
Evaluation of the Muscle Strength of the Tongue with the Tongue Digital Spoon (TDS) in Patients with Obstructive Sleep Apnea
 ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Sleep Laboratory
2.3. Inclusion and Exclusion Criteria
2.4. IOPI
2.5. TDS
2.6. Statistical Analysis
3. Results
3.1. Main Features
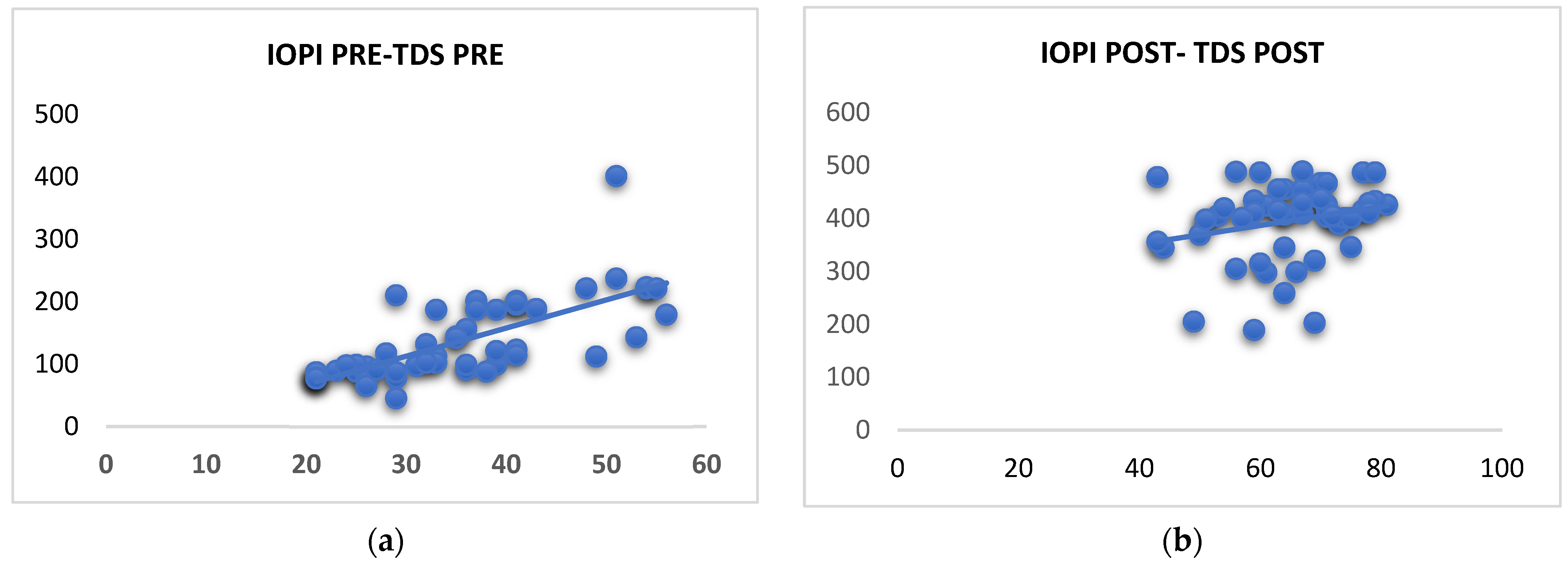
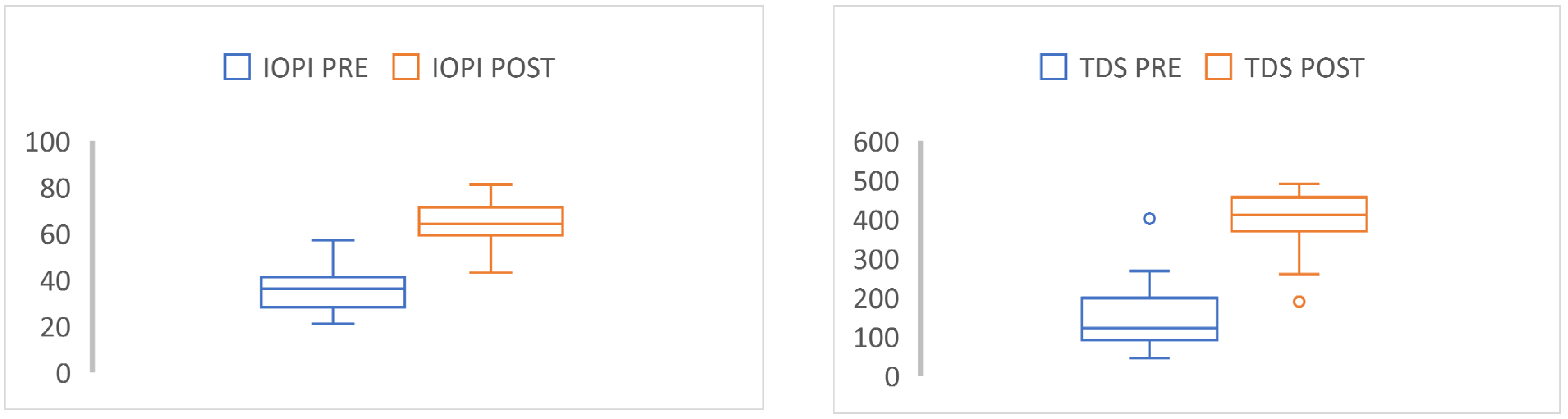
3.2. Analysis of Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Eckert, D.J.; White, D.P.; Jordan, A.S.; Malhotra, A.; Wellman, A. Defining phenotypic causes of obstructive sleep apnea. Identification of novel therapeutic targets. Am. J. Respir. Crit. Care Med. 2013, 188, 996–1004. [Google Scholar] [CrossRef] [Green Version]
- Bosi, M.; De Vito, A.; Kotecha, B.; Viglietta, B.; Braghiroli, A.; Steier, J.; Pengo, M.; Sorrenti, G.; Gobbi, R.; Vicini, C.; et al. Phenotyping the pathophysiology of obstructive sleep apnea using polygraphy/polysomnography: A review of the literature. Sleep Breath. 2018, 22, 579–592. [Google Scholar] [CrossRef] [Green Version]
- Ieto, V.; Kayamori, F.; Montes, M.I.; Hirata, R.P.; Gregório, M.G.; Alencar, A.M.; Drager, L.F.; Genta, P.R.; Lorenzi-Filho, G. Effects of oropharyngeal exercises on snoring: A randomized trial. Chest 2015, 148, 683–691. [Google Scholar] [CrossRef] [Green Version]
- de Felício, C.M.; da Silva Dias, F.V.; Trawitzki, L.V. Obstructive sleep apnea: Focus on myofunctional therapy. Nat. Sci. Sleep 2018, 610, 271–286. [Google Scholar] [CrossRef] [Green Version]
- Guilleminault, C.; Huang, Y.S.; Monteyrol, P.J.; Sato, R.; Quo, S.; Lin, C.H. Critical role of myofascial reeducation in pediatric sleep-disordered breathing. Sleep Med. 2013, 14, 518–525. [Google Scholar] [CrossRef]
- Villa, M.P.; Evangelisti, M.; Martella, S.; Barreto, M.; Del Pozzo, M. Can myofunctional therapy increase tongue tone and reduce symptoms in children with sleep-disordered breathing? Sleep Breath. 2017, 211, 1025–1032. [Google Scholar] [CrossRef]
- Koka, V.; DeVito, A.; Roisman, G.; Petitjean, M.; Filograna Pignatelli, G.R.; Padovani, D.; Randerath, W. Orofacial myofunctional therapy in obstructive sleep apnea syndrome: A pathophysiological perspective. Medicina 2021, 57, 323. [Google Scholar] [CrossRef]
