
Genital Microbiota and Outcome of Assisted Reproductive Treatment—A Systematic Review

Abstract
:1. Introduction
1.1. Microscopy and Culture-Based Methods
1.2. Quantitative Polymerase Chain Reaction (qPCR)
1.3. Next-Generation Sequencing (NGS)
1.4. Whole Genome Sequencing (WGS)
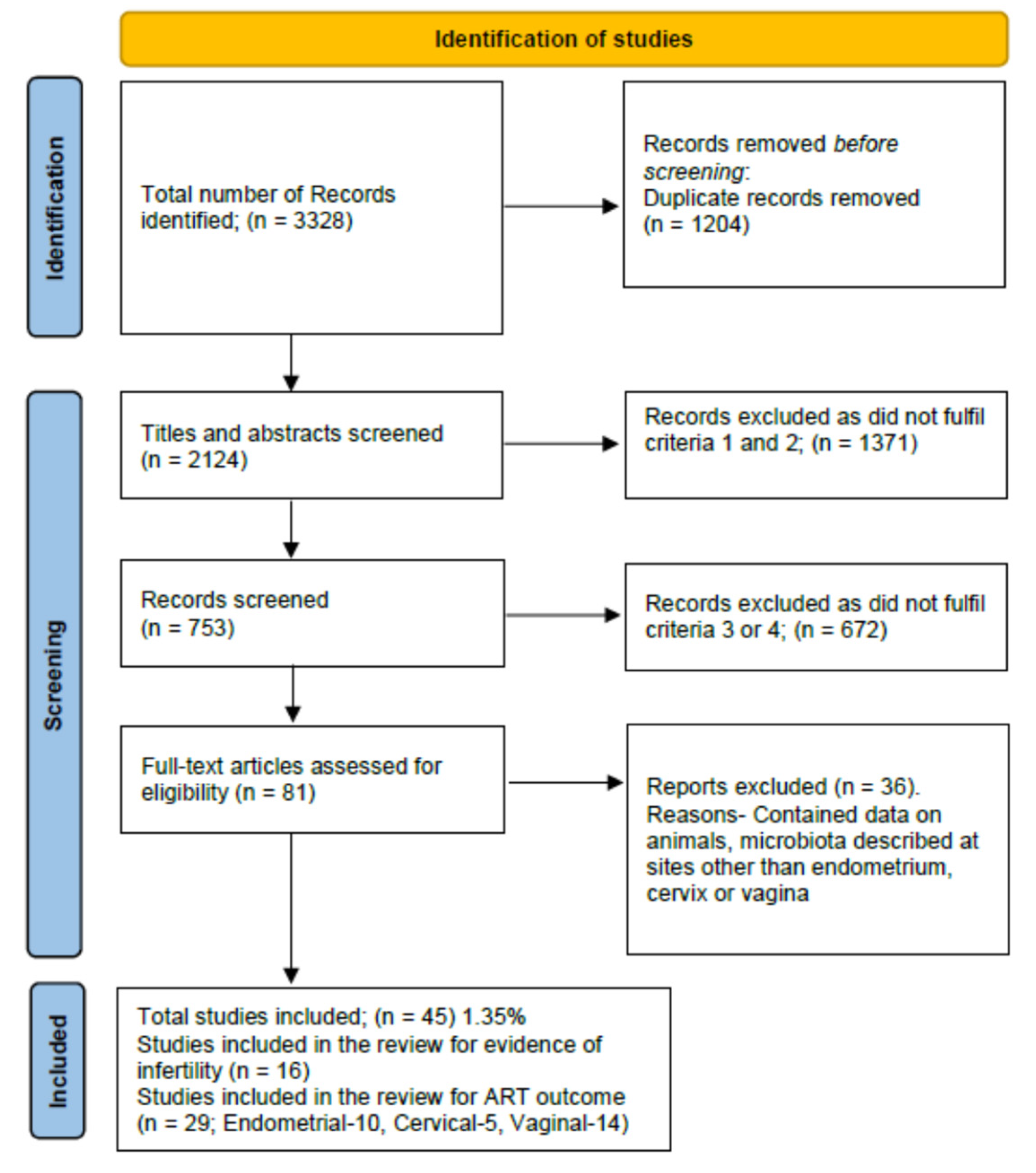
2. Materials and Methods
- Women or couples with infertility regardless of the cause or non-pregnant women planning for pregnancy.
- Studies where the microbial assessment of the genital tract was carried out.
- Studies where a comparison of the microbiome was available between fertile and infertile women.
- Studies where a comparison of the microbial flora was available between women with ART/IVF success and failure.
