
Negative Impact of the UEFA European Soccer Championship on Central Hemodynamics and Arterial Stiffness: A Multicenter Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort and Design
2.2. Measurement of Peripheral and Central Blood Pressure and Arterial Stiffness
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
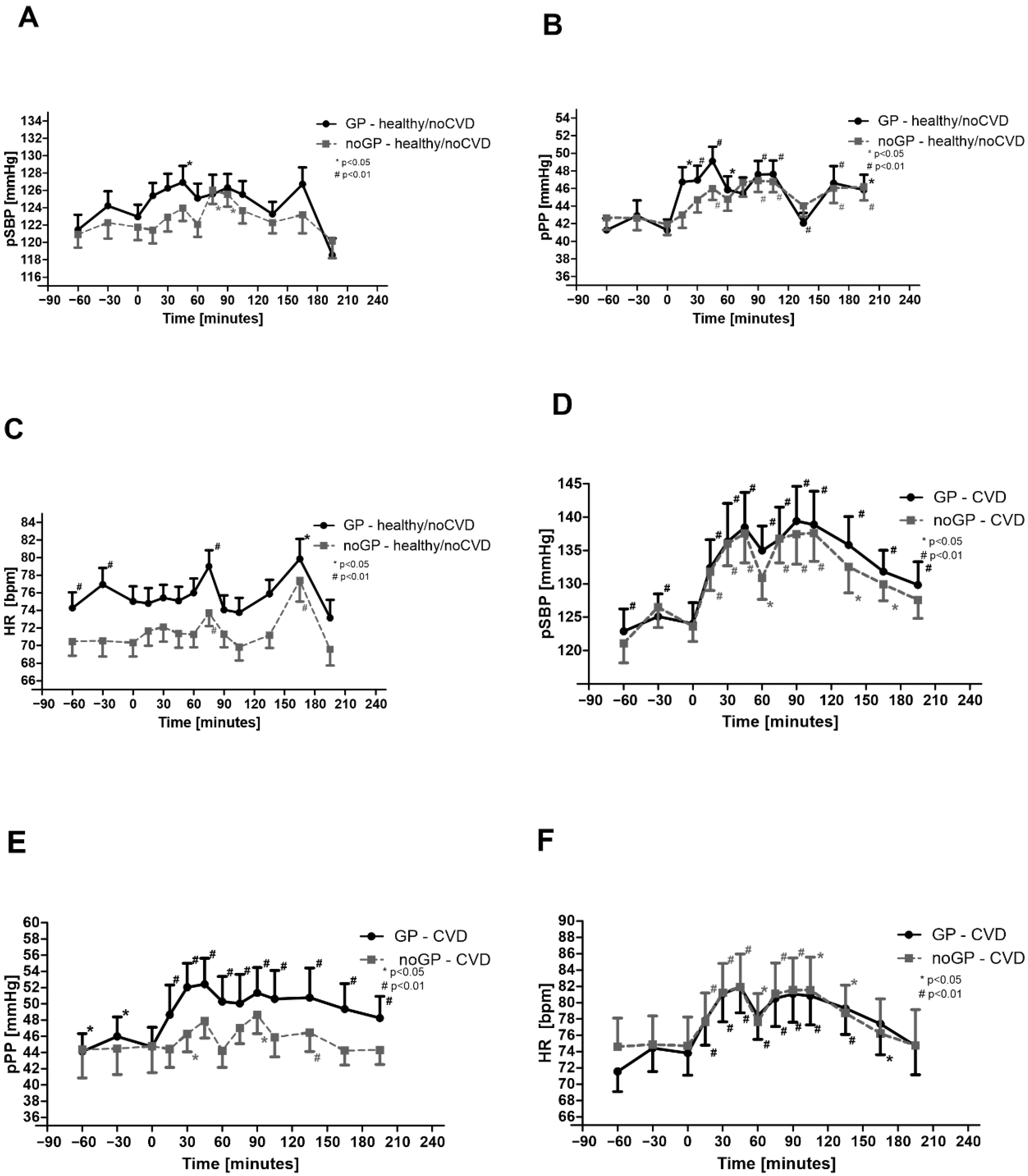
3.2. Peripheral Hemodynamics Are Increased by Watching Soccer Games—Effects in noCVD
3.3. Peripheral Hemodynamics Are Increased by Watching Soccer Games—Effects in CVD
3.4. Central Hemodynamics Are Increased by Watching Soccer Games—Effects in noCVD
3.5. Central Hemodynamics Are Increased by Watching Soccer Games—Effects in CVD
3.6. Total Vascular Resistance and Pulse Wave Velocity in noCVD
3.7. Total Vascular Resistance and Pulse Wave Velocity in CVD
3.8. Comparison of noCVD and CVD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilbert-Lampen, U.; Nickel, T.; Scheipl, F.; Greven, S.; Küchenhoff, H.; Kääb, S.; Steinbeck, G. Mortality Due to Myocardial Infarction in the Bavarian Population during World Cup Soccer 2006. Clin. Res. Cardiol. 2011, 100, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Niederseer, D.; Thaler, C.W.; Egger, A.; Niederseer, M.C.; Plöderl, M.; Niebauer, J. Watching Soccer Is Not Associated with an Increase in Cardiac Events. Int. J. Cardiol. 2013, 170, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Reppel, M.; Franzen, K.; Bode, F.; Weil, J.; Kurowski, V.; Schneider, S.A.; Baulmann, J.; von Lukowicz, T.; Mirau, W.; Mortensen, E.; et al. Central Hemodynamics and Arterial Stiffness during the Finals of the World Cup Soccer Championship 2010. Int. J. Cardiol. 2013, 166, 627–632. [Google Scholar] [CrossRef]
- Crestani, C.C. Adolescent Vulnerability to Cardiovascular Consequences of Chronic Emotional Stress: Review and Perspectives for Future Research. Neurosci. Biobehav. Rev. 2017, 74, 466–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westcott, S.K.; Beach, L.Y.; Matsushita, F.; Albert, C.M.; Chatterjee, N.; Wong, J.; Williams, D.R.; Vinayagamoorthy, M.; Buring, J.E.; Albert, M.A. Relationship Between Psychosocial Stressors and Atrial Fibrillation in Women >45 Years of Age. Am. J. Cardiol. 2018, 122, 1684–1687. [Google Scholar] [CrossRef] [PubMed]
