
Long Term Results of Reduction Ascending Aortoplasty
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
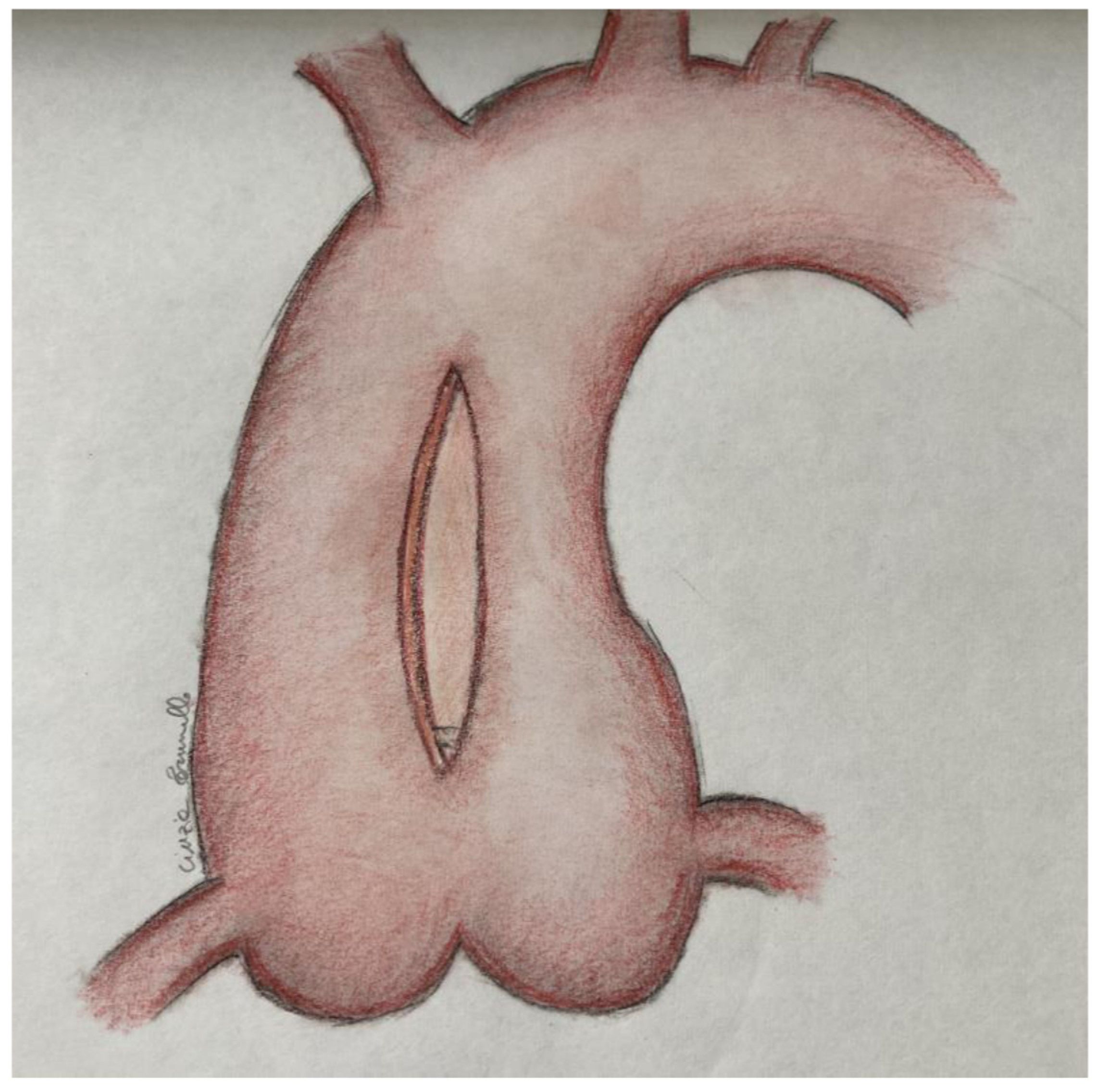
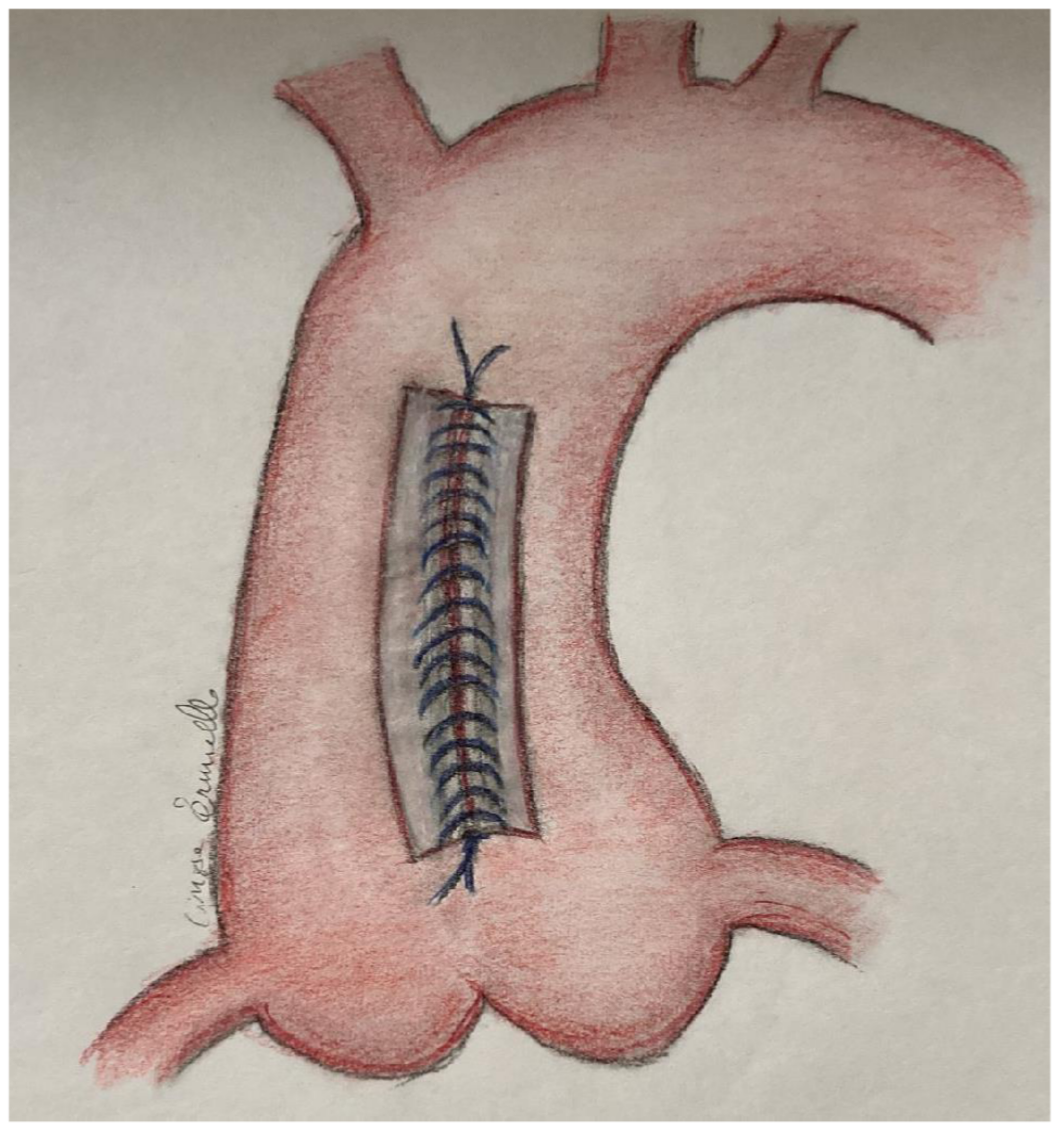
2.1. Surgery
2.2. Statistical Analysis
3. Results
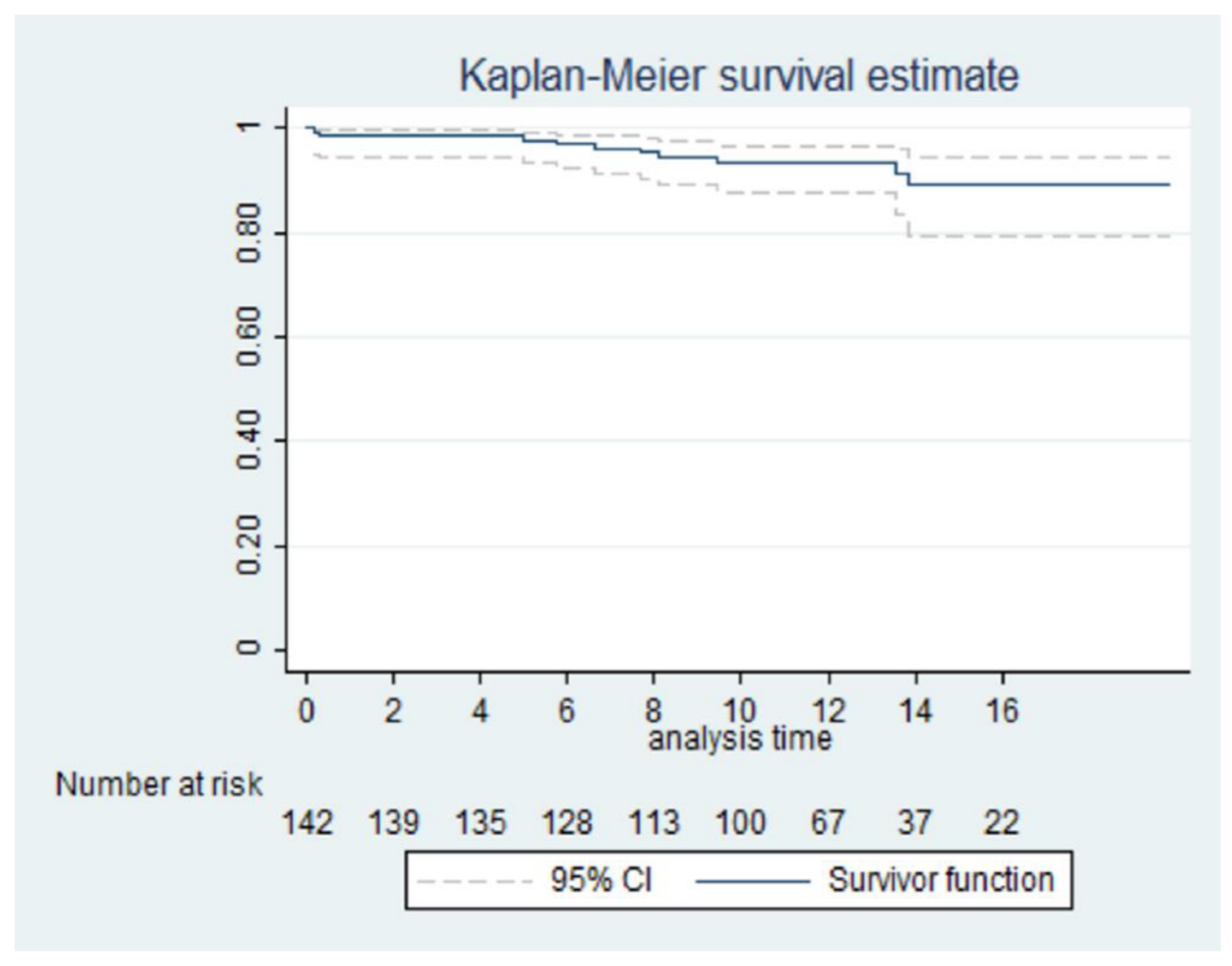
3.1. Follow Up
3.2. Cardiac Death
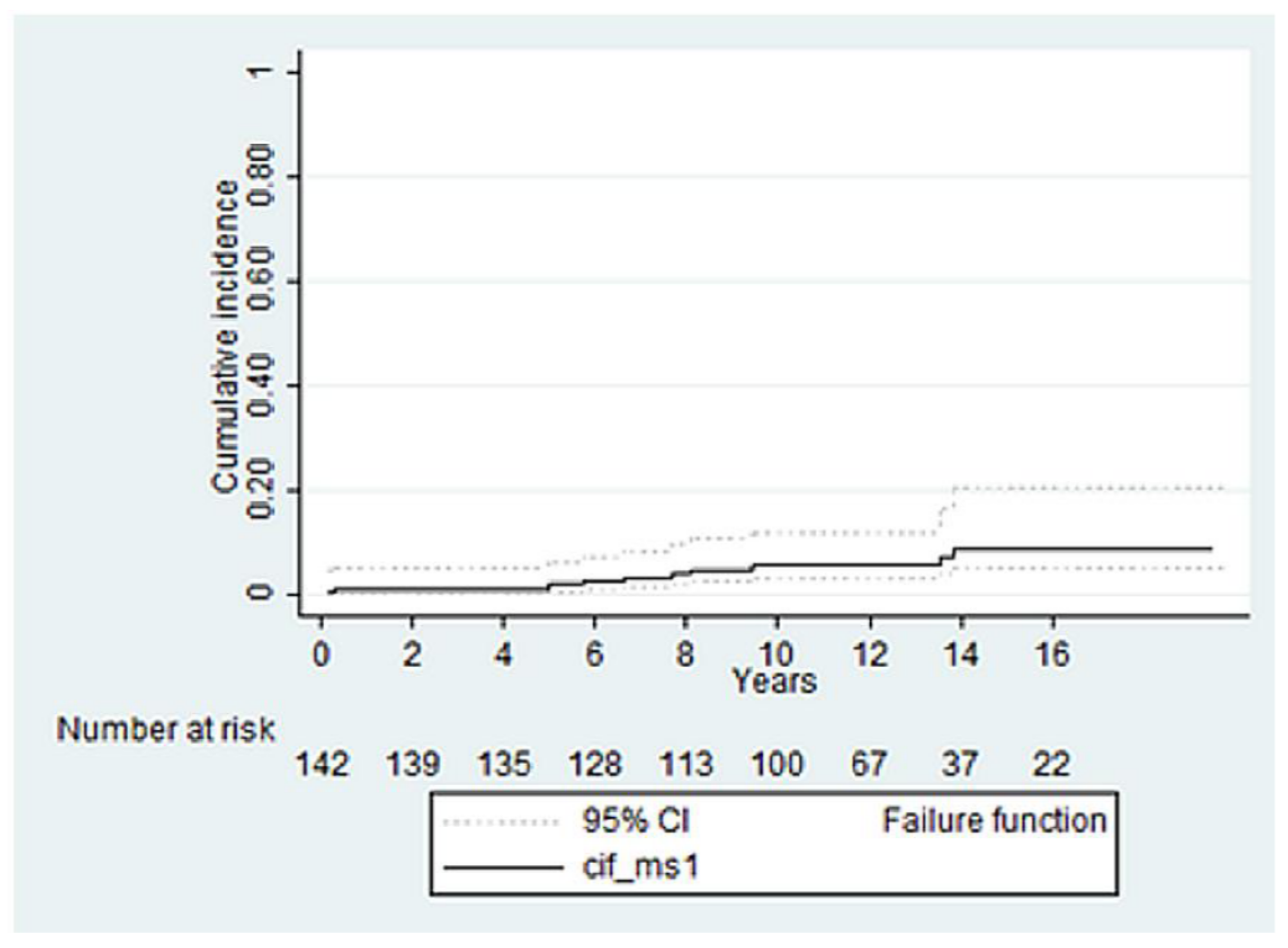
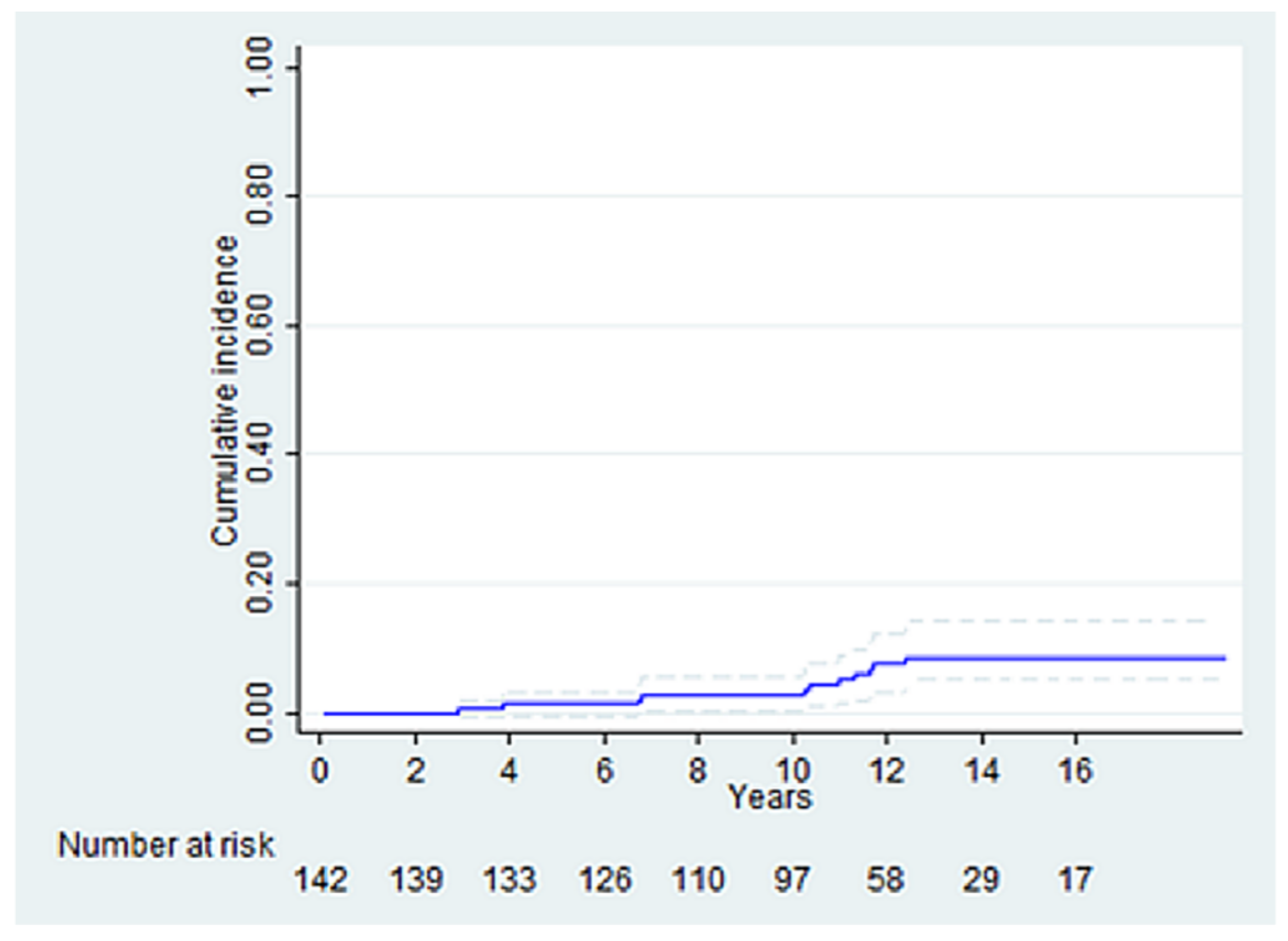
3.3. Ascending Aorta Re-Intervention
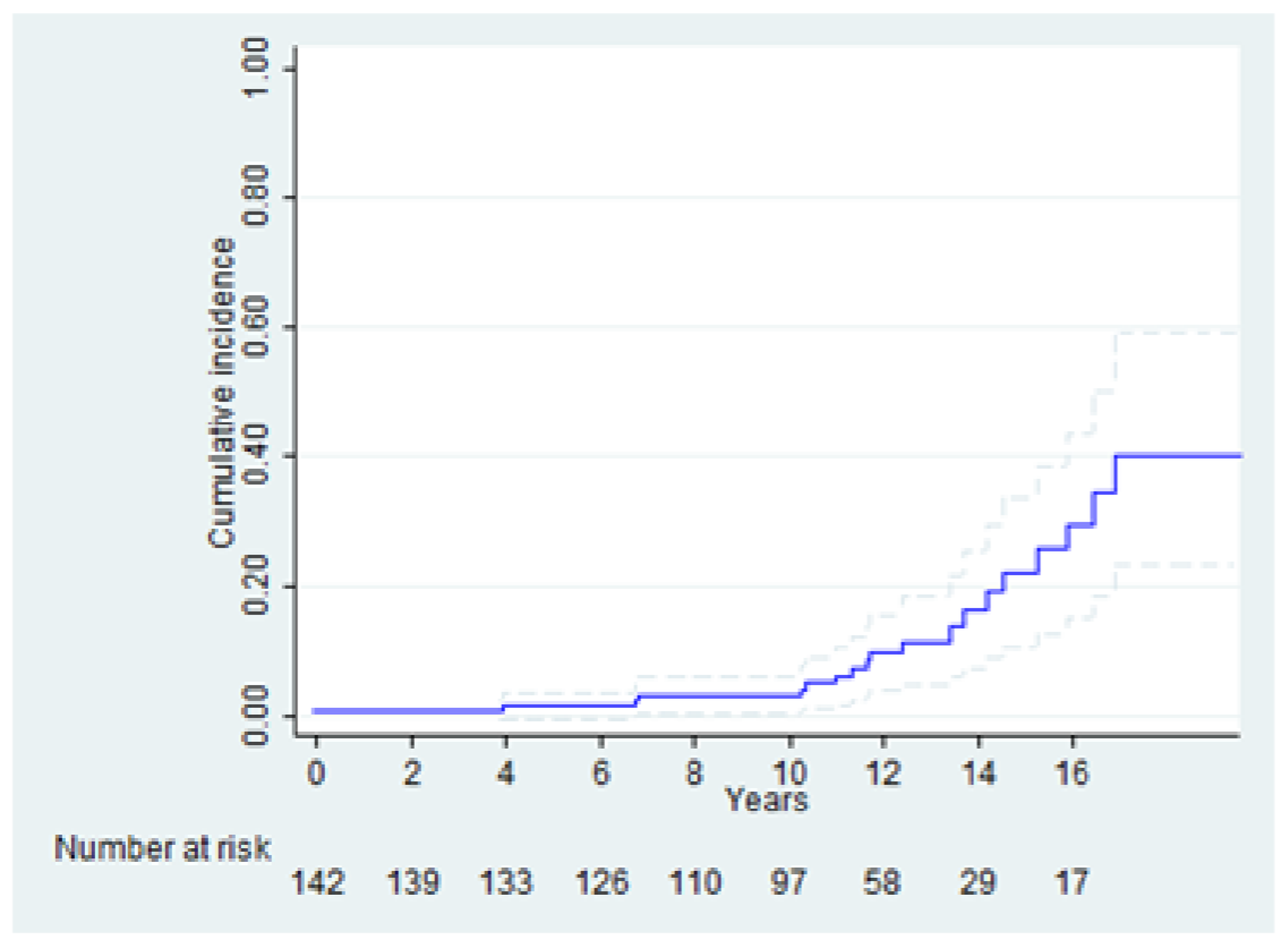
3.4. Aortic-Related Events
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roman, M.J.; Devereux, R.B.; Kramer-Fox, R.; O’Loughlin, J. Two-dimensional echocardiographic aortic root dimensions in normal children and adults. Am. J. Cardiol. 1989, 64, 507–512. [Google Scholar] [CrossRef]
- Rogers, I.S.; Massaro, J.M.; Truong, Q.A.; Mahabadi, A.A.; Kriegel, M.F.; Fox, C.S.; Thanassoulis, G.; Isselbacher, E.M.; Hoffmann, U.; Odonnell, C.J. Distribution, determinants, and normal reference values of thoracic and abdominal aortic diameters by computed tomography (from the Framingham Heart Study). Am. J. Cardiol. 2013, 111, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Devereux, R.B.; de Simone, G.; Arnett, D.K.; Best, L.G.; Boerwinkle, E.; Howard, B.V.; Kitzman, D.; Lee, E.T.; Mosley, T.H.; Weder, A. Normal limits in relation to age, body size and gender of two-dimensional echocardiographic aortic root dimensions in persons ≥15 years of age. Am. J. Cardiol. 2012, 110, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Kälsch, H.; Lehmann, N.; Möhlenkamp, S.; Becker, A.; Moebus, S.; Schmermund, A.; Stang, A.; Mahabadi, A.A.; Mann, K.; Jöckel, K.-H.; et al. Body-surface adjusted aortic reference diameters for improved identification of patients with thoracic aortic aneurysms: Results from the population-based Heinz Nixdorf Recall study. Int. J. Cardiol. 2013, 163, 72–78. [Google Scholar] [CrossRef]