3. Results
3.1. Genital Microbiota and Association with Infertility
3.2. Endometrial Microbiota (EM) and ART Outcome
3.3. Cervical Microbiota and Art Outcome
3.4. Vaginal Microbiota and IVF Outcome
4. Discussion
4.1. Association with Infertility
4.2. Microbiota and ART Outcomes
4.2.1. Richness and Diversity of Species
4.2.2. Lactobacillus Species and ART Outcomes
- (a)
- Pregnancy Rate
- (b)
- Live Birth Rate
- (c)
- Miscarriage Rate
4.2.3. Presence of Other Species and ART Outcomes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sender, R.; Fuchs, S.; Milo, R. Revised Estimates for the Number of Human and Bacteria Cells in the Body. PLOS Biol. 2016, 14, e1002533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchesi, J.R.; Ravel, J. The vocabulary of microbiome research: A proposal. Microbiome 2015, 3, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, I.; Blaser, M.J. The human microbiome: At the interface of health and disease. Nat. Rev. Genet. 2012, 13, 260–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ursell, L.K.; Metcalf, J.L.; Parfrey, L.W.; Knight, R. Defining the human microbiome. Nutr. Rev. 2012, 70 (Suppl. S1), S38–S44. [Google Scholar] [CrossRef] [Green Version]
- Hok, T.T.; Loen, L.K.; Tjiat, N.T. Comparative bacteriology of the endocervical mucus. Am. J. Obstet. Gynecol. 1967, 98, 781–783. [Google Scholar] [CrossRef]
- Huttenhower, C.; Gevers, D.; Knight, R.; Abubucker, S.; Badger, J.H.; Chinwalla, A.T.; Creasy, H.H.; Earl, A.M.; FitzGerald, M.G.; Fulton, R.S.; et al. Structure, function and diversity of the healthy human microbiome. Nature 2012, 486, 207–214. [Google Scholar] [CrossRef] [Green Version]
- The Integrative HMP (iHMP) Research Network Consortium. The Integrative Human Microbiome Project. Nature 2019, 569, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Aagaard, K.; Ma, J.; Antony, K.M.; Ganu, R.; Petrosino, J.; Versalovic, J. The Placenta Harbors a Unique Microbiome. Sci. Transl. Med. 2014, 6, 237ra65. [Google Scholar] [CrossRef] [Green Version]
- Stewart, E.J. Growing Unculturable Bacteria. J. Bacteriol. 2012, 194, 4151–4160. [Google Scholar] [CrossRef] [Green Version]
- Kralik, P.; Ricchi, M. A Basic Guide to Real Time PCR in Microbial Diagnostics: Definitions, Parameters, and Everything. Front. Microbiol. 2017, 8, 108. [Google Scholar] [CrossRef]
- Schuster, S.C. Next-generation sequencing transforms today’s biology. Nat. Methods 2007, 5, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Prince, A.L.; Chu, D.M.; Seferovic, M.D.; Antony, K.M.; Ma, J.; Aagaard, K.M. The Perinatal Microbiome and Pregnancy: Moving Beyond the Vaginal Microbiome. Cold Spring Harb. Perspect. Med. 2015, 5, a023051. [Google Scholar] [CrossRef] [PubMed]
- Balvočiūtė, M.; Huson, D.H. SILVA, RDP, Greengenes, NCBI and OTT—How do these taxonomies compare? BMC Genom. 2017, 18, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dijk, E.L.; Jaszczyszyn, Y.; Naquin, D.; Thermes, C. The Third Revolution in Sequencing Technology. Trends Genet. 2018, 34, 666–681. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, R.; Rani, A.; Metwally, A.; McGee, H.S.; Perkins, D.L. Analysis of the microbiome: Advantages of whole genome shotgun versus 16S amplicon sequencing. Biochem. Biophys. Res. Commun. 2016, 469, 967–977. [Google Scholar] [CrossRef] [Green Version]
- Reese, A.T.; Dunn, R.R. Drivers of Microbiome Biodiversity: A Review of General Rules, Feces, and Ignorance. mBio 2018, 9, e01294-18. [Google Scholar] [CrossRef] [Green Version]
