
Unilateral Optic Nerve Sheath Fenestration in Idiopathic Intracranial Hypertension: A 6-Month Follow-Up Study on Visual Outcome and Prognostic Markers

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Non-Surgical Treatment
2.3. Surgical Procedure
2.4. Statistical Analisys
3. Results
3.1. Demographics
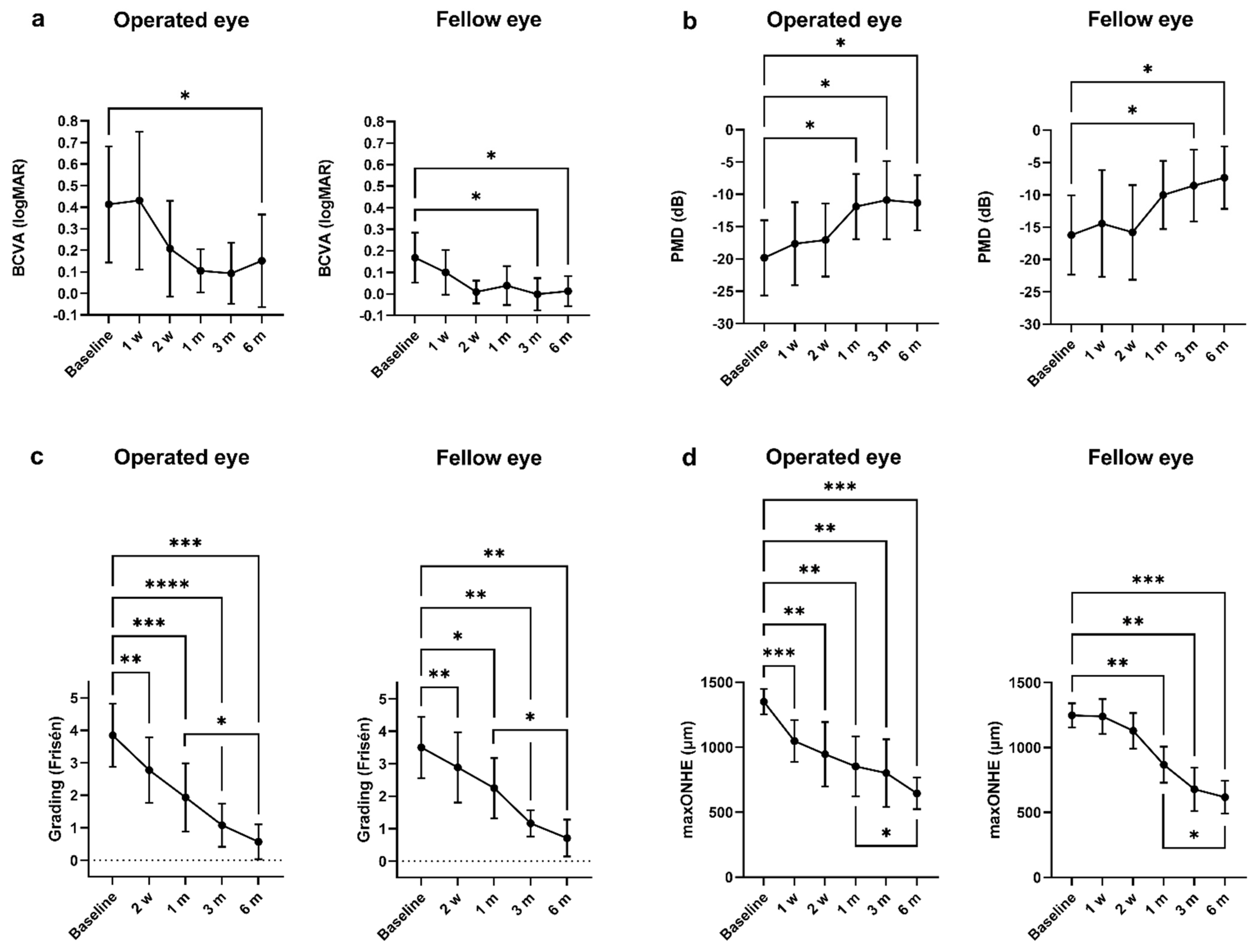
3.2. Visual Acuity
3.3. Visual Fields
3.4. Papilledema Grading and Maximum Optic Nerve Head Elevation (maxONHE)
3.5. Preoperative Prognostic Factors and Short-Term Postoperative Improvements on Long-Term (6 Month) Outcome
4. Discussion
4.1. Visual Function
4.2. Papilledema
4.3. Limitations and Strengths
4.4. Correlations and Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Friedman, D.I.; Liu, G.T.; Digre, K.B. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2013, 81, 1159–1165. [Google Scholar] [CrossRef]
- Mikkilineni, S.; Trobe, J.D.; Cornblath, W.T.; de Lott, L. Visual field mean deviation at diagnosis of idiopathic intracranial hypertension predicts visual outcome. J. Neuro Ophthalmol. 2019, 39, 186–190. [Google Scholar] [CrossRef]
- Keltner, J.L.; Johnson, C.A.; Cello, K.E.; Wall, M. Baseline visual field findings in the idiopathic intracranial hypertension treatment trial (IIHTT). Investig. Ophthalmol. Vis. Sci. 2014, 55, 3200–3207. [Google Scholar] [CrossRef]
- Wall, M.; McDermott, M.P.; Kieburtz, K.D.; Corbett, J.J.; Feldon, S.E.; Friedman, D.I.; Katz, D.M.; Keltner, J.L.; Schron, E.B.; Kupersmith, M.J.; et al. Effect of acetazolamide on visual function in patients with idiopathic intracranial hypertension and mild visual loss: The idiopathic intracranial hypertension treatment trial. JAMA 2014, 311, 1641–1651. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Burdon, M.A.; Nightingale, P.G.; Ball, A.K.; Good, P.; Matthews, T.D.; Jacks, A.; Lawden, M.; Clarke, C.E.; Stewart, P.M.; et al. Low energy diet and intracranial pressure in women with idiopathic intracranial hypertension: Prospective cohort study. BMJ 2010, 341, c2701. [Google Scholar] [CrossRef] [PubMed]
- Mollan, S.P.; Aguiar, M.; Evison, F.; Frew, E.; Sinclair, A.J. The expanding burden of idiopathic intracranial hypertension. Eye 2019, 33, 478–485. [Google Scholar] [CrossRef]
- Hamedani, A.G.; Thibault, D.P.; Revere, K.E.; Lee, J.Y.K.; Grady, M.S.; Willis, A.W.; Liu, G.T. Trends in the surgical treatment of pseudotumor cerebri syndrome in the United States. JAMA Netw. Open 2020, 3, e2029669. [Google Scholar] [CrossRef]
