
Abnormal Intracranial Pulse Pressure Amplitude Despite Normalized Static Intracranial Pressure in Idiopathic Intracranial Hypertension Refractory to Conservative Medical Therapy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Approvals and Study Design
2.2. IIH Patients
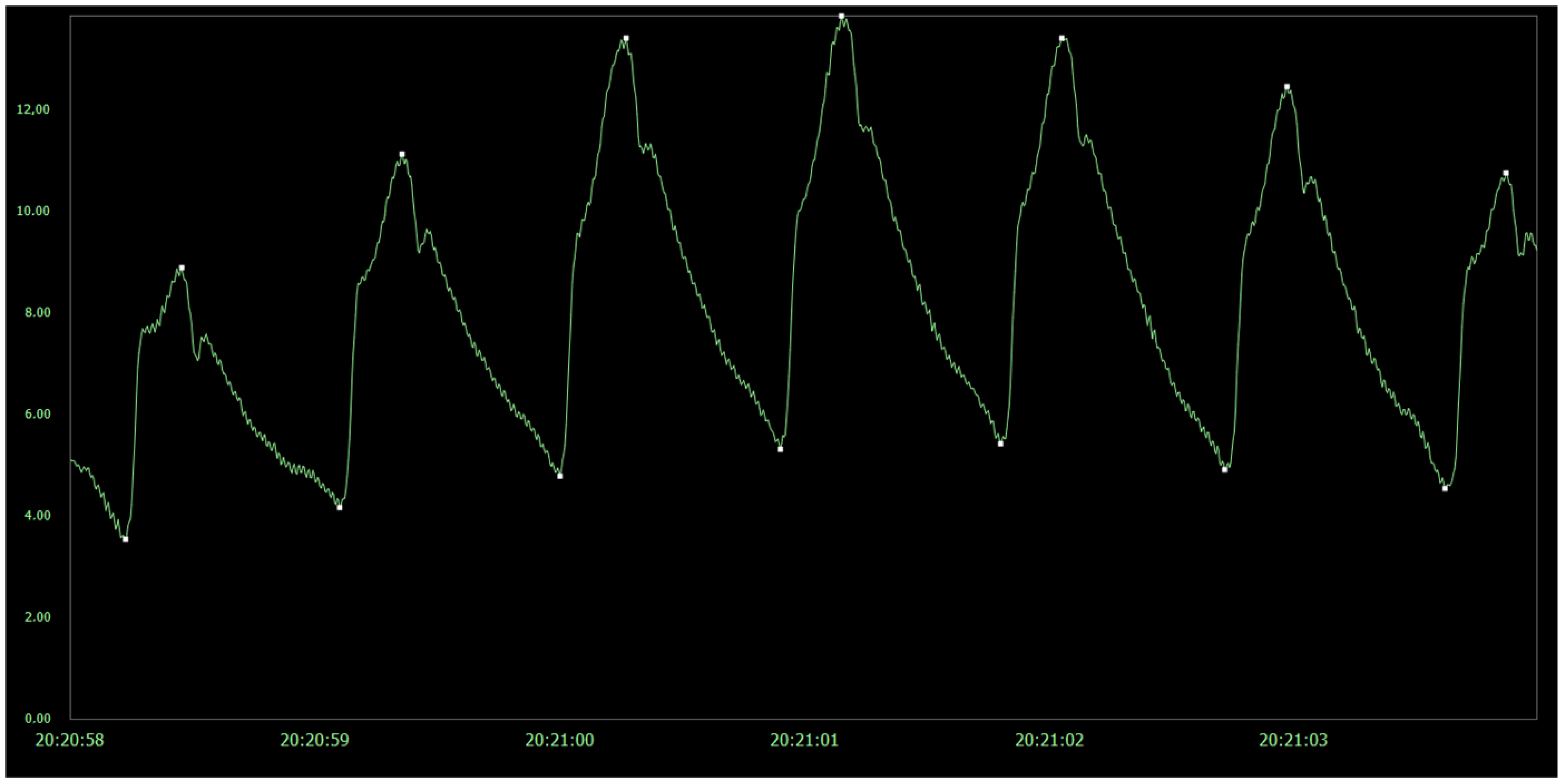
2.3. Measurements of Pulsatile and Static ICP
2.4. Statistical Analyses
3. Results
3.1. Patients
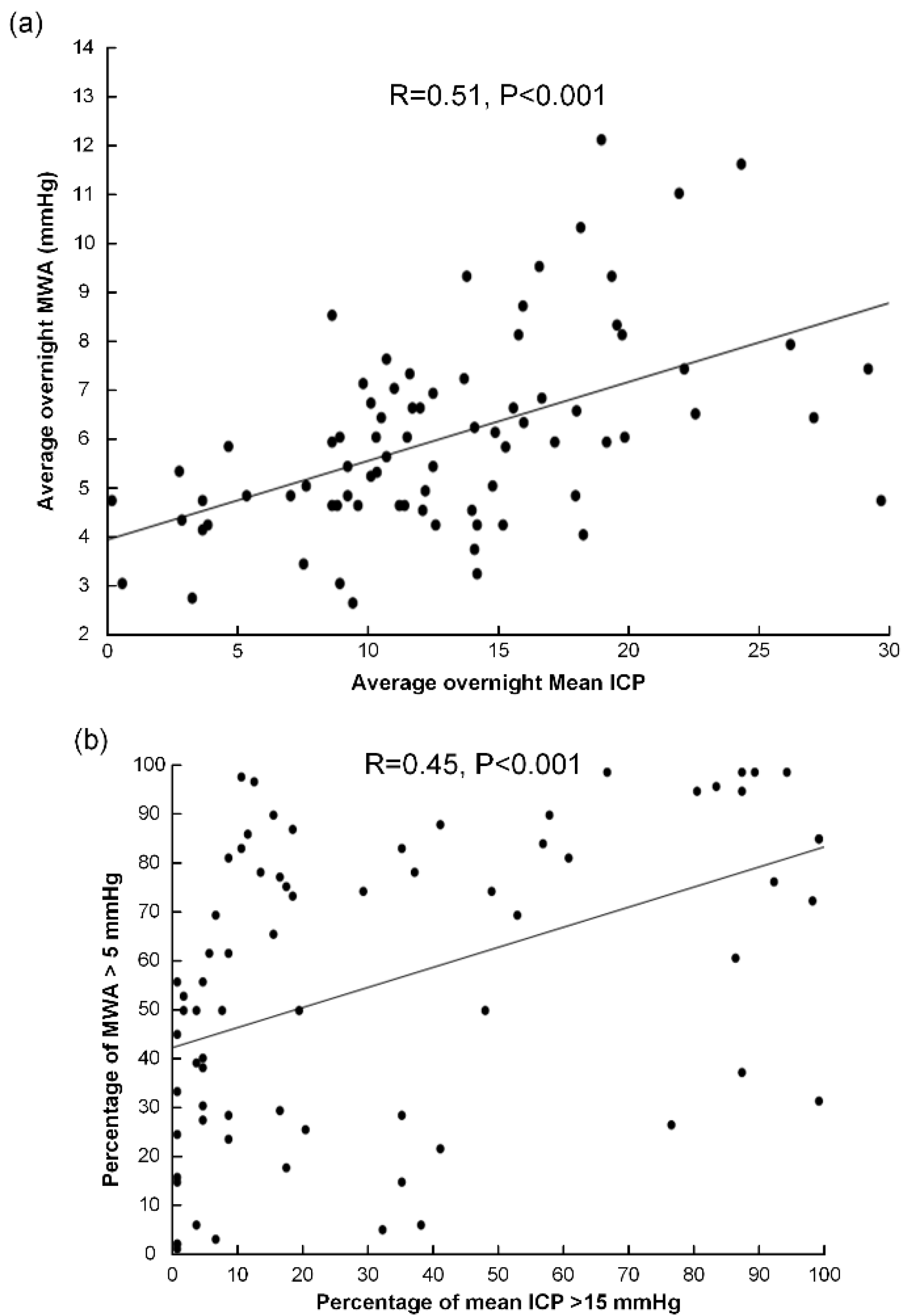
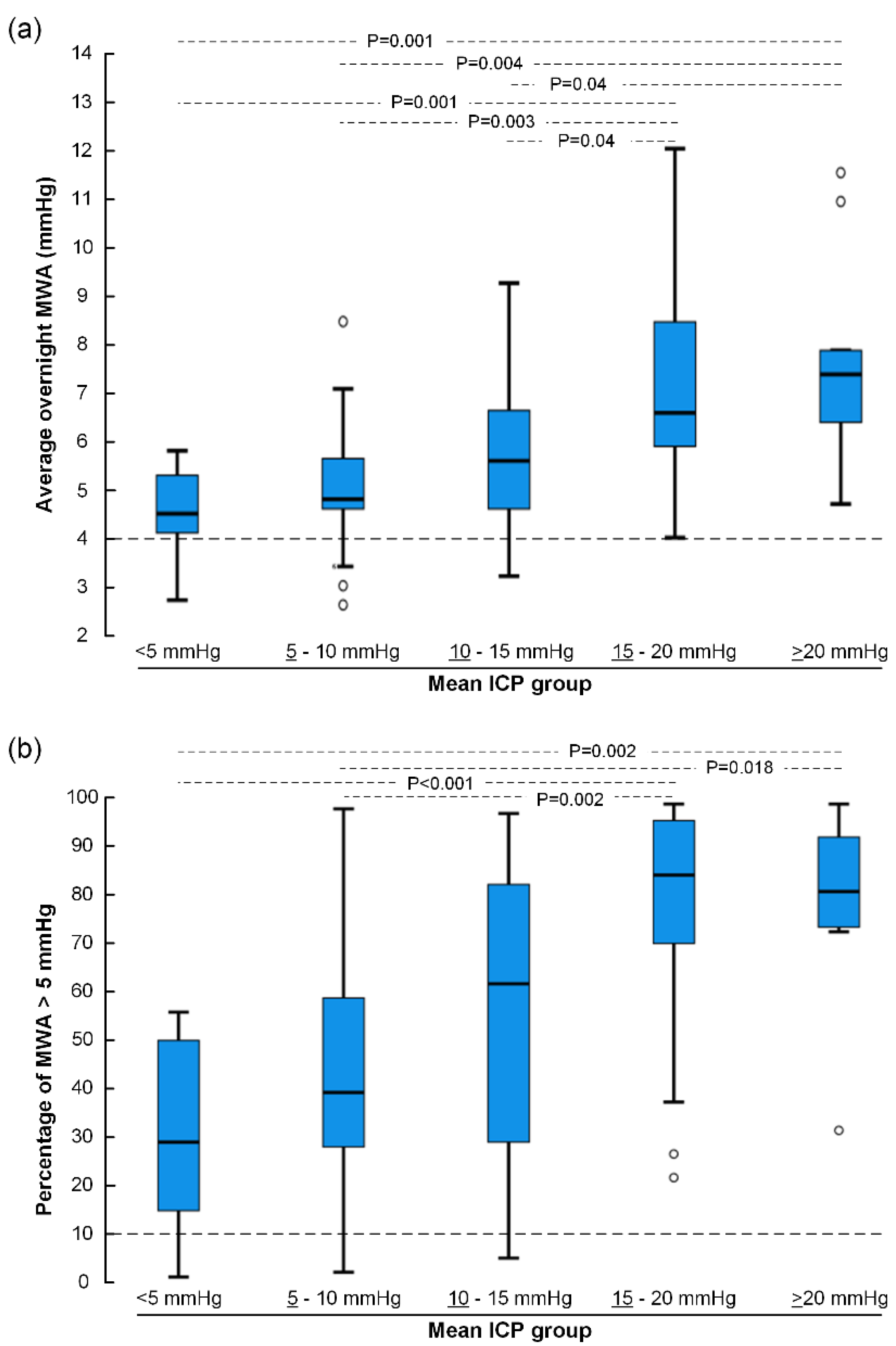
3.2. Pulsatile Versus Static ICP at Group Level
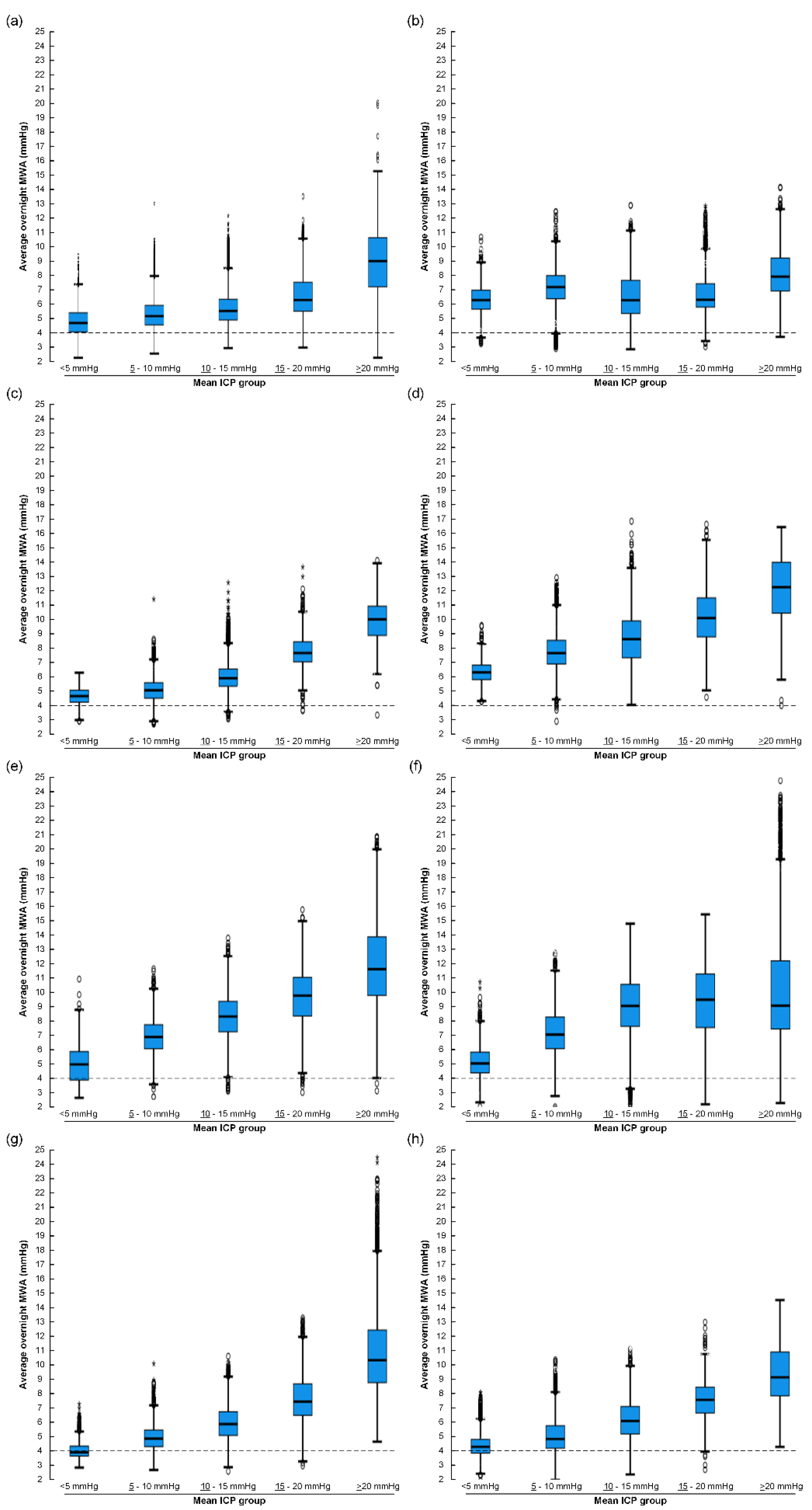
3.3. Pulsatile Versus Static ICP at the Individual Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mollan, S.P.; Davies, B.; Silver, N.C.; Shaw, S.; Mallucci, C.L.; Wakerley, B.R.; Krishnan, A.; Chavda, S.V.; Ramalingam, S.; Edwards, J.; et al. Idiopathic intracranial hypertension: Consensus guidelines on management. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1088–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ball, A.K.; Clarke, C.E. Idiopathic intracranial hypertension. Lancet Neurol. 2006, 5, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Kharkar, S.; Hernandez, R.; Batra, S.; Metellus, P.; Hillis, A.; Williams, M.A.; Rigamonti, D. Cognitive impairment in patients with Pseudotumor Cerebri Syndrome. Behav. Neurol. 2011, 24, 143–148. [Google Scholar] [CrossRef]
- Yri, H.M.; Fagerlund, B.; Forchhammer, H.B.; Jensen, R.H. Cognitive function in idiopathic intracranial hypertension: A prospective case-control study. BMJ Open 2014, 4, e004376. [Google Scholar] [CrossRef] [Green Version]
