
Novel Biomarkers Predictive of Diabetic Charcot Foot—An Overview of the Literature
 , , , , , and
, , , , , and
Abstract
:1. Introduction
1.1. Epidemiology
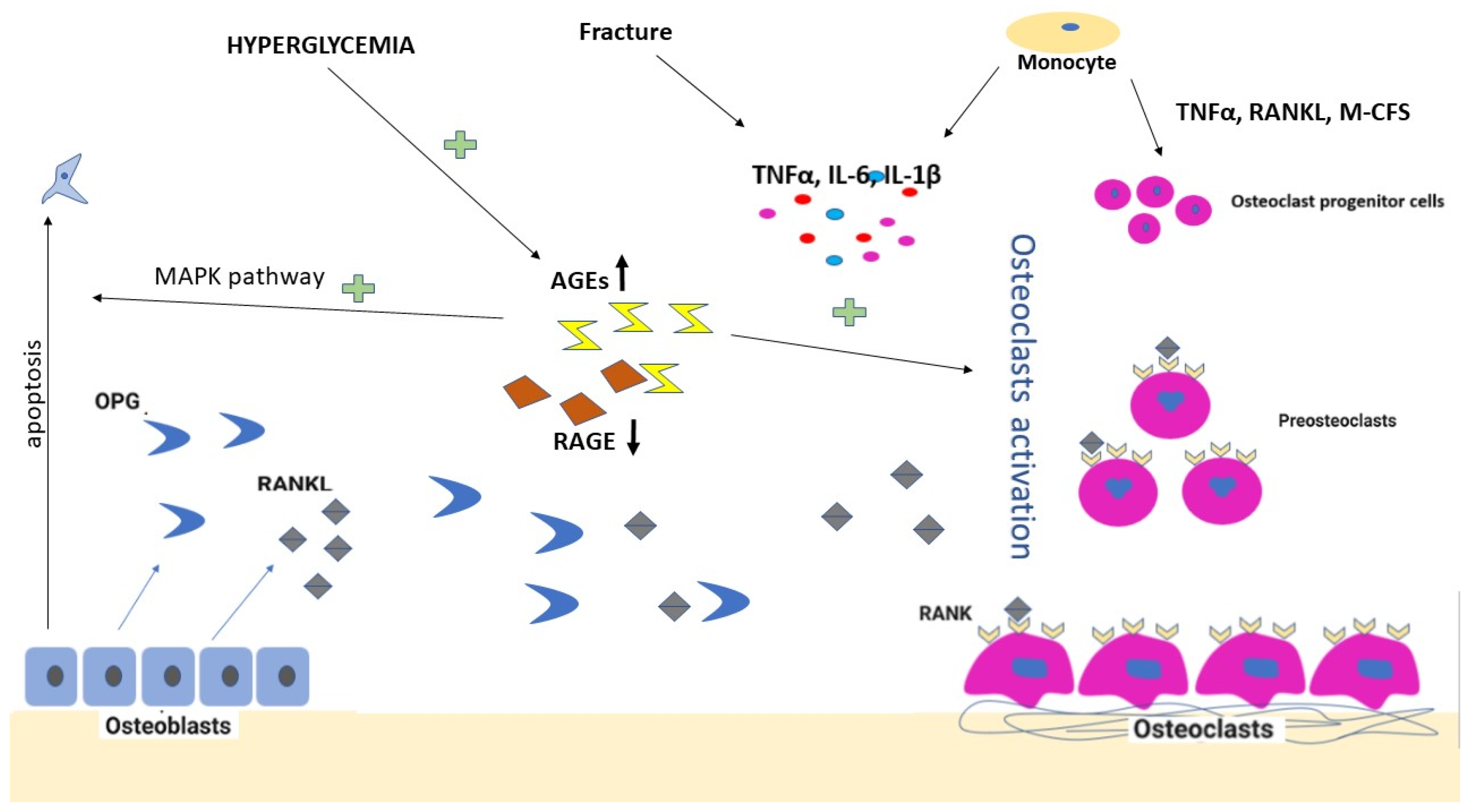
1.2. Pathogenesis
1.3. Inflammatory Signaling
1.4. Cytokine Balance
1.5. Additional Contributing Factors
1.6. Genetics
1.7. Clinical Features and Classifications
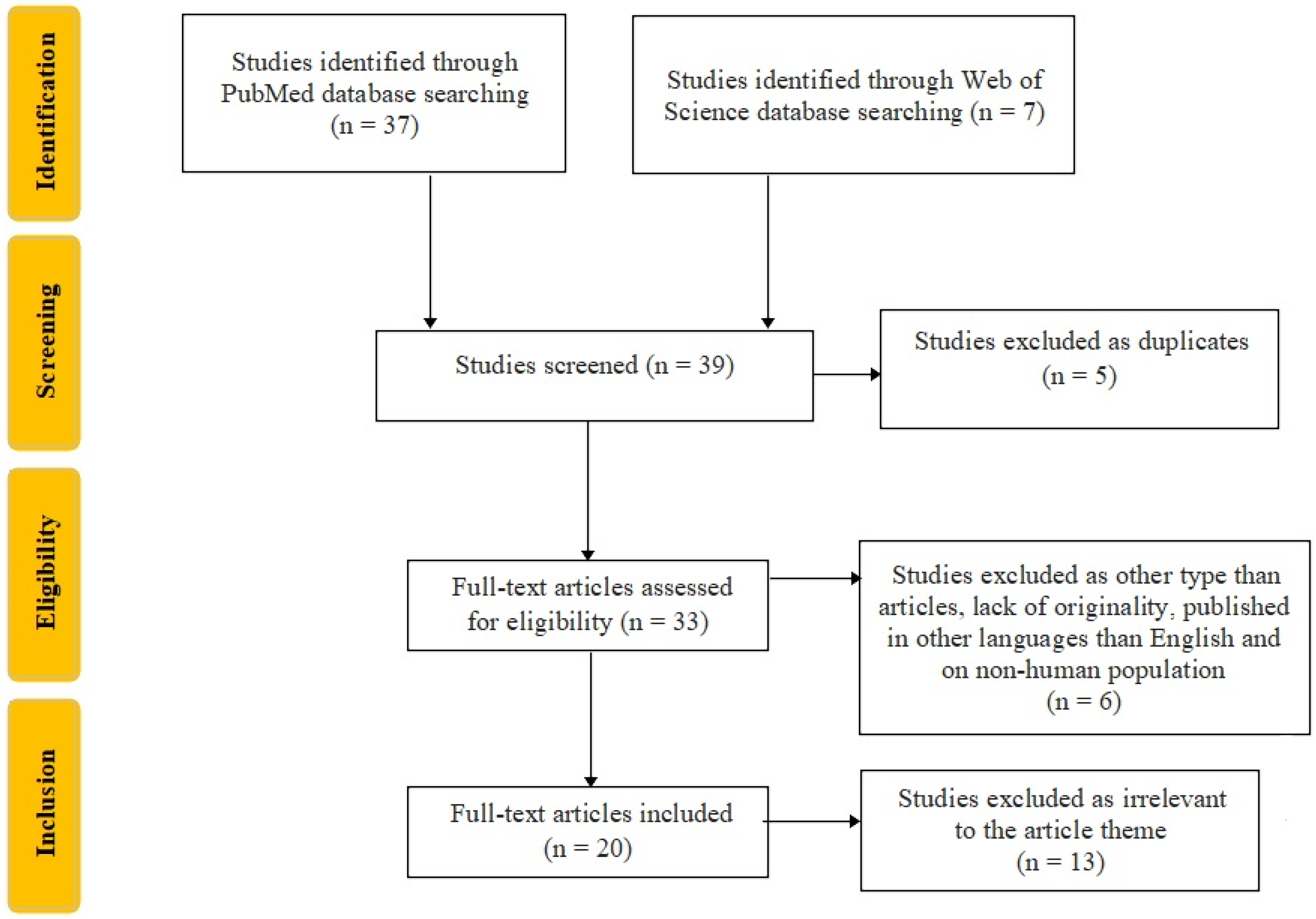
2. Material and Methods
3. Results
3.1. The Inflammatory Cascade
3.2. Pro-Inflammatory Changes in the Immune Phenotype and the Whole Methylome of Monocytes
3.3. Calcium and Bone Turnover Parameters
3.4. Genotype Predisposition
3.5. Paraclinical Investigations
4. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lavery, L.A.; Oz, O.K.; Bhavan, K.; Wukich, D.K. Diabetic Foot Syndrome in the Twenty-First Century. Clin. Podiatr. Med. Surg. 2019, 36, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Carro, G.V.; Saurral, R.; Witman, E.L.; Braver, J.D.; David, R.; Alterini, P.A.; Illuminati, G.; Carrió, L.M.; Torres, J.C. Ataque