
Large Animal Model of Osteoporotic Defect Healing: An Alternative to Metaphyseal Defect Model

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
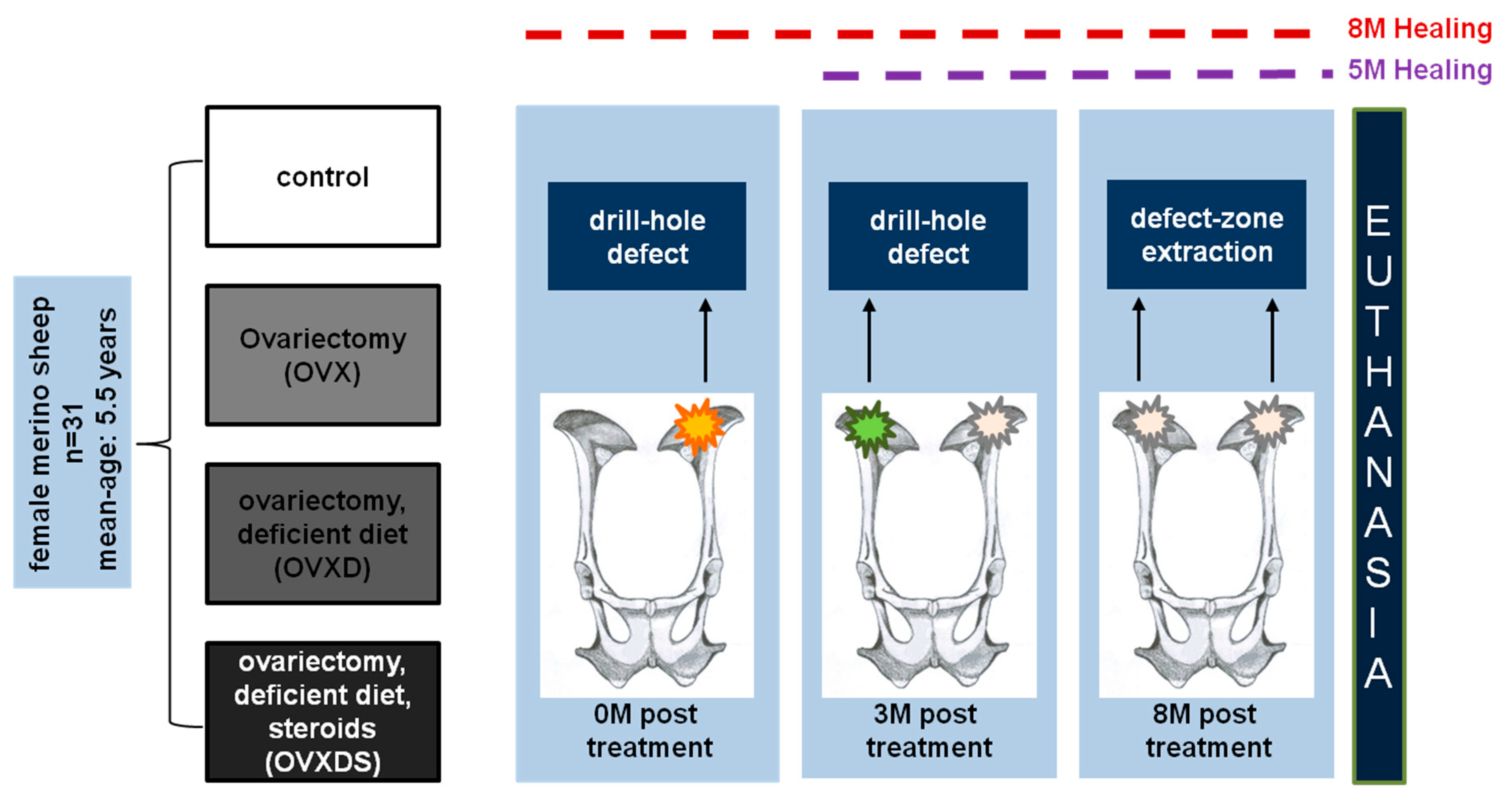
2.1. Experimental Design
2.2. Animal Diet
2.3. Steroid Administration
2.4. Dual Energy X-ray Absorptiometry (DXA)
2.5. Micro-Computed Tomography (µCT)
2.6. Fluorochrome Labelling
2.7. Sample Preparation and Histology
2.8. Image Capturing and Quantitative Evaluation
2.9. Ethical Statement
2.10. Statistical Analysis
3. Results
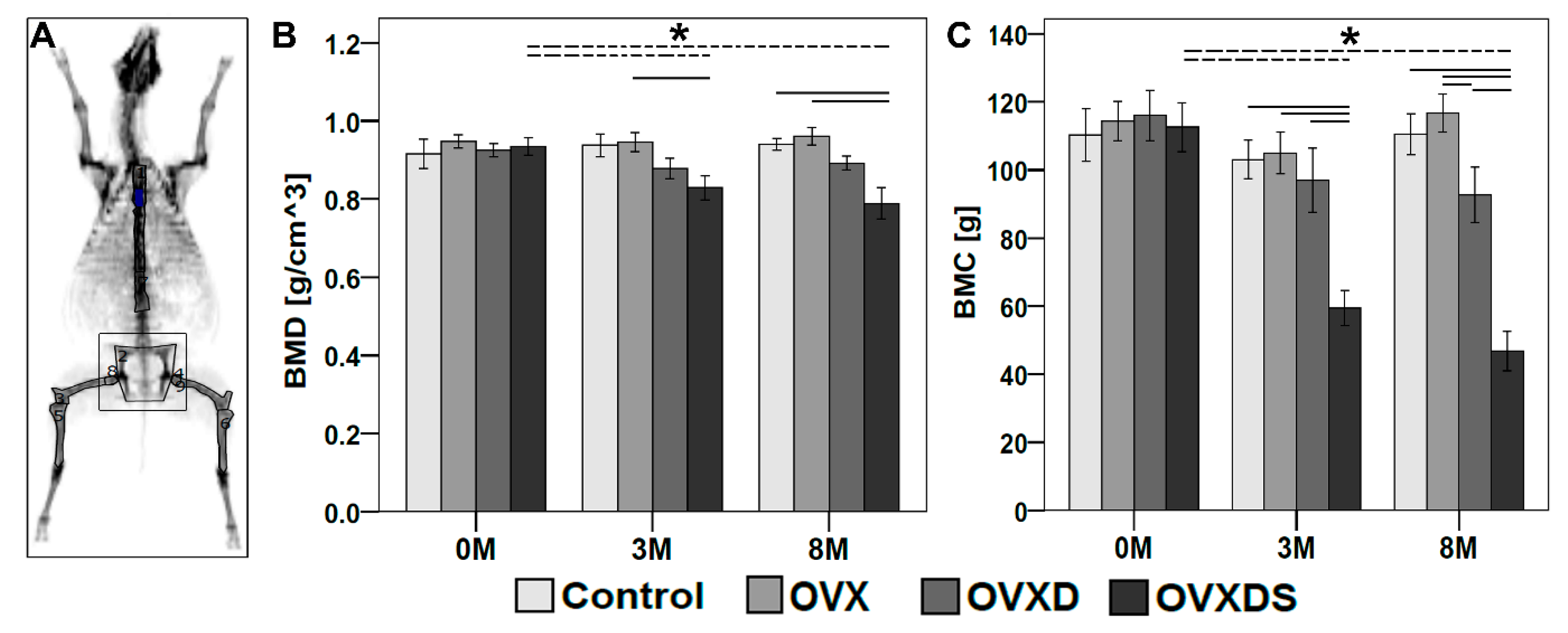
3.1. In Vivo DXA Measurements Showed Bone Loss in OVXDS at 8 M Post-Treatment
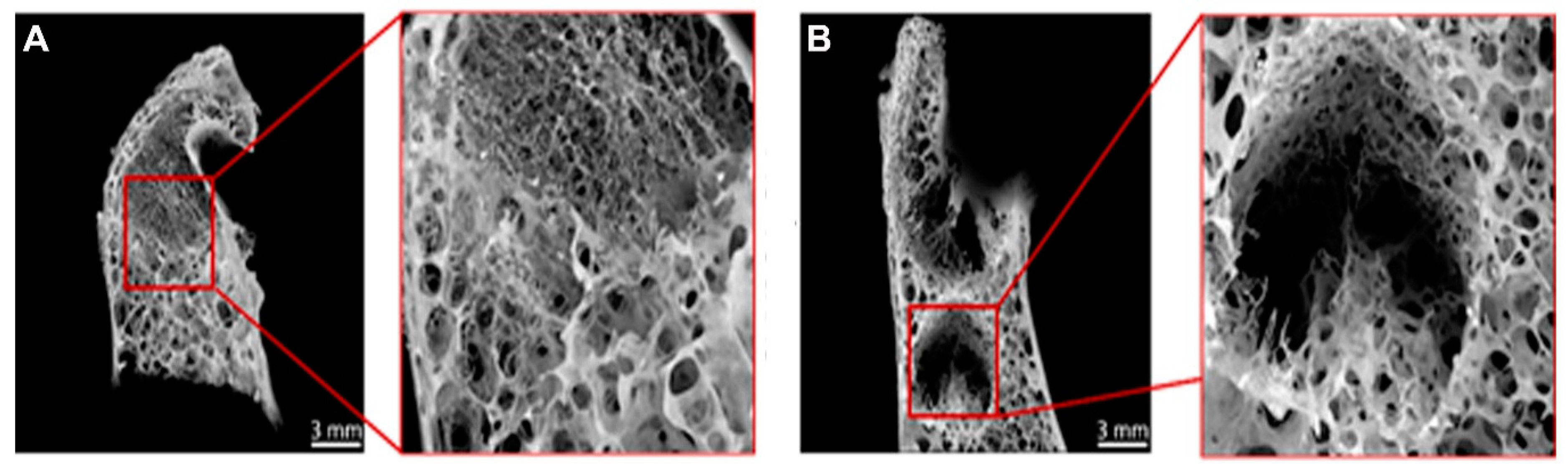
3.2. Radiological Testing Using µCT Showed Impaired Healing of Defect Zone in OVXDS after 8 M
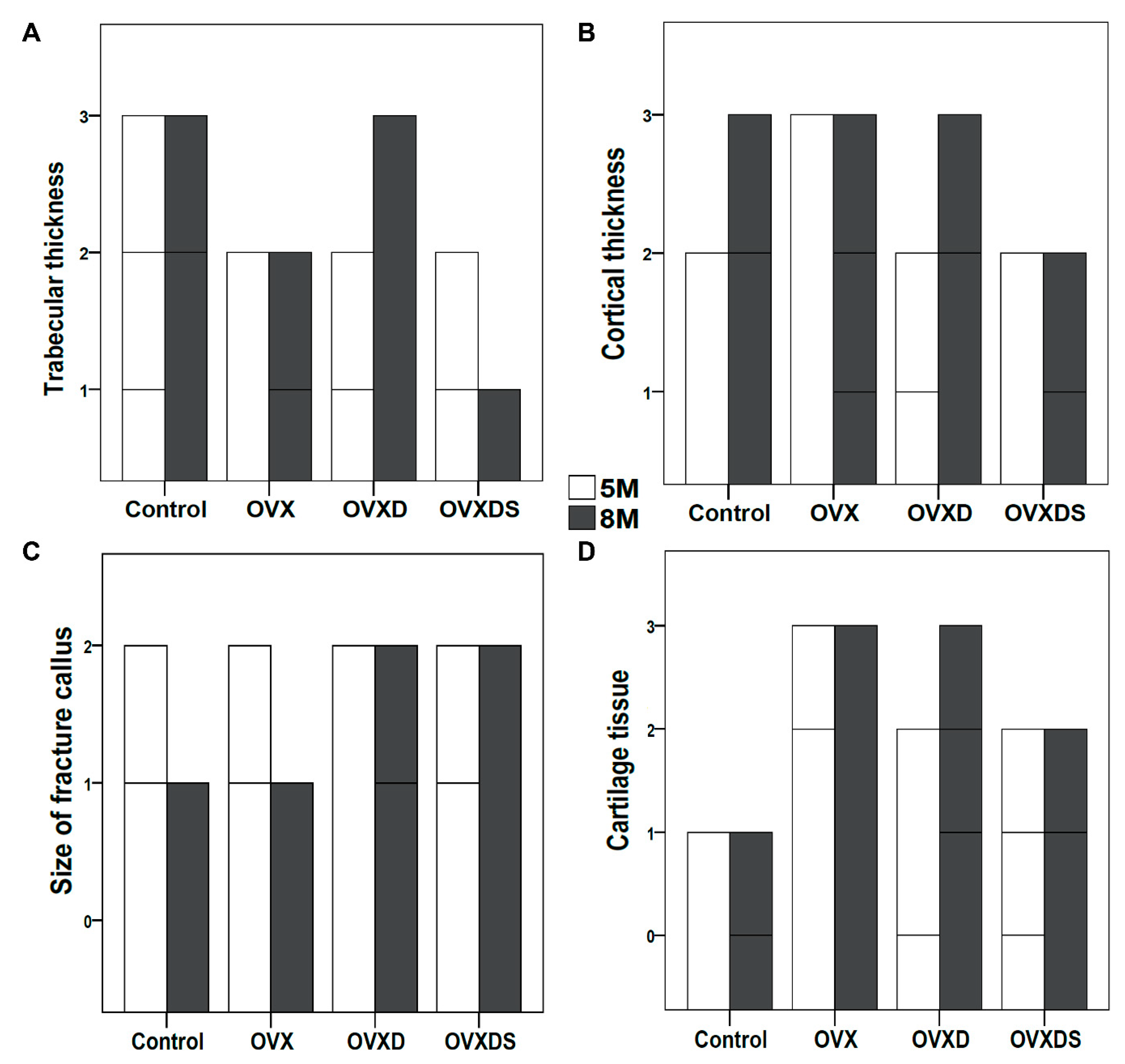
3.3. Impaired Healing in OVXDS Defect Zone Reflects Trabecular Thinning and Failed Fractured Callus Mineralization
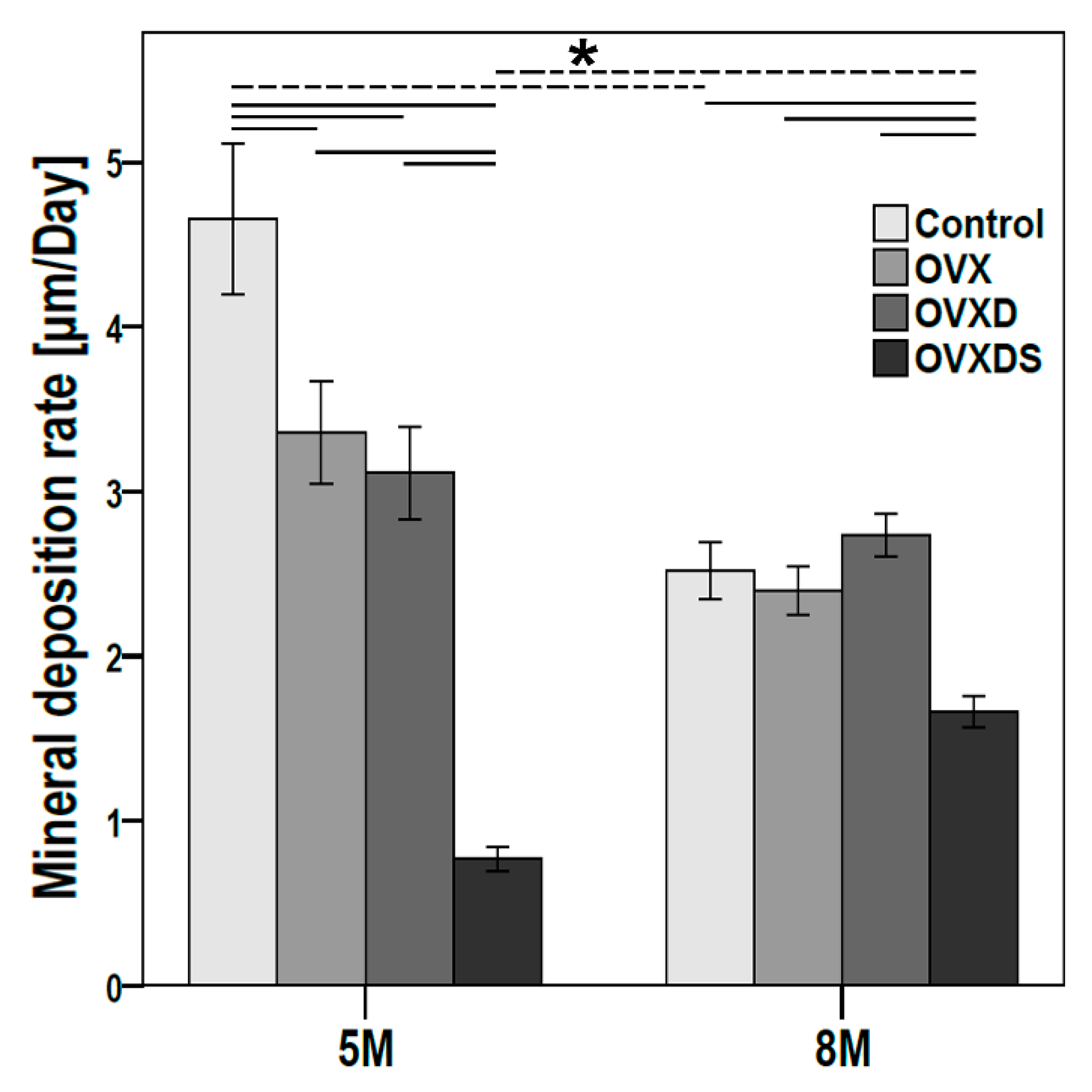
3.4. Deteriorated Bone Matrix Mineralization Seen in OVXDS Defect Zone after 8 M of Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ikeda, K. Osteocytes in the pathogenesis of osteoporosis. Geriatr. Gerontol. Int. 2008, 8, 213–217. [Google Scholar] [CrossRef]
- Corbiere, N.C.; Lewicki, K.A.; Issen, K.A.; Kuxhaus, L. Creating Physiologically Realistic Vertebral Fractures in a Cervine Model. J. Biomech. Eng. 2014, 136, 064504. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Rotter, R.; Pflugmacher, R.; Kandziora, F.; Ewert, A.; Duda, G.; Mittlmeier, T. Biomechanical In Vitro Testing of Human Osteoporotic Lumbar Vertebrae Following Prophylactic Kyphoplasty with Different Candidate Materials. Spine 2007, 32, 1400–1405. [Google Scholar] [CrossRef]
- Mundy, G.; Garrett, R.; Harris, S.; Chan, J.; Chen, D.; Rossini, G.; Boyce, B.; Zhao, M.; Gutierrez, G. Stimulation of Bone Formation in Vitro and in Rodents by Statins. Science 1999, 286, 1946–1949. [Google Scholar] [CrossRef] [PubMed]
