

Optical Coherence Tomography Reflectivity in Foveal Cysts: A Novel Biomarker for Early-Response Prediction of Diabetic Macular Edema Treated with Dexamethasone

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Participants
2.3. Ophthalmic Examinations
2.4. Statistical Analysis
3. Results
3.1. Comparison of Clinical Characteristics between the Better and Lesser Responder Groups
3.2. Comparison of OCT Parameters between the Better and Lesser Responder Groups
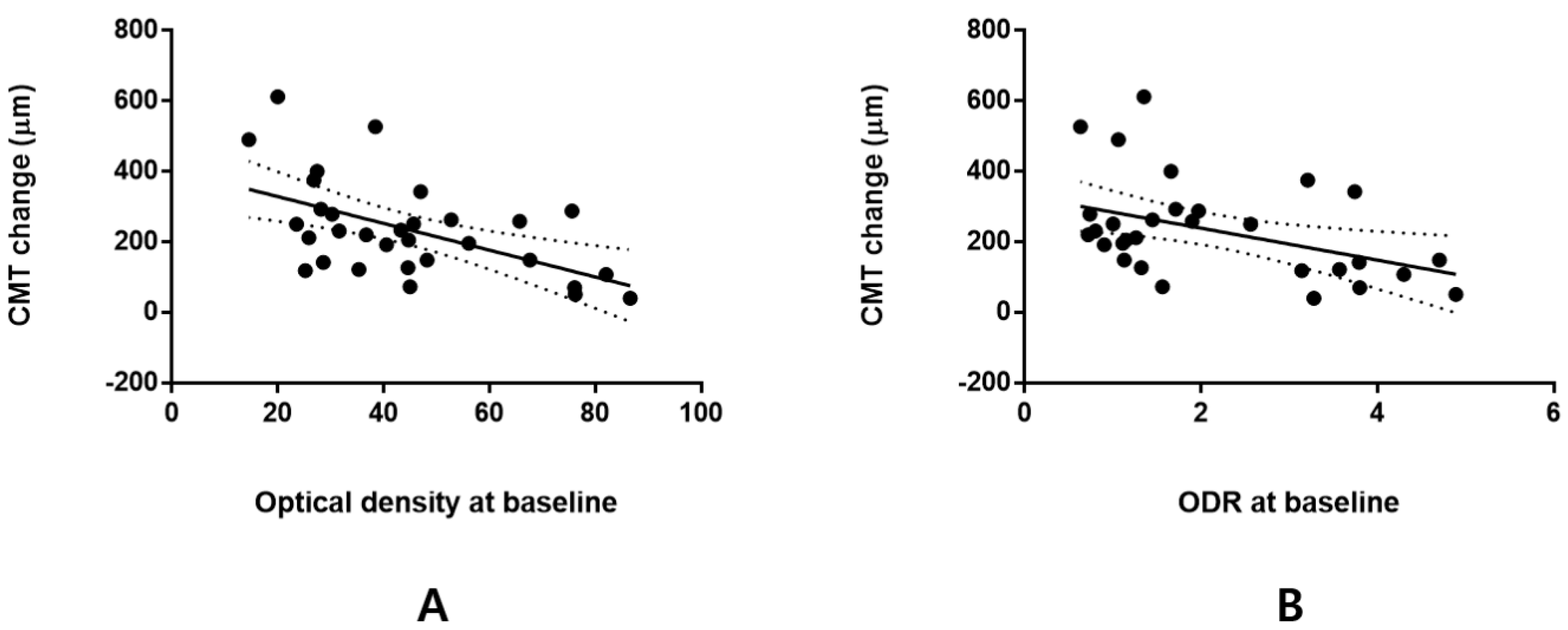
3.3. Correlation between Optical Density in ONL Cysts or Optical Density Ratio and CMT or VA Change
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brown, D.M.; Nguyen, Q.D.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Schlottmann, P.G.; Rundle, A.C.; Zhang, J.; Rubio, R.G.; et al. Long-term outcomes of ranibizumab therapy for diabetic macular edema: The 36-month results from two phase III trials: RISE and RIDE. Ophthalmology 2013, 120, 2013–2022. [Google Scholar] [CrossRef]
- Gonzalez, V.H.; Campbell, J.; Holekamp, N.M.; Kiss, S.; Loewenstein, A.; Augustin, A.J.; Ma, J.; Ho, A.C.; Patel, V.; Whitcup, S.M.; et al. Early and Long-Term Responses to Anti-Vascular Endothelial Growth Factor Therapy in Diabetic Macular Edema: Analysis of Protocol I Data. Am. J. Ophthalmol. 2016, 172, 72–79. [Google Scholar] [CrossRef]
- Bressler, S.B.; Ayala, A.R.; Bressler, N.M.; Melia, M.; Qin, H.; Ferris, F.L., III; Flaxel, C.J.; Friedman, S.M.; Glassman, A.R.; Jampol, L.M.; et al. Persistent Macular Thickening After Ranibizumab Treatment for Diabetic Macular Edema with Vision Impairment. JAMA Ophthalmol. 2016, 134, 278–285. [Google Scholar] [CrossRef]
- Alshahrani, S.T.; Dolz-Marco, R.; Gallego-Pinazo, R.; Diaz-Llopis, M.; Arevalo, J.F.; KKESH International Collaborative Retina Study Group. Intravitreal Dexamethasone Implant for the Treatment of Refractory Macular Edema in Retinal Vascular Diseases: Results of the KKESH International Collaborative Retina Study Group. Retina 2016, 36, 131–136. [Google Scholar] [CrossRef]
- Busch, C.; Fraser-Bell, S.; Iglicki, M.; Lupidi, M.; Couturier, A.; Chaikitmongkol, V.; Giancipoli, E.; Rodriguez-Valdes, P.J.; Gabrielle, P.H.; Lains, I.; et al. Real-world outcomes of non-responding diabetic macular edema treated with continued anti-VEGF therapy versus early switch to dexamethasone implant: 2-year results. Acta Diabetol. 2019, 56, 1341–1350. [Google Scholar] [CrossRef]
- Busch, C.; Zur, D.; Fraser-Bell, S.; Lains, I.; Santos, A.R.; Lupidi, M.; Cagini, C.; Gabrielle, P.H.; Couturier, A.; Mane-Tauty, V.; et al. Shall we stay, or shall we switch? Continued anti-VEGF therapy versus early switch to dexamethasone implant in refractory diabetic macular edema. Acta Diabetol. 2018, 55, 789–796. [Google Scholar] [CrossRef]