de pie diabético. Descripción fisiopatológica, presentación clínica, tratamiento y evolución [Diabetic foot attack. Pathophysiological description, clinical presentation, treatment and outcomes]. Med. (B Aires) 2020, 80, 523–530. [Google Scholar]
- Schmidt, B.M. Clinical insights into Charcot foot. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101563. [Google Scholar] [CrossRef] [PubMed]
- Kwaadu, K.Y. Charcot Reconstruction. Clin. Podiatr. Med. Surg. 2020, 37, 247–261. [Google Scholar] [CrossRef] [PubMed]
- Rosskopf, A.B.; Loupatatzis, C.; Pfirrmann, C.; Böni, T.; Berli, M.C. The Charcot foot: A pictorial review. Insights Imaging 2019, 10, 77. [Google Scholar] [CrossRef] [Green Version]
- Bobirca, F.; Smarandache, C.G.; Bobirca, A.; Alexandru, C.; Dumitrescu, D.; Stoian, A.P.; Bica, C.; Brinduse, L.A.; Musetescu, A.; Gheoca-Mutu, D.-E.; et al. The Outcome of Surgical Treatment for the Neuropathic Diabetic Foot Lesions—A Single-Center Study. Life 2022, 12, 1156. [Google Scholar] [CrossRef]
- Fabrin, J.; Larsen, K.; Holstein, P.E. Long-term follow-up in diabetic Charcot feet with spontaneous onset. Diabetes Care 2000, 23, 796–800. [Google Scholar] [CrossRef] [Green Version]
- Zakin, E.; Abrams, R.; Simpson, D.M. Diabetic Neuropathy. Semin Neurol. 2019, 39, 560–569. [Google Scholar] [CrossRef]
- Stuck, R.M.; Sohn, M.-W.; Budiman-Mak, E.; Lee, T.A.; Weiss, K.B. Charcot Arthropathy Risk Elevation in the Obese Diabetic Population. Am. J. Med. 2008, 121, 1008–1014. [Google Scholar] [CrossRef]
- Metcalf, L.; Musgrove, M.; Bentley, J.; Berrington, R.; Bunting, D.; Mousley, M.; Thompson, J.; Sprengel, M.; Turtle-Savage, V.; Game, F.; et al. Prevalence of active Charcot disease in the East Midlands of England. Diabet. Med. 2018, 35, 1371–1374. [Google Scholar] [CrossRef]
- Lesley, M.; Hordon, D. Available online: https://www.uptodate.com/contents/diabetic-neuroarthropathy (accessed on 6 October 2022).