- Vriz, O.; Driussi, C.; Bettio, M.; Ferrara, F.; D’Andrea, A.; Bossone, E. Aortic root dimensions and stiffness in healthy subjects. Am. J. Cardiol. 2013, 112, 1224–1229. [Google Scholar] [CrossRef]
- Lam, C.S.P.; Xanthakis, V.; Sullivan, L.M.; Lieb, W.; Aragam, J.; Redfield, M.M.; Mitchell, G.F.; Benjamin, E.J.; Vasan, R.S. Aortic Root Remodeling over the Adult Life Course. Circulation 2010, 122, 884–890. [Google Scholar] [CrossRef]
- Braverman, A.C.; Thompson, R.W.; Sanchez, L.A. Braunwald’s Heart Disease, 9th ed.; Elsevier: Philadelphia, PA, USA, 2012. [Google Scholar]
- Members, A.F.; Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Bartolomeo, R.D.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar]
- Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; Kazerooni, E.A.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010, 121, e266–e369. [Google Scholar]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; Bonis, M.D.; Paulis, R.D.; et al. ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. Cardiovasc. Imaging 2022, 43, 561–632. [Google Scholar]
- Bahnson, H.T. The dilemma of the ascending aortic aneurysm. Ann. Thorac. Surg. 1982, 34, 115–116. [Google Scholar] [CrossRef]
- Kim, H.-H.; Lee, S.; Lee, S.H.; Youn, Y.-N.; Yoo, K.-J.; Joo, H.C. The long-term fate of ascending aorta aneurysm after wrapping versus replacement. J. Thorac. Cardiovasc. Surg. 2022, 164, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Carlestål, E.; Ezer, M.S.; Franco-Cereceda, A.; Olsson, C. Proximal aortic repair in asymptomatic patients. JTCVS