- Hagerty, S.L.; Hutchison, K.E.; Lowry, C.A.; Bryan, A.D. An empirically derived method for measuring human gut microbiome alpha diversity: Demonstrated utility in predicting health-related outcomes among a human clinical sample. PLoS ONE 2020, 15, e0229204. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Velasco, J.; Menabrito, M.; Catalán, I.B. What fertility specialists should know about the vaginal microbiome: A review. Reprod. Biomed. Online 2017, 35, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Borovkova, N.; Korrovits, P.; Ausmees, K.; Türk, S.; Jõers, K.; Punab, M.; Mändar, R. Influence of sexual intercourse on genital tract microbiota in infertile couples. Anaerobe 2011, 17, 414–418. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. S1), 4680–4687. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D.O.C. The Vaginal Microenvironment: The Physiologic Role of Lactobacilli. Front. Med. 2018, 5, 181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, J.; Bian, G.; Zheng, M.; Lu, G.; Chan, W.; Li, W.; Yang, K.; Chen, Z.; Du, Y. Fertility factors affect the vaginal microbiome in women of reproductive age. Am. J. Reprod. Immunol. 2020, 83, e13220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandão, P.; Gonçalves-Henriques, M. The Impact of Female Genital Microbiota on Fertility and Assisted Reproductive Treatments. J. Fam. Reprod. Heal. 2020, 14, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Verstraelen, H.; Vilchez-Vargas, R.; Desimpel, F.; Jauregui, R.; Vankeirsbilck, N.; Weyers, S.; Verhelst, R.; De Sutter, P.; Pieper, D.H.; Van De Wiele, T. Characterisation of the human uterine microbiome in non-pregnant women through deep sequencing of the V1-2 region of the 16S rRNA gene. PeerJ 2016, 4, e1602. [Google Scholar] [CrossRef] [Green Version]
- Egbase, P.; Al-Sharhan, M.; Al-Othman, S.; Al-Mutawa, M.; Udo, E.; Grudzinskas, J. Fertilization and early embryology: Incidence of microbial growth from the tip of the embryo transfer catheter after embryo transfer in relation to clinical pregnancy rate following in-vitro fertilization and embryo transfer. Hum. Reprod. 1996, 11, 1687–1689. [Google Scholar] [CrossRef] [Green Version]
- Agostinis, C.; Mangogna, A.; Bossi, F.; Ricci, G.; Kishore, U.; Bulla, R. Uterine Immunity and Microbiota: A Shifting Paradigm. Front. Immunol. 2019, 10, 2387. [Google Scholar] [CrossRef] [Green Version]
- Franasiak, J.M.; Scott, R.T. Endometrial microbiome. Curr. Opin. Obstet. Gynecol. 2017, 29, 146–152. [Google Scholar] [CrossRef]
- Chen, C.; Song, X.; Chunwei, Z.; Zhong, H.; Dai, J.; Lan, Z.; Li, F.; Yu, X.; Feng, Q.; Wang, Z.; et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nat. Commun. 2017, 8, 875. [Google Scholar] [CrossRef] [Green Version]
- Odawara, K.; Akino, R.; Sekizawa, A.; Sakamoto, M.; Yuriko, S.; Tanaka, K.; Mikashima, M.; Suzuki, M.; Odawara, Y. Examination of clinical factors affecting intrauterine microbiota. Reprod. Fertil. 2021, 2, 1–6. [Google Scholar] [CrossRef]
- Ilesanmi, O.A.; Adeyemi-Doro, F.A.B.; Edozien, L.; Akang, E. Culture of the endometrium of infertile women. J. Obstet. Gynaecol. 1995, 15, 50–52. [Google Scholar] [CrossRef]
- Moreno, I.; Codoñer, F.M.; Vilella, F.; Valbuena, D.; Martinez-Blanch, J.F.; Jimenez-Almazán, J.; Alonso, R.; Alamá, P.; Remohí, J.; Pellicer, A.; et al. Evidence That the Endometrial Microbiota Has an Effect on Implantation Success or Failure. Obstet. Gynecol. Surv. 2017, 72, 341–342. [Google Scholar] [CrossRef]
- Liu, Y.; Ko, E.Y.-L.; Wong, K.K.-W.; Chen, X.; Cheung, W.-C.; Law, T.S.-M.; Chung, J.P.-W.; Tsui, S.K.-W.; Li, T.-C.; Chim, S.S.-C. Endometrial microbiota in infertile women with and without chronic endometritis as diagnosed using a quantitative and reference range-based method. Fertil. Steril. 2019, 112, 707–717.e1. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Franasiak, J.M.; Zhan, Y.; Scott, R.T.; Rajchel, J.; Bedard, J.; Newby, R.; Treff, N.R.; Chu, T. Characterizing the endometrial microbiome by analyzing the ultra-low bacteria from embryo transfer catheter tips in IVF cycles: Next generation sequencing (NGS) analysis of the 16S ribosomal gene. Hum. Microbiome J. 2017, 3, 15–21. [Google Scholar] [CrossRef]
- Kyono, K.; Hashimoto, T.; Nagai, Y.; Sakuraba, Y. Analysis of endometrial microbiota by 16S ribosomal RNA gene sequencing among infertile patients: A single-center pilot study. Reprod. Med. Biol. 2018, 17, 297–306. [Google Scholar] [CrossRef]