- Dutra Medeiros, M.; Postorino, M.; Navarro, R.; Garcia-Arumi, J.; Mateo, C.; Corcostegui, B. Dexamethasone intravitreal implant for treatment of patients with persistent diabetic macular edema. Ophthalmologica 2014, 231, 141–146. [Google Scholar] [CrossRef]
- Iglicki, M.; Busch, C.; Zur, D.; Okada, M.; Mariussi, M.; Chhablani, J.K.; Cebeci, Z.; Fraser-Bell, S.; Chaikitmongkol, V.; Couturier, A.; et al. Dexamethasone Implant for Diabetic Macular Edema in Naive Compared with Refractory Eyes: The International Retina Group Real-Life 24-Month Multicenter Study. The IRGREL-DEX Study. Retina 2019, 39, 44–51. [Google Scholar] [CrossRef]
- Pacella, F.; Romano, M.R.; Turchetti, P.; Tarquini, G.; Carnovale, A.; Mollicone, A.; Mastromatteo, A.; Pacella, E. An eighteen-month follow-up study on the effects of Intravitreal Dexamethasone Implant in diabetic macular edema refractory to anti-VEGF therapy. Int. J. Ophthalmol. 2016, 9, 1427–1432. [Google Scholar] [CrossRef]
- Choi, M.; Kim, S.W. Intravitreal Triamcinolone Injection in Diabetic Macular Edema Refractory to Intravitreal Bevacizumab Injection: Clinical Characteristics According to Response. J. Retina 2020, 5, 12–22. [Google Scholar] [CrossRef]
- Yilmaz, T.; Weaver, C.D.; Gallagher, M.J.; Cordero-Coma, M.; Cervantes-Castaneda, R.A.; Klisovic, D.; Lavaque, A.J.; Larson, R.J. Intravitreal triamcinolone acetonide injection for treatment of refractory diabetic macular edema: A systematic review. Ophthalmology 2009, 116, 902–913. [Google Scholar] [CrossRef]
- Kim, M.W.; Moon, H.; Yang, S.J.; Joe, S.G. Effect of Posterior Subtenon Triamcinolone Acetonide Injection on Diabetic Macular Edema Refractory to Intravitreal Bevacizumab Injection. Korean J. Ophthalmol. 2016, 30, 25–31. [Google Scholar] [CrossRef]
- Zur, D.; Iglicki, M.; Busch, C.; Invernizzi, A.; Mariussi, M.; Loewenstein, A.; International Retina, G. OCT Biomarkers as Functional Outcome Predictors in Diabetic Macular Edema Treated with Dexamethasone Implant. Ophthalmology 2018, 125, 267–275. [Google Scholar] [CrossRef]
- Cicinelli, M.V.; Cavalleri, M.; Querques, L.; Rabiolo, A.; Bandello, F.; Querques, G. Early response to ranibizumab predictive of functional outcome after dexamethasone for unresponsive diabetic macular oedema. Br. J. Ophthalmol. 2017, 101, 1689–1693. [Google Scholar] [CrossRef]
- Hwang, H.S.; Chae, J.B.; Kim, J.Y.; Kim, D.Y. Association Between Hyperreflective Dots on Spectral-Domain Optical Coherence Tomography in Macular Edema and Response to Treatment. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5958–5967. [Google Scholar] [CrossRef]
