
Screening for the Detection of Toxoplasma gondii IgG, IgM and IgA in Females of Reproductive Age from Western Romania

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Serologic Tests
2.3. Interpretation of the Serologic Test Results
2.4. Data Management and Statistical Analysis
2.5. Ethical Consideration
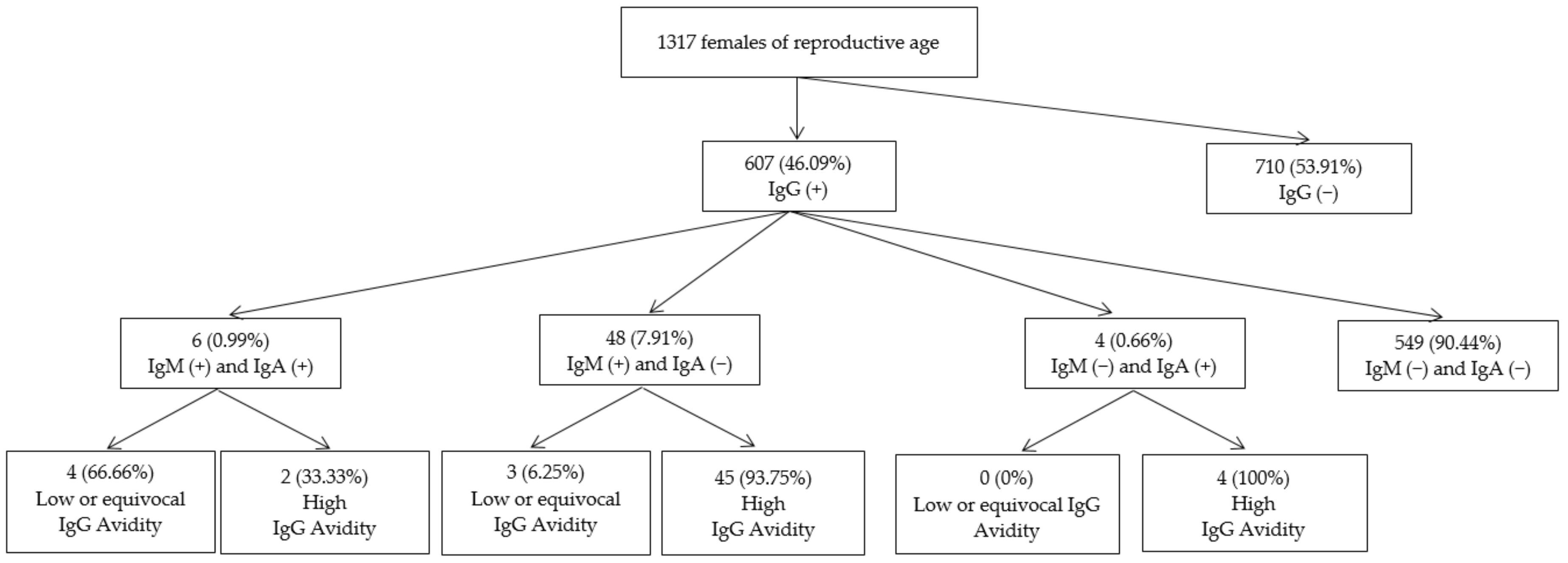
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dubey, J.P. The History of Toxoplasma Gondii—The First 100 Years. J. Eukaryot. Microbiol. 2008, 55, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Robert-Gangneux, F.; Dardé, M.-L. Epidemiology of and Diagnostic Strategies for Toxoplasmosis. Clin. Microbiol. Rev. 2012, 25, 264–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendez, O.A.; Koshy, A.A. Toxoplasma Gondii: Entry, Association, and Physiological Influence on the Central Nervous System. PLoS Pathog. 2017, 13, e1006351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibley, L.D.; Khan, A.; Ajioka, J.W.; Rosenthal, B.M. Genetic Diversity of Toxoplasma Gondii in Animals and Humans. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 2009, 364, 2749–2761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olariu, T.R.; Ursoniu, S.; Hotea, I.; Dumitrascu, V.; Anastasiu, D.; Lupu, M.A. Seroprevalence and Risk Factors of Toxoplasma Gondii Infection in Pregnant Women from Western Romania. Vector Borne Zoonotic Dis. Larchmt. N 2020, 20, 763–767. [Google Scholar] [CrossRef] [PubMed]
- Furtado, J.M.; Smith, J.R.; Belfort, R.; Gattey, D.; Winthrop, K.L. Toxoplasmosis: A Global Threat. J. Glob. Infect. Dis. 2011, 3, 281–284. [Google Scholar] [CrossRef]
- McAuley, J.B. Congenital Toxoplasmosis. J. Pediatr. Infect. Dis. Soc. 2014, 3 (Suppl 1), S30–S35. [Google Scholar] [CrossRef]
- Olariu, T.R.; Remington, J.S.; McLeod, R.; Alam, A.; Montoya, J.G. Severe Congenital Toxoplasmosis in the United States: Clinical and Serologic Findings in Untreated Infants. Pediatr. Infect. Dis. J. 2011, 30, 1056–1061. [Google Scholar] [CrossRef]
- Olariu, T.R.; Press, C.; Talucod, J.; Olson, K.; Montoya, J.G. Congenital Toxoplasmosis in the United States: Clinical and Serologic Findings in Infants Born to Mothers Treated during Pregnancy. Parasite Paris Fr. 2019, 26, 13. [Google Scholar] [CrossRef]
