
Comparison of Androgen Receptor, VEGF, HIF-1, Ki67 and MMP9 Expression between Non-Metastatic and Metastatic Stages in Stromal and Tumor Cells of Oral Squamous Cell Carcinoma

 ,
,
Abstract
:1. Introduction
2. Material and Subjects
Statistics
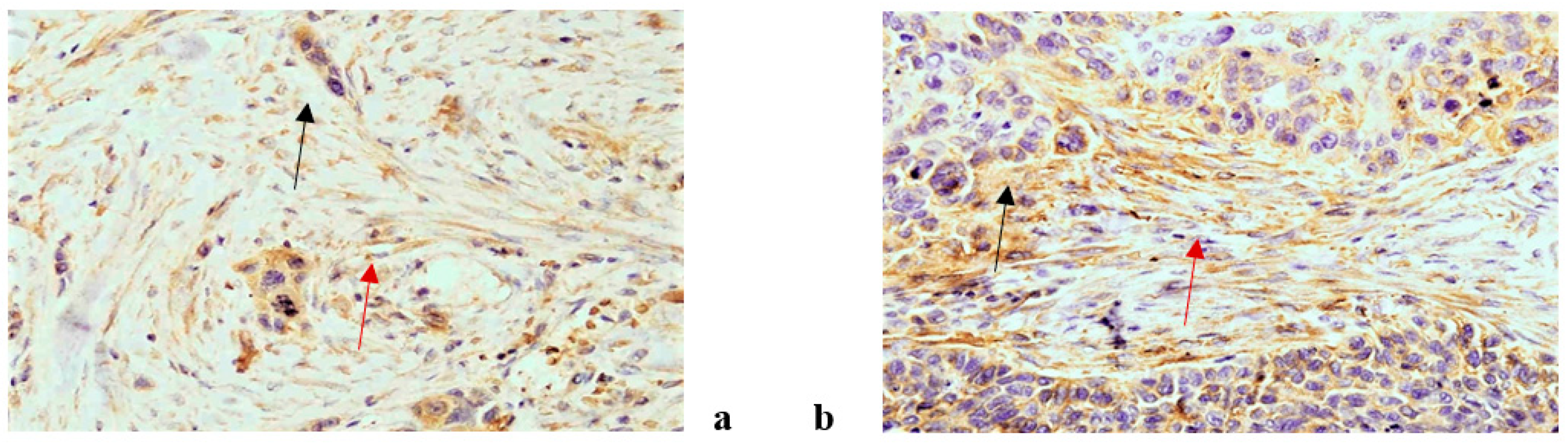
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, L.; Chen, J.; Cai, X.; Yao, Z.; Huang, J. Progress in targeted therapeutic drugs for oral squamous cell carcinoma. Surg. Oncol. 2019, 31, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Shigetomi, S.; Imanishi, Y.; Shibata, K.; Sakai, N.; Sakamoto, K.; Fujii, R.; Habu, N.; Otsuka, K.; Sato, Y.; Watanabe, Y.; et al. VEGF-C/Flt-4 axis in tumor cells contributes to the progression of oral squamous cell carcinoma via upregulating VEGF-C itself and contactin-1 in an autocrine manner. Am. J. Cancer Res. 2018, 8, 2046–2063. [Google Scholar] [PubMed]
- Koyfman, S.A.; Ismaila, N.; Crook, D.; D’Cruz, A.; Rodriguez, C.P.; Sher, D.J.; Silbermins, D.; Sturgis, E.M.; Tsue, T.T.; Weiss, J.; et al. Management of the Neck in Squamous Cell Carcinoma of the Oral Cavity and Oropharynx: ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 1753–1774. [Google Scholar] [CrossRef] [PubMed]
- Rivera, C.; Oliveira, A.K.; Costa, R.A.P.; De Rossi, T.; Leme, A.F.P. Prognostic biomarkers in oral squamous cell carcinoma: A systematic review. Oral Oncol. 2017, 72, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Modjtahedi, H. Molecular therapy of head and neck cancer. Cancer Metastasis Rev. 2005, 24, 129–146. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, A.P.G.; Vicente, C.M.; Porto, C.S. Estrogen Receptors Promote Migration, Invasion and Colony Formation of the Androgen-Independent Prostate Cancer Cells PC-3 Through β-Catenin Pathway. Front. Endocrinol. (Lausanne) 2020, 11. [Google Scholar] [CrossRef]
- Chang, W.-C.; Chang, C.-F.; Li, Y.-H.; Yang, C.-Y.; Su, R.-Y.; Lin, C.-K.; Chen, Y.-W. A histopathological evaluation and potential prognostic implications of oral squamous cell carcinoma with adverse features. Oral Oncol. 2019, 95, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Tomasovic-Loncaric, C.; Fucic, A.; Andabak, A.; Andabak, M.; Ceppi, M.; Bruzzone, M.; Vrdoljak, D.; Vucicevic-Boras, V. Androgen Receptor as a Biomarker of Oral Squamous Cell Carcinoma Progression Risk. Anticancer. Res. 2019, 39, 4285–4289. [Google Scholar] [CrossRef]
- Miguelánez-Medrán, B.C.; Pozo-Kreilinger, J.J.; Cebrián-Carretero, J.L.; Martínez-García, M.A.; López-Sánchez, A.F. Oral squamous cell carcinoma of tongue: Histological risk assessment. A pilot study. Med. Oral. Patol. Oral. Cir. Bucal. 2019, 1, e603–e609. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.P.; Javan, L.; Dineshkumar, T.; Raman, S. Oral squamous cell carcinoma under microscopic vision: A review of histological variants and its prognostic indicators. SRM J. Res. Dent. Sci. 2019, 10, 90–97. [Google Scholar] [CrossRef]
- Taghavi, N.; Yazdi, I. Prognostic factors of survival rate in oral squamous cell carcinoma: Clinical, histologic, genetic and molecular concepts. Arch. Iran. Med. 2015, 18, 314–319. [Google Scholar]