- Moreno, I.; Garcia-Grau, I.; Perez-Villaroya, D.; Gonzalez-Monfort, M.; Bahçeci, M.; Barrionuevo, M.J.; Taguchi, S.; Puente, E.; Dimattina, M.; Lim, M.W.; et al. Endometrial microbiota composition is associated with reproductive outcome in infertile patients. Microbiome 2022, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Graspeuntner, S.; Bohlmann, M.K.; Gillmann, K.; Speer, R.; Kuenzel, S.; Mark, H.; Hoellen, F.; Lettau, R.; Griesinger, G.; König, I.; et al. Microbiota-based analysis reveals specific bacterial traits and a novel strategy for the diagnosis of infectious infertility. PLoS ONE 2018, 13, e0191047. [Google Scholar] [CrossRef] [Green Version]
- Koskimies, A.; Paavonen, J.; Meyer, B.; Kajanoja, P. Cervicitis and Infertility. Am. J. Reprod. Immunol. 1981, 1, 299–302. [Google Scholar] [CrossRef]
- Cheong, H.C.; Yap, P.S.X.; Chong, C.W.; Cheok, Y.Y.; Lee, C.Y.Q.; Tan, G.M.Y.; Sulaiman, S.; Hassan, J.; Sabet, N.S.; Looi, C.Y.; et al. Diversity of endocervical microbiota associated with genital Chlamydia trachomatis infection and infertility among women visiting obstetrics and gynecology clinics in Malaysia. PLoS ONE 2019, 14, e0224658. [Google Scholar] [CrossRef]
- Wee, B.A.; Thomas, M.; Sweeney, E.L.; Frentiu, F.D.; Samios, M.; Ravel, J.; Gajer, P.; Myers, G.; Timms, P.; Allan, J.A.; et al. A retrospective pilot study to determine whether the reproductive tract microbiota differs between women with a history of infertility and fertile women. Aust. N. Z. J. Obstet. Gynaecol. 2017, 58, 341–348. [Google Scholar] [CrossRef]
- Sahu, M.C.; Mishra, S.P.; Panda, R.; Patnaik, T. SURVEILLANCE OF MICROBIAL FLORA FOR INFERTILITY COUPLES IN AN INDIAN TERTIARY CARE TEACHING HOSPITAL. Asian J. Pharm. Clin. Res. 2017, 10, 405. [Google Scholar] [CrossRef]
- Campisciano, G.; Florian, F.; D’Eustacchio, A.; Stanković, D.; Ricci, G.; De Seta, F.; Comar, M. Subclinical alteration of the cervical-vaginal microbiome in women with idiopathic infertility. J. Cell. Physiol. 2017, 232, 1681–1688. [Google Scholar] [CrossRef] [PubMed]
- Babu, G. Comparative Study on the Vaginal Flora and Incidence of Asymptomatic Vaginosis among Healthy Women and in Women with Infertility Problems of Reproductive Age. J. Clin. Diagn. Res. 2017, 11, DC18–DC22. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Zhao, J.; Yin, J.; Zhao, F.; Wang, W.; Ding, X.; Yu, H.; Ma, X.; Wang, B. The association between the pre-pregnancy vaginal microbiome and time-to-pregnancy: A Chinese pregnancy-planning cohort study. BMC Med. 2022, 20, 246. [Google Scholar] [CrossRef] [PubMed]
- Moberg, P.; Eneroth, P.; Harlin, J.; Ljung-Wadström, A.; Nord, C.-E. Cervical bacterial flora in infertile and pregnant women. Med. Microbiol. Immunol. 1978, 165, 139–145. [Google Scholar] [CrossRef]
- Franasiak, J.M.; Werner, M.D.; Juneau, C.R.; Tao, X.; Landis, J.; Zhan, Y.; Treff, N.R.; Scott, R.T. Endometrial microbiome at the time of embryo transfer: Next-generation sequencing of the 16S ribosomal subunit. J. Assist. Reprod. Genet. 2016, 33, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Grau, I.; Perez-Villaroya, D.; Bau, D.; Gonzalez-Monfort, M.; Vilella, F.; Moreno, I.; Simon, C. Taxonomical and Functional Assessment of the Endometrial Microbiota in A Context of Recurrent Reproductive Failure: A Case Report. Pathogens 2019, 8, 205. [Google Scholar] [CrossRef] [Green Version]
- Moreno, I.; Garcia-Grau, I.; Bau, D.; Perez-Villaroya, D.; Gonzalez-Monfort, M.; Vilella, F.; Romero, R.; Simón, C. The first glimpse of the endometrial microbiota in early pregnancy. Am. J. Obstet. Gynecol. 2020, 222, 296–305. [Google Scholar] [CrossRef]
- Moore, D.E.; Soules, M.R.; Klein, N.A.; Fujimoto, V.Y.; Agnew, K.J.; Eschenbach, D.A. Bacteria in the transfer catheter tip influence the live-birth rate after in vitro fertilization. Fertil. Steril. 2000, 74, 1118–1124. [Google Scholar] [CrossRef]
- Hashimoto, T.; Kyono, K. Does dysbiotic endometrium affect blastocyst implantation in IVF patients? J. Assist. Reprod. Genet. 2019, 36, 2471–2479. [Google Scholar] [CrossRef] [Green Version]
- Riganelli, L.; Iebba, V.; Piccioni, M.; Illuminati, I.; Bonfiglio, G.; Neroni, B.; Calvo, L.; Gagliardi, A.; Levrero, M.; Merlino, L.; et al. Structural Variations of Vaginal and Endometrial Microbiota: Hints on Female Infertility. Front. Cell. Infect. Microbiol. 2020, 10, 350. [Google Scholar] [CrossRef]