- Kunte, H.; Schmidt, F.; Kronenberg, G.; Hoffmann, J.; Schmidt, C.; Harms, L.; Goektas, O. Olfactory dysfunction in patients with idiopathic intracranial hypertension. Neurology 2013, 81, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Mollan, S.P.; Ali, F.; Hassan-Smith, G.; Botfield, H.; Friedman, D.I.; Sinclair, A.J. Evolving evidence in adult idiopathic intracranial hypertension: Pathophysiology and management. J. Neurol. Neurosurg. Psychiatry 2016, 87, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Kalyvas, A.V.; Hughes, M.; Koutsarnakis, C.; Moris, D.; Liakos, F.; Sakas, D.E.; Stranjalis, G.; Fouyas, I. Efficacy, complications and cost of surgical interventions for idiopathic intracranial hypertension: A systematic review of the literature. Acta Neurochir. 2017, 159, 33–49. [Google Scholar] [CrossRef] [PubMed]
- Friesner, D.; Rosenman, R.; Lobb, B.M.; Tanne, E. Idiopathic intracranial hypertension in the USA: The role of obesity in establishing prevalence and healthcare costs. Obes. Rev. 2011, 12, e372–e380. [Google Scholar] [CrossRef]
- Yri, H.M.; Wegener, M.; Sander, B.; Jensen, R. Idiopathic intracranial hypertension is not benign: A long-term outcome study. J. Neurol. 2012, 259, 886–894. [Google Scholar] [CrossRef]
- Eide, P.K.; Brean, A. Lumbar cerebrospinal fluid pressure waves versus intracranial pressure waves in idiopathic normal pressure hydrocephalus. Br. J. Neurosurg. 2006, 20, 407–414. [Google Scholar] [CrossRef]