- Azad, T.D.; Zhang, Y.; Varshneya, K.; Veeravagu, A.; Ratliff, J.K.; Li, G. Lumboperitoneal and ventriculoperitoneal shunting for idiopathic intracranial hypertension demonstrate comparable failure and complication rates. Clin. Neurosurg. 2020, 86, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Kalyvas, A.; Neromyliotis, E.; Koutsarnakis, C.; Komaitis, S.; Drosos, E.; Skandalakis, G.P.; Pantazi, M.; Gobin, Y.P.; Stranjalis, G.; Patsalides, A. A systematic review of surgical treatments of idiopathic intracranial hypertension (IIH). Neurosurg. Rev. 2020, 44, 773–792. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, N.S.; Mahmoud, A.M.; Buzzacco, D.; Katz, S.E. Visual outcomes following optic nerve sheath fenestration via the medial transconjunctival approach. Orbit 2016, 35, 271–277. [Google Scholar] [CrossRef]
- Malik, A.I.; Xu, J.; Lee, A.G. Outcomes of optic nerve sheath fenestration from superomedial eyelid crease approach. Orbit 2021, 1–9. [Google Scholar] [CrossRef]
- Sergott, R.C.; Savino, P.J.; Bosley, T.M. Modified optic nerve sheath decompression provides long-term visual improvement for pseudotumor cerebri. Arch. Ophthalmol. 1988, 106, 1384–1390. [Google Scholar] [CrossRef]
- Blessing, N.W.; Tse, D.T. Optic nerve sheath fenestration: A revised lateral approach for nerve access. Orbit 2019, 38, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Sobel, R.K.; Syed, N.A.; Carter, K.D.; Allen, R.C. Optic nerve sheath fenestration: Current preferences in surgical approach and biopsy. Ophthalmic Plast. Reconstr. Surg. 2015, 31, 310–312. [Google Scholar] [CrossRef]
- Alsuhaibani, A.H.; Carter, K.D.; Nerad, J.A.; Lee, A.G. Effect of optic nerve sheath fenestration on papilledema of the operated and the contralateral nonoperated eyes in idiopathic intracranial hypertension. Ophthalmology 2011, 118, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Auinger, P.; Durbin, M.; Feldon, S.; Garvin, M.; Kardon, R.; Keltner, J.; Kupersmith, M.; Sibony, P.; Plumb, K.; Wang, J.K.; et al. Papilledema outcomes from the optical coherence tomography substudy of the idiopathic intracranial hypertension treatment trial. Ophthalmology 2015, 122, 1939–1945. [Google Scholar] [CrossRef]
- Hatem, C.F.; Yri, H.M.; Sørensen, A.L.; Wegener, M.; Jensen, R.H.; Hamann, S. Long-term visual outcome in a Danish population of patients with idiopathic intracranial hypertension. Acta Ophthalmol. 2018, 96, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Frisén, L. Swelling of the optic nerve head: A staging scheme. J. Neurol. Neurosurg. Psychiatry 1982, 45, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.J.; Kardon, R.H.; Lee, A.G.; Frisén, L.; Wall, M. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs. clinical expert assessment using a clinical staging scale. Arch. Ophthalmol. 2010, 128, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.K.; Lao, C.K.; Hildebrand, L.P. FBK. Superonasal Transconjunctival Optic Nerve Sheath Decompression (stONSD). Spencer S. Eccles Health Sciences Library, University of Utah. 2014. Available online: https://collections.lib.utah.edu/details?id=187598 (accessed on 3 April 2021).