- Kitaya, K.; Nagai, Y.; Arai, W.; Sakuraba, Y.; Ishikawa, T. Characterization of Microbiota in Endometrial Fluid and Vaginal Secretions in Infertile Women with Repeated Implantation Failure. Mediat. Inflamm. 2019, 2019, 4893437. [Google Scholar] [CrossRef] [Green Version]
- Salim, R.; Ben-Shlomo, I.; Colodner, R.; Keness, Y.; Shalev, E. Bacterial colonization of the uterine cervix and success rate in assisted reproduction: Results of a prospective survey. Hum. Reprod. 2002, 17, 337–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanchin, R.; Harmas, A.; Benaoudia, F.; Lundkvist, U.; Olivennes, F.; Frydman, R. Microbial flora of the cervix assessed at the time of embryo transfer adversely affects in vitro fertilization outcome. Fertil. Steril. 1998, 70, 866–870. [Google Scholar] [CrossRef]
- Hyman, R.W.; Herndon, C.N.; Jiang, H.; Palm, C.; Fukushima, M.; Bernstein, D.; Vo, K.C.; Zelenko, Z.; Davis, R.W.; Giudice, L.C. The dynamics of the vaginal microbiome during infertility therapy with in vitro fertilization-embryo transfer. J. Assist. Reprod. Genet. 2012, 29, 105–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernabeu, A.; Lledo, B.; Díaz, M.C.; Lozano, F.M.; Ruiz, V.; Fuentes, A.; Lopez-Pineda, A.; Moliner, B.; Castillo, J.C.; Ortiz, J.A.; et al. Effect of the vaginal microbiome on the pregnancy rate in women receiving assisted reproductive treatment. J. Assist. Reprod. Genet. 2019, 36, 2111–2119. [Google Scholar] [CrossRef]
- Haahr, T.; Humaidan, P.; Elbaek, H.O.; Alsbjerg, B.; Laursen, R.J.; Rygaard, K.; Johannesen, T.B.; Andersen, P.S.; Ng, K.L.; Jensen, J.S. Vaginal Microbiota and In Vitro Fertilization Outcomes: Development of a Simple Diagnostic Tool to Predict Patients at Risk of a Poor Reproductive Outcome. J. Infect. Dis. 2019, 219, 1809–1817. [Google Scholar] [CrossRef]
- Amato, V.; Papaleo, E.; Pasciuta, R.; Viganò, P.; Ferrarese, R.; Clementi, N.; Sanchez, A.M.; Quaranta, L.; Burioni, R.; Ambrosi, A.; et al. Differential Composition of Vaginal Microbiome, but Not of Seminal Microbiome, Is Associated With Successful Intrauterine Insemination in Couples With Idiopathic Infertility: A Prospective Observational Study. Open Forum Infect. Dis. 2019, 7, ofz525. [Google Scholar] [CrossRef]
- Wang, R.; Zhou, G.; Wu, L.; Huang, X.; Li, Y.; Luo, B.; Zhu, H.; Huang, W. The Microbial Composition of Lower Genital Tract May Affect the Outcome of in vitro Fertilization-Embryo Transfer. Front. Microbiol. 2021, 12, 729744. [Google Scholar] [CrossRef]
- Villani, A.; Fontana, A.; Barone, S.; de Stefani, S.; Primiterra, M.; Copetti, M.; Panebianco, C.; Parri, C.; Sciannamè, N.; Quitadamo, P.A.; et al. Identifying Predictive Bacterial Markers from Cervical Swab Microbiota on Pregnancy Outcome in Woman Undergoing Assisted Reproductive Technologies. J. Clin. Med. 2022, 11, 680. [Google Scholar] [CrossRef]
- Koedooder, R.; Singer, M.; Schoenmakers, S.; Savelkoul, P.H.M.; Morré, S.A.; De Jonge, J.D.; Poort, L.; Cuypers, W.J.S.S.; Beckers, N.G.M.; Broekmans, F.J.M.; et al. The vaginal microbiome as a predictor for outcome of in vitro fertilization with or without intracytoplasmic sperm injection: A prospective study. Hum. Reprod. 2019, 34, 1042–1054. [Google Scholar] [CrossRef]
- Hao, X.; Li, P.; Wu, S.; Tan, J. Association of the Cervical Microbiota With Pregnancy Outcome in a Subfertile Population Undergoing In Vitro Fertilization: A Case-Control Study. Front. Cell. Infect. Microbiol. 2021, 11, 654202. [Google Scholar] [CrossRef] [PubMed]
- Mangot-Bertrand, J.; Fenollar, F.; Bretelle, F.; Gamerre, M.; Raoult, D.; Courbiere, B. Molecular diagnosis of bacterial vaginosis: Impact on IVF outcome. Eur. J. Clin. Microbiol. 2013, 32, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Okwelogu, S.I.; Ikechebelu, J.I.; Agbakoba, N.R.; Anukam, K.C. Microbiome Compositions From Infertile Couples Seeking In Vitro Fertilization, Using 16S rRNA Gene Sequencing Methods: Any Correlation to Clinical Outcomes? Front. Cell. Infect. Microbiol. 2021, 11, 709372. [Google Scholar] [CrossRef] [PubMed]