Open 2021, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Prenger, K.; Pieters, F.; Cheriex, E. Aortic dissection after aortic valve replacement: Incidence and consequences for strategy. J. Card. Surg. 1994, 9, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Davies, R.R.; Goldstein, L.J.; Coady, M.A.; Tittle, S.L.; Rizzo, J.A.; Kopf, G.S.; Elefteriades, J.A. Yearly rupture or dissection rates for thoracic aortic aneurysms: Simple prediction based on size. Ann. Thorac. Surg. 2002, 73, 17–28. [Google Scholar] [CrossRef]
- Robicsek, F. A new method to treat fusiform aneurysms of the ascending aorta associated with aortic valve disease: An alternative to radical resection. Ann. Thorac. Surg. 1982, 34, 92–94. [Google Scholar] [CrossRef]
- Kim, J.B.; Spotnitz, M.; Lindsay, M.E.; MacGillivray, T.E.; Isselbacher, E.M.; Sundt, T.M., III. Risk of Aortic Dissection in the Moderately Dilated Ascending Aorta. J. Am. Coll. Cardiol. 2016, 68, 1209–1219. [Google Scholar] [CrossRef]
- Kim, E.K.; Choi, S.H.; Sung, K.; Kim, W.S.; Choe, Y.H.; Oh, J.K.; Kim, D.-K. Aortic diameter predicts acute type A aortic dissection in patients with Marfan syndrome but not in patients without Marfan syndrome. J. Thorac. Cardiovasc. Surg. 2014, 147, 1505–1510. [Google Scholar] [CrossRef]
- Kiessling, A.H.; Odwody, E.; Doss, M.; Metentzidou, K.; Miskovic, A.; Moritz, A. Midterm follow up in patients with reduction ascending aortoplasty. J. Cardiothorac. Surg. 2014, 9, 120. [Google Scholar] [CrossRef]
- Choi, M.S.; Jeong, D.S.; Lee, H.Y.; Sung, K.; Kim, W.S.; Lee, Y.T.; Park, P.W. Aortic wrapping for a dilated ascending aorta in bicuspid aortic stenosis. Circ. J. 2015, 79, 778–784. [Google Scholar] [CrossRef]