- Sheelam, S.; Reddy, S.P.; Kulkarni, P.G.; Nandan, S.; Keerthi, M.; Raj, G.S. Role of cell proliferation and vascularity in malignant transformation of potentially malignant disorders. J. Oral Maxillofac. Pathol. 2018, 22, 281. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Li, W.; Zhu, J.; Deng, S.; Tao, X. Low expression of RECK in oral squamous cell carcinoma patients induces a shorter survival rate through an imbalance of RECK/MMPs. Int. J. Clin. Exp. Pathol. 2020, 13, 501–508. [Google Scholar]
- Zheng, H.; Takahashi, H.; Murai, Y.; Cui, Z.; Nomoto, K.; Niwa, H.; Tsuneyama, K.; Takano, Y. Expressions of MMP-2, MMP-9 and VEGF are closely linked to growth, invasion, metastasis and angiogenesis of gastric carcinoma. Anticancer. Res. 2006, 26, 3579–3583. [Google Scholar]
- Patel, N.R.; Jain, L.; Mahajan, A.M.; Hiray, P.V.; Shinde, S.S.; Patel, P.A. An Immunohistochemical Study of HIF-1 Alpha in Oral Epithelial Dysplasia and Oral Squamous Cell Carcinoma. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.-T.; Wong, Y.-K.; Chan, M.-Y.; Chang, K.-W.; Chen, S.-C.; Chang, C.-T.; Wang, J. The correlation between HIF-1 alpha and VEGF in oral squamous cell carcinomas: Expression patterns and quantitative immunohistochemical analysis. J. Chin. Med Assoc. 2018, 81, 370–375. [Google Scholar] [CrossRef]
- Eisermann, K.; Fraizer, G. The Androgen Receptor and VEGF: Mechanisms of Androgen-Regulated Angiogenesis in Prostate Cancer. Cancers 2017, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Qiu, J.; Jiang, M.; Song, W.; Yeh, S.; Yu, H.; Zang, L.; Xia, S.; Chang, C. Infiltrating T Cells Promote Bladder Cancer Progression via Increasing IL1→Androgen Receptor→HIF1α→VEGFa Signals. Mol. Cancer Ther. 2016, 15, 1943–1951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Wahlde, M.-K.; Hülsewig, C.; Rückert, C.; Götte, M.; Kiesel, L.; Bernemann, C. The anti-androgen drug dutasteride renders triple negative breast cancer cells more sensitive to chemotherapy via inhibition of HIF-1α-/VEGF-signaling. Gynecol. Endocrinol. 2014, 31, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Larsson, P.; Syed Khaja, A.S.; Semenas, J.; Wang, T.; Sarwar, M.; Dizeyi, N.; Simoulis, A.; Hedblom, A.; Wai, S.N.; Ødum, N.; et al. The functional interlink between AR and MMP9/VEGF signaling axis is mediated through PIP5K1α/pAKT in prostate cancer. Int. J. Cancer 2020, 146, 1686–1699. [Google Scholar] [CrossRef] [PubMed]
- D’Arcangelo, E.; Wu, N.C.; Cadavid, J.L.; McGuigan, A.P. The life cycle of cancer-associated fibroblasts within the tumour stroma and its importance in disease outcome. Br. J. Cancer 2020, 122, 931–942. [Google Scholar] [CrossRef] [PubMed]
