arch. Otorhinolaryngol. 2019, 276, 2755–2762. [Google Scholar] [CrossRef] [PubMed]
- Curca, I.A.; Parsa, V.; Macpherson, E.A.; Scollie, S.; Vansevenant, K.; Zimmerman, K.; Lewis-Teeter, J.; Allen, P.; Parnes, L.; Agrawal, S. Audiological Outcome Measures with the BONEBRIDGE Transcutaneous Bone Conduction Hearing Implant: Impact of Noise, Reverberation and Signal Processing Features. Int. J. Audiol. 2020, 59, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Garcier, M.; Lavedrine, A.; Gagneux, C.; Eluecque, T.; Grayeli, A.B. Bone-Anchored and Closed Skin Bonebridge Implant in Adults: Hearing Performances and Quality of Life. AUD 2021, 26, 310–316. [Google Scholar] [CrossRef]
- Salcher, R.; Zimmermann, D.; Giere, T.; Lenarz, T.; Maier, H. Audiological Results in SSD With an Active Transcutaneous Bone Conduction Implant at a Retrosigmoidal Position. Otol. Neurotol. 2017, 38, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Löhler, J.; Gräbner, F.; Wollenberg, B.; Schlattmann, P.; Schönweiler, R. Sensitivity and Specificity of the Abbreviated Profile of Hearing Aid Benefit (APHAB). Eur. Arch. Otorhinolaryngol. 2017, 274, 3593–3598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BIAP-Bureau International d’Audiophonologie. Available online: https://www.biap.org/en/component/content/article/65-recommendations/ct-2-classification/5-biap-recommendation-021-bis (accessed on 25 November 2021).
- Laske, R.D.; Röösli, C.; Pfiffner, F.; Veraguth, D.; Huber, A.M. Functional Results and Subjective Benefit of a Transcutaneous Bone Conduction Device in Patients With Single-Sided Deafness. Otol. Neurotol. 2015, 36, 1151–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giolas, T.G.; Wark, D.J. Communication Problems Associated with Unilateral Hearing Loss. J. Speech Hear Disord. 1967, 32, 336–343. [Google Scholar] [CrossRef]
- Kim, G.; Ju, H.M.; Lee, S.H.; Kim, H.-S.; Kwon, J.A.; Seo, Y.J. Efficacy of Bone-Anchored Hearing Aids in Single-Sided Deafness: A Systematic Review. Otol. Neurotol. 2017, 38, 473–483. [Google Scholar] [CrossRef]
- Hol, M.K.S.; Kunst, S.J.W.; Snik, A.F.M.; Bosman, A.J.; Mylanus, E.A.M.; Cremers, C.W.R.J. Bone-Anchored Hearing Aids in Patients with Acquired and Congenital Unilateral Inner Ear Deafness (Baha CROS): Clinical Evaluation of 56 Cases. Ann. Otol. Rhinol. Laryngol. 2010, 119, 447–454. [Google Scholar] [CrossRef]
- Saroul, N.; Nicolas, S.; Akkari, M.; Mohamed, A.; Pavier, Y.; Yoann, P.; Gilain, L.; Laurent, G.; Mom, T.; Thierry, M. Long-Term Benefit and Sound Localization in Patients with Single-Sided Deafness Rehabilitated with an Osseointegrated Bone-Conduction Device. Otol. Neurotol. 2013, 34, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Lorens, A.; Kruszyńska, M.; Obrycka, A.; Skarzynski, P.H.; Wilson, B.; Skarzynski, H. Binaural Advantages in Using a Cochlear Implant for Adults with Profound Unilateral Hearing Loss. Acta Otolaryngol. 2019, 139, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Vermeire, K.; Van de Heyning, P. Binaural Hearing after Cochlear Implantation in Subjects with Unilateral Sensorineural Deafness and Tinnitus. Audiol. Neurootol. 2009, 14, 163–171. [Google Scholar] [CrossRef]
- Skarzynski, H.; Lorens, A.; Kruszynska, M.; Obrycka, A.; Pastuszak, D.; Skarzynski, P.H. The Hearing Benefit of Cochlear Implantation for Individuals with Unilateral Hearing Loss, but No Tinnitus. Acta Otolaryngol. 2017, 137, 723–729. [Google Scholar] [CrossRef]
- Távora-Vieira, D.; Marino, R.; Acharya, A.; Rajan, G.P. The Impact of Cochlear Implantation on Speech Understanding, Subjective Hearing Performance, and Tinnitus Perception in Patients with Unilateral Severe to Profound Hearing Loss. Otol. Neurotol. 2015, 36, 430–436. [Google Scholar] [CrossRef]