- Rostami, A.; Riahi, S.M.; Gamble, H.R.; Fakhri, Y.; Nourollahpour Shiadeh, M.; Danesh, M.; Behniafar, H.; Paktinat, S.; Foroutan, M.; Mokdad, A.H.; et al. Global prevalence of latent toxoplasmosis in pregnant women: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 673–683. [Google Scholar] [CrossRef]
- Rostami, A.; Riahi, S.M.; Contopoulos-Ioannidis, D.G.; Gamble, H.R.; Fakhri, Y.; Shiadeh, M.N.; Foroutan, M.; Behniafar, H.; Taghipour, A.; Maldonado, Y.A.; et al. Acute Toxoplasma infection in pregnant women worldwide: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2019, 13, e0007807. [Google Scholar] [CrossRef] [Green Version]
- Fanigliulo, D.; Marchi, S.; Montomoli, E.; Trombetta, C.M. Toxoplasma Gondii in Women of Childbearing Age and during Pregnancy: Seroprevalence Study in Central and Southern Italy from 2013 to 2017. Parasite Paris Fr. 2020, 27, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubey, J.P.; Hotea, I.; Olariu, T.R.; Jones, J.L.; Dărăbuş, G. Epidemiological Review of Toxoplasmosis in Humans and Animals in Romania. Parasitology 2014, 141, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Căpraru, I.D.; Lupu, M.A.; Horhat, F.; Olariu, T.R. Toxoplasmosis Seroprevalence in Romanian Children. Vector Borne Zoonotic Dis. Larchmt. N 2019, 19, 867–869. [Google Scholar] [CrossRef]
- Olariu, T.R.; Darabus, G.; Cretu, O.; Jurovits, O.; Erdelean, V.; Marincu, I.; Iacobiciu, I.; Petrescu, C.; Koreck, A. Prevalence of Toxoplasma Gondii Antibodies among Women of Childbearing Age in Timis Country. Lucr. Stiintifice Med. Vet. Timisoara 2008, 41, 367–371. [Google Scholar]
- Halonen, S.K.; Weiss, L.M. Toxoplasmosis. Handb. Clin. Neurol. 2013, 114, 125–145. [Google Scholar] [CrossRef] [Green Version]
- Fricker-Hidalgo, H.; Cimon, B.; Chemla, C.; Darde, M.L.; Delhaes, L.; L’ollivier, C.; Godineau, N.; Houze, S.; Paris, L.; Quinio, D.; et al. Toxoplasma Seroconversion with Negative or Transient Immunoglobulin M in Pregnant Women: Myth or Reality? A French Multicenter Retrospective Study. J. Clin. Microbiol. 2013, 51, 2103–2111. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.L.; Lopez, A.; Wilson, M.; Schulkin, J.; Gibbs, R. Congenital Toxoplasmosis: A Review. Obstet. Gynecol. Surv. 2001, 56, 296–305. [Google Scholar] [CrossRef]