- Smyth, A.; O’Donnell, M.; Lamelas, P.; Teo, K.; Rangarajan, S.; Yusuf, S. INTERHEART Investigators Physical Activity and Anger or Emotional Upset as Triggers of Acute Myocardial Infarction: The INTERHEART Study. Circulation 2016, 134, 1059–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chida, Y.; Steptoe, A. Greater Cardiovascular Responses to Laboratory Mental Stress Are Associated with Poor Subsequent Cardiovascular Risk Status: A Meta-Analysis of Prospective Evidence. Hypertension 2010, 55, 1026–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilbert-Lampen, U.; Nickel, T.; Leistner, D.; Güthlin, D.; Matis, T.; Völker, C.; Sper, S.; Küchenhoff, H.; Kääb, S.; Steinbeck, G. Modified Serum Profiles of Inflammatory and Vasoconstrictive Factors in Patients with Emotional Stress-Induced Acute Coronary Syndrome during World Cup Soccer 2006. J. Am. Coll. Cardiol. 2010, 55, 637–642. [Google Scholar] [CrossRef]
- Witte, D.R.; Bots, M.L.; Hoes, A.W.; Grobbee, D.E. Cardiovascular Mortality in Dutch Men during 1996 European Football Championship: Longitudinal Population Study. BMJ 2000, 321, 1552–1554. [Google Scholar] [CrossRef] [Green Version]
- Carroll, D.; Ebrahim, S.; Tilling, K.; Macleod, J.; Smith, G.D. Admissions for Myocardial Infarction and World Cup Football: Database Survey. BMJ 2002, 325, 1439–1442. [Google Scholar] [CrossRef]
- Wilbert-Lampen, U.; Leistner, D.; Greven, S.; Pohl, T.; Sper, S.; Völker, C.; Güthlin, D.; Plasse, A.; Knez, A.; Küchenhoff, H.; et al. Cardiovascular Events during World Cup Soccer. N. Engl. J. Med. 2008, 358, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Borges, D.G.S.; Monteiro, R.A.; Schmidt, A.; Pazin-Filho, A. World Soccer Cup as a Trigger of Cardiovascular Events. Arq. Bras. Cardiol. 2013, 100, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Barone-Adesi, F.; Vizzini, L.; Merletti, F.; Richiardi, L. It Is Just a Game: Lack of Association between Watching Football Matches and the Risk of Acute Cardiovascular Events. Int. J. Epidemiol. 2010, 39, 1006–1013. [Google Scholar] [CrossRef] [PubMed]
- Jauss, M.; Sitzer, M.; Stolz, E.; Misselwitz, B.; Rosenow, F. Lack of Increase of Cerebrovascular Events during German World Cup Soccer Games in 2006. J. Neurol. 2009, 256, 863–866. [Google Scholar] [CrossRef]
- van Popele, N.M.; Grobbee, D.E.; Bots, M.L.; Asmar, R.; Topouchian, J.; Reneman, R.S.; Hoeks, A.P.; van der Kuip, D.A.; Hofman, A.; Witteman, J.C. Association between Arterial Stiffness and Atherosclerosis: The Rotterdam Study. Stroke 2001, 32, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Sutton-Tyrrell, K.; Najjar, S.S.; Boudreau, R.M.; Venkitachalam, L.; Kupelian, V.; Simonsick, E.M.; Havlik, R.; Lakatta, E.G.; Spurgeon, H.; Kritchevsky, S.; et al. Elevated Aortic Pulse Wave Velocity, a Marker of Arterial Stiffness, Predicts Cardiovascular Events in Well-Functioning Older Adults. Circulation 2005, 111, 3384–3390. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Wang, N.; Palmisano, J.N.; Larson, M.G.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J.; Vasan, R.S. Hemodynamic Correlates of Blood Pressure across the Adult Age Spectrum: Noninvasive Evaluation in the Framingham Heart Study. Circulation 2010, 122, 1379–1386. [Google Scholar] [CrossRef] [Green Version]
- Baulmann, J.; Nürnberger, J.; Slany, J.; Schmieder, R.; Schmidt-Trucksäss, A.; Baumgart, D.; Cremerius, P.; Hess, O.; Mortensen, K.; Weber, T. Arterielle Gefäßsteifigkeit und Pulswellenanalyse. Dtsch. Med. Wochenschr. 2010, 135, S4–S14. [Google Scholar] [CrossRef]
- Townsend, R.R.; Wilkinson, I.B.; Schiffrin, E.L.; Avolio, A.P.; Chirinos, J.A.; Cockcroft, J.R.; Heffernan, K.S.; Lakatta, E.G.; McEniery, C.M.; Mitchell, G.F.; et al. Recommendations for Improving and Standardizing Vascular Research on Arterial Stiffness: A Scientific Statement From the American Heart Association. Hypertension 2015, 66, 698–722. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial Stiffness and Cardiovascular Events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef]
- Agabiti-Rosei, E.; Mancia, G.; O’Rourke, M.F.; Roman, M.J.; Safar, M.E.; Smulyan, H.; Wang, J.-G.; Wilkinson, I.B.; Williams, B.; Vlachopoulos, C. Central Blood Pressure Measurements and Antihypertensive Therapy: A Consensus Document. Hypertension 2007, 50, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Roman, M.J.; Devereux, R.B.; Kizer, J.R.; Lee, E.T.; Galloway, J.M.; Ali, T.; Umans, J.G.; Howard, B.V. Central Pressure More Strongly Relates to Vascular Disease and Outcome than Does Brachial Pressure: The Strong Heart Study. Hypertension 2007, 50, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, C.; Kosmopoulou, F.; Alexopoulos, N.; Ioakeimidis, N.; Siasos, G.; Stefanadis, C. Acute Mental Stress Has a Prolonged Unfavorable Effect on Arterial Stiffness and Wave Reflections. Psychosom. Med. 2006, 68, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Hinterdobler, J.; Schunkert, H.; Kessler, T.; Sager, H.B. Impact of Acute and Chronic Psychosocial Stress on Vascular Inflammation. Antioxid. Redox Signal. 2021, 35, 1531–1550. [Google Scholar] [CrossRef]
- Roman, M.J.; Devereux, R.B.; Kizer, J.R.; Okin, P.M.; Lee, E.T.; Wang, W.; Umans, J.G.; Calhoun, D.; Howard, B.V. High Central Pulse Pressure Is Independently Associated with Adverse Cardiovascular Outcome the Strong Heart Study. J. Am. Coll. Cardiol. 2009, 54, 1730–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Bortel, L.M.; Duprez, D.; Starmans-Kool, M.J.; Safar, M.E.; Giannattasio, C.; Cockcroft, J.; Kaiser, D.R.; Thuillez, C. Clinical Applications of Arterial Stiffness, Task Force III: Recommendations for User Procedures. Am. J. Hypertens. 2002, 15, 445–452. [Google Scholar] [CrossRef] [Green Version]