- Fini, M.; Giavaresi, G.; Torricelli, P.; Krajewski, A.; Ravaglioli, A.; Belmonte, M.M.; Biagini, G.; Giardino, R. Biocompatibility and osseointegration in osteoporotic bone. J. Bone Jt. Surgery. Br. Vol. 2001, 83, 139–143. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, L.; Scott, P.G.; Tredget, E.E. Mesenchymal Stem Cells Enhance Wound Healing Through Differentiation and Angiogenesis. Stem Cells 2007, 25, 2648–2659. [Google Scholar] [CrossRef] [Green Version]
- Torricelli, P.; Fini, M.; Giavaresi, G.; Giardino, R. In vitroModels to Test Orthopedic Biomaterials in View of Their Clinical Application in Osteoporotic Bone. Int. J. Artif. Organs 2004, 27, 658–663. [Google Scholar] [CrossRef]
- El Khassawna, T.; Böcker, W.; Brodsky, K.; Weisweiler, D.; Govindarajan, P.; Kampschulte, M.; Thormann, U.; Henss, A.; Rohnke, M.; Bauer, N.; et al. Impaired extracellular matrix structure resulting from malnutrition in ovariectomized mature rats. Histochem. Cell Biol. 2015, 144, 491–507. [Google Scholar] [CrossRef]
- El Khassawna, T.; Böcker, W.; Govindarajan, P.; Schliefke, N.; Hürter, B.; Kampschulte, M.; Schlewitz, G.; Alt, V.; Lips, K.S.; Faulenbach, M.; et al. Effects of Multi-Deficiencies-Diet on Bone Parameters of Peripheral Bone in Ovariectomized Mature Rat. PLoS ONE 2013, 8, e71665. [Google Scholar] [CrossRef]
- Heiss, C.; Govindarajan, P.; Schlewitz, G.; Hemdan, N.Y.; Schliefke, N.; Alt, V.; Thormann, U.; Lips, K.S.; Wenisch, S.; Langheinrich, A.C.; et al. Induction of osteoporosis with its influence on osteoporotic determinants and their interrelationships in rats by DEXA. Med. Sci. Monit. 2012, 18, BR199–BR207. [Google Scholar] [CrossRef] [PubMed]
- Egermann, M.; Goldhahn, J.; Schneider, E. Animal models for fracture treatment in osteoporosis. Osteoporos. Int. 2005, 16, S129–S138. [Google Scholar] [CrossRef]
