
Patient Reported Outcome Measure in Atopic Dermatitis Patients Treated with Dupilumab: 52-Weeks Results

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Outcome Variables
2.3. Statistical Analysis
3. Results
3.1. Evolution of Visits: Baseline, 16, 40 and 52 Weeks
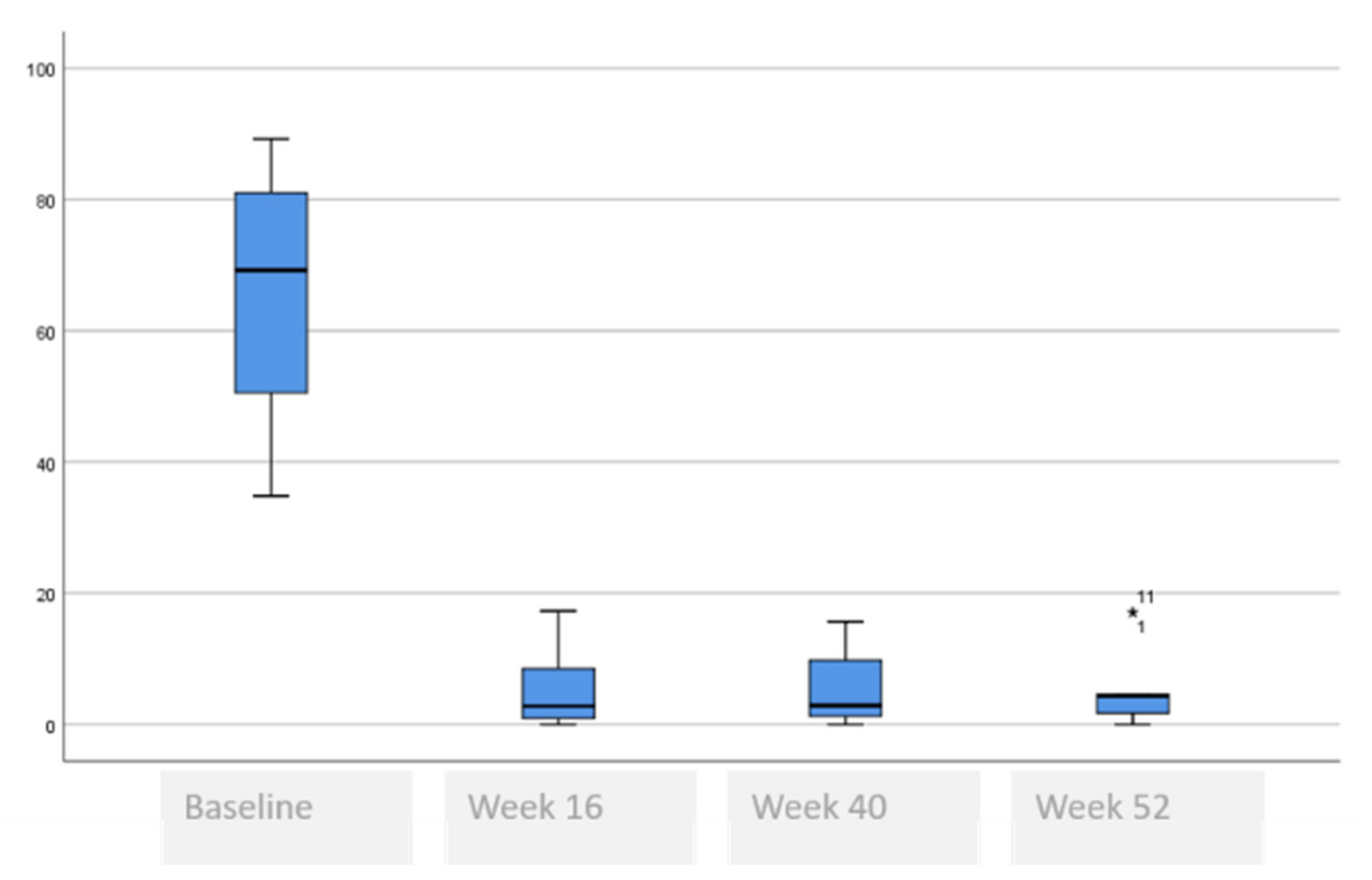
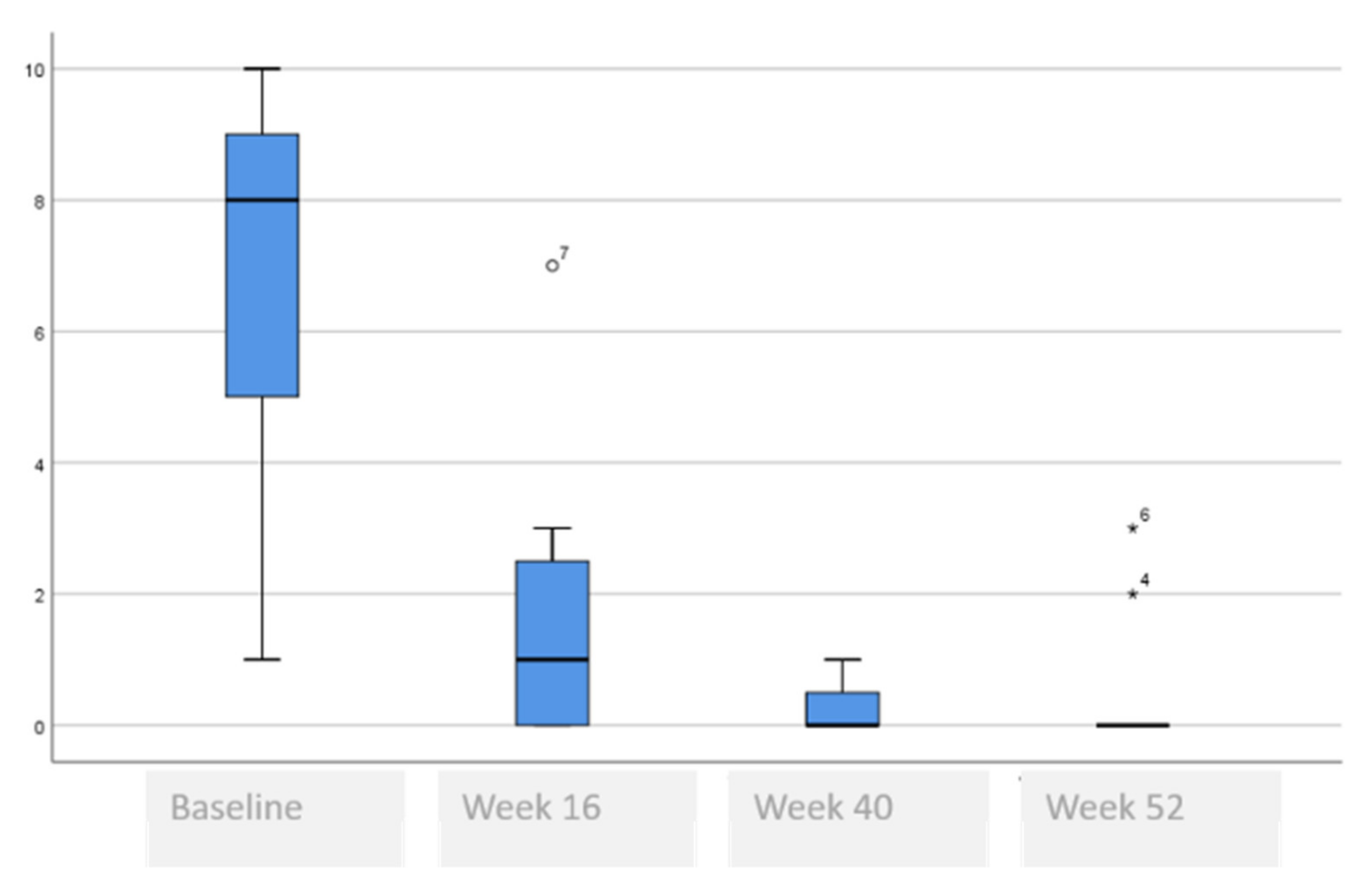
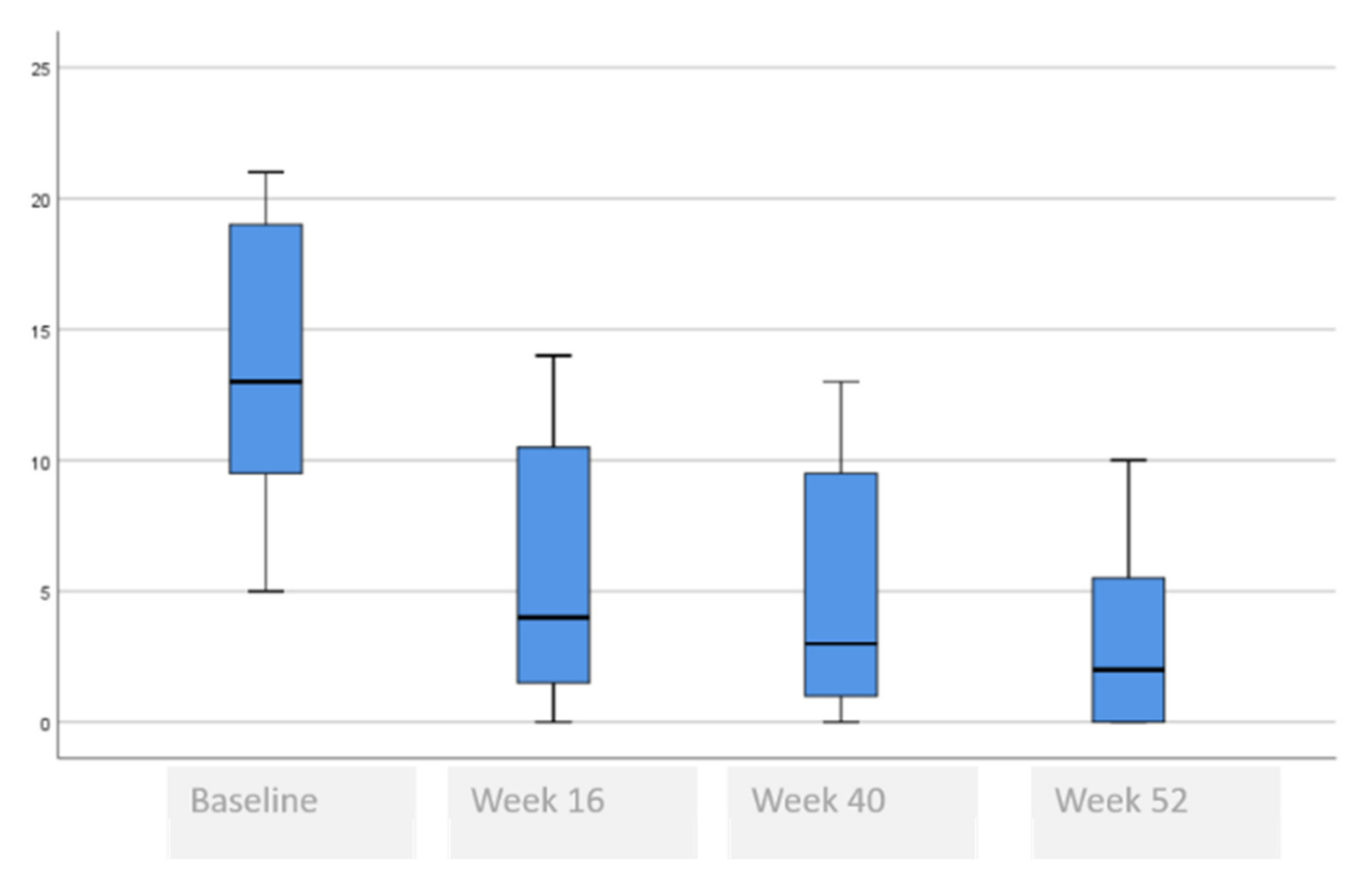
3.2. Comparative of Symptoms Analysis at Baseline, 16, 40 and 52 Weeks
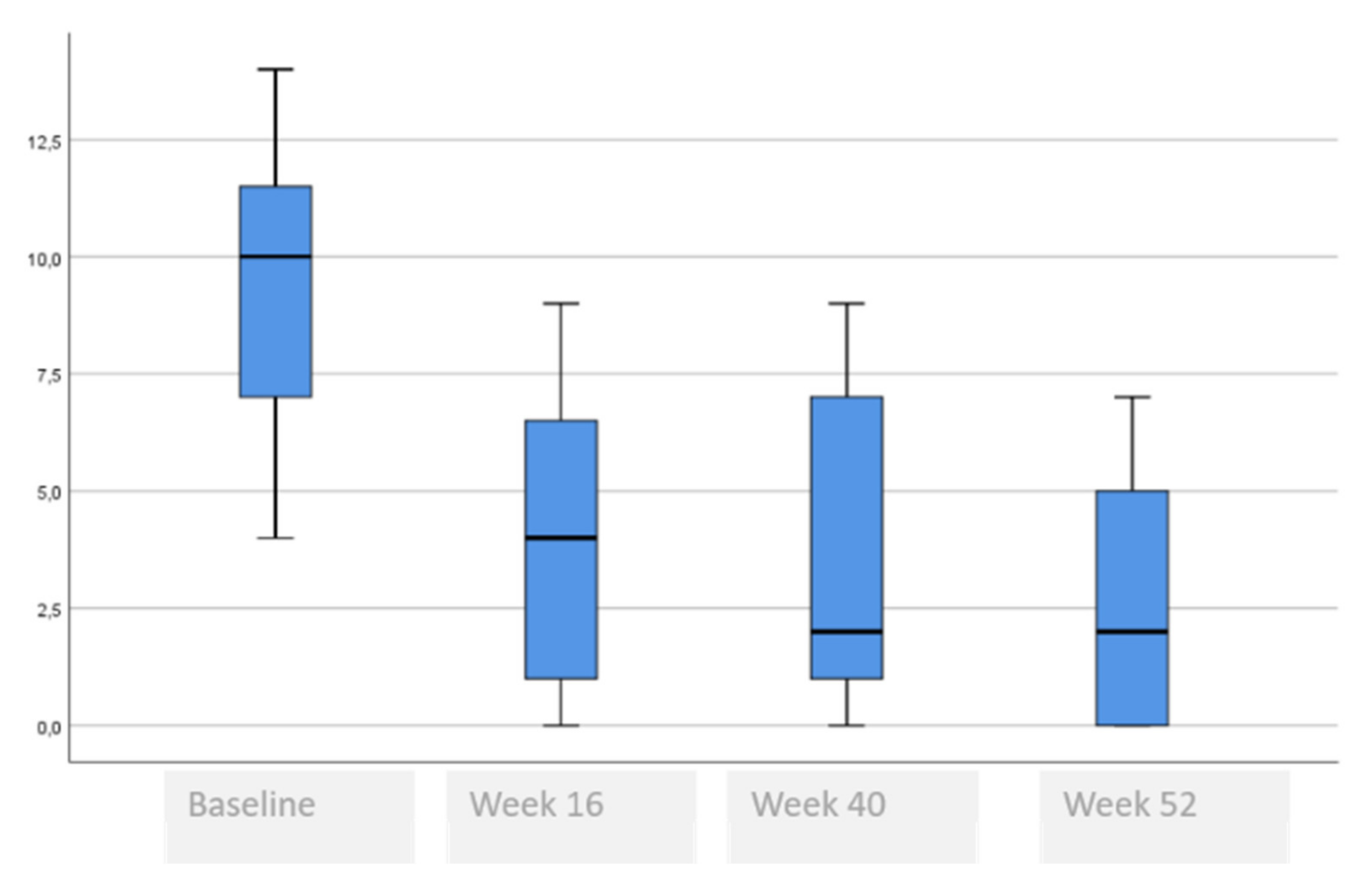
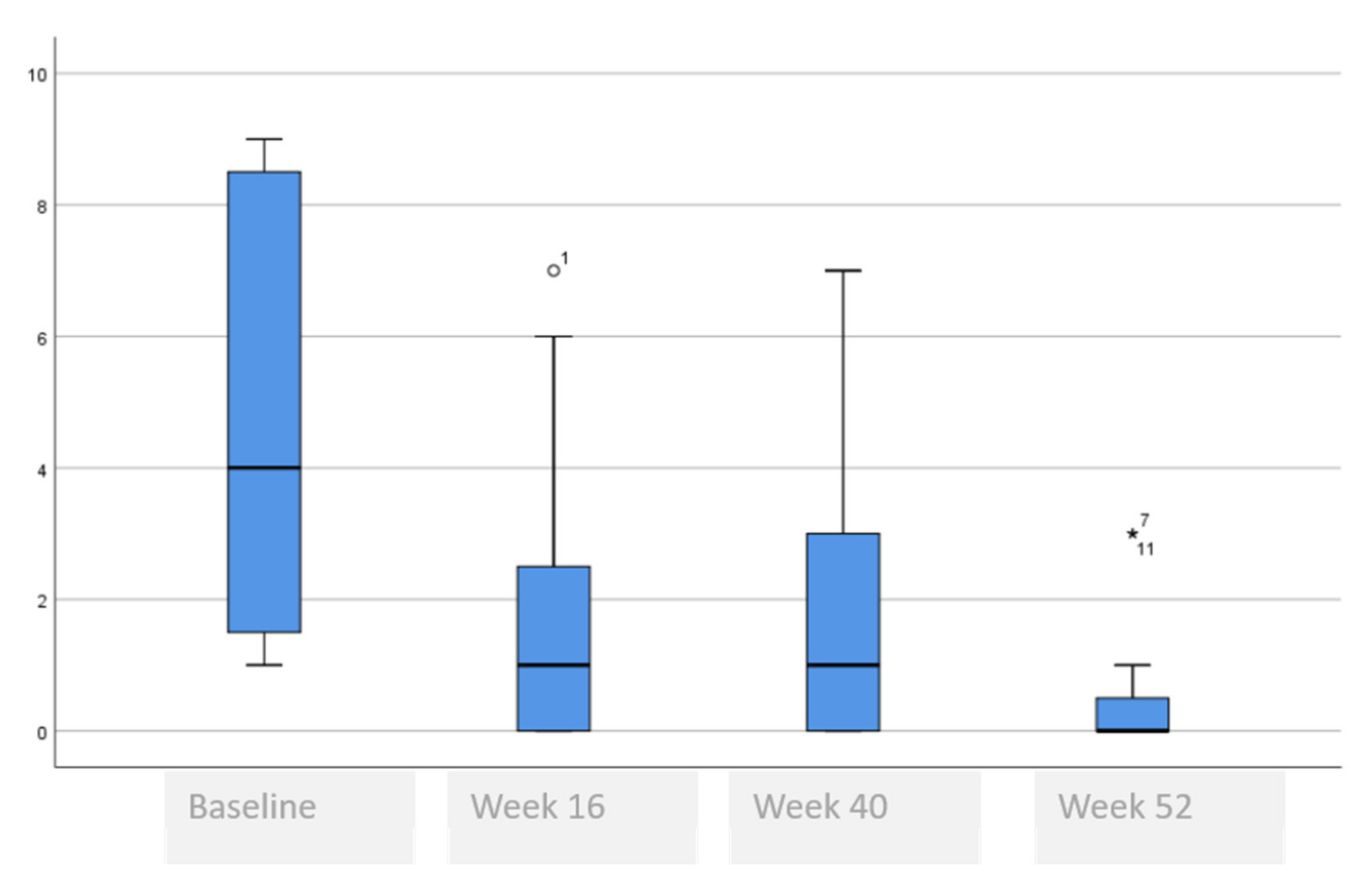
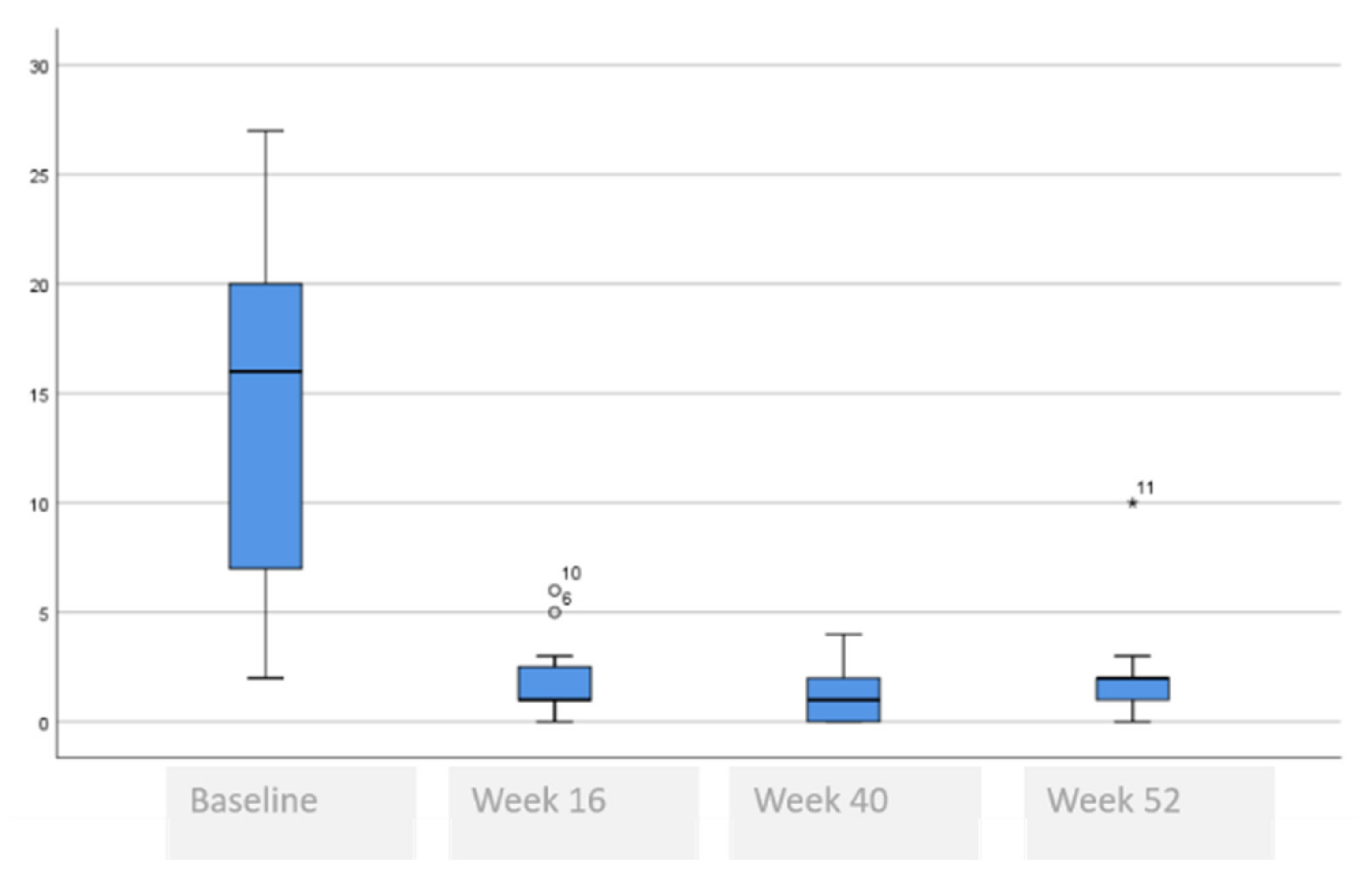
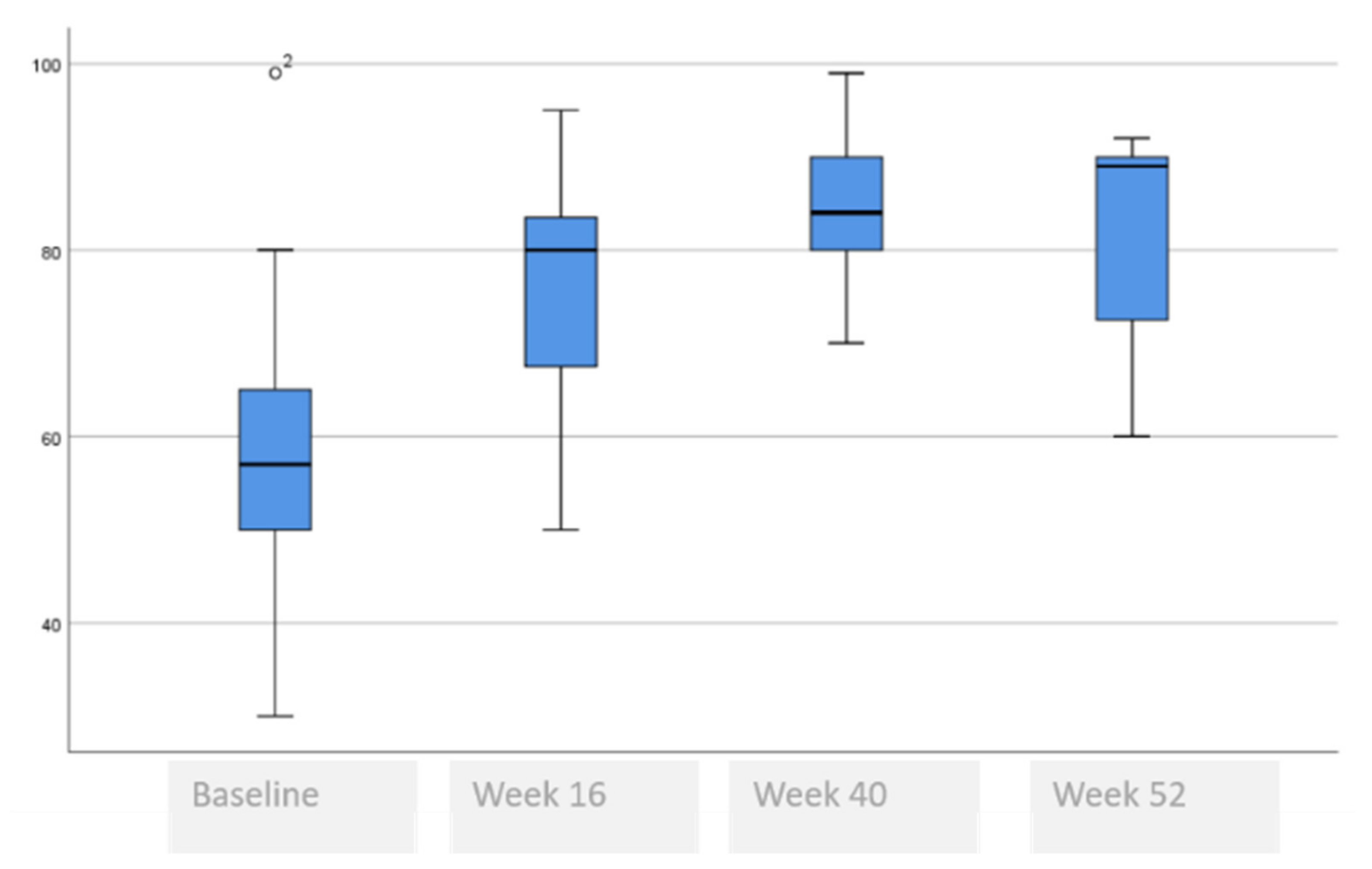
3.3. Comparative Self-Perceived Psychological and Quality of Life Issues Analysis at Baseline, 16, 40 and 52 Weeks
3.4. Comparative Satisfaction Analysis at Baseline, 16, 40 and 52 Weeks
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McHenry, P.M.; Williams, H.C.; Bingham, E.A. Management of atopic eczema. Joint workshop of the British Association of Dermatologists and the Research Unit of the Royal College of Physicians of London. BMJ 1995, 310, 843–847. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Hanifin, J.M. Adult eczema prevalence and associations with asthma and other health and demographic factor: A US population-based study. J. Allergy Clin. Inmunol. 