- Wassertheurer, S.; Kropf, J.; Weber, T.; van der Giet, M.; Baulmann, J.; Ammer, M.; Hametner, B.; Mayer, C.C.; Eber, B.; Magometschnigg, D. A New Oscillometric Method for Pulse Wave Analysis: Comparison with a Common Tonometric Method. J. Hum. Hypertens. 2010, 24, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.; Wassertheurer, S.; Rammer, M.; Maurer, E.; Hametner, B.; Mayer, C.C.; Kropf, J.; Eber, B. Validation of a Brachial Cuff-Based Method for Estimating Central Systolic Blood Pressure. Hypertension 2011, 58, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H.; et al. Expert Consensus Document on Arterial Stiffness: Methodological Issues and Clinical Applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinterdobler, J.; Schott, S.; Jin, H.; Meesmann, A.; Steinsiek, A.-L.; Zimmermann, A.-S.; Wobst, J.; Müller, P.; Mauersberger, C.; Vilne, B.; et al. Acute Mental Stress Drives Vascular Inflammation and Promotes Plaque Destabilization in Mouse Atherosclerosis. Eur. Heart J. 2021, 42, 4077–4088. [Google Scholar] [CrossRef]
- Nunan, D.; Wassertheurer, S.; Lasserson, D.; Hametner, B.; Fleming, S.; Ward, A.; Heneghan, C. Assessment of Central Haemomodynamics from a Brachial Cuff in a Community Setting. BMC Cardiovasc. Disord. 2012, 12, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steptoe, A.; Kivimäki, M. Stress and Cardiovascular Disease. Nat. Rev. Cardiol. 2012, 9, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Eisenhofer, G.; Friberg, P.; Rundqvist, B.; Quyyumi, A.A.; Lambert, G.; Kaye, D.M.; Kopin, I.J.; Goldstein, D.S.; Esler, M.D. Cardiac Sympathetic Nerve Function in Congestive Heart Failure. Circulation 1996, 93, 1667–1676. [Google Scholar] [CrossRef] [PubMed]
- Esler, M.; Kaye, D.; Lambert, G.; Esler, D.; Jennings, G. Adrenergic Nervous System in Heart Failure. Am. J. Cardiol. 1997, 80, 7L–14L. [Google Scholar] [CrossRef]
- Reference Values for Arterial Stiffness’ Collaboration. Determinants of Pulse Wave Velocity in Healthy People and in the Presence of Cardiovascular Risk Factors: “Establishing Normal and Reference Values”. Eur. Heart J. 2010, 31, 2338–2350. [Google Scholar] [CrossRef]
- Eckberg, D.L.; Drabinsky, M.; Braunwald, E. Defective Cardiac Parasympathetic Control in Patients with Heart Disease. N. Engl. J. Med. 1971, 285, 877–883. [Google Scholar] [CrossRef]