- Lledo, B.; Fuentes, A.; Lozano, F.M.; Cascales, A.; Morales, R.; Hortal, M.; Sellers, F.; Palacios-Marques, A.; Bermejo, R.; Quereda, F.; et al. Identification of vaginal microbiome associated with IVF pregnancy. Sci. Rep. 2022, 12, 6807. [Google Scholar] [CrossRef] [PubMed]
- Haahr, T.; Jensen, J.; Thomsen, L.; Duus, L.; Rygaard, K.; Humaidan, P. Abnormal vaginal microbiota may be associated with poor reproductive outcomes: A prospective study in IVF patients. Hum. Reprod. 2016, 31, 795–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vergaro, P.; Tiscornia, G.; Barragán, M.; García, D.; Rodriguez, A.; Santaló, J.; Vassena, R. Vaginal microbiota profile at the time of embryo transfer does not affect live birth rate in IVF cycles with donated oocytes. Reprod. Biomed. Online 2019, 38, 883–891. [Google Scholar] [CrossRef]
- Selman, H.; Mariani, M.; Barnocchi, N.; Mencacci, A.; Bistoni, F.; Arena, S.; Pizzasegale, S.; Brusco, G.F.; Angelini, A. Examination of bacterial contamination at the time of embryo transfer, and its impact on the IVF/pregnancy outcome. J. Assist. Reprod. Genet. 2007, 24, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mändar, R.; Punab, M.; Borovkova, N.; Lapp, E.; Kiiker, R.; Korrovits, P.; Metspalu, A.; Krjutškov, K.; Nõlvak, H.; Preem, J.-K.; et al. Complementary seminovaginal microbiome in couples. Res. Microbiol. 2015, 166, 440–447. [Google Scholar] [CrossRef]
- Ndiokwere, C.; Olise, N.A.; Nmewurum, V.; Omoregie, R.; Agbakoba, N.R.; Anukam, K.C. 16s rRNA Metagenomics of Seminal Fluids From Medical Microbiology Laboratory in a Tertiary Hospital, Southern Nigeria. J. Med. Lab. Sci. 2019, 29, 86–109. [Google Scholar] [CrossRef]
- Igenomix Foundation. EMMA Endometrial Microbiome Metagenomic Analysis: A Screening Test to Evaluate the Endometrium at the Microbiological Level. Available online: https://www.igenomix.com/geneticsolutions/emma-clinics/ (accessed on 23 September 2022).
- Varinos Inc. Innovate Reproductive Health by Genomic Testing. Available online: https://www.varinos.com/english (accessed on 23 September 2022).
- Haahr, T.; Jensen, J.S.; Humaidan, P. Research and business—The yin and yang in modern medicine. Reprod. Biomed. Online 2020, 40, 613–616. [Google Scholar] [CrossRef]
- Nzisa, J. Review of the European Society of Human Reproduction and Embryology (ESHRE) 38th Annual Meeting 2022. EMJ Reprod. Heal. 2022, 8, 8–16. [Google Scholar] [CrossRef]


{kind=link}
| Genital Tract Area | Findings | Study Population | Author [Reference] |
|---|---|---|---|
| Endometrium | Lactobacillus abundance was 2% in CE and 81% in NCE. L. crispatus was less abundant in CE. Non-lactobacillus taxa were more abundant in CE, Anaerococcus and Gardnerella were negatively correlated with relative abundance of Lactobacillus. | 130 infertile women | Liu et al. [32] |
| Lactobacillus, Atopobium, Clostridium, Gardnerella, Megasphaera, Parvimonas, Prevotella, Sphingomonas, or Sneathia genera. | 35 infertile women (2016); 342 infertile women (2022) | Moreno et al. [31,35] | |
| Lactobacillus spp. >90% (n = 33), >70% (n = 53). Corynebacterium (n = 40), Bifidobacterium (n = 15), Staphylococcus spp. (n = 38). | 70 infertile women | Tao et al. [33] | |
| Lactobacillus spp. percentage lowest in the IVF patients, followed by non-IVF patients, and highest in healthy volunteers (64% vs. 96% vs. 99.5%). Lactobacillus spp. >90% lowest in IVF group (38% vs. 74% vs. 86%). | 102 infertile women | Kyono et al. [34] | |
| Cervix | Infertile women had more Gardnerella in the cervix. | 15 infertile women | Wee et al. [39] |
| Higher occurrence of Mycobacterium tuberculosis in infertile patients | 112 infertile couples | Hok et al. [5] | |
| Only anaerobic bacteria were found (51% of infertile, 26% of early pregnancy loss, 0% in labor); The largest proportion of patients with both aerobic and anaerobic bacteria was found in the labor group. | 47 Women with infertility, early pregnancy loss, and labor | Moberg et al. [44] | |