2013, 132, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Zonnerveld, I.M.; De Rie, M.A.; Beljaards, R.C.; Van Der Rhee, H.J.; Wuite, J.; Zeegelaar, J.; Bos, J.D. The-long term safety and efficacy of cyclosporin in severe refractory atopic dermatitis: A comparison of two dosage regimens. Br. J. Dermatol. 1996, 135, 15–20. [Google Scholar] [CrossRef]
- Van de Schaft, J.; Politiek, K.; van der Reek, J.M.; Christoffers, W.A.; Kievit, W.; de Jong, E.M.G.J.; Brujinzeel-Koonmen, C.A.F.M.; Schuttelaar, M.L.A.; de Bruin-Weller, M.S. Drug survival for cyclosporin A in a long-term daily practice cohort of adult patients with atopic dermatitis. Br. J. Dermatol. 2015, 172, 1621–1627. [Google Scholar] [CrossRef] [PubMed]
- Granlund, H.; Erkko, P.; Remitz, A.; Langeland, T.; Helsing, P.; Nuutinen, M.; Reitamo, S. Comparison of cyclosporin and UVAB phototherapy for intermittent one-year treatment of atopic dermatitis. Acta Derm. Venereol. 2001, 81, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Politiek, K.; van der Schaft, J.; Coenraads, P.J.; de Bruin-Weller, M.S.; Schuttelaar, M.L.A. Drug survival for methotrexate in a daily practice cohort of adult patients with severe atopic dermatitis. Br. J. Dermatol. 