- Molines, L.; Darmon, P.; Raccah, D. Charcot’s foot: Newest findings on its pathophysiology, diagnosis and treatment. Diabetes Metab. 2010, 36, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Baumhauer, J.F.; O’Keefe, R.J.; Schon, L.C.; Pinzur, M.S. Cytokine-Induced Osteoclastic Bone Resorption in Charcot Arthropathy: An Immunohistochemical Study. Foot Ankle Int. 2006, 27, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Kloska, A.; Korzon-Burakowska, A.; Malinowska, M.; Bruhn-Olszewska, B.; Gabig-Cimińska, M.; Jakóbkiewicz-Banecka, J. The role of genetic factors and monocyte-to-osteoclast differentiation in the pathogenesis of Charcot neuroarthropathy. Diabetes Res. Clin. Pract. 2020, 166, 108337. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.B.; Christensen, T.M.; Bülow, J.; Rørdam, L.; Jørgensen, N.R.; Svendsen, O.L. Markers of Local Inflammation and Bone Resorption in the Acute Diabetic Charcot Foot. J. Diabetes Res. 2018, 2018, 5647981. [Google Scholar] [CrossRef] [Green Version]
- Petrova, N.L.; Dew, T.K.; Musto, R.L.; Sherwood, R.A.; Bates, M.; Moniz, C.F.; Edmonds, M.E. Inflammatory and bone turnover markers in a cross-sectional and prospective study of acute Charcot osteoarthropathy. Diabet. Med. 2015, 32, 267–273. [Google Scholar] [CrossRef]
- Mabilleau, G.; Petrova, N.L.; Edmonds, M.E.; Sabokbar, A. Increased osteoclastic activity in acute Charcot’s osteoarthropathy: The role of receptor activator of nuclear factor-kappaB ligand. Diabetologia 2008, 51, 1035–1040. [Google Scholar] [CrossRef] [Green Version]
- Pitocco, D.; Scavone, G.; Di Leo, M.; Vitiello, R.; Rizzi, A.; Tartaglione, L.; Costantini, F.; Flex, A.; Galli, M.; Caputo, S.; et al. Charcot Neuroarthropathy: From the Laboratory to the Bedside. Curr. Diabetes Rev. 2019, 16, 62–72. [Google Scholar] [CrossRef]
- Das, L.; Rastogi, A.; Jude, E.B.; Prakash, M.; Dutta, P.; Bhansali, A. Long-term foot outcomes following differential abatement of inflammation and osteoclastogenesis for active Charcot neuroarthropathy in diabetes mellitus. PLoS ONE 2021, 16, e0259224. [Google Scholar] [CrossRef]
- Folestad, A.; Ålund, M.; Asteberg, S.; Fowelin, J.; Aurell, Y.; Göthlin, J.; Cassuto, J. Role of Wnt/β-catenin and RANKL/OPG in bone healing of diabetic Charcot arthropathy patients. Acta Orthop. 2015, 86, 415–425. [Google Scholar] [CrossRef] [Green Version]
- Gaudio, A.; Privitera, F.; Pulvirenti, I.; Canzonieri, E.; Rapisarda, R.; Fiore, C.E. The relationship between inhibitors of the Wnt signalling pathway (sclerostin and Dickkopf-1) and carotid intima-media thickness in postmenopausal women with type 2 diabetes Mellitus. Diabetes Vasc. Dis. Res. 2014, 11, 48–52. [Google Scholar] [CrossRef]
- Agholme, F.; Li, X.; Isaksson, H.; Ke, H.Z.; Aspenberg, P. Sclerostin antibody treatment enhances metaphyseal bone healing in rats. J. Bone Miner. Res. 2010, 25, 2412–2418. [Google Scholar] [CrossRef] [PubMed]