- Kim, K.T.; Kim, D.Y.; Chae, J.B. Association between Hyperreflective Foci on Spectral-Domain Optical Coherence Tomography and Early Recurrence of Diabetic Macular Edema after Intravitreal Dexamethasone Implantation. J. Ophthalmol. 2019, 2019, 3459164. [Google Scholar] [CrossRef]
- Choi, M.Y.; Jee, D.; Kwon, J.W. Characteristics of diabetic macular edema patients refractory to anti-VEGF treatments and a dexamethasone implant. PLoS ONE 2019, 14, e0222364. [Google Scholar] [CrossRef]
- Zur, D.; Iglicki, M.; Sala-Puigdollers, A.; Chhablani, J.; Lupidi, M.; Fraser-Bell, S.; Mendes, T.S.; Chaikitmongkol, V.; Cebeci, Z.; Dollberg, D.; et al. Disorganization of retinal inner layers as a biomarker in patients with diabetic macular oedema treated with dexamethasone implant. Acta Ophthalmol. 2020, 98, e217–e223. [Google Scholar] [CrossRef]
- Vujosevic, S.; Toma, C.; Villani, E.; Muraca, A.; Torti, E.; Florimbi, G.; Leporati, F.; Brambilla, M.; Nucci, P.; De Cilla, S. Diabetic macular edema with neuroretinal detachment: OCT and OCT-angiography biomarkers of treatment response to anti-VEGF and steroids. Acta Diabetol. 2020, 57, 287–296. [Google Scholar] [CrossRef]
- Lee, H.; Kang, K.E.; Chung, H.; Kim, H.C. Three-dimensional analysis of morphologic changes and visual outcomes in diabetic macular edema. Jpn. J. Ophthalmol. 2019, 63, 234–242. [Google Scholar] [CrossRef]
- Hatz, K.; Ebneter, A.; Tuerksever, C.; Pruente, C.; Zinkernagel, M. Repeated Dexamethasone Intravitreal Implant for the Treatment of Diabetic Macular Oedema Unresponsive to Anti-VEGF Therapy: Outcome and Predictive SD-OCT Features. Ophthalmologica 2018, 239, 205–214. [Google Scholar] [CrossRef]
- Huang, Y.T.; Chang, Y.C.; Meng, P.P.; Lin, C.J.; Lai, C.T.; Hsia, N.Y.; Chen, H.S.; Tien, P.T.; Bair, H.; Lin, J.M.; et al. Optical Coherence Tomography Biomarkers in Predicting Treatment Outcomes of Diabetic Macular Edema after Dexamethasone Implants. Front. Med. 2022, 9, 852022. [Google Scholar] [CrossRef]
- Sun, J.K.; Lin, M.M.; Lammer, J.; Prager, S.; Sarangi, R.; Silva, P.S.; Aiello, L.P. Disorganization of the retinal inner layers as a predictor of visual acuity in eyes with center-involved diabetic macular edema. JAMA Ophthalmol. 2014, 132, 1309–1316. [Google Scholar] [CrossRef]
- Baek, J.; Park, Y.H. Optical density ratio in the subretinal fluid: Differentiating chronic central serous chorioretinopathy and polypodial choroidal vasculopathy. Am. J. Ophthalmol. 2015, 159, 386–392. [Google Scholar] [CrossRef]
- Hartig, S.M. Basic image analysis and manipulation in ImageJ. Curr. Protoc. Mol. Biol. 2013, 102, 14–15. [Google Scholar] [CrossRef] [PubMed]