| Women examined for infertility had significantly higher levels of anti-chlamydial antibodies. | 52 Women with reproductive failure and clinically “inflamed cervixes”, and Infertile women | Koskimies et al. [37] | |
| E. coli growth in cervical samples was associated with infertility. | 288 infertile couples | Mishra et al. [40] | |
| Women with previous chlamydia infection (ININF > nININF and FSW); Lactobacillus-78.34% in FF, 69% in nININF, 58% in ININF; growth of Gardnerella, Prevotella, and Sneathia (ININF > nININF > FF). | 47 [nININF (n = 26), ININF (n = 21)], FSW (n = 54), FF (n = 89) | Graspeuntner et al. [36] | |
| Chlamydia trachomatis infection 88% in the infertile group vs. 28% in the fertile group. | 34 infertile women | Cheong et al. [38] | |
| Vagina | Infertile women had more Ureaplasma in the vagina. | 15 infertile women | Wee et al. [39] |
| L. iners, L. crispatus, and L. gasseri distinguished idiopathic infertile from other groups. Fusobacteria was present in women with bacterial vaginosis but not in women with idiopathic infertility. | 96 women with idiopathic infertility, bacterial vaginosis, non-idiopathic infertility, and healthy women | Campisciano et al. et al. [41] | |
| Detection of Candida spp. (27%), Enterococcus(23%), E. coli (14%) in infertile women. The percentage of Lactobacillus was relatively low (4%) and asymptomatic vaginosis was present in 28% of women with infertility. | 200 (116 women with Infertility and 84 healthy) | Babu et al. [42] | |
| Lower fecundability was associated with higher Actinobacteria, Gardnerella, L. iners, Fannyhessea vaginalis, and a lower abundance of L. crispatus and L. gasseri. Higher Lactobacillales in the pregnant group. | 478 women planning pregnancy | Hong, X. et al. [43] |
| Parameter | Outcome * [Reference] | No Effect Author [Reference] | Positive Correlation Author [Reference] | Negative Correlation Author [Reference] |
|---|---|---|---|---|
| High richness of species | On-going pregnancy | Franasiak et al. [27] Moreno et al. [31] | ||
| High diversity | Franasiak et al. [27] Moreno et al. [31] | |||
| High % of Lactobacillus sp.** | On-going pregnancy [33,34,35] Live birth rate [33,35,48] Miscarriage [34] | Franasiak et al. [27] Kyono et al. [34] # Hashimoto et al. [49] $ | Moreno et al. [31] (# or $) Kyono et al. [34] $ Moore et al. [48] | Tao et al. [33] # Riganelli et al. [50] |
| Bifidobacterium sp. ** | On-going pregnancy [34] | Kyono et al. [34] # Hashimoto et al. [49] $ | Kyono et al. [34] (≥80%) | |
| Gardnerella sp. | Hashimoto et al. [49] | Moreno et al. [35] Kitaya et al. [51] | ||
| Streptococcus sp. | Hashimoto et al. [49] | Moreno et al. [35] | ||
| Atopobium sp. | Hashimoto et al. [49] | |||
| Flavobacterium sp. | Franasiak et al. [27] | |||
| Pseudomonas sp. | Franasiak et al. [27] | |||
| Acinetobacter sp. | Franasiak et al. [27] | |||
| Burkholderia sp. | RIF [51] | Kitaya et al. [51] | ||
| Kocuria dechangensis | Riganelli et al. [50] |
| Parameter | Outcome * [Reference] | No Effect Author [Reference] | Positive Correlation Author [Reference] | Negative Correlation Author [Reference] | Comments |
|---|---|---|---|---|---|
| High richness of species | Hyman et al. [54] Bernabeu et al. [55] | ||||
| High diversity | Graspeuntner et al. [36] Hyman et al. [54] Haahr et al. [56] Amato et al. [57] | ||||
| High % of Lactobacillus sp. ** | Hyman et al. [54] Bernabeu et al. [55] Kyono et al. [34] # Wang et al. [58] | Graspeuntner et al. [36] (infectious) Kyono et al. [34] $ | Different cut-off values correlate differently | ||
| L. crispatus (CST 1) | Haahr et al. [56] | Graspeuntner et al. [36] Villani et al. [59] | Koedooder et al. [60] Hao et al. [61] | Low levels in fresh ET and frozen-thawed ET favored pregnancy | |
| L. gasseri (CST 2) | Haahr et al. [56] | Hao et al. [61] | Graspeuntner et al. [36] Hao et al. [61] | Low levels in fresh ET and high levels in frozen-thawed ET favored pregnancy | |
| L. iners (CST 3) | Graspeuntner et al. [36] | Villani et al. [59] | |||