- Khurana, S.; Batra, N. Toxoplasmosis in Organ Transplant Recipients: Evaluation, Implication, and Prevention. Trop. Parasitol. 2016, 6, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Pomares, C.; Gonfrier, G.; Koh, B.; Zhu, S.; Gong, M.; Montoya, J.G.; Dai, H. Multiplexed Anti-Toxoplasma IgG, IgM, and IgA Assay on Plasmonic Gold Chips: Towards Making Mass Screening Possible with Dye Test Precision. J. Clin. Microbiol. 2016, 54, 1726–1733. [Google Scholar] [CrossRef] [Green Version]
- Olariu, T.R.; Blackburn, B.G.; Press, C.; Talucod, J.; Remington, J.S.; Montoya, J.G. Role of Toxoplasma IgA as Part of a Reference Panel for the Diagnosis of Acute Toxoplasmosis during Pregnancy. J. Clin. Microbiol. 2019, 57, e01357-18. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Wang, Z.-D.; Huang, S.-Y.; Zhu, X.-Q. Diagnosis of Toxoplasmosis and Typing of Toxoplasma Gondii. Parasit. Vectors 2015, 8, 292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villard, O.; Cimon, B.; L’Ollivier, C.; Fricker-Hidalgo, H.; Godineau, N.; Houze, S.; Paris, L.; Pelloux, H.; Villena, I.; Candolfi, E. Help in the Choice of Automated or Semiautomated Immunoassays for Serological Diagnosis of Toxoplasmosis: Evaluation of Nine Immunoassays by the French National Reference Center for Toxoplasmosis. J. Clin. Microbiol. 2016, 54, 3034–3042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, M.; Remington, J.S.; Clavet, C.; Varney, G.; Press, C.; Ware, D. Evaluation of Six Commercial Kits for Detection of Human Immunoglobulin M Antibodies to Toxoplasma Gondii. The FDA Toxoplasmosis Ad Hoc Working Group. J. Clin. Microbiol. 1997, 35, 3112–3115. [Google Scholar] [CrossRef] [Green Version]
- Gharavi, M.J.; Oormazdi, H.; Roointan, E.S. A Comparative Study on Sensitivity and Specificity of Conventional and Unconventional IgG and IgM Assays for Diagnosis of Toxoplasmosis. Iran. J. Public Health 2008, 37, 42–45. [Google Scholar]
- Smets, A.; Fauchier, T.; Michel, G.; Marty, P.; Pomares, C. Comparison of Toxoplasma gondii IgG Avidity Architect and Vidas Assays with the Estimated Date of Infection in Pregnant Women. Parasite Paris Fr. 2016, 23, 45. [Google Scholar] [CrossRef] [Green Version]
- Toxoplasma Gondii IgA ELISA EIA-3683, Version 3.0. Available online: https://www.drg-diagnostics.de/files/eia-3683_ifu--toxoplasma-gondii-iga_2017-10-10_ce_endeites.pdf (accessed on 17 September 2022).