- Agholme, F.; Macias, B.; Hamang, M.; Lucchesi, J.; Adrian, M.D.; Kuhstoss, S.; Harvey, A.; Sato, M.; Aspenberg, P. Efficacy of a sclerostin antibody compared to a low dose of PTH on metaphyseal bone healing. J. Orthop. Res. 2014, 32, 471–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molligan, J.; Barr, C.; Mitchell, R.; Schon, L.; Zhang, Z. Pathological role of fibroblast-like synoviocytes in Charcot neuroarthropathy. J. Orthop. Res. 2016, 34, 224–230. [Google Scholar] [CrossRef] [PubMed]
- la Fontaine, J.; Shibuya, N.; Sampson, H.W.; Valderrama, P. Trabecular Quality and Cellular Characteristics of Normal, Diabetic, and Charcot Bone. J. Foot Ankle Surg. 2011, 50, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Koeck, F.-X.; Bobrik, V.; Fassold, A.; Grifka, J.; Kessler, S.; Straub, R.H. Marked loss of sympathetic nerve fibers in chronic Charcot foot of diabetic origin compared to ankle joint osteoarthritis. J. Orthop. Res. 2009, 27, 736–741. [Google Scholar] [CrossRef] [PubMed]
- Schon, L.C.; Mitchell, R.; Zahoor, T.A.; Zhang, Z. Distribution of Neuropeptides in the Synovium of Charcot Neuroarthropathy. Foot Ankle Orthop. 2016, 1, 2473011416S0016. [Google Scholar] [CrossRef]
- la Fontaine, J.; Harkless, L.B.; Sylvia, V.L.; Carnes, D.; Heim-Hall, J.; Jude, E. Levels of Endothelial Nitric Oxide Synthase and Calcitonin Gene-Related Peptide in the Charcot Foot: A Pilot Study. J. Foot Ankle Surg. 2008, 47, 424–429. [Google Scholar] [CrossRef]
- Tan, S.D.; Bakker, A.D.; Semeins, C.M.; Kuijpers-Jagtman, A.M.; Klein-Nulend, J. Inhibition of osteocyte apoptosis by fluid flow is mediated by nitric oxide. Biochem. Biophys. Res. Commun. 2008, 369, 1150–1154. [Google Scholar] [CrossRef]
- Imai, S.; Matsusue, Y. Neuronal regulation of bone metabolism and anabolism: Calcitonin gene-related peptide-, substance P-, and tyrosine hydroxylase-containing nerves and the bone. Microsc. Res. Tech. 2002, 58, 61–69. [Google Scholar] [CrossRef]
- Kaynak, G.; Birsel, O.; Güven, M.F.; Öğüt, T. An overview of the Charcot foot pathophysiology. Diabet. Foot Ankle 2013, 4, 21117. [Google Scholar] [CrossRef] [Green Version]
- Connors, J.C.; Hardy, M.A.; Kishman, L.L.; Botek, G.G.; Verdin, C.J.; Rao, N.M.; Kingsley, J.D. Charcot Pathogenesis: A Study of In Vivo Gene Expression. J. Foot Ankle Surg. 2018, 57, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, D.E.; Mustăţea, P.; Mihalache, O.; Bobircă, F.; Agache, A.; Georgescu, T.F.; Chiriac, O.; Marin, V.; Doran, H.; Pătraşcu, T. Surgical Management of Diabetic Neuropathy Foot Complications. Chirurgia 2018, 113, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Petrova, N.L.; Edmonds, M.E. Pathogenesis of Charcot Neuroarthropathy and Acute Management. In The Foot in Diabetes; Wiley: New York, NY, USA, 2020; pp. 311–321. [Google Scholar] [CrossRef]