- Arsan, S.; Akgun, S.; Kurtoglu, N.; Yildirim, T.; Tekinsoy, B. Reduction aortoplasty and external wrapping for moderately sized tubular ascending aortic aneurysm with concomitant operations. Ann. Thorac. Surg. 2004, 78, 858–861. [Google Scholar] [CrossRef]
- Ozcan, A.V.; Alşalaldeh, M.; Boysan, E.; Goksin, I. Ascending aortic aneurysm treatment with linear plication and external wrapping technique: Mid-term results. J. Card. Surg. 2013, 28, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Gill, M.; Dunning, J. Is reduction aortoplasty (with or without external wrap) an acceptable alternative to replacement of the dilated ascending aorta? Interact. Cardiovasc. Thorac. Surg. 2009, 9, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Gozdek, M.; Kowalewski, M.; Ruchalski, M.; Malvindi, P.G.; Anisimowicz, L. Mortality benefit after reinforced reduction aortoplasty for dilated ascending aorta. Meta-analysis. Int. J. Cardiol. 2015, 199, 50–52. [Google Scholar] [CrossRef] [PubMed]
- Robicsek, F.; Cook, J.W.; Reames, M.K., Sr.; Skipper, E.R. Size reduction ascending aortoplasty: Is it dead or alive? J. Thorac. Cardiovasc. Surg. 2004, 128, 562–570. [Google Scholar] [CrossRef]
- Neri, E.; Massetti, M.; Tanganelli, P.; Capannini, G.; Carone, E.; Tripodi, A.; Tucci, E.; Sassi, C. Is it only a mechanical matter? Histologic modifications of the aorta underlying external banding. J. Thorac. Cardiovasc. Surg. 1999, 118, 1116–1118. [Google Scholar] [CrossRef]
- Bauer, M.; Grauhan, O.; Hetzer, R. Dislocated wrap after previous reduction aortoplasty causes erosion of the ascending aorta. Ann. Thorac. Surg. 2003, 75, 583–584. [Google Scholar] [CrossRef]