- Robert-Gangneux, F.; Guegan, H. Anti-Toxoplasma IgG assays: What performances for what purpose? A systematic review. Parasite 2021, 28, 39. [Google Scholar] [CrossRef]
- Murat, J.B.; Dard, C.; Fricker Hidalgo, H.; Dardé, M.L.; Brenier-Pinchart, M.P.; Pelloux, H. Comparison of the Vidas system and two recent fully automated assays for diagnosis and follow-up of toxoplasmosis in pregnant women and newborns. Clin. Vaccine Immunol. 2013, 20, 1203–1212. [Google Scholar] [CrossRef] [Green Version]
- Montoya, J.G.; Liesenfeld, O. Toxoplasmosis. Lancet Lond. Engl. 2004, 363, 1965–1976. [Google Scholar] [CrossRef]
- Cañedo-Solares, I.; Gómez-Chávez, F.; Luna-Pastén, H.; Ortiz-Alegría, L.B.; Flores-García, Y.; Figueroa-Damián, R.; Macedo-Romero, C.A.; Correa, D. What Do Anti-Toxoplasma Gondii IgA and IgG Subclasses in Human Saliva Indicate? Parasite Immunol. 2018, 40, e12526. [Google Scholar] [CrossRef]
- El Bissati, K.; Levigne, P.; Lykins, J.; Adlaoui, E.B.; Barkat, A.; Berraho, A.; Laboudi, M.; El Mansouri, B.; Ibrahimi, A.; Rhajaoui, M.; et al. Global Initiative for Congenital Toxoplasmosis: An Observational and International Comparative Clinical Analysis. Emerg. Microbes Infect. 2018, 7, 165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallon, M.; Peyron, F.; Cornu, C.; Vinault, S.; Abrahamowicz, M.; Kopp, C.B.; Binquet, C. Congenital Toxoplasma Infection: Monthly Prenatal Screening Decreases Transmission Rate and Improves Clinical Outcome at Age 3 Years. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2013, 56, 1223–1231. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, S.A.; Gad, N.; Koren, G. Toxoplasmosis and Pregnancy. Can. Fam. Physician Med. Fam. Can. 2014, 60, 334–336. [Google Scholar]
- Guegan, H.; Stajner, T.; Bobic, B.; Press, C.; Olariu, R.T.; Olson, K.; Srbljanovic, J.; Montoya, J.G.; Djurković-Djaković, O.; Robert-Gangneux, F. Maternal Anti-Toxoplasma Treatment during Pregnancy Is Associated with Reduced Sensitivity of Diagnostic Tests for Congenital Infection in the Neonate. J. Clin. Microbiol. 2021, 59, e01368-20. [Google Scholar] [CrossRef] [PubMed]
- Augustine, S.A.J. Towards Universal Screening for Toxoplasmosis: Rapid, Cost-Effective, and Simultaneous Detection of Anti-Toxoplasma IgG, IgM, and IgA Antibodies by Use of Very Small Serum Volumes. J. Clin. Microbiol. 2016, 54, 1684–1685. [Google Scholar] [CrossRef] [Green Version]
- Lupu, M.A.; Lighezan, R.; Paduraru, A.A.; Dragomir, A.; Pavel, R.; Grada, S.; Mihu, A.G.; Ursoniu, S.; Olariu, T.R. Seroepidemiology of Toxoplasma Gondii Infection in Blood Donors from Western Romania. Microorganisms 2022, 10, 973. [Google Scholar] [CrossRef]
- Berger, F.; Goulet, V.; Le Strat, Y.; Desenclos, J.-C. Toxoplasmosis among Pregnant Women in France: Risk Factors and Change of Prevalence between 1995 and 2003. Rev. Epidemiol. Sante Publique 2009, 57, 241–248. [Google Scholar] [CrossRef]