- Toft, P.B.; Fugleholm, K. Superonasal Transconjunctival Optic Nerve Sheat Fenestration. 2017. Available online: https://youtu.be/iK82N8hXxT0 (accessed on 3 April 2021).
- Meyer, J.; Karri, R.; Danesh-Meyer, H.; Drummond, K.; Symons, A. A normative database of a-scan data using the Heidelberg spectralis spectral domain optical coherence tomography machine. medRxiv 2020, 1–13. [Google Scholar] [CrossRef]
- Melson, A.T.; Warmath, J.D.; Moreau, A.; Farris, B.K. Superonasal transconjunctival optic nerve sheath decompression: A simplified technique for safe and efficient decompression. J. Neuro Ophthalmol. 2021, 41, e16–e21. [Google Scholar] [CrossRef] [PubMed]
- Keltner, J.L. Optic nerve sheath decompression. How does it work? Has its time come? Arch. Ophthalmol. 1988, 106, 1365–1369. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Shin, D.H.; Spoor, T.C.; Kim, C.; McCarty, B.; Kim, D. Bilateral retinal venous caliber decrease following unilateral optic nerve sheath decompression. Ophthalmic Surg. 1995, 26, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, M.A.; Mehboob, M.A.; Islam, Q.U. Efficacy and safety of optic nerve sheath fenestration in patients with raised intracranial pressure. Pak. J. Med. Sci. 2017, 33, 471–475. [Google Scholar]
- Jefferis, J.M.; Littlewood, R.A.; Pepper, I.M.; Hickman, S.J.; Salvi, S.M. Optic nerve sheath fenestration via a supero-medial eyelid skin crease approach for the treatment of idiopathic intracranial hypertension in a UK population. Eye 2020, 35, 1418–1426. [Google Scholar] [CrossRef]
- Kupersmith, M.J. Baseline OCT measurements in the idiopathic intracranial hypertension treatment trial, part II: Correlations and relationship to clinical features. Investig. Ophthalmol. Vis. Sci. 2014, 55, 8173–8179. [Google Scholar]
- Dreesbach, M.; Joachimsen, L.; Küchlin, S.; Reich, M.; Gross, N.J.; Brandt, A.U.; Schuchardt, F.; Harloff, A.; Böhringer, D.; Lagrèze, W.A. Optic nerve head volumetry by optical coherence tomography in papilledema related to idiopathic intracranial hypertension. Transl. Vis. Sci. Technol. 2020, 9, 24. [Google Scholar] [CrossRef]
- Vijay, V.; Mollan, S.P.; Mitchell, J.L.; Bilton, E.; Alimajstorovic, Z.; Markey, K.A.; Fong, A.; Walker, J.K.; Lyons, H.S.; Yiangou, A.; et al. Using optical coherence tomography as a surrogate of measurements of intracranial pressure in idiopathic intracranial hypertension. JAMA Ophthalmol. 2020, 138, 1264–1271. [Google Scholar] [CrossRef]
- Pineles, S.L.; Volpe, N.J. Long-term results of optic nerve sheath fenestration for idiopathic intracranial hypertension: Earlier intervention favours improved outcomes. Neuro Ophthalmol. 2013, 37, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; Moreau, A.; O’Meilia, R.; Pagteilan, J.; Ding, K.; Siatkowski, R.M.; Farris, B.K. The relationship between optic nerve sheath decompression failure and intracranial pressure in idiopathic intracranial hypertension. J. Neuro Ophthalmol. 2016, 36, 246–251. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients, n | 10 | |||
| Gender, n (%) | Female, 10 (100) | |||
| Range | ||||
| Age, mean | 28.7 ± 11.4 years | [16.4, 46.3] | ||
| Body mass index, mean ± SD | 34.4 ± 4.8 kg/m2 | [29.1, 42.3] | ||
| Opening pressure, mean ± SD | 50.3 ± 12.0 cm CSF | [31, 651] | ||