- Ameye, L.; Young, M.F. Mice deficient in small leucine-rich proteoglycans: Novel in vivo models for osteoporosis, osteoarthritis, Ehlers-Danlos syndrome, muscular dystrophy, and corneal diseases. Glycobiology 2002, 12, 107R–116R. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.S. Animal models of osteoporosis-necessity and limitations. Eur. Cells Mater. 2001, 1, 66–81. [Google Scholar] [CrossRef]
- Martini, L.; Fini, M.; Giavaresi, G.; Giardino, R. Sheep model in orthopedic research: A literature review. Comp. Med. 2001, 51, 292–299. [Google Scholar]
- Egermann, M.; Goldhahn, J.; Holz, R.; Schneider, E.; A Lill, C. A sheep model for fracture treatment in osteoporosis: Benefits of the model versus animal welfare. Lab. Anim. 2008, 42, 453–464. [Google Scholar] [CrossRef] [Green Version]
- Maissen, O.; Eckhardt, C.; Gogolewski, S.; Glatt, M.; Arvinte, T.; Steiner, A.; Rahn, B.; Schlegel, U. Mechanical and radiological assessment of the influence of rhTGFβ-3 on bone regeneration in a segmental defect in the ovine tibia: Pilot study. J. Orthop. Res. 2006, 24, 1670–1678. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.L.; Zhu, X.S.; Chen, L.; Chen, C.M.; Mangham, D.C.; Coulton, L.A.; Aiken, S.S. Bone healing response to a synthetic calcium sulfate/β-tricalcium phosphate graft material in a sheep vertebral body defect model. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100, 1911–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, H.; Turner, A.S.; Seim, H.B.; Kawamoto, T.; Bauer, T.W. Evaluation of a silica-containing bone graft substitute in a vertebral defect model. J. Biomed. Mater. Res. Part A 2009, 92, 596–603. [Google Scholar] [CrossRef]
- El Khassawna, T.; Merboth, F.; Malhan, D.; Böcker, W.; Daghma, D.E.; Stoetzel, S.; Kern, S.; Hassan, F.; Rosenbaum, D.; Langenstein, J. Osteocyte Regulation of Receptor Activator of NF-κB Ligand/Osteoprotegerin in a Sheep Model of Osteoporosis. Am. J. Pathol. 2017, 187, 1686–1699. [Google Scholar] [CrossRef] [Green Version]