- Walker, T.; Bail, D.H.L.; Gruler, M.; Vonthein, R.; Steger, V.; Ziemer, G. Unsupported reduction ascending aortoplasty: Fate of diameter and of Windkessel function. Ann. Thorac. Surg. 2007, 83, 1047–1053. [Google Scholar] [CrossRef]
- Zhang, H.; Lu, F.; Qu, D.; Han, L.; Xu, J.; Ji, G.; Xu, Z. Treatment of fusiform ascending aortic aneurysms: A comparative study with 2 options. J. Thorac. Cardiovasc. Surg. 2011, 141, 738–743. [Google Scholar] [CrossRef]
- Carrel, T.; von Segesser, L.; Jenni, R.; Gallino, A.; Egloff, L.; Bauer, E.; Laske, A.; Turina, M. Dealing with dilated ascending aorta during aortic valve replacement: Advantages of conservative surgical approach. Eur. J. Cardio-Thorac. Surg. 1991, 5, 137–143. [Google Scholar] [CrossRef]
- Feindt, P.; Litmathe, J.; Börgens, A.; Boeken, U.; Kurt, M.; Gams, E. Is size-reducing ascending aortoplasty with external reinforcement an option in modern aortic surgery? Eur. J. Cardio-Thorac. Surg. 2007, 31, 614–617. [Google Scholar] [CrossRef]
- Bauer, M.; Pasic, M.; Schaffarzyk, R.; Siniawski, H.; Hetzer, R. Reduction aortoplasty for dilatation of the ascending aorta in patients with bicuspid aortic valve. Ann. Thorac. Surg. 2002, 73, 720–724. [Google Scholar] [CrossRef]
- Liu, S.; Shi, Y.; Liu, R.; Tong, M.; Luo, X.; Xu, J. Early Prognosis of Reduction Ascending Aortoplasty in Patients with Aortic Valve Disease: A Single Center’s Experience. Ann. Thorac. Surg. 2017, 103, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Polvani, G.; Barili, F.; Dainese, L.; Topkara, V.K.; Cheema, F.H.; Penza, E.; Ferrarese, S.; Parolari, A.; Alamanni, F.; Biglioli, P. Reduction ascending aortoplasty: Midterm follow-up and predictors of redilatation. Ann. Thorac. Surg. 2006, 82, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Yun, K.L.; Miller, D.C.; Fann, J.I.; Mitchell, R.S.; Robbins, R.C.; Moore, K.A.; Oyer, P.E.; Stinson, E.B.; Shumway, N.E.; Reitz, B.A. Composite valve graft versus separate aortic valve and ascending aortic replacement: Is there still a role for the separate procedure? Circulation 1997, 96, II–368. [Google Scholar]
- Malashenkov, A.I.; Rusanov, N.I.; Muratov, R.M.; Movsesian, R.A.; Fursov, B.A.; Bykova, V.A.; Tsoukerman, G.I. Eight years clinical experience with the replacement of the ascending aorta using composite xenopericardial conduit. Eur. J. Cardio-Thorac. Surg. 2000, 18, 168–173. [Google Scholar] [CrossRef]
- Ehrlich, T.; Federspiel, J.M.; Bohle, R.M.; Schäfers, H.-J. Severe aortic wall degeneration after aortic wrapping. Eur. J. Cardio-Thorac. Surg. 2021, 60, 425–427. [Google Scholar] [CrossRef]
- Spadaccio, C.; Nappi, F.; Al-Attar, N.; Sutherland, F.W.; Acar, C.; Nenna, A.; Trombetta, M.; Chello, M.; Rainer, A. Old Myths, New Concerns: The Long-Term Effects of Ascending Aorta Replacement with Dacron Grafts. Not All That Glitters Is Gold. J. Cardiovasc. Transl. Res. 2016, 9, 334–342. [Google Scholar] [CrossRef]
- Belov, I.V.; Stepanenko, A.B.; Gens, A.P.; Savichev, D.D.; Charchyan, E.R. Reduction aortoplasty for ascending aortic aneurysm: A 14-year experience. Asian Cardiovasc. Thorac. Ann. 2009, 17, 162–166. [Google Scholar] [CrossRef]
- Borger, M.A.; Preston, M.; Ivanov, J.; Fedak, P.W.M.; Davierwala, P.; Armstrong, S.; David, T. Should the ascending aorta be replaced more frequently in patients with bicuspid aortic valve disease? J. Thorac. Cardiovasc. Surg. 2004, 128, 677–683. [Google Scholar] [CrossRef]
- Tadros, T.M.; Klein, M.D.; Shapira, O.M. Ascending aortic dilatation associated with bicuspid aortic valve: Pathophysiology, molecular biology, and clinical implications. Circulation 2009, 119, 880–890. [Google Scholar] [CrossRef]