2016, 174, 201–203. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Tom, W.L.; Berger, T.G.; Krol, A.; Paller, A.S.; Schwarzemberger, K.; Bergman, J.N.; Chamlis, S.L.; Cohen, D.E.; Cooper, K.D.; et al. Guidelines of care for the management of atopic dermatitis: Section 2. Management and treatment of atopic dermatitis with topical therapies. J. Am. Acad. Dermatol. 2014, 71, 116–132. [Google Scholar] [CrossRef] [Green Version]
- Katayama, I.; Aihara, M.; Ohya, Y.; Saeki, H.; Shimojo, N.; Shoji, S.; Taniguchi, M.; Yamada, M. Japanese guidelines for atopic dermatitis 2017. Allergol. Int. 2017, 66, 230–247. [Google Scholar] [CrossRef]
- Sidbury, R.; Davis, D.M.; Cohen, D.E.; Cordoro, K.M.; Beerger, T.G.; Bergman, J.N.; Chamlin, S.L.; Cooper, K.D.; Feldman, S.R.; Hanifin, J.M.; et al. Guidelines of care for the management of atopic dermatitis: Section 3. Management and treatment with phototherapy and systemic agents. J. Am. Acad. Dermatol. 2014, 71, 327–349. [Google Scholar] [CrossRef] [Green Version]
- Garritsen, F.M.; Brouwer, M.W.D.; Limpens, J.; Spuls, P.I. Photo(chemo)therapy in the management of atopic dermatitis: An updated systemic review with implications for practice and research. Br. J. Dermatol. 2014, 170, 501–513. [Google Scholar] [CrossRef]