- Nogareda, F.; Le Strat, Y.; Villena, I.; De Valk, H.; Goulet, V. Incidence and Prevalence of Toxoplasma Gondii Infection in Women in France, 1980–2020: Model-Based Estimation. Epidemiol. Infect. 2014, 142, 1661–1670. [Google Scholar] [CrossRef] [Green Version]
- Gargaté, M.J.; Ferreira, I.; Vilares, A.; Martins, S.; Cardoso, C.; Silva, S.; Nunes, B.; Gomes, J.P. Toxoplasma Gondii Seroprevalence in the Portuguese Population: Comparison of Three Cross-Sectional Studies Spanning Three Decades. BMJ Open 2016, 6, e011648. [Google Scholar] [CrossRef] [Green Version]
- Afonso, E.; Germain, E.; Poulle, M.-L.; Ruette, S.; Devillard, S.; Say, L.; Villena, I.; Aubert, D.; Gilot-Fromont, E. Environmental Determinants of Spatial and Temporal Variations in the Transmission of Toxoplasma Gondii in Its Definitive Hosts. Int. J. Parasitol. Parasites Wildl. 2013, 2, 278–285. [Google Scholar] [CrossRef]
- Guigue, N.; Léon, L.; Hamane, S.; Gits-Muselli, M.; Le Strat, Y.; Alanio, A.; Bretagne, S. Continuous Decline of Toxoplasma Gondii Seroprevalence in Hospital: A 1997–2014 Longitudinal Study in Paris, France. Front. Microbiol. 2018, 9, 2369. [Google Scholar] [CrossRef]
- Amin, A.; Mazloomzadeh, S.; Haniloo, A.; Mohammadian, F.; Fazaeli, A. Evaluation of Anti-Toxoplasma IgG, IgM, and IgA in Mothers with Spontaneous Abortion in Zanjan, Northwest Iran. Korean J. Parasitol. 2012, 50, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Gontijo da Silva, M.; Clare Vinaud, M.; de Castro, A.M. Prevalence of Toxoplasmosis in Pregnant Women and Vertical Transmission of Toxoplasma Gondii in Patients from Basic Units of Health from Gurupi, Tocantins, Brazil, from 2012 to 2014. PLoS ONE 2015, 10, e0141700. [Google Scholar] [CrossRef]
- Berredjem, H.; Aouras, H.; Benlaifa, M.; Becheker, I.; Djebar, M.R. Contribution of IgG Avidity and PCR for the Early Diagnosis of Toxoplasmosis in Pregnant Women from the North-Eastern Region of Algeria. Afr. Health Sci. 2017, 17, 647–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murata, F.H.A.; Ferreira, M.N.; Camargo, N.S.; Santos, G.S.; Spegiorin, L.C.J.F.; Silveira-Carvalho, A.P.; Pereira-Chioccola, V.L.; de Mattos, L.C.; de Mattos, C.C.B. Frequency of Anti- Toxoplasma Gondii IgA, IgM, and IgG Antibodies in High-Risk Pregnancies, in Brazil. Rev. Soc. Bras. Med. Trop. 2016, 49, 512–514. [Google Scholar] [CrossRef] [Green Version]
- Foudrinier, F.; Marx-Chemla, C.; Aubert, D.; Bonhomme, A.; Pinon, J.M. Value of Specific Immunoglobulin A Detection by Two Immunocapture Assays in the Diagnosis of Toxoplasmosis. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 1995, 14, 585–590. [Google Scholar] [CrossRef]