- Suciu, C.I.; Suciu, V.I.; Nicoara, S.D. Optical Coherence Tomography (Angiography) Biomarkers in the Assessment and Monitoring of Diabetic Macular Edema. J. Diabetes Res. 2020, 2020, 6655021. [Google Scholar] [CrossRef] [PubMed]
- Markan, A.; Agarwal, A.; Arora, A.; Bazgain, K.; Rana, V.; Gupta, V. Novel imaging biomarkers in diabetic retinopathy and diabetic macular edema. Ther. Adv. Ophthalmol. 2020, 12, 2515841420950513. [Google Scholar] [CrossRef]
- Shin, H.J.; Lee, S.H.; Chung, H.; Kim, H.C. Association between photoreceptor integrity and visual outcome in diabetic macular edema. Graefes. Arch. Clin. Exp. Ophthalmol. 2012, 250, 61–70. [Google Scholar] [CrossRef]
- Horii, T.; Murakami, T.; Akagi, T.; Uji, A.; Ueda-Arakawa, N.; Nishijima, K.; Yoshimura, N. Optical coherence tomographic reflectivity of cystoid spaces is related to recurrent diabetic macular edema after triamcinolone. Retina 2015, 35, 264–271. [Google Scholar] [CrossRef]
- Horii, T.; Murakami, T.; Nishijima, K.; Akagi, T.; Uji, A.; Arakawa, N.; Muraoka, Y.; Yoshimura, N. Relationship between fluorescein pooling and optical coherence tomographic reflectivity of cystoid spaces in diabetic macular edema. Ophthalmology 2012, 119, 1047–1055. [Google Scholar] [CrossRef] [Green Version]
- Murakami, T.; Nishijima, K.; Akagi, T.; Uji, A.; Horii, T.; Ueda-Arakawa, N.; Muraoka, Y.; Yoshimura, N. Optical coherence tomographic reflectivity of photoreceptors beneath cystoid spaces in diabetic macular edema. Investig. Ophthalmol. Vis. Sci. 2012, 53, 1506–1511. [Google Scholar] [CrossRef]
- Barthelmes, D.; Sutter, F.K.; Gillies, M.C. Differential optical densities of intraretinal spaces. Investig. Ophthalmol. Vis. Sci. 2008, 49, 3529–3534. [Google Scholar] [CrossRef]
- Barber, A.J.; Lieth, E.; Khin, S.A.; Antonetti, D.A.; Buchanan, A.G.; Gardner, T.W. Neural apoptosis in the retina during experimental and human diabetes. Early onset and effect of insulin. J. Clin. Investig. 1998, 102, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Madjedi, K.; Pereira, A.; Ballios, B.G.; Arjmand, P.; Kertes, P.J.; Brent, M.; Yan, P. Switching between anti-VEGF agents in the management of refractory diabetic macular edema: A systematic review. Surv. Ophthalmol. 2022, 67, 1364–1372. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Age (years) | 58.77 ± 10.32 |
| Sex (M/F) | 13/18 |
| OD/OS | 15/16 |
| Previous bevacizumab treatment | 4.19 ± 2.07 |
| DR stage | |
| Proliferative DR Non-proliferative DR | 23 (74.2%) 8 (25.8%) |
| Lens status | |
| Phakic Pseudophakic | 11 (35.5%) 20 (64.5%) |
| Duration of diabetes mellitus (years) | 9.94 ± 9.00 |
| HbA1c (%) | 7.47 ± 1.31 |
| BUN (mg/dL) | 24.29 ± 16.06 |
| Cr (mg/dL) | 1.45 ± 0.95 |
| BCVA (logMAR) | 0.46 ± 0.32 |
| IOP (mmHg) | 15.42 ± 2.69 |
| CMT (µm) | 544.45 ± 131.55 |