- Ring, J.; Alomar, A.; Bieber, T.; Deleuran, M.; Fink-Wagner, A.; Gelmetti, C.; Gieler, U.; Lipozencic, J.; Luger, T.; Oranje, A.P.; et al. Guidelines for treatment of atopic eczema (atopic dermatitis) part II. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 1176–1193. [Google Scholar] [CrossRef] [PubMed]
- Sidbury, R.; Tom, W.L.; Bergman, J.N.; Cooper, K.D.; Silverman, R.A.; Berger, T.G.; Chamlin, S.L.; Cohen, D.E.; Cordoro, K.M.; Davis, D.M.; et al. Guidelines of care for the management of atopic dermatitis: Section 4. Prevention of disease flares and use of adjuntive therapies and approaches. J. An. Acad. Dermatol. 2014, 71, 1218–1233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandhi, N.A.; Bennett, B.L.; Graham, N.M.H.; Pirozzi, G.; Sthal, N.; Yancopoulos, G.D. Targeting key proximal drivers in type 2 inflammation in disease. Nat. Rev. Drug. Discov. 2016, 15, 35–50. [Google Scholar] [CrossRef]
- Thaci, D.; Simpson, E.L.; Beck, L.A.; Bieber, T.; Blauvelt, A.; Papp, K.; Soong, W.; Worm, M.; Szepietovski, J.C.; Sofen, H.; et al. Efficacy and safety of dupilumab in adults with moderate-to-severe atopic dermatitis inadequately controlled by topical treatments: A randomized, placebo-controlled, dosage-ranging phase 2b trial. Lancet 2016, 387, 40–52. [Google Scholar] [CrossRef]
- Simpson, E.L.; Gadkari, A.; Worm, M.; Soong, W.; Blauvelt, L.E.; Wu, R.; Ardeleanu, M.; Graham, N.M.H.; Pirozi, G.; Sutherland, E.R.; et al. Dupilumab therapy provides clinically meaningful improvement in patients-reported outcomes (PROs): A phase IIb, randomizes, placebo-controlled, clinical trial in adult patients with moderate to severe atopic dermatitis (AD). J. Am. Acad. Dermatol. 2016, 75, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Simpsom, E.L.; Bieber, T.; Guttman-Yassky, E.; Beck, L.A.; Blauvelt, A.; Cork, M.J.; Silverberg, J.I.; Deleuran, M.; Kataoka, Y.; Lacour, J.P.; et al. SOLO 1 and SOLO 2 investigators. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N. Engl. J. Med. 2016, 375, 2335–2348. [Google Scholar] [CrossRef] [PubMed]
- European Medical Agency (EMA) Anexo I Ficha Técnica o Resumen de Las Características de Dupixent. 2018. Available online: https://www.ema.europa.eu/en/documents/product-information/dupixent-epar-product-information_es.pdf (accessed on 3 March 2021).
