
Magnetic Resonance Imaging Features and Clinical Findings in Pediatric Idiopathic Intracranial Hypertension: A Case–Control Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
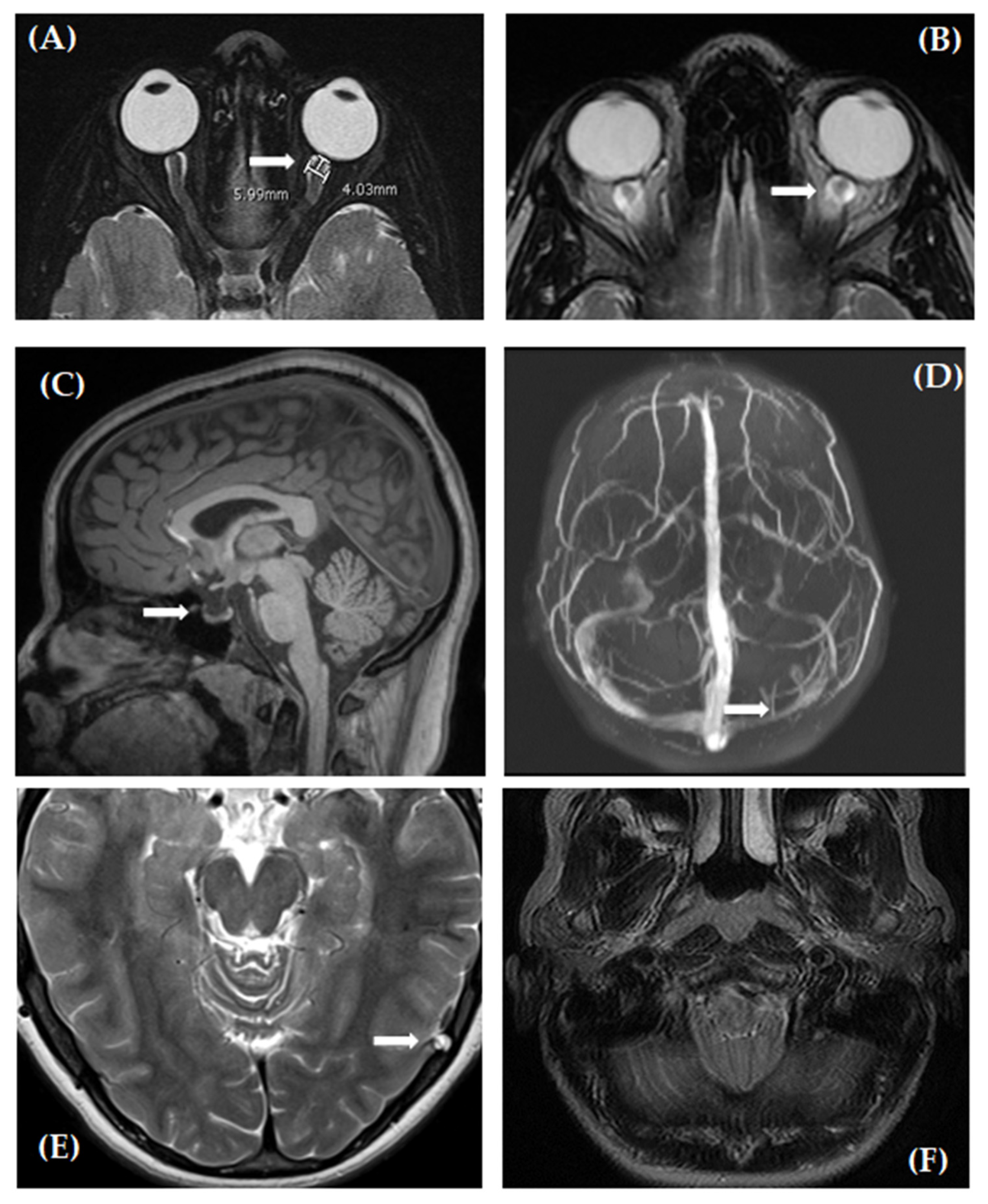
2.3. Quantitative Assessment of Neuroimaging
2.4. Qualitative Assessment of Neuroimaging
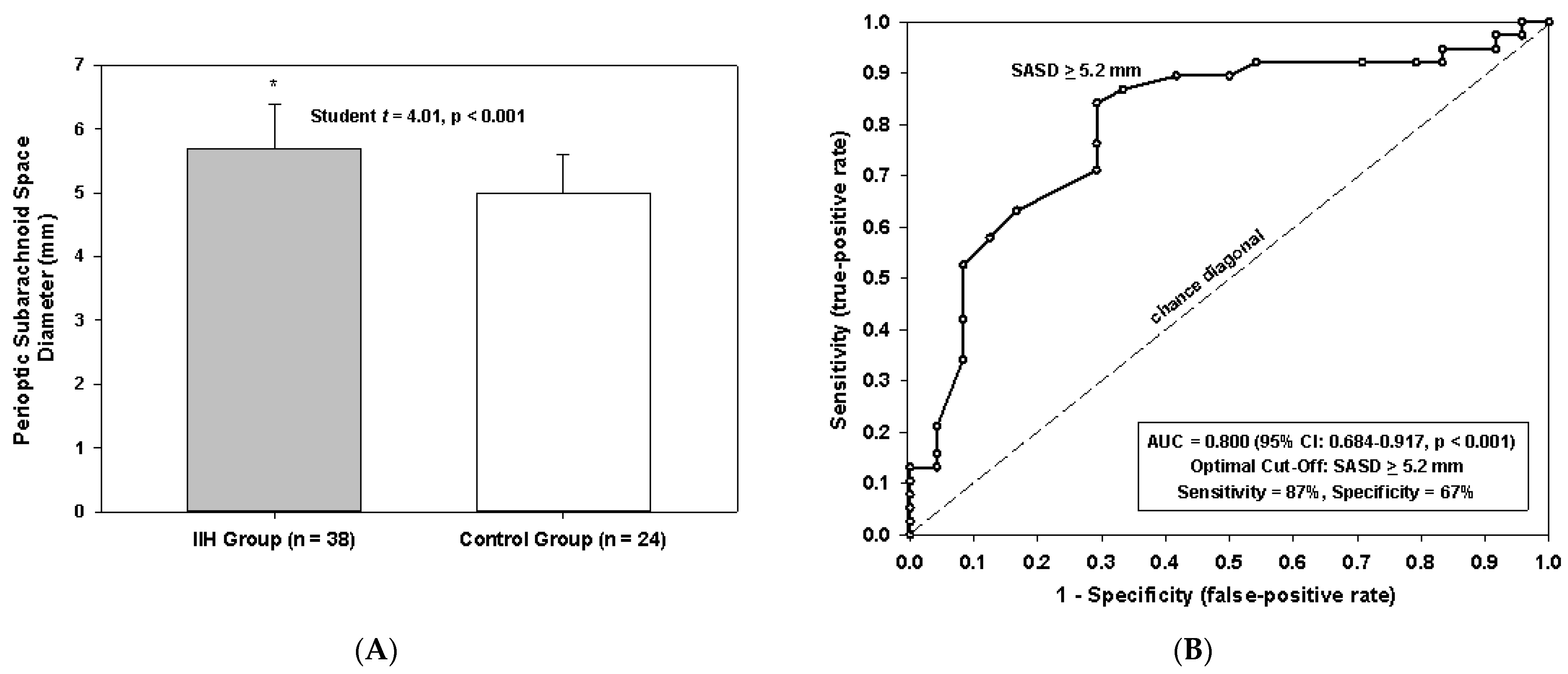
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cinciripini, G.S.; Donahue, S.; Borchert, M.S. Idiopathic intracranial hypertension in prepubertal pediatric patients: Characteristics, treatment, and outcome. Am. J. Ophthalmol. 1999, 127, 178–182. [Google Scholar] [CrossRef]
- Stiebel-Kalish, H.; Kalish, Y.; Lusky, M.; Gaton, D.D.; Ehrlich, R.; Shuper, A. Puberty as a risk factor for less favorable visual outcome in idiopathic intracranial hypertension. Am. J. Ophthalmol. 2006, 142, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, M.C.; Vaphiades, M. Magnetic resonance imaging in pseudotumor cerebri. Ophthalmology 1998, 105, 1686–1693. [Google Scholar] [CrossRef]
- Görkem, S.B.; Doğanay, S.; Canpolat, M.; Koc, G.; Dogan, M.S.; Per, H.; Coskun, A. MR imaging findings in children with pseudotumor cerebri and comparison with healthy controls. Childs. Nerv. Syst. 2015, 31, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Hirfanoglu, T.; Aydin, K.; Serdaroglu, A.; Havali, C. Novel Magnetic Resonance Imaging Findings in Children with Intracranial Hypertension. Pediatr. Neurol. 2015, 53, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Shofty, B.; Ben-Sira, L.; Constantini, S.; Freedman, S.; Kelser, A. Optic nerve sheath diameter on MR imaging: Establishment of norms and comparison of pediatric patients with idiopathic intracranial hypertension with healthy controls. AJNR. Am. J. Neuroradiol. 