- Hwang, H.Y.; Shim, M.S.; Park, E.A.; Ahn, H. Reduction aortoplasty for the ascending aortic aneurysm with aortic valve disease. Does bicuspid valve matter? Circ. J. 2011, 7, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, N.A.; Rorris, F.-P. Elective replacement of the ascending aorta: Is the 5.5-cm threshold appropriate? The insidious, small aorta. Eur. J. Cardio-Thorac. Surg. 2021, 59, 554–561. [Google Scholar] [CrossRef]
- Zafar, M.A.; Li, Y.; Rizzo, J.A.; Charilaou, P.; Saeyeldin, A.; Velasquez, C.A.; Mansour, A.M.; Mahmood, S.U.B. Height alone, rather than body surface area, suffices for risk estimation in ascending aortic aneurysm. J. Thorac. Cardiovasc. Surg. 2018, 155, 1938–1950. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zafar, M.A.; Li, Y.; Saeyeldin, A.; Huang, Y.; Zhao, R.; Qiu, J.; Tanweer, M.; Abdelbaky, M.; Gryaznov, A.; et al. Ascending Aortic Length and Risk of Aortic Adverse Events: The Neglected Dimension. J. Am. Coll. Cardiol. 2019, 74, 1883–1894. [Google Scholar] [CrossRef]
- Ostberg, N.P.; Zafar, M.A.; Ziganshin, B.A.; Elefteriades, J.A. The Genetics of Thoracic Aortic Aneurysms and Dissection: A Clinical Perspective. Biomolecules 2020, 10, 182. [Google Scholar] [CrossRef]
- Bayar, N.; Erkal, Z.; Köklü, E.; Güven, R.; Arslan, Ş. Increased Intima-Media Thickness of the Ascending Aorta May Predict Neurological Complications Associated with TAVI. J. Stroke Cerebrovasc. Dis. 2021, 30, 105665. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) |
|---|---|
| Age | 64.4 ± 10.46 |
| Female sex | 42 (30) |
| BMI | 25.3 [22.8, 27.2] |
| BSA | 1.82 [1.69, 1.93] |