- Barrett, A.; Hahn-Pedersen, J.; Kragh, N.; Evans, E.; Ganasakthy, A. Patient-Reported Outcome Measures in Atopic Dermatitis and Chronic Hand Eczema in Adults. Patient 2019, 12, 445–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marron, S.E.; Tomas-Aragones, L.; Moncin-Torres, C.A.; Gomez-Barrera, M.; Alcalde-Herrero, V.M.; Garcia-Latasa de Aranibar, F.J. Adult patients with atopic dermatitis treated with Dupilumab in routine clinical practice: Preliminary data at week-16. Neuropsychiatry 2019, 9, 749–755. [Google Scholar]
- Severity Scoring of Atopic Dermatitis: The SCORAD index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology 1993, 186, 23–31. [CrossRef] [PubMed]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A Validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Seguna, A. The Spanish version of EuroQol: A description and its applications. European Quality of Life Scale. Med. Clin. 1999, 112, 79–85. [Google Scholar]
- Badia, X.; Mascaro, J.M.; Lozano, R. Measuring health-related quality of life in patients with mild to moderate eczema and psoriasis: Clinical validity, reliability and sensitivity to change of the DLQI: The Cavide Research Group. Br. J. Dermatol. 1999, 141, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, F.M.; Bago, J.; Royuela, A.; Seco, J.; Gimenez, S.; Muriel, A.; Abraira, V.; Martin, J.L.; Peña, J.L.; Gestoso, M.; et al. Psychometrics characteristics of the Spanish version of instruments to measure neck pain disability. BMC. Musculoeskeletal Disord. 2008, 9, 42–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feixas, G.; Pucurull, O.; Roca, C.; Paz, C.; Garcia-Grau, E.; Bados, A. Escala de satisfacción con el tratamiento recibido (CRES-4): Versión en español. Revista Psicoterapia 2012, 23, 51–58. [Google Scholar] [CrossRef]
- de Bruin-Weller, M.; ThaçI, D.; Smith, C.H.; Reich, K.; Cork, M.J.; Radin, A.; Zhang, Q.; Akinlade, B.; Gadkari, A.; Eckert, L.; et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: A placebo-controlled, randomized phase III clinical trial (LIBERTY AD CAFÉ). Br. J. Dermatol. 2018, 178, 1083–1101. [Google Scholar]
- Blauvelt, A.; de Bruin-Weller, M.; Gooderham, M.; Cather, J.C.; Weisman, J.; Pariser, D.; Simpson, E.L.; Papp, K.A.; Hong, H.C.; Rubel, D.; et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): A 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet 2017, 389, 2287–2303. [Google Scholar] [CrossRef]
- Tofte, S.J.; Papp, K.; Sadick, N.; Bohnert, K.; Simson, E.; Thaci, D.; Bieber, T.; Blaubelt, A.; Sofem, H.; Gooderham, M.; et al. Efficacy and safety of dupilumab for the treatment of moderate-to-severe atopic dermatitis in adults: A pooled analysis of two phase 2 clinical trials. J. Am. Asoc. Nurse Pract. 2018, 30, 529–541. [Google Scholar] [CrossRef]
- Faiz, S.; Giovanelli, J.; Podevin, C.; Jachiet, M.; Bouaziz, J.D.; Reguiai, Z.; Nosbaum, A.; Lasek, A.; Ferrier le Bouedec, M.C.; Du Thanh, A.; et al. Effectiveness and safety of dupilumab for the treatment of atopic dermatitis in a real-life French multicenter adult cohort. J. Am. Acad. Dermatol. 2019, 81, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Barbarot, S.; Wollenberg, A.; Silverberg, J.I.; Deleuran, M.; Pellacani, G.; Armario-Hita, J.C.; Chen, Z.; Schumel, B.; Eckert, L.; Gadkari, A.; et al. Dupilumab provide rapid and sustained improvement in SCORAD outcome in adults with moderate-to-severe atopic dermatitis: Combined results of four randomized phase 3 trial. Dermatolog. Treat. 2020, 8, 1–12. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Baseline | Week 16 | Week 40 | Week 52 |
|---|---|---|---|---|
| Severity, n (%) | ||||
| Without lesions | 0 (0.0) | 3 (27.3) | 2 (18.2) | 4 (36.4) |
| Almost no lesions | 0 (0.0 | 2 (18.2) | 8 (72.7) | 6 (54.5) |
| Mild | 0 (0.0) | 4 (36.4) | 1 (9.1) | 1 (9.1) |
| Moderate | 0 (0.0) | 2 (18.2) | 0 (0.0) | 0 (0.0) |
| Severe | 11(100) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Weight, mean (SD) | 74.7 (14.2) | 74.0 (15.3) | 75.4 (13.6) | 75.0 (15.8) |
| BMI, mean (SD) | 27.0 (4.4) | 26.8 (4.9) | 27.2 (4.2) | 27.1 (5.0) |
| SCORAD, mean (SD) | 64.5 (19.6) | 5.5 (5.9) | 5.8 (5.7) | 5.3 (6.0) |
| Itching; Yes, n (%) | 11 (100) | 8 (72.7) | 7 (63.6) | 9 (81.8) |
| VAS pruritus, median (range) | 8 (6–10) | 1 (0–6) | 1 (0–4) | 1 (0–6) |
| Pruritus, characteristics; Yes, n (%) | ||||
| Itching only | 4 (36.4) | 9 (81.8) | 9 (81.8) | 9 (81.8) |