- Meghpara, S.; Chohan, M.; Bandyopadhyay, A.; Kozlowski, C.; Casinas, J.; Kushida, C.; Camacho, M. Myofunctional therapy for OSA: A meta-analysis. Exp. Rev. Respir. Med. 2022, 16, 285–291. [Google Scholar] [CrossRef]
- O'Connor-Reina, C.; Ignacio Garcia, J.M.; Rodriguez Alcala, L.; Rodríguez Ruiz, E.; Garcia Iriarte, M.T.; Casado Morente, J.C.; Baptista, P.; Plaza, G. Improving Adherence to Myofunctional Therapy in the Treatment of Sleep-Disordered Breathing. J. Clin. Med. 2021, 10, 5772. [Google Scholar] [CrossRef]
- Youmans, S.R.; Stierwalt, J.A.G. Measures of tongue function related to swallowing. Dysphagia 2006, 21, 102–111. [Google Scholar] [CrossRef]
- O’Connor-Reina, C.; Plaza, G.; Garcia Iriarte, M.T.; Ignacio-Garcia, J.M.; Baptista, P.; Casado-Morente, J.C.; De Vicente, E. Tongue peak pressure: A tool to aid in the identification of obstruction sites in patients with obstructive sleep apnea/hypopnea syndrome. Sleep Breath. 2020, 24, 281–286. [Google Scholar] [CrossRef]
- Rodríguez-Alcalá, L.; Martín-Lagos Martínez, J.; O’Connor-Reina, C.; Plaza, G. Assessment of muscular tone of the tongue using a digital measure spoon in a healthy population: A pilot study. PLoS ONE 2021, 16, e0245901. [Google Scholar] [CrossRef]
- Rodriguez-Alcalá, L.; Ignacio-García, J.; Serrano Angulo, M.S.; Casado Morente, J.C.; Flores, F.B.; O’Connor-Reina, C. Tongue+ protocol for the diagnosis of obstructive sleep apnoea in Quirónsalud Marbella hospital. F1000Research 2022, 11, 322. [Google Scholar] [CrossRef]
- IOPI Medical. Iowa Performance Instrument: User’s Manual. 2008. Available online: http://www.iopimedical.com (accessed on 14 September 2022).
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Rodríguez-Alcalá, L.; Martín-Lagos Martínez, J.; Baptista, P.; Ríos Fernández, R.; Gómez, F.J.; Parejo Santaella, J.; Plaza, G. Sensorimotor tongue evaluation and rehabilitation in patients with sleep-disordered breathing: A novel approach. J. Oral Rehabil. 2021, 48, 1363–1372. [Google Scholar] [CrossRef]
- Berry, R.B.; Gamaldo, C.E.; Harding, S.M.; Brooks, R.; Lloyd, R.M.; Vaughn, B.V.; Marcus, C.L. AASM Scoring Manual Version 2.2 Updates: New chapters for scoring infant sleep staging and home sleep apnea testing. J. Clin. Sleep Med. 2015, 11, 1253–1254. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.C. Effects of Tongue Strength Training and Detraining on Tongue Pressures in Healthy Adults. Dysphagia 2015, 30, 315–320. [Google Scholar] [CrossRef]