- Stepick-Biek, P.; Thulliez, P.; Araujo, F.G.; Remington, J.S. IgA Antibodies for Diagnosis of Acute Congenital and Acquired Toxoplasmosis. J. Infect. Dis. 1990, 162, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Liesenfeld, O.; Montoya, J.G.; Kinney, S.; Press, C.; Remington, J.S. Effect of Testing for IgG Avidity in the Diagnosis of Toxoplasma Gondii Infection in Pregnant Women: Experience in a US Reference Laboratory. J. Infect. Dis. 2001, 183, 1248–1253. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.L.; Kruszon-Moran, D.; Elder, S.; Rivera, H.N.; Press, C.; Montoya, J.G.; McQuillan, G.M. Toxoplasma gondii Infection in the United States, 2011-2014. Am. J. Trop. Med. Hyg. 2018, 98, 551–557. [Google Scholar] [CrossRef] [Green Version]
- Pinto-Ferreira, F.; Caldart, E.T.; Pasquali, A.K.S.; Mitsuka-Breganó, R.; Freire, R.L.; Navarro, I.T. Patterns of Transmission and Sources of Infection in Outbreaks of Human Toxoplasmosis. Emerg. Infect. Dis. 2019, 25, 2177–2182. [Google Scholar] [CrossRef]


{kind=link}
| Prevalence of T. gondii Infection Univariate Analysis | ||||
|---|---|---|---|---|
| Variables | No. Tested | N (%) | OR (95% CI) | p Value |
| Age groups (years) | ||||
| 15–24 | 285 | 101 (35.44) | 1 (Ref.) | |
| 25–34 | 779 | 347 (44.54) | 1.46 (1.11–1.94) | 0.007 |
| 35–45 | 253 | 159 (62.85) | 3.08 (2.17–4.38) | <0.001 |
| Total | 1317 | 607 (46.09) | - | |
| Result(s) for Individual Serum Samples | No. (%) of Females Aged 15–45 Years with Detectable T. gondii IgG Antibodies |
|---|---|
| IgM (+) | 54 (8.90) |
| IgM (−) | 553 (91.10) |
| IgA (+) | 10 (1.65) |
| IgA (−) | 597 (98.35) |
| IgM (+), IgA (+) | 6 (0.99) |
| IgM (+), IgA (−) | 48 (7.91) |
| IgM (−), IgA (+) | 4 (0.66) |
| IgM (−), IgA (−) | 549 (90.44) |
| Serologic Tests | IgG Avidity Assay | No. of Samples Tested | |
|---|---|---|---|
| Low or Equivocal | High | ||
| No. (%) of Samples | No. (%) of Samples | ||
| IgM (+) | 7 (12.96) | 47 (87.04) | 54 |
| IgM (−) | 0 (0) | 4 (100) | 4 |
| IgA (+) | 4 (40) | 6 (60) | 10 |
| IgA (−) | 3 (6.25) | 45 (93.75) | 48 |
| IgM (+), IgA (+) | 4 (66.67) | 2 (33.33) | 6 |
| IgM (+), IgA (−) | 3 (6.25) | 45 (93.75) | 48 |
| IgM (−), IgA (+) | 0 (0) | 4 (100) | 4 |
| IgG Avidity | IgG Avidity Test Interpretation | No. of Females Tested | No. (%) of Females Tested Positive | |
|---|---|---|---|---|
| IgM | IgA | |||
| 0.0–0.19 | low avidity | 4 | 4 (100) | 3 (75) |
| 0.20–0.29 | equivocal | 3 | 3 (100) | 1 (33.33) |
| ≥0.3 | high avidity | 51 | 47 (92.16) | 6 (11.76) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihu, A.G.; Lupu, M.A.; Nesiu, A.; Marti, D.T.; Olariu, T.R. Screening for the Detection of Toxoplasma gondii IgG, IgM and IgA in Females of Reproductive Age from Western Romania. Life 2022, 12, 1771. https://doi.org/10.3390/life12111771
Mihu AG, Lupu MA, Nesiu A, Marti DT, Olariu TR. Screening for the Detection of Toxoplasma gondii IgG, IgM and IgA in Females of Reproductive Age from Western Romania. Life. 2022; 12(11):1771. https://doi.org/10.3390/life12111771
Chicago/Turabian StyleMihu, Alin Gabriel, Maria Alina Lupu, Alexandru Nesiu, Daniela Teodora Marti, and Tudor Rares Olariu. 2022. "Screening for the Detection of Toxoplasma gondii IgG, IgM and IgA in Females of Reproductive Age from Western Romania" Life 12, no. 11: 1771. https://doi.org/10.3390/life12111771