| Burning | 8 (72.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Stinging | 8 (72.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Pain | 7 (63.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Pruritus, frequency; Yes, n (%) | ||||
| Never | 0 (0.0) | 2 (18.2) | 1 (9.1) | 2 (18.2) |
| Rarely | 0 (0.0) | 3 (27.3) | 6 (54.5) | 6 (54.5) |
| Sometimes | 1 (9.1) | 4 (36.4) | 4 (36.4) | 2 (18.2) |
| Often | 5 (45.5) | 2 (18.2) | 0 (0.0) | 1 (9.1) |
| Always | 5 (45.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Unbearable itching, n (%) | ||||
| Never | 0 (0.0) | 6 (54.5) | 7 (63.6) | 7 (63.6) |
| Rarely | 0 (0.0) | 3 (27.3) | 1 (9.1) | 3 (27.3) |
| Sometimes | 3 (27.3) | 2 (18.2) | 2 (18.2) | 1 (9.1) |
| Often | 3 (27.3) | 0 (0.0) | 1 (9.1) | 0 (0.0) |
| Always | 5 (45.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Impact of pruritus on others, n (%) | ||||
| Never | 2 (18.2) | 9 (81.8) | 7 (63.6) | 8 (72.7) |
| Rarely | 0 (0.0) | 2 (18.2) | 2 (18.2) | 2 (18.2) |
| Sometimes | 1 (9.1) | 0 (0.0) | 2 (18.2) | 1 (9.1) |
| Often | 5 (45.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Always | 3 (27.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Impact of pruritus on sleep, n (%) | ||||
| Never | 0 (0.0) | 7 (63.6) | 8 (72.7) | 7 (63.6) |
| Rarely | 1 (9.1) | 4 (36.4) | 1 (9.1) | 3 (27.3) |
| Sometimes | 1 (9.1) | 0 (0.0) | 2 (18.2) | 1 (9.1) |
| Often | 5 (45.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Always | 4 (36.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Impact of pruritus on mood, n (%) | ||||
| Never | 0 (0.0) | 8 (72.7) | 7 (63.6) | 9 (81.8) |
| Rarely | 2 (18.2) | 3 (27.3) | 2 (18.2) | 1 (9.1) |
| Sometimes | 1 (9.1) | 0 (0.0) | 2 (18.2) | 1 (9.1) |
| Often | 6 (54.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Always | 2 (18.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Difficulty sleeping; Yes, n (%) | 11 (100) | 6 (54.5) | 1 (9.1) | 2 (18.2) |
| VAS difficulty sleeping, median (range) | 8 (1–10) | 1 (0–7) | 0 (0–1) | 0 (0–3) |
| Variable | Baseline | Week 16 | Week 40 | Week 52 |
|---|---|---|---|---|
| EQ-5D-3L mobility problems, n (%) | ||||
| None | 11 (100) | 11 (100) | 11 (100) | 11 (100) |
| Some | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Many | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| EQ-5D-3L personal care problems, n (%) | ||||
| None | 9 (81.8) | 11 (100) | 11 (100) | 11 (100) |
| Some | 2 (18.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Many | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| EQ-5D-3L problems in daily activities, n (%) | ||||
| None | 6 (54.5) | 11 (100) | 100 (0.0) | 11 (100) |
| Some | 5 (45.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Many | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| EQ-5D-3L discomfort, pain problems, n (%) | ||||
| None | 3 (27.3) | 10 (90.1) | 10 (90.9) | 11 (100) |
| Some | 8 (72.7) | 1 (9.1) | 1 (9.1) | 0 (0.0) |
| Many | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| EQ-5D-3L anxiety/depression problems, n (%) | ||||
| None | 3 (27.3) | 9 (81.8) | 9 (81.8) | 11 (100) |
| Some | 6 (54.5) | 1 (9.1) | 2 (18.2) | 0 (0.0) |
| Many | 2 (18.2) | 1 (9,1) | 0 (0.0) | 0 (0.0) |
| EQ-5D-3L VAS, mean (range) | 57 (99–30) | 80 (95–50) | 84 (99–70) | 89 (92–60) |
| Variable | Baseline | Week 16 | Week 40 | Week 52 |
|---|---|---|---|---|
| SBP, mmHg, mean (SD) | 127.3 (16.4) | 121.8 (14.2) | 121.2 (9.7) | 128.0 (11.1) |
| DBP, mmHg, mean (SD) | 82.1 (12.4) | 78.7 (12.6) | 80.0 (10.6) | 83.1 (8.4) |
| Pulse, BPM, mean (SD) | 79.0 (17.9) | 72.7 (12.6) | 76.2 (10.6) | 83.7 (7.7) |
| Temperature, mean °C (SD) | 36.1 (10.3) | 36.0 (0.3) | 36.2 (0.3) | 36.1 (0.3) |
| Local reaction; Yes, n (%) | 2 (18.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Severity, n (%) | ||||
| Mild | 2 (18.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Moderate | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Severe | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| General reaction; Yes, n (%) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Analytical alteration; Yes, n (%) | 0 (0.0) | 1 (9.1) | 0 (0.0) | 0 (0.0) |
| Variable | Week-16 | Dupilumab Week-40 | Week-52 | Previous |
|---|---|---|---|---|
| Satisfaction with training received to administer treatment, median (range) | 9 (6–10) | 9 (6–10) | 9 (6–10) | 6 (0–10) |
| Satisfaction with information from dermatologist, median (range) | 9 (6–10) | 9 (6–10) | 9 (6–10) | 6 (0–9) |