- Evensen, K.B.; Eide, P.K. Measuring intracranial pressure by invasive, less invasive or non-invasive means: Limitations and avenues for improvement. Fluids Barriers CNS 2020, 17, 1–33. [Google Scholar] [CrossRef]
- Eide, P.K.; Kerty, E. Static and pulsatile intracranial pressure in idiopathic intracranial hypertension. Clin. Neurol. Neurosurg. 2011, 113, 123–128. [Google Scholar] [CrossRef]
- Eide, P.K. The correlation between pulsatile intracranial pressure and indices of intracranial pressure-volume reserve capacity: Results from ventricular infusion testing. J. Neurosurg. 2016, 125, 1493–1503. [Google Scholar] [CrossRef] [Green Version]
- Eide, P.K.; Pripp, A.H.; Ringstad, G.; Valnes, L.M. Impaired glymphatic function in idiopathic intracranial hypertension. Brain Commun. 2021. [Google Scholar] [CrossRef]
- Ringstad, G.; Valnes, L.M.; Dale, A.M.; Pripp, A.H.; Vatnehol, S.S.; Emblem, K.E.; Mardal, K.A.; Eide, P.K. Brain-wide glymphatic enhancement and clearance in humans assessed with MRI. JCI Insight 2018, 3, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Eide, P.K.; Sorteberg, W. Diagnostic intracranial pressure monitoring and surgical management in idiopathic normal pressure hydrocephalus: A 6-year review of 214 patients. Neurosurgery 2010, 66, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A paravascular pathway facilitates CSF flow through the brain parenchyma and the clearance of interstitial solutes, including amyloid beta. Sci. Transl. Med. 2012, 4, ra111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mestre, H.; Tithof, J.; Du, T.; Song, W.; Peng, W.; Sweeney, A.M.; Olveda, G.; Thomas, J.H.; Nedergaard, M.; Kelley, D.H. Flow of cerebrospinal fluid is driven by arterial pulsations and is reduced in hypertension. Nat. Commun. 2018, 9. [Google Scholar] [CrossRef]