- Robin, D.A.; Luschei, E.S. IOPI: Iowa Oral Performance Instrument Reference Manual; Breakthrough: Oakdale, IA, USA, 1992. [Google Scholar]
- Baz, H.; Elshafey, M.; Elmorsy, S.; Abu-Samra, M. The role of oral myofunctional therapy in managing patients with mild to moderate obstructive sleep apnea. PAN Arab. J. Rhinol. 2012, 2, 17–22. [Google Scholar]
- Rueda, J.-R.; Mugueta-Aguinaga, I.; Vilaró, J.; Rueda-Etxebarria, M. Myofunctional therapy (oropharyngeal exercises) for obstructive sleep apnoea. Cochrane Database Syst. Rev. 2020, 11, CD013449. [Google Scholar] [CrossRef]
- Diaféria, G.; Santos-Silva, R.; Truksinas, E.; Haddad, F.L.; Santos, R.; Bommarito, S.; Gregório, L.C.; Tufik, S.; Bittencourt, L. Myofunctional therapy improves adherence to continuous positive airway pressure treatment. Sleep Breath. 2017, 21, 387–395. [Google Scholar] [CrossRef]
- Guimarães, K.C.; Drager, L.F.; Genta, P.R.; Marcondes, B.F.; Lorenzi-Filho, G. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am. J. Respir. Crit. Care Med. 2009, 179, 962–966. [Google Scholar] [CrossRef] [Green Version]
- Franciotti, R.; Di Maria, E.; D'Attilio, M.; Aprile, G.; Cosentino, F.G.; Perrotti, V. Quantitative Measurement of Swallowing Performance Using Iowa Oral Performance Instrument: A Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 2319. [Google Scholar] [CrossRef]
- Borrmann, P.F.; O’Connor-Reina, C.; Ignacio, J.M.; Ruiz, E.R.; Alcala, L.R.; Dzembrovsky, F.; Baptista, P.; Garcia Iriarte, M.T.; Alba, C.C.; Plaza, G. Muscular assessment in patients with severe obstructive sleep apnea syndrome: Protocol for a case-control study. JMIR Res. Protoc. 2021, 10, e30500. [Google Scholar] [CrossRef]
- O’Connor-Reina, C.; Ignacio Garcia, J.M.; Rodriguez Ruiz, E.; Morillo Dominguez, M.D.C.; Ignacio Barrios, V.; Baptista Jardin, P.; Casado Morente, J.C.; Garcia Iriarte, M.T.; Plaza, G. Myofunctional therapy app for severe apnea-hypopnea sleep obstructive syndrome: Pilot randomized controlled trial. JMIR Mhealth Uhealth 2020, 9, e23123. [Google Scholar] [CrossRef]
- Mediano, O.; Mangado, N.G.; Montserrat, J.M.; Alonso-Álvarez, M.L.; Almendros, I.; Alonso-Fernández, A.; Barbé, F.; Borsini, E.; Caballero-Eraso, C.; Cano-Pumarega, I.; et al. International Consensus Document on Obstructive Sleep Apnea. Arch. Bronconeumol. 2022, 58, 52–68. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Moderate to severe OSA (AHI > 15) | BMI > 32 kg/m2 |