2012, 33, 366–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, M.J.; Pushparajah, K.; Jan, W.; Calver, D.; Lin, J. Magnetic resonance imaging changes in idiopathic intracranial hypertension in children. J. Child. Neurol. 2010, 25, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.J.; Soares, B.P.; Bruce, B.B.; Saindane, A.M.; Newman, N.J.; Biousse, V.; Peragallo, J.H. Imaging Features of Idiopathic Intracranial Hypertension in Children. J. Child. Neurol. 2017, 32, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Kohli, A.A.; Vossough, A.; Mallery, R.M.; Woo, J.H.; Sheldon, C.A.; Paley, G.L.; Digre, K.B.; Fridman, D.I.; Farrar, J.T.; McComack, S.E.; et al. Magnetic Resonance Imaging Findings in Pediatric Pseudotumor Cerebri Syndrome. Pediatr. Neurol. 2019, 99, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Rosa, N.; Giamundo, A.; Jura, A.; Iaccarino, G.; Romano, A. Mesalazine-associated benign intracranial hypertension in a patient with ulcerative colitis. Am. J. Ophthalmol. 2003, 136, 212–213. [Google Scholar] [CrossRef]
- Price, D.A.; Grzybowski, A.; Eikenberry, J.; Januleviciene, I.; Verticchio Vercellin, A.C.; Mathew, S.; Siesky, B.; Harris, A. Review of non-invasive intracranial pressure measurement techniques for ophthalmology applications. Br. J. Ophthalmol. 2020, 104, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Radvany, M.G.; Solomon, D.; Nijjar, S.; Subramanian, P.S.; Miller, N.R.; Rigamonti, D.; Blitz, A.; Gailloud, P.; Moghekar, A. Visual and neurological outcomes following endovascular stenting for pseudotumor cerebri associated with transverse sinus stenosis. J. Neuroophthalmol. 2013, 33, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.I.; Liu, G.T.; Digre, K.B. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2013, 81, 1159–1165. [Google Scholar] [CrossRef]