- Curry, J.M.; Sprandio, J.; Cognetti, D.; Luginbuhl, A.; Bar-Ad, V.; Pribitkin, E.; Tuluc, M. Tumor Microenvironment in Head and Neck Squamous Cell Carcinoma. Semin. Oncol. 2014, 41, 217–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Liang, C.; Chen, M.; Su, W. Association between tumor-stroma ratio and prognosis in solid tumor patients: A systematic review and meta-analysis. Oncotarget 2016, 7, 68954–68965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dourado, M.R.; Guerra, E.N.S.; Salo, T.; Lambert, D.W.; Coletta, R.D. Prognostic value of the immunohistochemical detection of cancer-associated fibroblasts in oral cancer: A systematic review and meta-analysis. J. Oral Pathol. Med. 2018, 47, 443–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almangush, A.; Heikkinen, I.; Bakhti, N.; Mäkinen, L.K.; Kauppila, J.H.; Pukkila, M.; Hagström, J.; Laranne, J.; Soini, Y.; Kowalski, L.P.; et al. Prognostic impact or tumor-stroma ratio in early-stage oral tongue cancers. Histopathology 2018, 72, 1128–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jimenez, L.; Jayakar, S.K.; Ow, T.J.; Segall, J.E. Mechanisms of Invasion in Head and Neck Cancer. Arch. Pathol. Lab. Med. 2015, 139, 1334–1348. [Google Scholar] [CrossRef] [Green Version]
- Boccellino, M.; Di Stasio, D.; DiPalma, G.; Cantore, S.; Ambrosio, P.; Coppola, M.; Quagliuolo, L.; Scarano, A.; Malcangi, G.; Borsani, E.; et al. Steroids and growth factors in oral squamous cell carcinoma: Useful source of dental-derived stem cells to develop a steroidogenic model in new clinical strategies. Eur. Rev. Med. Pharmacol. Sci 2019, 23, 8730–8740. [Google Scholar] [PubMed]
- Jayanthi, P.; Varun, B.R.; Selvaraj, J. Epithelial–mesenchymal transition in oral squamous cell carcinoma: An insight into molecular mechanisms and clinical implications. J. Oral Maxillofac. Pathol. 2020, 24, 189. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-Y.; Li, X.-Y.; Tadashi, N.; Dong, P. Clinical significance of tumor-associated macrophage infiltration in supraglottic laryngeal carcinoma. Chin. J. Cancer 2011, 30, 280–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karagiannis, G.S.; Poutahidis, T.; Erdman, S.E.; Kirsch, R.; Riddell, R.H.; Diamandis, E.P. Cancer-Associated Fibroblasts Drive the Progression of Metastasis through both Paracrine and Mechanical Pressure on Cancer Tissue. Mol. Cancer Res. 2012, 10, 1403–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Qing, S.; Che, K.; Li, L.; Liao, X. Androgen receptor promotes oral squamous cell carcinoma cell migration by increasing EGFR phosphorylation. OncoTargets Ther. 2019, 12, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, C.; Fang, D.; Xu, H.; Wang, Q.; Xia, H. The androgen receptor expression and association with patient’s survival in different cancers. Genomics 2020, 112, 1926–1940. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.; Ribeiro-Silva, A. Prognostic significance of immunohistochemical biomarkers in oral squamous cell carcinoma. Int. J. Oral. Maxillofac. Surg. 2011, 40, 298–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goulioumis, A.K.; Varakis, J.; Goumas, P.; Papadaki, H. Androgen Receptor in Laryngeal Carcinoma: Could There Be an Androgen-Refratory Tumor? ISNR Oncol. 2011, 2011, 180518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisermann, K.; Broderick, C.J.; Bazarov, A.; Moazam, M.M.; Fraizer, G.C. Androgen up-regulates vascular endothelial growth factor expression in prostate cancer cells via an Sp1 binding site. Mol. Cancer 2013, 12, 7. [Google Scholar] [CrossRef] [Green Version]