- Mrozikiewicz-Rakowska, B.; Nehring, P.; Szymański, K.; Sobczyk-Kopcioł, A.; Płoski, R.; Drygas, W.; Krzymień, J.; Acharya, N.A.; Czupryniak, L.; Przybyłkowski, A. Selected RANKL/RANK/OPG system genetic variants in diabetic foot patients. J. Diabetes Metab. Disord. 2018, 17, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Dardari, D. An overview of Charcot’s neuroarthropathy. J. Clin. Transl. Endocrinol. 2020, 22, 100239. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.B.; Christensen, T.M.; Bülow, J.; Rørdam, L.; Holstein, P.E.; Jørgensen, N.R.; Svendsen, O.L. Bone mineral density and markers of bone turnover and inflammation in diabetes patients with or without a Charcot’s foot: An 8.5-year prospective case-control study. J. Diabetes Complicat. 2018, 32, 164–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uccioli, L.; Sinistro, A.; Almerighi, C.; Ciaprini, C.; Cavazza, A.; Giurato, L.; Ruotolo, V.; Spasaro, F.; Vainieri, E.; Rocchi, G.; et al. Proinflammatory Modulation of the Surface and Cytokine Phenotype of Monocytes in Patients with Acute Charcot Foot. Diabetes Care 2010, 33, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Mabilleau, G.; Petrova, N.; Edmonds, M.E.; Sabokbar, A. Number of Circulating CD14-Positive Cells and the Serum Levels of TNF-α Are Raised in Acute Charcot Foot. Diabetes Care 2011, 34, e33. [Google Scholar] [CrossRef] [Green Version]
- Bruhn-Olszewska, B.; Korzon-Burakowska, A.; Węgrzyn, G.; Jakóbkiewicz-Banecka, J. Prevalence of polymorphisms in OPG, RANKL and RANK as potential markers for Charcot arthropathy development. Sci. Rep. 2017, 7, 501. [Google Scholar] [CrossRef] [Green Version]
- SaiPrathiba, A.; Senthil, G.; Juttada, U.; Selvaraj, B.; Kumpatla, S.; Viswanathan, V. RANKL Gene Polymorphism as a Potential Biomarker to Identify Acute Charcot Foot Among Indian Population with Type 2 Diabetes: A Preliminary Report. Int. J. Low Extrem. Wounds 2019, 18, 287–293. [Google Scholar] [CrossRef]
- Hingsammer, A.M.; Bauer, D.; Renner, N.; Borbas, P.; Boeni, T.; Berli, M. Correlation of Systemic Inflammatory Markers with Radiographic Stages of Charcot Osteoarthropathy. Foot Ankle Int. 2016, 37, 924–928. [Google Scholar] [CrossRef]
- Sinacore, D.R.; Bohnert, K.L.; Smith, K.E.; Hastings, M.K.; Commean, P.K.; Gutekunst, D.J.; Johnson, J.E.; Prior, F.W. Persistent inflammation with pedal osteolysis 1year after Charcot neuropathic osteoarthropathy. J. Diabetes Complicat. 2017, 31, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Jude, E.B.; Selby, P.; Burgess, J.; Lilleystone, P.; Mawer, E.B.; Page, S.R.; Donohoe, M.; Foster, A.V.M.; Edmonds, M.E.; Boulton, A.J.M. Bisphosphonates in the treatment of Charcot neuroarthropathy: A double-blind randomized controlled trial. Diabetologia 2001, 44, 2032–2037. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, P.; Pitocco, D.; Zaccardi, F.; Di Stasio, E.; Strollo, R.; Rizzi, A.; Scavone, G.; Costantini, F.; Galli, M.; Tinelli, G.; et al. Autoantibodies to post-translationally modified type I and II collagen in Charcot neuroarthropathy in subjects with type 2 diabetes Mellitus. Diabetes Metab. Res. Rev. 2017, 33, e2839. [Google Scholar] [CrossRef] [PubMed]