| Smoking | 18 (13) |
| Hypertension | 90 (63) |
| Diabetes | 12 (8.5) |
| Chronic renal failure | 10 (7.0) |
| Echocardiographic parameters | |
| Ascending aorta | 46.5 ± 5.11 |
| Ejection fraction | 56 [47, 60] |
| End diastolic diameter | 57 [50, 65] |
| Diagnosis | |
| Aortic stenosis | 43 (30.3) |
| Aortic regurgitation | 71 (50) |
| Mixed aortic disease | 23 (16.2) |
| Coronaropathy | 5 (3.5) |
| Aortic Valve | N (%) |
|---|---|
| Bicuspid | 35 (25) |
| Tricuspid | 83 (58) |
| Prosthesis | 1 (0.7) |
| Unknown | 23 (16.3) |
| Variable | N (%) |
|---|---|
| Arrhythmias | 33 (23) |
| Neurologic events | 1 (0.7) |
| Pericardial effusion | 3 (2.1) |
| Surgical revisions | 3 (2.1) |
| PM implant | 4 (2.8) |
| Acute kidney failure | 6 (4.2) |
| Blood transfusions | 16 (11) |
| Low cardiac output syndrome | 3 (2.1) |
| Respiratory failure | 4 (2.8) |
| Others | 5 (3.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trumello, C.; Giambuzzi, I.; Bargagna, M.; Tavana, K.; Bisogno, A.; Ascione, G.; Calabrese, M.; Castiglioni, A.; Alfieri, O.; De Bonis, M. Long Term Results of Reduction Ascending Aortoplasty. Life 2022, 12, 1526. https://doi.org/10.3390/life12101526
Trumello C, Giambuzzi I, Bargagna M, Tavana K, Bisogno A, Ascione G, Calabrese M, Castiglioni A, Alfieri O, De Bonis M. Long Term Results of Reduction Ascending Aortoplasty. Life. 2022; 12(10):1526. https://doi.org/10.3390/life12101526
Chicago/Turabian StyleTrumello, Cinzia, Ilaria Giambuzzi, Marta Bargagna, Kevin Tavana, Arturo Bisogno, Guido Ascione, Mariachiara Calabrese, Alessandro Castiglioni, Ottavio Alfieri, and Michele De Bonis. 2022. "Long Term Results of Reduction Ascending Aortoplasty" Life 12, no. 10: 1526. https://doi.org/10.3390/life12101526