- Fric, R.; Eide, P.K. Comparative observational study on the clinical presentation, intracranial volume measurements, and intracranial pressure scores in patients with either Chiari malformation Type I or idiopathic intracranial hypertension. J. Neurosurg. 2017, 126, 1312–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mollan, S.P.; Aguiar, M.; Evison, F.; Frew, E.; Sinclair, A.J. The expanding burden of idiopathic intracranial hypertension. Eye 2019, 33, 478–485. [Google Scholar] [CrossRef] [Green Version]
- Raoof, N.; Sharrack, B.; Pepper, I.M.; Hickman, S.J. The incidence and prevalence of idiopathic intracranial hypertension in Sheffield, UK. Eur. J. Neurol. 2011, 18, 1266–1268. [Google Scholar] [CrossRef]
- Corbett, J.J.; Mehta, M.P. Cerebrospinal fluid pressure in normal obese subjects and patients with pseudotumor cerebri. Neurology 1983, 33, 1386–1388. [Google Scholar] [CrossRef]
- Eide, P.K.; Sorteberg, W. Association among intracranial compliance, intracranial pulse pressure amplitude and intracranial pressure in patients with intracranial bleeds. Neurol. Res. 2007, 29, 798–802. [Google Scholar] [CrossRef]
- Sweeney, M.D.; Ayyadurai, S.; Zlokovic, B.V. Pericytes of the neurovascular unit: Key functions and signaling pathways. Nat. Neurosci. 2016, 19, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Winkler, E.A.; Sagare, A.P.; Zlokovic, B.V. The pericyte: A forgotten cell type with important implications for Alzheimer’s disease? Brain Pathol. 2014, 24, 371–386. [Google Scholar] [CrossRef] [PubMed]