- Lam, B.L.; Glasier, C.M.; Feuer, W.J. Subarachnoid fluid of the optic nerve in normal adults. Ophthalmology 1997, 104, 1629–1633. [Google Scholar] [CrossRef]
- Watanabe, A.; Kinouchi, H.; Horikoshi, T.; Uchida, M.; Ishigame, K. Effect of intracranial pressure on the diameter of the optic nerve sheath. J. Neurosurg. 2008, 109, 255–258. [Google Scholar] [CrossRef]
- Passi, N.; Degnan, A.J.; Levy, L.M. MR Imaging of Papilledema and Visual Pathways: Effects of Increased Intracranial Pressure and Pathophysiologic Mechanisms. Am. J. Neuroradiol. 2013, 34, 919–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staffa, S.J.; Zurakowski, D. Statistical power and sample size calculations: A primer for pediatric surgeons. J. Pediatric Surg. 2020, 55, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology 2005, 16, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.N.; Gillard, J.H.; Owler, B.K.; Harkness, K.; Pickard, J.D. MR venography in idiopathic intracranial hypertension: Unappreciated and misunderstood. J. Neurol. Neurosurg. Psychiatry 2004, 75, 621–625. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | IIH Patients (n = 38) | Control Group (n = 24) | Univariate p-Value |
|---|---|---|---|
| Demographics, Clinical Symptoms | |||
| Age, years | 11.9 ± 4.7 | 13.9 ± 3.2 | 0.071 |
| Female gender (%) | 24 (63) | 17 (71) | 0.591 |
| Body mass index, kg/m2 | 27.2 ± 9.9 | 23.5 ± 7.1 | 0.119 |
| Lumbar puncture pressure, cm H2O | 40 ± 10 | NP | - |
| Sixth nerve palsy (%) | 6 (16) | 0 (0) | 0.073 |