- Liebsch, M.; Grune, B.; Seiler, A.; Butzke, D.; Oelgeschläger, M.; Pirow, R.; Adler, S.; Riebeling, C.; Luch, A. Alternatives to animal testing: Current status and future perspectives. Arch. Toxicol. 2011, 85, 841–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, A.; Pelletier, M.H.; Yu, Y.; Christou, C.; Walsh, W.R. A Sheep Model for Cancellous Bone Healing. Front. Surg. 2014, 1, 37. [Google Scholar] [CrossRef] [Green Version]
- Bindl, R.; Oheim, R.; Pogoda, P.; Beil, F.T.; Gruchenberg, K.; Reitmaier, S.; Wehner, T.; Calcia, E.; Radermacher, P.; Claes, L.; et al. Metaphyseal fracture healing in a sheep model of low turnover osteoporosis induced by hypothalamic-pituitary disconnection (HPD). J. Orthop. Res. 2013, 31, 1851–1857. [Google Scholar] [CrossRef]
- Claes, L.; Veeser, A.; Göckelmann, M.; Simon, U.; Ignatius, A. A novel model to study metaphyseal bone healing under defined biomechanical conditions. Arch. Orthop. Trauma Surg. 2009, 129, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Vasquez, S.X.; Shah, N.; Hoberman, A.M. Small Animal Imaging and Examination by Micro-CT. Adv. Struct. Saf. Stud. 2012, 947, 223–231. [Google Scholar] [CrossRef]
- Ding, M.; Odgaard, A.; Hvid, I. Accuracy of cancellous bone volume fraction measured by micro-CT scanning. J. Biomech. 1999, 32, 323–326. [Google Scholar] [CrossRef]
- Bergholt, N.L.; Lysdahl, H.; Lind, M.; Foldager, C.B. A Standardized Method of Applying Toluidine Blue Metachromatic Staining for Assessment of Chondrogenesis. Cartilage 2018, 10, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Martin, T.J.; Sims, N.A. RANKL/OPG; Critical role in bone physiology. Rev. Endocr. Metab. Disord. 2015, 16, 131–139. [Google Scholar] [CrossRef]
- Sridharan, G.; A Shankar, A. Toluidine blue: A review of its chemistry and clinical utility. J. Oral Maxillofac. Pathol. 2012, 16, 251–255. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-S.; Paik, I.-Y.; Rhie, Y.-J.; Suh, S.-H. Integrative Physiology: Defined Novel Metabolic Roles of Osteocalcin. J. Korean Med. Sci. 2010, 25, 985–991. [Google Scholar] [CrossRef] [Green Version]