- Clague, J.; Bernstein, L. Physical Activity and Cancer. Curr. Oncol. Rep. 2012, 14, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Meisel, S.R.; Kutz, I.; Dayan, K.I.; Pauzner, H.; Chetboun, I.; Arbel, Y.; David, D. Effect of Iraqi Missile War on Incidence of Acute Myocardial Infarction and Sudden Death in Israeli Civilians. Lancet 1991, 338, 660–661. [Google Scholar] [CrossRef]
- Steptoe, A.; Kivimäki, M. Stress and Cardiovascular Disease: An Update on Current Knowledge. Annu. Rev. Public Health 2013, 34, 337–354. [Google Scholar] [CrossRef]
- Ono, R.; Falcão, L.M. Takotsubo Cardiomyopathy Systematic Review: Pathophysiologic Process, Clinical Presentation and Diagnostic Approach to Takotsubo Cardiomyopathy. Int. J. Cardiol. 2016, 209, 196–205. [Google Scholar] [CrossRef]
- Dimsdale, J.E. Psychological Stress and Cardiovascular Disease. J. Am. Coll. Cardiol. 2008, 51, 1237–1246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crestani, C.C. Emotional Stress and Cardiovascular Complications in Animal Models: A Review of the Influence of Stress Type. Front. Physiol. 2016, 7, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubzansky, L.D.; Huffman, J.C.; Boehm, J.K.; Hernandez, R.; Kim, E.S.; Koga, H.K.; Feig, E.H.; Lloyd-Jones, D.M.; Seligman, M.E.P.; Labarthe, D.R. Positive Psychological Well-Being and Cardiovascular Disease: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1382–1396. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| UEFA European Soccer Championship 2012—Poland/Ukraine | ||
| noGP | GP | |
| Group stage | Ireland/Croatia | Germany/Portugal |
| (1:3, 10 June 2012, 8:45 p.m.) | (1:0, 9 June 2012, 8:45 p.m.) | |
| Spain/Ireland | The Netherlands/Germany | |
| (4:0, 14 June 2012, 8:45 p.m.) | (1:2, 13 June 2012, 8:45 p.m.) | |
| Czech Republic/Poland | Denmark/Germany | |
| (1:0, 16 June 2012, 8:45 p.m.) | (1:2, 17 June 2012, 8:45 p.m.) | |
| Quarterfinals | Czech Republic/Portugal | Germany/Greece |
| (0:1, 21 June 2012, 8:45 p.m.) | (4:2, 22 June 2012, 8:45 p.m.) | |
| Semifinals | Portugal/Spain | Germany/Italy |
| (2:4, 27 June 2012, 8:45 p.m.) | (1:2, 28 June 2012, 8:45 p.m.) | |
| UEFA European Soccer Championship 2021—Europe | ||
| noGP | GP | |
| Group stage | Spain/Sweden | France/Germany |
| (0:0, 14 June 2012, 9:00 p.m.) | (1:0, 15 June 2012, 9:00 p.m.) | |
| Croatia/Czech Republic | Portugal/Germany | |
| (1:1, 18 June 2012, 6:00 p.m.) | (2:4, 19 June 2012, 6:00 p.m.) | |
| Czech Republic/England | Germany/Hungary | |