| Grade I–IV tonsils | Ankyloglossia |
| Age between 18 and 75 years | Unstable coronary disease |
| Complete dentition | Hypnotic medication |
| Systemic disease with a known inflammatory state | |
| Severe nasal obstruction | |
| Previous treatment for OSA or musculature rehabilitation |
| Moderate OSA (N = 31) | Severe OSA (N = 18) | |||
|---|---|---|---|---|
| Variable | Mean | SD | Mean | SD |
| Age (years) | 52.7 | 6.6 | 51.1 | 10.2 |
| BMI (kg/m2) | 25.4 | 4.1 | 26.4 | 5.3 |
| AHI (e/h) | 23.9 | 6.2 | 41.2 | 8.3 |
| Moderate OSA (N = 31) (SD) | Severe OSA (N = 18) (SD) | p a | |
|---|---|---|---|
| Epworth Scale | 11 (3.53) | 15.8 (2.4) | 0.41 |
| Pittsburgh Scale | 10.3 (2.1) | 16.9 (2.5) | 0.73 |
| IOPI tongue (kPa) | 35.6 (9.05) | 32.8 (12.4) | 0.08 |
| IOPI lips (kPa) | 23 (9.6) | 22 (8.9) | 0.45 |
| TDS (g/cm2) | 168.5 (42.8) | 129.8 (53.7) | 0.23 |
| Before Airway Gym® Mean (SD) (N = 49) | After Airway Gym® Mean (SD) (N = 49) | p | |
|---|---|---|---|
| Epworth Scale | 13.7 (4.2) | 11.1 (2.6) | 0.04 |
| Pittsburgh Scale | 15.2 (7.5) | 9.8 (6.9) | 0.02 |
| IOPI tongue (kPa) | 35.1 (14.8) | 54.7 (10.1) | 0.03 |
| IOPI lips (kPa) | 21.7 (9.7) | 31.5 (8.6) | 0.03 |
| TDS (g/cm2) | 149.4 (46.8) | 397.3 (93.4) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Alcalá, L.; Benjumea, F.; Casado-Morente, J.C.; Baptista, P.M.; O’Connor-Reina, C.; Plaza, G. Evaluation of the Muscle Strength of the Tongue with the Tongue Digital Spoon (TDS) in Patients with Obstructive Sleep Apnea. Life 2022, 12, 1841. https://doi.org/10.3390/life12111841
Rodríguez-Alcalá L, Benjumea F, Casado-Morente JC, Baptista PM, O’Connor-Reina C, Plaza G. Evaluation of the Muscle Strength of the Tongue with the Tongue Digital Spoon (TDS) in Patients with Obstructive Sleep Apnea. Life. 2022; 12(11):1841. https://doi.org/10.3390/life12111841
Chicago/Turabian StyleRodríguez-Alcalá, Laura, Felipe Benjumea, Juan Carlos Casado-Morente, Peter M. Baptista, Carlos O’Connor-Reina, and Guillermo Plaza. 2022. "Evaluation of the Muscle Strength of the Tongue with the Tongue Digital Spoon (TDS) in Patients with Obstructive Sleep Apnea" Life 12, no. 11: 1841. https://doi.org/10.3390/life12111841