- Jansen, J.P.; Bergman, G.J.D.; Huels, J.; Olson, M. Prevention of vertebral fractures in osteoporosis: Mixed treatment comparison of bisphosphonate therapies. Curr. Med Res. Opin. 2009, 25, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Martens, M.G. Risk of fracture and treatment to prevent osteoporosis-related fracture in postmenopausal women. A review. J. Reprod. Med. 2003, 48, 425–434. [Google Scholar]
- Chesnut, C.H.; Silverman, S.; Andriano, K.; Genant, H.; Gimona, A.; Harris, S.; Kiel, D.; LeBoff, M.; Maricic, M.; Miller, P.; et al. A randomized trial of nasal spray salmon calcitonin in postmenopausal women with established osteoporosis: The prevent recurrence of osteoporotic fractures study. Am. J. Med. 2000, 109, 267–276. [Google Scholar] [CrossRef]
- Shapiro, F. Bone development and its relation to fracture repair. The role of mesenchymal osteoblasts and surface osteoblasts. Eur. Cells Mater. 2008, 15, 53–76. [Google Scholar] [CrossRef]
- Chen, X.; Kidder, L.S.; Lew, W.D. Osteogenic protein-1 induced bone formation in an infected segmental defect in the rat femur. J. Orthop. Res. 2002, 20, 142–150. [Google Scholar] [CrossRef]
- Wong, R.M.Y.; Choy, M.H.V.; Li, M.C.M.; Leung, K.-S.; Chow, S.K.-H.; Cheung, W.-H.; Cheng, J.C.Y. A systematic review of current osteoporotic metaphyseal fracture animal models. Bone Jt. Res. 2018, 7, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Oheim, R.; Amling, M.; Ignatius, A.; Pogoda, P. Large animal model for osteoporosis in humans: The ewe. Eur. Cells Mater. 2012, 24, 372–385. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, S. The Sheep as an Experimental Model for Osteoporosis; The University of Melbourne: Melbourne, Australia, 1999. [Google Scholar]