- Pasquier, J.; Spurgeon, M.; Bradic, M.; Thomas, B.; Robay, A.; Chidiac, O.; Dib, M.-J.; Turjoman, R.; Liberska, A.; Staudt, M.; et al. Whole-methylome analysis of circulating monocytes in acute diabetic Charcot foot reveals differentially methylated genes involved in the formation of osteoclasts. Epigenomics 2019, 11, 281–296. [Google Scholar] [CrossRef] [PubMed]
- Jirkovská, A.; Kasalický, P.; Bouček, P.; Hosová, J.; Skibová, J. Calcaneal ultrasonometry in patients with Charcot osteoarthropathy and its relationship with densitometry in the lumbar spine and femoral neck and with markers of bone turnover. Diabet. Med. 2001, 18, 495–500. [Google Scholar] [CrossRef]
- Yates, T.H.; Cooperman, S.R.; Shofler, D.; Agrawal, D.K. Current concepts underlying the pathophysiology of acute Charcot neuroarthropathy in the diabetic foot and ankle. Expert Rev. Clin. Immunol. 2020, 16, 839–845. [Google Scholar] [CrossRef]
- Commean, P.K.; Smith, K.E.; Hildebolt, C.F.; Bohnert, K.L.; Sinacore, D.R.; Prior, F.W. A Candidate Imaging Marker for Early Detection of Charcot Neuroarthropathy. J. Clin. Densitom. 2018, 21, 485–492. [Google Scholar] [CrossRef]
- Herlyn, A.; Prakasam, R.K.; Peschel, S.; Allgeier, S.; Köhler, B.; Winter, K.; Guthoff, R.F.; Mittlmeier, T.; Stachs, O. Corneal Subbasal Nerve Plexus Changes in Severe Diabetic Charcot Foot Deformity: A Pilot Study in Search for a DNOAP Biomarker. J. Diabetes Res. 2018, 2018, 5910639. [Google Scholar] [CrossRef]
- Ochinciuc, R.; Ochinciuc, U.; Stanca, H.T.; Barac, R.; Darabus, D.; Şuţă, M.; Baltă, F.; Burcea, M. Photoreceptor assessment in focal laser-treated central serous chorioretinopathy using adaptive optics and fundus autofluorescence. Medicine 2020, 99, e19536. [Google Scholar] [CrossRef]
- Hartmannsberger, B.; Doppler, K.; Stauber, J.; Schlotter-Weigel, B.; Young, P.; Sereda, M.W.; Sommer, C. Intraepidermal nerve fibre density as biomarker in Charcot–Marie–Tooth disease type 1A. Brain Commun. 2020, 2, fcaa012. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IL-1 β | IL-6 | TNF-α | RANKL | OPG | AGE | fsRANKL | sRAGE | fsRANKL/OPG Ratio | C-RP | ESR | WCC | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Schmidt et al. [3] | ↑ | ↑ | ↑ | ↑ | ↑ | ↑ | ||||||
| Molines et al. [12] | ↑ | ↑ | ↑ | ↑ | ||||||||
| Jansen et al. [15] | Δ value: 10.04 pg/mL, p = 0.049 | No difference | No difference | Δ value: 2.5 ng/mL, p = 0.002 | ||||||||
| Petrova et al. [16] | 0.27 vs. 0.2 vs. 0.18, p = 0.254 | 3.3 vs. 2 vs. 1.4, p = 0.002 | 1.3 vs. 1 vs. 0.8, p = 0.01 | 0.29 vs. 0.41 vs. 0.13, p = 0.915 | 5.4 vs. 4.4 vs. 2.9, p < 0.001 | 5.4 vs. 3.7 vs. 0.8, p = 0.007 | ||||||
| Jansen et al. [37] | 5.93 vs. 7.71, p = 0.812 | 0.04 vs. 0.68, p = 0.002 | 1593 vs. 399, p = 0.005 | (−2.9 vs. −0.1, p = 0.046 | ||||||||
| Uccioli et al. [38] | 0.6 ± 0.3 vs. <0.125, p < 0.005 | 15.3 ± 7.4 vs. 6.7 ± 3.5, p < 0.05 | 5.2 ± 3.2 vs. 2.6 ± 1.2, p < 0.05 | ↑, p < 0.001 | ||||||||
| Mabilleau et al. [39] | 4.3 ± 0.9 vs. 1.93 ± 0.8, p = 0.009 | |||||||||||
| Bruhn-Olszewska et al. [40] | 1.01 ± 1.45 vs. 2.66 ± 1.74 vs. 0.5 ± 0.43 pmol/L, p < 0.001 | 7.36 ± 4.1 vs. 6.29 ± 1.68 vs. 4.77 ± 2.38 pmol/L, p < 0.001 | ↑ | |||||||||
| Folestad et al. [20] | ↑, p = 0.004 | ↑, p < 0.001 | ↔ | |||||||||
| SaiPrathiba et al. [41] | 8.9 vs. 7.4 vs. 5.12 ng/mL, p = 0.008 | |||||||||||
| Hingsammer et al. [42] | 34.7 vs. 9.5 mg/L, p = 0.01 | 25.9 vs. 18.3 mm/h, p = 0.02 | 11.8 vs. 8.2 109/L, p = 0.01 | |||||||||
| Petrova et al. [43] | 5.8 (5–11) vs. ≤5 mg/L | ↑ | normal | |||||||||
| Jude et al. [44] | No difference | No difference |
| X | Osteocalcin | C-Terminal Telopeptide | b-ALP | Tartrate-Resistant Acid Phosphatase | |
|---|---|---|---|---|---|
| Petrova et al. [16] | 0.24 vs. 0.12 vs. 0.15 μg/L, p = 0.004 | 16.4 vs. 13.6 vs. 10.1 μg/L, p = 0.006 | 3.9 vs. 3.9 vs. 2.7 UI/L, p = 0.126 | ||
| Jansen et al. [37] | 387 ± 136 vs. 95 ± 83 ng/L, p < 0.001 | 16.9 ± 5.7 vs. 14.7 ± 11.5 μg/L, p = 0.153 | |||
| Jirkovská et al. [47] | ↓, p < 0.03 |
| Total Hip BMD | L2-L4 BMD | Calcaneal BMD | Femoral Neck BMD | Sclerostin | Dkk-1 | Wnt-1 | Wif-1 | |
|---|---|---|---|---|---|---|---|---|
| Folestad et al. [20] | ↑ | ↑ | ↑ | ↑ | ||||
| Jansen et al. [37] | ↔, p = 0.294 | +0.036 g/cm2 (+2.9%) vs. +0.125 g/cm2 (+10.1%) | ||||||
| Jirkovská et al. [47] | −0.57 ± 1.28 vs. −0.91 ± 0.84, p > 0.05 | −3.00 ± 1.39 vs ±2.36 ± 1.12; p < 0.01 | −1.58 ± 1.24 vs. −0.76 ± 0.98, p < 0.05 | |||||
| Christensen et al. [48] | ↓, p < 0.01 |
| Common Biomarkers | Novel Biomarkers |
|---|---|
| C-RP [15,16,43,44] | RANKL [20,35,40,41] |
| ESR [3,42,43,44] | OPG [20,35] |
| WCC [3,18] | AGE [3,15,37] |
| IL-1 β [12,16,38] | fsRANKL [15,16,37] |
| IL-6 [12,15,16,37,38] | sRAGE [15,37] |
| TNF-α [16,24,38,39] | Osteocalcin [15,37] |
| C-terminal telopeptide [16] | |
| b-ALP [16,44,47] | |
| Tartrate-resistant acid phosphatase [16] | |
| Sclerostin [20,21,22,23] | |
| Dkk-1 [20,21,22,23] | |
| Wnt-1 [20,21,22,23] | |
| Wif-1 [20,21,22,23] | |
| Total hip BMD [37,45] | |
| L2-L4 BMD [37,47] | |
| Calcaneal BMD [37,38,47,48] | |
| Femoral neck BMD [47,48,49] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bobircă, A.; Musetescu, A.E.; Bordianu, A.; Pantea Stoian, A.; Salmen, T.; Marinescu, D.-C.; Alexandru, C.; Florescu, A.; Radu, R.; Isac, S.; et al. Novel Biomarkers Predictive of Diabetic Charcot Foot—An Overview of the Literature. Life 2022, 12, 1944. https://doi.org/10.3390/life12111944
Bobircă A, Musetescu AE, Bordianu A, Pantea Stoian A, Salmen T, Marinescu D-C, Alexandru C, Florescu A, Radu R, Isac S, et al. Novel Biomarkers Predictive of Diabetic Charcot Foot—An Overview of the Literature. Life. 2022; 12(11):1944. https://doi.org/10.3390/life12111944
Chicago/Turabian StyleBobircă, Anca, Anca Emanuela Musetescu, Anca Bordianu, Anca Pantea Stoian, Teodor Salmen, Dan-Cristian Marinescu, Cristina Alexandru, Alesandra Florescu, Raluca Radu, Sebastian Isac, and et al. 2022. "Novel Biomarkers Predictive of Diabetic Charcot Foot—An Overview of the Literature" Life 12, no. 11: 1944. https://doi.org/10.3390/life12111944