- Mathiisen, T.M.; Lehre, K.P.; Danbolt, N.C.; Ottersen, O.P. The perivascular astroglial sheath provides a complete covering of the brain microvessels: An electron microscopic 3D reconstruction. Glia 2010, 58, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Nagelhus, E.A.; Ottersen, O.P. Physiological roles of aquaporin-4 in brain. Physiol. Rev. 2013, 93, 1543–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, E.H.; Eide, P.K.; Zurakowski, D.; Madsen, J.R. Impaired pulsation absorber mechanism in idiopathic normal pressure hydrocephalus: Laboratory investigation. J. Neurosurg. 2012, 117, 1189–1196. [Google Scholar] [CrossRef]
- Eidsvaag, V.A.; Hansson, H.A.; Heuser, K.; Nagelhus, E.A.; Eide, P.K. Cerebral microvascular abnormalities in patients with idiopathic intracranial hypertension. Brain Res. 2018, 1686, 72–82. [Google Scholar] [CrossRef]
- Hasan-Olive, M.M.; Hansson, H.A.; Enger, R.; Nagelhus, E.A.; Eide, P.K. Blood-Brain Barrier Dysfunction in Idiopathic Intracranial Hypertension. J. Neuropathol. Exp. Neurol. 2019, 78, 808–818. [Google Scholar] [CrossRef]
- Eide, P.K.; Eidsvaag, V.A.; Nagelhus, E.A.; Hansson, H.A. Cortical astrogliosis and increased perivascular aquaporin-4 in idiopathic intracranial hypertension. Brain Res. 2016, 1644, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Eide, P.K.; Hasan-Olive, M.M.; Hansson, H.A.; Enger, R. Increased occurrence of pathological mitochondria in astrocytic perivascular endfoot processes and neurons of idiopathic intracranial hypertension. J. Neurosci. Res. 2021, 99, 467–480. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | IIH Patients |
|---|---|
| N | 80 |
| F (N, %) | 67 (84%) |
| M (N, %) | 13 (16%) |
| Age (years) | 30.6 ± 13.5 |
| BMI (kg/m2) | 30.1 ± 7.0 |
| MWA Category (mmHg) | Mean ICP Category (mmHg) | |||||
|---|---|---|---|---|---|---|
| <5 | ≥5–<10 | ≥10–<15 | ≥15–<20 | ≥20 | Total (N, %) | |
| <4 | 2 | 3 | 2 | - | - | 7 (8.8%) |
| ≥4–<5 | 5 | 6 | 7 | 3 | 1 | 22 (27.5%) |
| ≥5 | 3 | 6 | 18 | 16 | 8 | 51 (63.8%) |
| Total (N, %) | 10 (12.5%) | 15 (18.8%) | 27 (33.8%) | 19 (23.8%) | 9 (11.3%) | 80 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eide, P.K. Abnormal Intracranial Pulse Pressure Amplitude Despite Normalized Static Intracranial Pressure in Idiopathic Intracranial Hypertension Refractory to Conservative Medical Therapy. Life 2021, 11, 537. https://doi.org/10.3390/life11060537
Eide PK. Abnormal Intracranial Pulse Pressure Amplitude Despite Normalized Static Intracranial Pressure in Idiopathic Intracranial Hypertension Refractory to Conservative Medical Therapy. Life. 2021; 11(6):537. https://doi.org/10.3390/life11060537
Chicago/Turabian StyleEide, Per Kristian. 2021. "Abnormal Intracranial Pulse Pressure Amplitude Despite Normalized Static Intracranial Pressure in Idiopathic Intracranial Hypertension Refractory to Conservative Medical Therapy" Life 11, no. 6: 537. https://doi.org/10.3390/life11060537