- Kiełbowicz, Z.; Piątek, A.; Bieżyński, J.; Skrzypczak, P.; Kuropka, P.; Kuryszko, J.; Nikodem, A.; Kafarski, P.; Pezowicz, C. The experimental osteoporosis in sheep–clinical approach. Pol. J. Veter. Sci. 2015, 18, 645–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- den Boer, F.C.; Patka, P.; Bakker, F.C.; Wippermann, B.W.; van Lingen, A.; Vink, G.Q.; Boshuizen, K.; Haarman, H.J. New segmental long bone defect model in sheep: Quantitative analysis of healing with dual energy x-ray absorptiometry. J. Orthop. Res. 1999, 17, 654–660. [Google Scholar] [CrossRef]
- Turner, A.; Alvis, M.; Myers, W.; Stevens, M.; Lundy, M. Changes in bone mineral density and bone-specific alkaline phosphatase in ovariectomized ewes. Bone 1995, 17, S395–S402. [Google Scholar] [CrossRef]
- Turner, A.S. The sheep as a model for osteoporosis in humans. Vet. J. 2002, 163, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Russell, W.M.S.; Burch, R.L.; Hume, C.W. The Principles of Humane Experimental Technique, 1st ed.; Methuen and Co LTD: London, UK, 1959. [Google Scholar]
- Schmitz, J.P.; Hollinger, J.O. The Critical Size Defect as an Experimental Model for Craniomaxillofacial Nonunions; Walter Reed Army Medical Center: Washington, DC, USA, 1985. [Google Scholar]
- Hollinger, J.O.; Kleinschmidt, J.C. The Critical Size Defect as an Experimental Model to Test Bone Repair Materials. J. Craniofacial Surg. 1990, 1, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Claes, L.E.; Cunningham, J.L. Monitoring the mechanical properties of healing bone. Clin. Orthop. Relat. Res. 2009, 467, 1964–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschler, A.; Röpenack, P.; Herlyn, P.K.; Roesner, J.; Pille, K.; Büsing, K.; Vollmar, B.; Mittlmeier, T.; Gradl, G. The standardized creation of a lumbar spine vertebral compression fracture in a sheep osteoporosis model induced by ovariectomy, corticosteroid therapy and calcium/phosphorus/vitamin D-deficient diet. Injury 2015, 46, S17–S23. [Google Scholar] [CrossRef]