| L. jensenii (CST 5) | Haahr et al. [56] | Hao et al. [61] | Koedooder et al. [60] Hao et al. [61] | Low levels in fresh ET and high levels in frozen-thawed ET favored pregnancy | |
| CST 4 (diverse bacteria) Presence of other species—No effect—Haahr et al. [56] | |||||
| Bifidobacterium sp. | Villani et al. [59] | ||||
| Gardnerella sp. | Kitaya et al. [51] Bernabeu et al. [55] | Koedooder et al. [60] Wee et al. [39] Graspeuntner et al. [36] | |||
| Streptococcus sp. | Bernabeu et al. [55] | Wang et al. [58] | |||
| Atopobium sp. | Villani et al. [59] | ||||
| Sneathia sp. | Graspeuntner et al. [36] | ||||
| Ureaplasma parvum | Bernabeu et al. [55] | ||||
| Prevotella sp. | Graspeuntner et al. [36] | ||||
| Clostridium | Bernabeu et al. [55] | ||||
| Proteobacteria | Villani et al. [59] | Koedooder et al. [60] | |||
| Solanum torvum | Wang et al. [58] | ||||
| Fusobacterium | Wang et al. [58] | ||||
| Yersinia | Villani et al. [59] | ||||
| Parameter | Outcome * [Reference] | No Effect Author [Reference] | Positive Correlation Author [Reference] | Negative Correlation Author [Reference] | Comments |
|---|---|---|---|---|---|
| High richness of species | Wee et al. [39] | Campisciano et al. [41] Hyman et al. [54] Bernabeu et al. [55] | |||
| High diversity | Wee et al. [39] Amato et al. [57] Bernabeu et al. [55] | Campisciano et al. [41] Graspeuntner et al. [36] Hyman et al. [54] Haahr et al. [56] Amato et al. [57] Bernabeu et al. [55] | While alpha-diversity has unfavorable outcomes, betadiversity has no effect | ||
| High % of Lactobacillus sp. ** | RIF [51] | Hyman et al. [54] | Graspeuntner et al. [36] (infectious) Kyono et al. [34] ($ or #) Bernabeu et al. [55] (p = 0.2) Koedooder et al. [60] | Kitaya et al. [51] # | Low load of lactobacilli associated with low pregnancy rate |
| L. crispatus (CST 1) | Live birth, miscarriage [63] | Haahr et al. [56] | Campisciano et al. [41] Graspeuntner et al. [36] Koedooder et al. [60] Riganelli et al. [50] | Koedooder et al. [60] Okwelogu et al. [63] | <60% has positive and >60% has negative correlation [60] |
| L. gasseri (CST 2) | Haahr et al. [56] | Okwelogu et al. [63] B. Lledo et al. [64] | Riganelli et al. [50] Campisciano et al. [41] Graspeuntner et al. [36] | ||
| L. iners (CST 3) | Live birth, miscarriage [63] PTB [64] | Graspeuntner et al. [36] | Riganelli et al. [50] | Wang et al. [58] Okwelogu et al. [63] B. Lledo et al. [64] | |
| L. jensenii (CST 5) | Haahr et al. [56] | Koedooder et al. [60] | |||
| CST 4 (diverse bacteria) Presence of other species—No effect—Haahr et al. [56] | |||||
| Bifidobacterium sp. | Amato et al. [57] | Amato et al. [57] Wang et al. [58] | |||
| Gardnerella sp. | Koedooder et al. [60] Campisciano et al. [41] Wee et al. [39] Graspeuntner et al. [36] Bernabeu et al. [55] (p = 0.11) Riganelli et al. [50] | IS-pro type 1 (IST1) is associated with low pregnancy rate | |||
| Staphyllococcus sp. | Campisciano et al. [41] | ||||
| Streptococcus sp. | Bernabeu et al. [55] | Riganelli et al. [50] | |||
| Atopobium sp. | Campisciano et al. [41] | ||||
| Sneathia sp. | Graspeuntner et al. [36] | ||||
| Ureaplasma parvum | Bernabeu et al. [55] | Campisciano et al. [41] Wee et al. [39] | |||
| Burkholderia sp. | Kitaya et al. [51] | ||||
| Prevotella sp. | Campisciano et al. [41] Graspeuntner et al. [36] Wang et al. [58] | ||||
| Veillonella sp. | Campisciano et al. [41] | ||||
| Closteridium | Bernabeu et al. [55] | ||||
| Proteobacteria | Koedooder et al. [60] | ||||
| Bacteroides | Live birth, miscarriage [63] | Okwelogu et al. [63] | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dube, R.; Kar, S.S. Genital Microbiota and Outcome of Assisted Reproductive Treatment—A Systematic Review. Life 2022, 12, 1867. https://doi.org/10.3390/life12111867
Dube R, Kar SS. Genital Microbiota and Outcome of Assisted Reproductive Treatment—A Systematic Review. Life. 2022; 12(11):1867. https://doi.org/10.3390/life12111867
Chicago/Turabian StyleDube, Rajani, and Subhranshu Sekhar Kar. 2022. "Genital Microbiota and Outcome of Assisted Reproductive Treatment—A Systematic Review" Life 12, no. 11: 1867. https://doi.org/10.3390/life12111867