| Satisfaction with disease control, median (range) | 9 (6–10) | 9 (6–10) | 9 (6–10) | 3 (0–8) |
| Satisfaction with frequency of administration, median (range) | 9 (6–10) | 9 (6–10) | 9 (6–10) | 2 (0–9) |
| Effectiveness of treatment to prolong time between flares, median (range) | 9 (6–10) | 9 (6–10) | 9 (6–10) | 2 (0–9) |
| Effectiveness of treatment in control of flares, median (range) | 9 (6–10) | 9 (6–10) | 9 (6–10) | 2 (0–8) |
| Overall satisfaction, median (range) | 9 (8–10) | 9 (8–10) | 9 (8–10) | 4 (0–10) |
| Variable | Baseline | Week 16 | Week 40 | Week 52 | p Value |
|---|---|---|---|---|---|
| Weight, mean (SD) | 74.7 (14.2) | 74.0 (15.3) | 75.4 (13.6) | 75.0 (15.8) | 0.993 £ |
| BMI, mean (SD) | 27.0 (4.4) | 26.8 (4.9) | 27.2 (4.2) | 27.1 (5.0) | 0.994 £ |
| SCORAD, mean (SD) | 64.5 (19.6) | 5.5 (5.9) | 5.8 (5.7) | 5.3 (6.0) | <0.001 £ * <0.001 Ω (baseline vs. rest) * |
| VAS pruritus, median (range) | 8 (6–10) | 1 (0–6) | 1 (0–4) | 1 (0–6) | <0.001 ¥ * 0.003 § (baseline vs. rest) * 0.259 § (week 40 vs. week 52) |
| VAS difficulty sleeping, median (range) | 8 (1–10) | 1 (0–7) | 0 (0–1) | 0 (0–3) | <0.001 ¥ * 0.006 § (baseline vs. rest) * 0.036 § (week 16 vs. rest) |
| Variable | Baseline | Week 16 | Week 40 | Week 52 | p Value |
|---|---|---|---|---|---|
| HADS anxiety, mean (SD) | 9.2 (3.0) | 3.9 (3.4) | 3.4 (3.5) | 2.6 (2.8) | <0.001 £ * <0.007 Ω (baseline vs. Week 16) * <0.224 Ω (baseline vs. Week 52) |
| HADS depression, mean (SD) | 4.7 (3.4) | 1.9 (2.5) | 2.0 (2.3) | 0.6 (1.0) | 0.001 £ * <0.008 Ω. (baseline vs. Week 16) * <0.127 Ω. (baseline vs. Week 52) |
| HADS Total, mean (SD) | 13.9 (5.5) | 5.8 (5.0) | 5.4 (5.0) | 3.2 (3.9) | 0.001 £ * <0.004 Ω (baseline vs. week 16) * <0.138 Ω (baseline vs. week 52) |
| DLQI, mean (SD) | 13.9 (8.3) | 2.0 (1.8) | 1.3 (1.4) | 2.1 (2.7) | <0.001 £ * 0.001 Ω (baseline vs. week 52) * 0.931 Ω (week 16 vs. week 52) |
| VAS EQ-5D-3L, median (range) | 57 (30–99) | 80 (50–95) | 84 (70–99) | 89 (60–92) | <0.001 £ * 0.035 Ω (baseline vs. week 16) 0.225 Ω (week 16 vs. week 52) |
| Variable | Previous | Current at Week 16 | p Value (Previous vs. Current at Week 16) | Current at Week 40 | p Value (Current vs. Previous at Week 16 and 40) | Current at Week 52 | p Value (Previous vs. Current at Week 40 and 52) |
|---|---|---|---|---|---|---|---|
| Satisfaction with training received to administer treatment, median (range) | 6 (0–10) | 9 (6–10) | 0.019 § | 9 (8–10) | 0.296 § | 9 (8–10) | 0.811 § |
| Satisfaction with information from dermatologist, median (range) | 6 (0–9) | 9 (6–10) | 0.01 § | 9 (8–10) | 0.397 § | 9 (8–10) | 0.900 § |
| Satisfaction with disease control, median (range) | 3 (0–8) | 9 (6–10) | <0.001 § | 9 (8–10) | 0.140 § | 9 (7–10) | 0.796 § |
| Satisfaction with frequency of administration, median (range) | 2 (0–9) | 9 (6–10) | 0.001 § | 9 (7–10) | 0.395 § | 9 (7–10) | 0.147 § |
| Effectiveness of treatment to prolong time between flares, median (range) | 2 (0–9) | 9 (6–10) | <0.001 § | 9 (6–10) | 0.733 § | 9 (5–10) | 0.362 § |
| Effectiveness of treatment in control of flares, median (range) | 2 (0–8) | 9 (6–10) | <0.001 § | 9 (4–10) | 0.887 § | 9 (7–10) | 0.104 § |
| Overall satisfaction, median (range) | 4 (0–10) | 9 (8–10) | 0.001 § | 9 (7–10) | 0.640 § | 9 (4–10) | <0.001 § * |
| Variable | Week 16 | Week 40 | Week 52 | p Value |
|---|---|---|---|---|
| Satisfaction, mean (SD) | 90.9 (24.2) | 92.7 (13.4) | 83.6 (19.6) | 0.079 ∞ |
| Problem solution, mean (SD) | 100 (0.0)) | 96.3 (8.0) | 100 (0.0) | 0.135 ∞ |
| Perception of emotional change, mean (SD) | 67.1 (19.4) | 71.5 (12.6) | 69.3 (10.2) | 0.690 ∞ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marron, S.E.; Tomas-Aragones, L.; Moncin-Torres, C.A.; Gomez-Barrera, M.; Aranibar, F.J.G.-L.d. Patient Reported Outcome Measure in Atopic Dermatitis Patients Treated with Dupilumab: 52-Weeks Results. Life 2021, 11, 617. https://doi.org/10.3390/life11070617
Marron SE, Tomas-Aragones L, Moncin-Torres CA, Gomez-Barrera M, Aranibar FJG-Ld. Patient Reported Outcome Measure in Atopic Dermatitis Patients Treated with Dupilumab: 52-Weeks Results. Life. 2021; 11(7):617. https://doi.org/10.3390/life11070617
Chicago/Turabian StyleMarron, Servando E., Lucia Tomas-Aragones, Carlos A. Moncin-Torres, Manuel Gomez-Barrera, and Francisco Javier Garcia-Latasa de Aranibar. 2021. "Patient Reported Outcome Measure in Atopic Dermatitis Patients Treated with Dupilumab: 52-Weeks Results" Life 11, no. 7: 617. https://doi.org/10.3390/life11070617