| (0:1, 22 June 2012, 9:00 p.m.) | (2:2, 23 June 2012, 9:00 p.m.) | |
| Round of 16 | Croatia/Spain | England/Germany |
| (3:5, 28 June 2012, 6:00 p.m.) | (2:0, 29 June 2012, 6:00 p.m.) | |
| Baseline Characteristics | |||
|---|---|---|---|
| All (n = 70) | Healthy/noCVD (n = 52) | CVD (n = 18) | |
| Age (years) | 37 ± 11 | 29 ± 8 | 54 ± 9 |
| Sex | 35 male, 35 female | 23 male; 29 female | 12 male; 6 female |
| Height (m) | 1.54 ± 6.5 | 154.9 ± 7.4 | 1.50 ± 13.6 |
| Weight (kg) | 73.4 ± 1.6 | 70.2 ± 1.7 | 81.6 ± 3.4 |
| Smoking (%) | 11.6 | 0 | 42.1 |
| Arterial hypertension (%) | 24.6 | 0 | 84.2 |
| Diabetes mellitus Type 1 and 2 (%) | 8.7 | 0 | 26.3 |
| ACS (%) | 11.6 | 0 | 42.1 |
| STEMI (%) | 8.7 | 0 | 31.6 |
| NSTEMI (%) | 7.2 | 0 | 26.3 |
| Coronary heart disease (%) | 13.0 | 0 | 47.4 |
| Heart failure—NYHA 1–2 (%) | 8.7 | 0 | 31.6 |
| Heart failure—NYHA 3 (%) | 2.9 | 0 | 10.5 |
| Atrial fibrillation (%) | 1.4 | 0 | 5.3 |
| Mitral valve insufficiency (%) | 1.4 | 0 | 5.3 |
| Tricuspidal valve insufficiency (%) | 1.4 | 0 | 5.3 |
| ICD (%) | 5.8 | 0 | 21.1 |
| Chronic kidney disease (%) | 4.3 | 0 | 15.8 |
| Hyperlipoproteinemia (%) | 8.7 | 0 | 31.6 |
| Arterial occlusive disease (%) | 1.4 | 0 | 5.3 |
| Bronchial asthma (%) | 1.4 | 2 | 0 |
| Beta blocker (%) | 15.9 | 0 | 57.9 |
| Aspirin (%) | 11.6 | 0 | 36.8 |
| Spironolactone (%) | 7.2 | 0 | 26.3 |
| ACE inhibitors (%) | 14.5 | 0 | 52.6 |
| ARB (%) | 2.9 | 0 | 10.5 |
| Statins (%) | 20.3 | 0 | 73.7 |
| Ticagrelor (%) | 1.4 | 0 | 5.3 |
| Clopidogrel (%) | 5.8 | 0 | 21.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzen, K.F.; Mortensen, K.; Ott, C.; Herber, K.; Busse, M.; Söling, C.; Schneppe, D.; Lässig, S.; Dörr, M.; Tilz, R.; et al. Negative Impact of the UEFA European Soccer Championship on Central Hemodynamics and Arterial Stiffness: A Multicenter Study. Life 2022, 12, 1696. https://doi.org/10.3390/life12111696
Franzen KF, Mortensen K, Ott C, Herber K, Busse M, Söling C, Schneppe D, Lässig S, Dörr M, Tilz R, et al. Negative Impact of the UEFA European Soccer Championship on Central Hemodynamics and Arterial Stiffness: A Multicenter Study. Life. 2022; 12(11):1696. https://doi.org/10.3390/life12111696
Chicago/Turabian StyleFranzen, Klaas F., Kai Mortensen, Christian Ott, Katrin Herber, Marlene Busse, Charlotte Söling, Daniel Schneppe, Saskia Lässig, Marcus Dörr, Roland Tilz, and et al. 2022. "Negative Impact of the UEFA European Soccer Championship on Central Hemodynamics and Arterial Stiffness: A Multicenter Study" Life 12, no. 11: 1696. https://doi.org/10.3390/life12111696