- Mabjeesh, N.J.; Willard, M.T.; Frederickson, C.E.; Zhong, H.; Simons, J.W. Androgens Stimulate Hypoxia-inducible Factor 1 activation via autocrine loop of tyrosine kinase receptor/phosphatidylinositol3-kinase/protein kinase b in prostate cancer cells. Clin. Cancer Res 2003, 9, 2416–2425. [Google Scholar] [PubMed]
- Adamo, B.; Ricciardi, G.R.R.; Ieni, A. The prognostic significance of combined androgen receptor, E-Cadherin, Ki67 and CK5/6 expression in patients with triple negative breast cancer. Oncotarget 2017, 16, 76974–76986. [Google Scholar] [CrossRef] [Green Version]
- Pezzuto, A.; Carico, E.; Aldo, P.; Elisabetta, C. Role of HIF-1 in Cancer Progression: Novel Insights. A Review. Curr. Mol. Med. 2018, 18, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Eckert, A.W.; Wickenhauser, C.; Salins, P.C.; Kappler, M.; Bukur, J.; Seliger, B. Clinical relevance of the tumor microenvironment and immune escape of oral squamous cell carcinoma. J. Trans. Med. 2016, 14, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.Y.; Jang, Y.S.; Min, S.Y.; Song, J.Y. Overexpression of MMP-9 and HIF-1α in Breast Cancer Cells under Hypoxic Conditions. J. Breast Cancer 2011, 14, 88–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petruzzi, M.N.M.R.; Cherubini, K.; Salum, F.G.; De Figueiredo, M.A.Z. Role of tumour-associated macrophages in oral squamous cells carcinoma progression: An update on current knowledge. Diagn. Pathol. 2017, 12, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujita, S.; Sumi, M.; Tatsukawa, E.; Nagano, K.; Katase, N. Expressions of extracellular matrix-remodeling factors in lymph nodes from oral cancer patients. Oral Dis. 2020. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non Metastatic 96 Patients | |||||
|---|---|---|---|---|---|
| Age Years (mean) | Sex (%) | Tumor Localization (%) | Cervical Lymph Node Resection (%) | pT (%) | Stage Grouping pTNM (%) |
| 62.8 | Male 71.9 Female 28.1 | Alveola ridges 31.1 Hard palate 6.9 Retromolar 13.8 Buccal mucosa and bucco alveolar sulci 24.1 Floor of mouth 24.1 | No-node resection 36.5 node resection 63.5 | T1 19.8 T2 42.7 T3 10.4 T4 27.1 | I 11.5 II 50.8 III 8.2 IVa 29.5 |
| Metastatic 91 patients | |||||
| Age Years (mean) | Sex (%) | Tumor Localization (%) | Cervical Lymph Node Resection (%) | pT (%) | Stage Grouping pTNM (%) |
| 61.9 | Male 68 Female 32 | Alveolar ridges 37.9 Retromolar 6.9 Buccal mucosa and Bucco alveolar sulci 20.7 Floor of mouth 34.5 | No-node resection 0 node resection 100 | T1 12.1 T2 34.1 T3 17.6 T4 6.2 | III 20.9 IVa 76.9 VIb 29.5 |
| Biomarker | Non Metastatic N = 96, Mean ± SD | Metastatic N = 91, Mean ± SD | MR * | 95% CI | p |
|---|---|---|---|---|---|
| AR | |||||
| cytoplasm | 14.4 (20.1) | 17.5 (19.7) | 1.55 | 0.87–2.73 | 0.134 |
| epithelium | 3.3 (6.7) | 5.7 (10.8) | 1.44 | 0.97–2.12 | 0.070 |
| stroma | 1.8 (4.5) | 4.5 (8.9) | 1.48 | 1.01–2.18 | 0.047 |