- Gómez-Barrena, E.; Rosset, P.; Lozano, D.; Stanovici, J.; Ermthaller, C.; Gerbhard, F. Bone fracture healing: Cell therapy in delayed unions and nonunions. Bone 2015, 70, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negrete-Corona, J.; Alvarado-Soriano, J.C.; A Reyes-Santiago, L. Hip fracture as risk factor for mortality in patients over 65 years of age. Case-control study. Acta Ortop. Mex. 2015, 28, 352–362. [Google Scholar]
- Giannoudis, P.; Tzioupis, C.; Almalki, T.; Buckley, R. Fracture healing in osteoporotic fractures: Is it really different? Injury 2007, 38, S90–S99. [Google Scholar] [CrossRef]
- Thormann, U.; El Khawassna, T.; Ray, S.; Duerselen, L.; Kampschulte, M.; Lips, K.; von Dewitz, H.; Heinemann, S.; Heiss, C.; Szalay, G.; et al. Differences of bone healing in metaphyseal defect fractures between osteoporotic and physiological bone in rats. Injury 2014, 45, 487–493. [Google Scholar] [CrossRef]
- Decambron, A.; Manassero, M.; Bensidhoum, M.; Lecuelle, B.; Logeart-Avramoglou, D.; Petite, H.; Viateau, V. A comparative study of tissue-engineered constructs from Acropora and Porites coral in a large animal bone defect model. Bone Jt. Res. 2017, 6, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Christou, C.; Oliver, A.R.; Pelletier, M.H.; Walsh, W.R. Ovine Model for Critical-Size Tibial Segmental Defects. Comp. Med. 2014, 64, 377–385. [Google Scholar]
- Anderson, M.L.; Dhert, W.J.; de Bruijn, J.D.; Dalmeijer, R.A.; Leenders, H.; van Blitterswijk, C.A.; Verbout, A.J. Critical Size Defect in the Goat’s Os Ilium: A Model to Evaluate Bone Grafts and Substitutes. Clin. Orthop. Relat. Res. 1999, 364, 231–239. [Google Scholar] [CrossRef]
- Lansdowne, J.L.; Devine, D.; Eberli, U.; Emans, P.; Welting, T.J.M.; Odekerken, J.C.E.; Schiuma, D.; Thalhauser, M.; Bouré, L.; Zeiter, S. Characterization of an Ovine Bilateral Critical Sized Bone Defect Iliac Wing Model to Examine Treatment Modalities Based on Bone Tissue Engineering. BioMed Res. Int. 2014, 2014, 250958. [Google Scholar] [CrossRef] [PubMed]