| Headache (%) | 27/37 (73) | 13 (54) | 0.171 |
| Pulsatile tinnitus (%) | 11/33 (33) | 0 (0) | 0.001 |
| Transient visual obscurations (%) | 7/28 (25) | 1 (4) | 0.056 |
| Diplopia (%) | 10/33 (30) | 1 (4) | 0.017 |
| MRI Signs | |||
| Perioptic subarachnoid space diameter, mm | 5.7 ± 0.7 | 5.0 ± 0.6 | <0.001 |
| Posterior globe flattening (%) | 28 (74) | 0 (0) | <0.001 |
| Optic nerve protrusion (%) | 17 (45) | 0 (0) | <0.001 |
| Empty sella (%) | 20 (53) | 2 (8) | <0.001 |
| Dural Venus Sinus Abnormalities (%) | 20/29 (69) | 9 (38) | 0.029 |
| Foramen magnum crowding (%) | 1 (3) | 1 (4) | 1.000 |
| Prominent arachnoid granulations (%) | 3 (8) | 5 (21) | 0.242 |
| Total Score per Patient | Predicted Probability IIH (%) |
|---|---|
| 0 | 3 |
| 1 | 17 |
| 2 | 55 |
| 3 | 93 |
| 4 | 99 |
| 5 | 100 |
| 6 | 100 |
| 7 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilbert, A.L.; Vaughn, J.; Whitecross, S.; Robson, C.D.; Zurakowski, D.; Heidary, G. Magnetic Resonance Imaging Features and Clinical Findings in Pediatric Idiopathic Intracranial Hypertension: A Case–Control Study. Life 2021, 11, 487. https://doi.org/10.3390/life11060487
Gilbert AL, Vaughn J, Whitecross S, Robson CD, Zurakowski D, Heidary G. Magnetic Resonance Imaging Features and Clinical Findings in Pediatric Idiopathic Intracranial Hypertension: A Case–Control Study. Life. 2021; 11(6):487. https://doi.org/10.3390/life11060487
Chicago/Turabian StyleGilbert, Aubrey L., Jennifer Vaughn, Sarah Whitecross, Caroline D. Robson, David Zurakowski, and Gena Heidary. 2021. "Magnetic Resonance Imaging Features and Clinical Findings in Pediatric Idiopathic Intracranial Hypertension: A Case–Control Study" Life 11, no. 6: 487. https://doi.org/10.3390/life11060487