| ki67 | |||||
| epithelium | 45.9 (14.7) | 50.1 (15.4) | 1.10 | 1.01–1.21 | 0.041 |
| stroma | 14.3 (7.5) | 12.2 (8.2) | 0.78 | 0.64–0.95 | 0.013 |
| HF1beta | |||||
| epithelium | 26.6 (29.1) | 14.3 (21.6) | 0.37 | 0.21–0.65 | 0.001 |
| stroma | 11.0 (19.2) | 6.4 (14.9) | 0.93 | 0.57–1.51 | 0.760 |
| VEGF | |||||
| epithelium | 15.5 (17.4) | 9.6 (15.1) | 0.48 | 0.29–0.80 | 0.005 |
| stroma | 16.5 (22.0) | 9.5 (12.8) | 0.57 | 0.34–0.97 | 0.036 |
| macrophages | 15.7 (22.4) | 5.5 (9.7) | 0.41 | 0.24–0.69 | 0.001 |
| lymphocytes | 0.8 (4.4) | 3.8 (10.4) | 1.49 | 1.07–2.08 | 0.019 |
| MMP9 | |||||
| epithelium | 18.9 (23.4) | 15.2 (25.7) | 0.54 | 0.30–0.98 | 0.044 |
| stroma | 39.1 (22.1) | 43.6 (25.0) | 1.22 | 0.88–1.69 | 0.240 |
| macrophages | 11.3 (15.5) | 15.4 (14.2) | 2.43 | 1.45–4.06 | 0.001 |
| lymphocytes | 27.5 (24.7) | 29.3 (24.7) | 1.17 | 0.58–2.33 | 0.662 |
| Mean Ratio [95% CI) | |||
|---|---|---|---|
| Cytoplasmic AR/Metastatic stage ª | |||
| >=20%/No | <20%/Yes | >=20%/Yes | |
| Ki67 epithelium | 0.89 (0.78–1.03) | 1.01 (0.90–1.14) | 1.14 * (1.01–1.30) |
| HF1beta epithelium | 1.01 (0.44–2.34) | 0.35 * (0.17–0.71) | 0.41 * (0.19–0.88) |
| VEGF macrophages | 0.52 (0.23–1.16) | 0.36 * (0.19–0.71) | 0.32 * (0.16–0.63) |
| VEGF lymphocytes | 1.35 (0.82–2.24) | 1.50 (0.98–2.29) | 1.80 * (1.15–2.80) |
| MMP9 macrophages | 1.62 (0.75–3.51) | 3.01 * (1.57–5.78) | 2.52 * (1.28–4.97) |
| Biomarker | Mean Ratio [95% CI) | ||
|---|---|---|---|
| TNM ª | |||
| 2 | 3 | 4 | |
| Ki67 stroma | 0.99 (0.75–1.32) | 1.09 (0.79–1.51) | 0.72 * (0.57–0.92) |
| HF1beta epithelium | 0.49 (0.22–1.12) | 0.18 * (0.07–0.46) | 0.37 * (0.18–0.74) |
| VEGF epithelium | 1.29 (0.63–2.66) | 0.95 (0.42–2.15) | 0.45 * (0.24–0.83) |
| VEGF lymphocytes | 0.87 (0.54–1.41) | 2.27 * (1.33–3.88) | 1.16 (0.78–1.74) |
| MMP9 macrophages | 1.27 (0.61–2.66) | 3.29 * (1.42–7.63) | 1.93 * (1.02–3.63) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batelja-Vuletic, L.; Tomasovic-Loncaric, C.; Ceppi, M.; Bruzzone, M.; Fucic, A.; Krstanac, K.; Boras Vucicevic, V. Comparison of Androgen Receptor, VEGF, HIF-1, Ki67 and MMP9 Expression between Non-Metastatic and Metastatic Stages in Stromal and Tumor Cells of Oral Squamous Cell Carcinoma. Life 2021, 11, 336. https://doi.org/10.3390/life11040336
Batelja-Vuletic L, Tomasovic-Loncaric C, Ceppi M, Bruzzone M, Fucic A, Krstanac K, Boras Vucicevic V. Comparison of Androgen Receptor, VEGF, HIF-1, Ki67 and MMP9 Expression between Non-Metastatic and Metastatic Stages in Stromal and Tumor Cells of Oral Squamous Cell Carcinoma. Life. 2021; 11(4):336. https://doi.org/10.3390/life11040336
Chicago/Turabian StyleBatelja-Vuletic, Lovorka, Cedna Tomasovic-Loncaric, Marcello Ceppi, Marco Bruzzone, Aleksandra Fucic, Karolina Krstanac, and Vanja Boras Vucicevic. 2021. "Comparison of Androgen Receptor, VEGF, HIF-1, Ki67 and MMP9 Expression between Non-Metastatic and Metastatic Stages in Stromal and Tumor Cells of Oral Squamous Cell Carcinoma" Life 11, no. 4: 336. https://doi.org/10.3390/life11040336