| Diagnosis to surgery, median | 10 days | [5, 76] | ||
| Operated eye | Range | Fellow eye | Range | |
| ONSD, median | 7 mm | [5, 8] | 7 mm | [5, 7] |
| Baseline | 1 Month | 6 Months | 1 Month–Baseline Diff. | 6 Months–Baseline Diff. | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of Patient, n | 10 | 8 | 8 | |||||||
| Operated Eye | Fellow Eye | Operated Eye | Fellow Eye | Operated Eye | Fellow Eye | Operated Eye | Fellow Eye | Operated Eye | Fellow Eye | |
| BCVA (logMAR) | ||||||||||
| Mean ± SD | 0.41 ± 0.38 | 0.17 ± 0.16 | 0.11 ± 0.12 | 0.04 ± 0.11 | 0.15 ± 0.23 | 0.01 ± 0.06 | −0.31 | −0.13 | −0.26 * | −0.16 * |
| Range [min, max] | [−0.08, 1.30] | [0.00, 0.52] | [−0.08, 0.30] | [−0.08, 0.22] | [−0.08, 0.62] | [−0.08, 0.10] | ||||
| 95% CI diff. | [−0.74, 0.12] | [−0.32, 0.06] | [−0.48, 0.05] | [−0.30, −0.01] | ||||||
| Snellen equivalent | 0.4 | 0.6 | 0.8 | 1.0 | 0.6 | 1.0 | ||||
| PMD (dB) | ||||||||||
| Mean ± SD | −19.8 ± 7.6 | −16.2 ± 8.0 | −11.9 ± 6.0 | −10.0 ± 6.3 | −11.3 ± 4.6 | −7.3 ± 5.2 | 7.9 * | 6.2 | 8.5 * | 8.9 * |
| Range [min, max] | [−27.8, −7.3] | [−25.9, −2.3] | [−19.0, −2.8] | [−18.7, −0.2] | [−18.7, −6.4] | [−16.7, −2.6] | ||||
| 95% CI diff. | [1.4, 14.4] | [1.7, 14.1] | [1.8, 15.2] | [1.3, 16.4] | ||||||
| Papilledema grade | ||||||||||
| Mean ± SD | 3.9 ± 1.0 | 3.5 ± 0.9 | 1.9 ± 1.1 | 2.3 ± 0.9 | 0.6 ± 0.5 | 0.7 ± 0.6 | −1.9 *** | −1.3 * | −3.3 *** | −2.8 ** |
| Range [min, max] | [2, 5] | [2, 5] | [1, 4] | [1, 4] | [0, 1.5] | [0, 1.5] | ||||
| 95% CI diff. | [−2.7, −1.2] | [−2.3, −0.2] | [−4.3, −2.3] | [−4.2, −1.3] | ||||||
| maxONHE (µm) | ||||||||||
| Mean ± SD | 1351 ± 128 | 1248 ± 120 | 853 ± 276 | 868 ± 165 | 646 ± 116 | 618 ± 136 | −498 ** | −380 ** | −705 *** | −630 *** |
| Range [min, max] | [1130, 1565] | [980, 1353] | [538, 1315] | [598, 1133] | [496, 809] | [451, 841] | ||||
| 95% CI diff. | [−775, −222] | [−635, −126] | [−927, −484] | [−889, −371] | ||||||
| Macular GCLvol (mm3) | ||||||||||
| Mean ± SD | 1.07 | 1.09 | 0.95 | 1.09 | 0.9 | 1.08 | −0.09 *† | −0.08 **† | −0.23 *† | −0.13 † |
| Range [min, max] | [0.46, 1.25] | [0.73, 1.36] | [0.46, 1.10] | [0.69, 1.26] | [0.79, 1.00] | [0.82, 1.14] | ||||
| 95% CI diff. | [−0.17, 0.00] | [−0.11, −0.01] | [−0.34, −0.06] | [−0.27, 0.00] | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hagen, S.M.; Wegener, M.; Toft, P.B.; Fugleholm, K.; Jensen, R.H.; Hamann, S. Unilateral Optic Nerve Sheath Fenestration in Idiopathic Intracranial Hypertension: A 6-Month Follow-Up Study on Visual Outcome and Prognostic Markers. Life 2021, 11, 778. https://doi.org/10.3390/life11080778
Hagen SM, Wegener M, Toft PB, Fugleholm K, Jensen RH, Hamann S. Unilateral Optic Nerve Sheath Fenestration in Idiopathic Intracranial Hypertension: A 6-Month Follow-Up Study on Visual Outcome and Prognostic Markers. Life. 2021; 11(8):778. https://doi.org/10.3390/life11080778
Chicago/Turabian StyleHagen, Snorre Malm, Marianne Wegener, Peter Bjerre Toft, Kåre Fugleholm, Rigmor Højland Jensen, and Steffen Hamann. 2021. "Unilateral Optic Nerve Sheath Fenestration in Idiopathic Intracranial Hypertension: A 6-Month Follow-Up Study on Visual Outcome and Prognostic Markers" Life 11, no. 8: 778. https://doi.org/10.3390/life11080778