| Characteristics | Better Responder DME (n = 22) | Lesser Responder DME (n = 9) | p-Value |
|---|---|---|---|
| Age (years) | 57.73 ± 11.58 | 61.33 ± 6.06 | 0.219 a |
| Sex (M/F) | 9/13 | 4/5 | 0.583 b |
| Duration of diabetes mellitus (years) | 8.50 ± 7.74 | 13.44 ± 11.26 | 0.254 a |
| HbA1c (%) | 7.66 ± 1.46 | 7.00 ± 0.74 | 0.356 a |
| BUN (mg/dL) | 26.4 ± 18.07 | 19.00 ± 8.37 | 0.569 |
| Cr (mg/dL) | 1.57 ± 1.08 | 1.15 ± 0.43 | 0.622 |
| BCVA (logMAR) | 0.50 ± 0.36 | 0.36 ± 0.17 | 0.453 a |
| IOP (mmHg) | 15.05 ± 2.90 | 16.33 ± 1.94 | 0.236 a |
| CMT (µm) | 577.68 ± 138.95 | 463.22 ± 61.27 | 0.020 a |
| Characteristics | Better Responder DME (n = 22) | Lesser Responder DME (n = 9) | p-Value |
|---|---|---|---|
| CMT (µm) Before injection After injection △CMT (µm) | 577.68 ± 138.95 287.32 ± 80.20 290.36 ± 123.31 | 463.22 ± 61.27 365.22 ± 66.27 98.00 ± 40.37 | 0.004 a 0.016 a <0.001 a |
| DRIL | |||
| Absent Present | 2 (9.1) 20 (90.9) | 0 (0) 9 (100.0) | 1.000 b |
| Intraretinal cysts in the INL | |||
| Absent Present | 1 (4.5) 21 (95.5) | 1 (11.1) 8 (88.9) | 0.503 b |
| Intraretinal cysts in the ONL | |||
| Absent Mild Moderate Severe | 0 (0) 0 (0) 2 (9.1) 20 (90.9) | 0 (0) 1 (11.1) 1 (11.1) 7 (77.8) | 0.273 b |
| Intraretinal cysts in the ONL | |||
| Optical density Optical density ratio | 38.54 ± 15.24 1.55 ± 0.88 | 60.22 ± 21.88 3.46 ± 1.26 | 0.020 a <0.001 a |
| ELM integrity | |||
| Normal Partly disrupted Moderately disrupted Severely disrupted | 5 (22.7) 11 (50.0) 4 (18.2) 2 (9.1) | 3 (33.3) 4 (44.4) 0 (0) 2 (22.2) | 0.422 b |
| EZ integrity | |||
| Normal Partly disrupted Moderately disrupted Severely disrupted | 5 (22.7) 9 (40.9) 4 (18.2) 4 (18.2) | 3 (33.3) 4 (44.4) 0 (0) 2 (22.2) | 0.575 b |
| SRF | |||
| Absent Present | 13 (59.1) 9 (40.9) | 5 (55.6) 4 (44.4) | 1.000 b |
| HRF | |||
| Absent <10 ≥10 | 0 (0) 10 (45.5) 12 (54.5) | 0 (0) 4 (44.4) 5 (55.6) | 1.000 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hwang, D.D.-J. Optical Coherence Tomography Reflectivity in Foveal Cysts: A Novel Biomarker for Early-Response Prediction of Diabetic Macular Edema Treated with Dexamethasone. Life 2022, 12, 1475. https://doi.org/10.3390/life12101475
Hwang DD-J. Optical Coherence Tomography Reflectivity in Foveal Cysts: A Novel Biomarker for Early-Response Prediction of Diabetic Macular Edema Treated with Dexamethasone. Life. 2022; 12(10):1475. https://doi.org/10.3390/life12101475
Chicago/Turabian StyleHwang, Daniel Duck-Jin. 2022. "Optical Coherence Tomography Reflectivity in Foveal Cysts: A Novel Biomarker for Early-Response Prediction of Diabetic Macular Edema Treated with Dexamethasone" Life 12, no. 10: 1475. https://doi.org/10.3390/life12101475