- Pobloth, A.-M.; Johnson, K.A.; Schell, H.; Kolarczik, N.; Wulsten, D.; Duda, G.N.; Schmidt-Bleek, K. Establishment of a preclinical ovine screening model for the investigation of bone tissue engineering strategies in cancellous and cortical bone defects. BMC Musculoskelet. Disord. 2016, 17, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Claes, L.E.; Heigele, C.A.; Neidlinger-Wilke, C.; Kaspar, D.; Seidl, W.; Margevicius, K.J.; Augat, P. Effects of mechanical factors on the fracture healing process. Clin. Orthop. Relat. Res. 1998, 355, S132–S147. [Google Scholar] [CrossRef] [PubMed]
- Swart, E.; Bezhani, H.; Greisberg, J.; Vosseller, J.T. How long should patients be kept non-weight bearing after ankle fracture fixation? A survey of OTA and AOFAS members. Injury 2015, 46, 1127–1130. [Google Scholar] [CrossRef]
- Augat, P.; Merk, J.; Ignatius, A.; Margevicius, K.; Bauer, G.; Rosenbaum, D.; Claes, L. Early, full weightbearing with flexible fixation delays fracture healing. Clin. Orthop. Relat. Res. 1996, 328, 194–202. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rupp, M.; Biehl, C.; Malhan, D.; Hassan, F.; Attia, S.; Rosch, S.; Schäfer, A.B.; McMahon, E.; Kampschulte, M.; Heiss, C.; et al. Large Animal Model of Osteoporotic Defect Healing: An Alternative to Metaphyseal Defect Model. Life 2021, 11, 254. https://doi.org/10.3390/life11030254
Rupp M, Biehl C, Malhan D, Hassan F, Attia S, Rosch S, Schäfer AB, McMahon E, Kampschulte M, Heiss C, et al. Large Animal Model of Osteoporotic Defect Healing: An Alternative to Metaphyseal Defect Model. Life. 2021; 11(3):254. https://doi.org/10.3390/life11030254
Chicago/Turabian StyleRupp, Markus, Christoph Biehl, Deeksha Malhan, Fathi Hassan, Sameh Attia, Sebastian Rosch, Annemarie B. Schäfer, Erin McMahon, Marian Kampschulte, