
Artificial Intelligence as an Aid in CBCT Airway Analysis: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
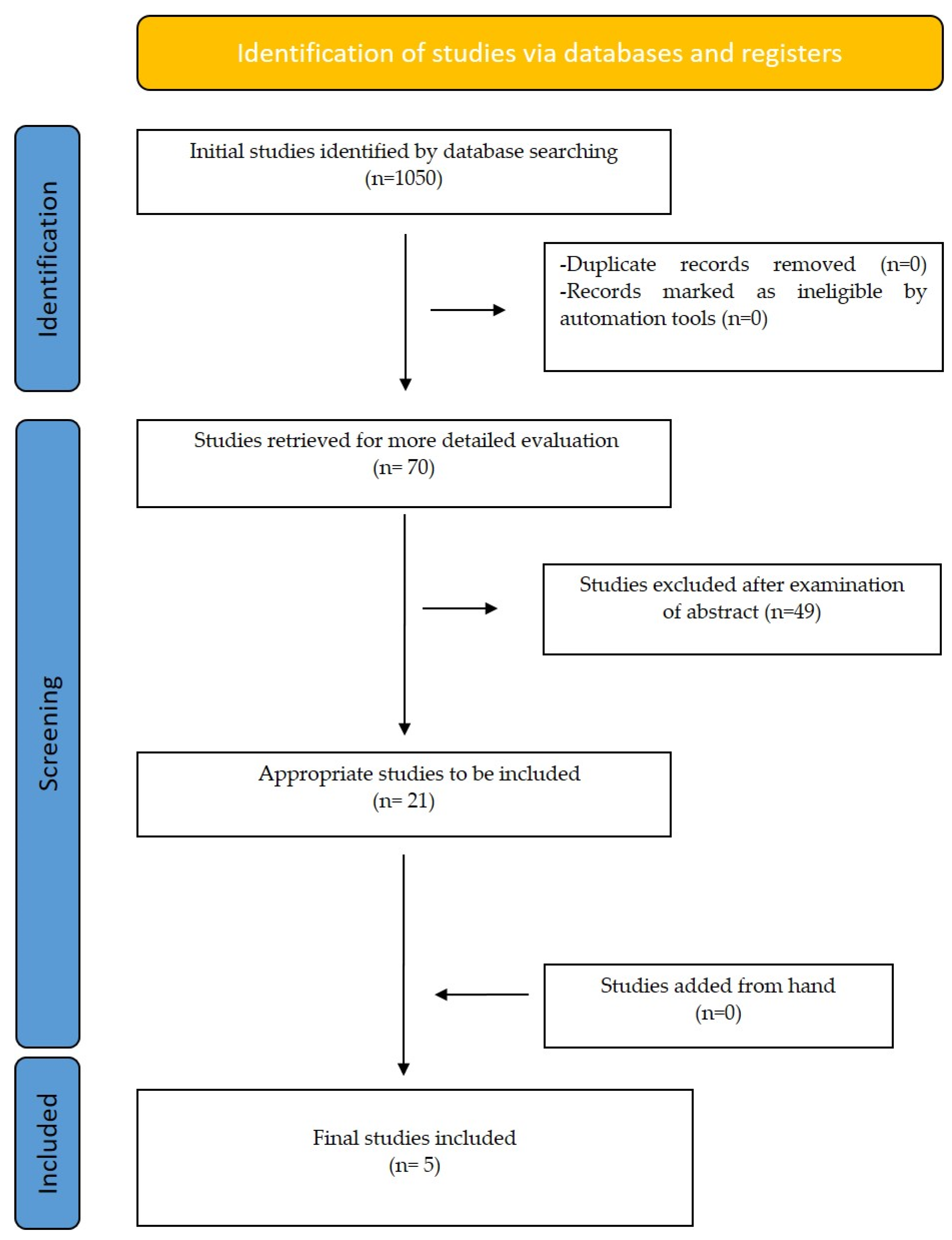
2. Materials and Methods
2.1. Protocol and Registration
2.2. Data Items and Collection Extraction and Management
2.3. Risk of Bias/Quality Assessment in Individual Studies
- Low risk of bias if all key domains of the study were at low risk of bias.
- Unclear risk of bias if one or more key domains of the study were unclear.
- High risk of bias if one or more key domains were at high risk of bias.
3. Results
Risk of Bias within Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thurzo, A.; Urbanová, W.; Novák, B.; Czako, L.; Siebert, T.; Stano, P.; Mareková, S.; Fountoulaki, G.; Kosnáčová, H.; Varga, I. Where Is the Artificial Intelligence Applied in Dentistry? Systematic Review and Literature Analysis. Healthcare 2022, 10, 1269. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.A.; Gizani, S.; Panayi, N.; Antonopoulos, G.; Tsolakis, A.I. Three-Dimensional Printing Technology in Orthodontics for Dental Models: A Systematic Review. Children 2022, 9, 1106. [Google Scholar] [CrossRef] [PubMed]
- Tsolakis, I.A.; Gizani, S.; Tsolakis, A.I.; Panayi, N. Three-Dimensional-Printed Customized Orthodontic and Pedodontic Appliances: A Critical Review of a New Era for Treatment. Children 2022, 9, 1107. [Google Scholar] [CrossRef] [PubMed]
- Obermeyer, Z.; Emanuel, E.J. Predicting the Future—Big Data, Machine Learning, and Clinical Medicine. N. Engl. J. Med. 2016, 375, 1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gharavi, S.M.H.; Faghihimehr, A. Clinical Application of Artificial Intelligence in PET Imaging of Head and Neck Cancer. PET Clin. 2022, 17, 65–76. [Google Scholar] [CrossRef]
- Patil, S.; Albogami, S.; Hosmani, J.; Mujoo, S.; Kamil, M.A.; Mansour, M.A.; Abdul, H.N.; Bhandi, S.; Ahmed, S.S.S.J. Artificial Intelligence in the Diagnosis of Oral Diseases: Applications and Pitfalls. Diagnostics 2022, 12, 1029. [Google Scholar] [CrossRef]
- Rasteau, S.; Ernenwein, D.; Savoldelli, C.; Bouletreau, P. Artificial Intelligence for Oral and Maxillo-Facial Surgery: A Narrative Review. J. Stomatol. Oral Maxillofac. Surg. 2022, 123, 276–282. [Google Scholar] [CrossRef]
- Monterubbianesi, R.; Tosco, V.; Vitiello, F.; Orilisi, G.; Fraccastoro, F.; Putignano, A.; Orsini, G. Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges. Appl. Sci. 2022, 12, 877. [Google Scholar] [CrossRef]
- Oshida, Y. Artificial Intelligence for Medicine. Artif. Intell. Med. 2021, 69, S36–S40. [Google Scholar]
- Obermeyer, Z.; Powers, B.; Vogeli, C.; Mullainathan, S. Dissecting Racial Bias in an Algorithm Used to Manage the Health of Populations. Science 2019, 366, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Weng, Y.; Lund, J.; Faust, O.; Su, L.; Acharya, R. Applications of Explainable Artificial Intelligence in Diagnosis andSurgery. Diagnostics 2022, 12, 237. [Google Scholar] [CrossRef] [PubMed]
- Kavya, R.; Christopher, J.; Panda, S.; Lazarus, Y.B. Machine Learning and XAI Approaches for Allergy Diagnosis. Biomed. Signal Process. Control 2021, 69, 102681. [Google Scholar] [CrossRef]
- Barredo Arrieta, A.; Díaz-Rodríguez, N.; del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; Garcia, S.; Gil-Lopez, S.; Molina, D.; Benjamins, R.; et al. Explainable Artificial Intelligence (XAI): Concepts, Taxonomies, Opportunities and Challenges toward Responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef] [Green Version]
- Di Carlo, G.; Polimeni, A.; Melsen, B.; Cattaneo, P.M. The relationship between upper airways and craniofacial morphology studied in 3D. A CBCT study. Orthod. Craniofac. Res. 2015, 18, 1–11. [Google Scholar] [CrossRef]
- Schendel, S.A.; Jacobson, R.; Khalessi, S. Airway growth and development: A computerized 3-dimensional analysis. J. Oral Maxillofac. Surg. 2012, 70, 2174–2183. [Google Scholar] [CrossRef]
- Claudino, L.V.; Mattos, C.T.; Ruellas, A.C.D.O.; Sant Anna, E.F. Pharyngeal airway characterization in adolescents related to facial skeletal pattern: A preliminary study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 799–809. [Google Scholar] [CrossRef]
- Zheng, Z.H.; Yamaguchi, T.; Kurihara, A.; Li, H.F.; Maki, K. Three-dimensional evaluation of upper airway in patients with different anteroposterior skeletal patterns. Orthod. Craniofac. Res. 2014, 17, 38–48. [Google Scholar] [CrossRef]
- Celikoglu, M.; Bayram, M.; Sekerci, A.E.; Buyuk, S.K.; Toy, E. Comparison of pharyngeal airway volume among different vertical skeletal patterns: A cone-beam computed tomography study. Angle Orthod. 2014, 84, 782–787. [Google Scholar] [CrossRef] [Green Version]
- Tsolakis, I.A.; Palomo, J.M.; Matthaios, S.; Tsolakis, A.I. Dental and Skeletal Side Effects of Oral Appliances Used for the Treatment of Obstructive Sleep Apnea and Snoring in Adult Patients—A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 483. [Google Scholar] [CrossRef]
- Pereira-Filho, V.A.; Castro-Silva, L.M.; De Moraes, M.; Gabrielli, M.F.R.; Campos, J.A.D.B.; Juergens, P. Cephalometric evaluation of pharyngeal airway space changes in class III patients undergoing orthognathic surgery. J. Oral Maxillofac. Surg. 2011, 69, e409–e415. [Google Scholar] [CrossRef]
- Gungor, A.Y.; Turkkahraman, H.; Yilmaz, H.H.; Yariktas, M. Cephalometric comparison of obstructive sleep apnea patients and healthy controls. Eur. J. Dent. 2013, 7, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Aboudara, C.; Nielsen, I.; Huang, J.C.; Maki, K.; Miller, A.J.; Hatcher, D. Comparison of airway space with conventional lateral headfilms and 3-dimensional reconstruction from cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 468–479. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Wang, Y.; Hu, H.; Liao, Q.; Zhang, W.; Xiang, X.; Fan, X. Impact on the upper airway space of different types of orthognathic surgery for the correction of skeletal class III malocclusion: A systematic review and meta-analysis. Int. J. Surg. 2017, 38, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Alsufyani, N.A.; Noga, M.L.; Witmans, M.; Major, P.W. Upper airway imaging in sleep-disordered breathing: Role of cone-beam computed tomography. Oral Radiol. 2017, 33, 161–169. [Google Scholar] [CrossRef]
- Tsolakis, I.A.; Venkat, D.; Hans, M.G.; Alonso, A.; Palomo, J.M. When static meets dynamic: Comparing cone-beam computed tomography and acoustic reflection for upper airway analysis. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 643–650. [Google Scholar] [CrossRef]
- Leonardi, R.; Lo Giudice, A.; Farronato, M.; Ronsivalle, V.; Allegrini, S.; Musumeci, G.; Spampinato, C. Fully automatic segmentation of sinonasal cavity and pharyngeal airway based on convolutional neural networks. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 824–835.e1. [Google Scholar] [CrossRef]
- Park, J.; Hwang, J.; Ryu, J.; Nam, I.; Kim, S.-A.; Cho, B.-H.; Shin, S.-H.; Lee, J.-Y. Deep Learning Based Airway Segmentation Using Key Point Prediction. Appl. Sci. 2021, 11, 3501. [Google Scholar] [CrossRef]
- Shujaat, S.; Jazil, O.; Willems, H.; Van Gerven, A.; Shaheen, E.; Politis, C.; Jacobs, R. Automatic segmentation of the pharyngeal airway space with convolutional neural network. J. Dent. 2021, 111, 103705. [Google Scholar] [CrossRef]
- Sin, Ç.; Akkaya, N.; Aksoy, S.; Orhan, K.; Öz, U. A deep learning algorithm proposal to automatic pharyngeal airway detection and segmentation on CBCT images. Orthod. Craniofac. Res. 2021, 24, 117–123. [Google Scholar] [CrossRef]
- Orhan, K.; Shamshiev, M.; Ezhov, M.; Plaksin, A.; Kurbanova, A.; Ünsal, G.; Gusarev, M.; Golitsyna, M.; Aksoy, S.; Mısırlı, M.; et al. AI-based automatic segmentation of craniomaxillofacial anatomy from CBCT scans for automatic detection of pharyngeal airway evaluations in OSA patients. Sci. Rep. 2022, 12, 118. [Google Scholar] [CrossRef]
- El Khateeb, S. Three-dimensional image segmentation of upper airway by cone beam CT: A review of literature. Egypt. Dent. J. 2020, 66, 1527–1535. [Google Scholar] [CrossRef]
- De Menezes Weissheimer, L.M.E.; Sameshima, G.T.; Enciso, R.; Pham, J.; Grauer, D. Imaging software accuracy for 3-dimensional analysis of the upper airway. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 801–813. [Google Scholar] [CrossRef]
- Lenza, M.G.; Lenza, M.D.O.; Dalstra, M.; Melsen, B.; Cattaneo, P.M. An analysis of different approaches to the assessment of upper airway morphology: A CBCT study. Orthod. Craniofacial Res. 2010, 13, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.; Baratieri, C.; Mattos, C.T.; Brunetto, D.; Fontes, R.D.C.; Santos, J.R.L.; Ruellas, A.C.D.O. Is the airway volume being correctly analyzed? Am. J. Orthod. Dentofac. Orthop. 2012, 141, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Van Eijnatten, M.; Koivisto, J.; Karhu, K.; Forouzanfar, T.; Wolff, J. The impact of manual threshold selection in medical additive manufacturing. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 607–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minnema, J.; van Eijnatten, M.; Kouw, W.; Diblen, F.; Mendrik, A.; Wolff, J. CT image segmentation of bone for medical additive manufacturing using a convolutional neural network. Comput. Biol. Med. 2018, 103, 130–139. [Google Scholar] [CrossRef] [Green Version]
- ElShebiny, T.; Morcos, S.; El, H.; Palomo, J.M. Comparing different software packages for measuring the oropharynx and minimum cross-sectional area. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 228–237.e32. [Google Scholar] [CrossRef]
- Shi, H.; Scarfe, W.C.; Farman, A.G. Upper airway segmentation and dimensions estimation from cone-beam CT image datasets. Int. J. Comput. Assist. Radiol. Surg. 2006, 1, 177–186. [Google Scholar] [CrossRef]
- Alsufyani, N.A.; Hess, A.; Noga, M.; Ray, N.; Al-Saleh, M.A.Q.; Lagrav‘ere, M.O.; Major, P.W. New algorithm for semiautomatic segmentation of nasal cavity and pharyngeal airway in comparison with manual segmentation using cone-beam computed tomography. Am. J. Orthod. Dentofac. Orthop. 2016, 150, 703–712. [Google Scholar] [CrossRef] [Green Version]
- Neelapu, B.C.; Kharbanda, O.P.; Sardana, V.; Gupta, A.; Vasamsetti, S.; Balachandran, R.; Rana, S.S.; Sardana, H.K. A pilot study for segmentation of pharyngeal and sino-nasal airway subregions by automatic contour initialization. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 1877–1893. [Google Scholar] [CrossRef]


{kind=link}
| “Cone-Beam Computed Tomography” [Mesh] AND airway volume | 330 results |
| “Cone-Beam Computed Tomography” [Mesh] AND Artificial Intelligence” [Mesh] | 257 results |
| Artificial Intelligence” [Mesh] AND airway volume | 76 results |
| “Cone-Beam Computed Tomography” [Mesh] AND Artificial Intelligence” [Mesh] AND airway volume | 4 results |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Studies that refer to the use of artificial intelligence for CBCT airway analysis | Studies that are reviews or authors’ opinion |
| prospective or retrospective studies |
| Authors/ Publication Year | Study Design | Participants (Number of CBCT) | Intervention | Outcomes | Method of Outcome Assessment | Results | Authors/ Publication Year |
|---|---|---|---|---|---|---|---|
| Leonardi R et al. [26] (2021) | prospective | 40 CBCT scans | 1 CBCT device was used. | Accuracy of the CNN fully automatic segmentation of the sinonasal cavity pharyngeal airway |
|
| The new deep learning–based method for automated segmentation is accurate for airway segmentation |
| Park et al. [27] | prospective | 315 CBCT scans | 1 CBCT device was used. | Accuracy of the airway volume measurement by a Regression Neural Network-based deep-learning model |
|
| These results indicate that fully automatic segmentation of the airway is possible by training via deep learning of artificial intelligence. |
| Shujaat S et al. [28] (2021) | prospective | 103 CT and CBCT scans | Scans from 1 CT and 2 CBCTs were grouped in:
| The performance of deep learning based 3D CNN model for automatic segmentation of the pharyngeal airway space |
|
| The proposed 3D U-Net model offered an accurate method for the segmentation of Airway from CT/CBCT images. |
| Sin Ç et al. [29] (2021) | prospective | 306 CBCT scans | 1 CBCT device was used and grouped in:
| The accuracy of an automatic detection algorithm for pharyngeal airway on CBCT images using a deep-learning artificial intelligence system |
version 3.8 ITK SNAP software
of U-Net and SGD Adam optimizer. |
| AI models based on deep learning techniques can be used for easy and error-free segmentation of pharyngeal airway volume from CBCT |
| Orhan K et al. [30] (2022) | prospective | 200 CBCT scans | 3 CBCT devices | To validate an automatic detection algorithm for pharyngeal airway on CBCT data using an AI software for OSA patients To validate the newly developed artificial intelligence system in comparison to commercially available software for 3D CBCT evaluation. |
|
| Activating this potential collaboration for OSA patients would significantly reduce the effort and time required for the initial diagnosis and follow-up of these patients. |
| Author (Year) | Outcomes | Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Measurement of Interventions | Bias Due to Departures from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|---|---|---|
| Leonardi R et al. [26] (2021) |
| Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | High for all outcomes | Low for all outcomes | High for all outcomes |
| Park et al. [27] (2021) |
| Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | High for all outcomes | Low for all outcomes | High for all outcomes |
| Shujaat S et al. [28] (2021) |
| Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes |
| Sin Ç et al. [29] (2021) |
| Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes |
| Orhan K et al. [30] (2022) |
| Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes | Low for all outcomes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsolakis, I.A.; Kolokitha, O.-E.; Papadopoulou, E.; Tsolakis, A.I.; Kilipiris, E.G.; Palomo, J.M. Artificial Intelligence as an Aid in CBCT Airway Analysis: A Systematic Review. Life 2022, 12, 1894. https://doi.org/10.3390/life12111894
Tsolakis IA, Kolokitha O-E, Papadopoulou E, Tsolakis AI, Kilipiris EG, Palomo JM. Artificial Intelligence as an Aid in CBCT Airway Analysis: A Systematic Review. Life. 2022; 12(11):1894. https://doi.org/10.3390/life12111894
Chicago/Turabian StyleTsolakis, Ioannis A., Olga-Elpis Kolokitha, Erofili Papadopoulou, Apostolos I. Tsolakis, Evangelos G. Kilipiris, and J. Martin Palomo. 2022. "Artificial Intelligence as an Aid in CBCT Airway Analysis: A Systematic Review" Life 12, no. 11: 1894. https://doi.org/10.3390/life12111894