- Newman, C.W.; Sandridge, S.A.; Wodzisz, L.M. Longitudinal Benefit from and Satisfaction with the Baha System for Patients with Acquired Unilateral Sensorineural Hearing Loss. Otol. Neurotol. 2008, 29, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.L.N.; Hickson, L.; McPherson, B. Hearing Aid Satisfaction: What Does Research from the Past 20 Years Say? Trends Amplif. 2003, 7, 117–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olusanya, B.O.; Davis, A.C.; Hoffman, H.J. Hearing Loss Grades and the International Classification of Functioning, Disability and Health. Bull. World Health Organ. 2019, 97, 725–728. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Participants n = 81 | CHL n = 25 | MHL n = 36 | SSD n = 20 | Test Result | ||
|---|---|---|---|---|---|---|
| Sex | Women | 39 (48.1) | 12 (48.0) | 17 (46.2) | 10 (50.0) | χ2 = 0.04; p = 0.980 |
| Men | 43 (51.9) | 13 (52.0) | 19 (52.8) | 10 (50.0) | ||
| Age | Range | 18–74 | 18–67 | 18–74 | 19–72 | F = 3.66; p = 0.030; e2 = 0.08 |
| M [SD] | 44.5 [16.2] | 39.1 [16.1] | 49.6 [15.9] | 42.0 [14.7] | ||
| Educational status | Primary | 24 (29.6) | 6 (24.0) | 12 (33.3) | 6 (30.0) | χ2 = 2.95; p = 0.567 |
| Secondary | 26 (32.1) | 9 (36.0) | 13 (36.1) | 4 (20.0) | ||
| University | 31 (38.3) | 10 (40.0) | 11 (30.6) | 10 (50.0) | ||
| Marital status | Married, in relationship | 50 (61.8) | 16 (64.0) | 21 (58.3) | 13 (65.0) | χ2 = 0.32; p = 0.852 |
| Not in relationship | 31 (38.2) | 9 (36.0) | 15 (41.7) | 7 (35.0) | ||
| Employment status | Employed | 52 (64.2) | 19 (76.0) | 18 (50.0) | 15 (75.0) | χ2 = 5.69; p = 0.058 |
| Unemployed | 29 (35.8) | 6 (24.0) | 18 (50.0) | 5 (25.0) | ||
| Place of residence | Rural | 22 (27.2) | 5 (20.0) | 12 (33.3) | 5 (25.0) | χ2 = 1.39; p = 0.499 |
| Urban | 59 (72.8) | 20 (80.0) | 24 (66.7) | 15 (75.0) | ||
| Use of a processor (hours/day) | Range | 4–20 | 5–20 | 4–20 | 4–12 | F = 5.18; p = 0.008; e2 = 0.12 |
| M [SD] | 9.8 [4.1] | 9.7 [3.7] | 11.0 [4.5] | 7.6 [2.8] | ||
| Use of BB (years) | Range | 0.5–6.2 | 0.6–6.1 | 0.5–6.2 | 0.6–4.7 | F = 9.87; p < 0.001; e2 = 0.20 |
| M [SD] | 2.8 [1.8] | 3.1 [1.8] | 3.7 [1.8] | 2.0 [1.2] |
| 1. Are you satisfied with the effect achieved? |
|
| 2. How do you rate your hearing (sound quality) with the Bonebridge system? |
|
| 3. How do you rate the change in hearing when you use the processor compared to the state before the implant surgery? |
|
| Hearing in Contralateral Ear | Unaided | Aided | t | p | ||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ES | ||||
| Normal hearing (n = 25) | EC | 33.24 | 16.87 | 13.88 | 12.13 | 8.39 | <0.001 | 1.68 |
| RV | 42.16 | 18.15 | 25.16 | 16.28 | 6.93 | <0.001 | 1.39 | |
| BN | 46.20 | 20.34 | 25.64 | 16.60 | 5.76 | <0.001 | 1.15 | |
| AV | 23.64 | 21.16 | 31.88 | 23.27 | 2.28 | 0.032 | 0.46 | |
| GS | 40.54 | 16.99 | 21.56 | 13.85 | 8.26 | <0.001 | 1.65 | |
| Mild/moderate HL (n = 25) | EC | 58.32 | 19.98 | 21.80 | 12.96 | 8.43 | <0.001 | 1.69 |
| RV | 62.20 | 20.08 | 29.08 | 18.24 | 6.81 | <0.001 | 1.36 | |
| BN | 61.68 | 16.87 | 26.32 | 16.55 | 8.92 | <0.001 | 1.78 | |
| AV | 24.52 | 15.84 | 35.96 | 21.52 | 2.22 | 0.036 | 0.45 | |
| GS | 60.73 | 17.69 | 25.73 | 14.25 | 9.12 | <0.001 | 1.82 | |
| Severe/very severe HL (n = 11) | EC | 74.82 | 28.08 | 25.73 | 16.71 | 5.46 | <0.001 | 1.65 |
| RV | 79.73 | 25.75 | 39.36 | 19.04 | 4.59 | 0.001 | 1.38 | |
| BN | 76.73 | 28.11 | 35.55 | 18.50 | 4.87 | 0.001 | 1.47 | |
| AV | 21.82 | 25.57 | 41.45 | 22.90 | 2.01 | 0.073 | 0.61 | |
| GS | 77.09 | 24.53 | 33.55 | 16.44 | 5.68 | <0.001 | 1.71 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratuszniak, A.; Skarzynski, P.H.; Gos, E.; Skarzynski, H. Self-Rated Benefits of Auditory Performance after Bonebridge Implantation in Patients with Conductive or Mixed Hearing Loss, or Single-Sided Deafness. Life 2022, 12, 137. https://doi.org/10.3390/life12020137
Ratuszniak A, Skarzynski PH, Gos E, Skarzynski H. Self-Rated Benefits of Auditory Performance after Bonebridge Implantation in Patients with Conductive or Mixed Hearing Loss, or Single-Sided Deafness. Life. 2022; 12(2):137. https://doi.org/10.3390/life12020137
Chicago/Turabian StyleRatuszniak, Anna, Piotr H. Skarzynski, Elżbieta Gos, and Henryk Skarzynski. 2022. "Self-Rated Benefits of Auditory Performance after Bonebridge Implantation in Patients with Conductive or Mixed Hearing Loss, or Single-Sided Deafness" Life 12, no. 2: 137. https://doi.org/10.3390/life12020137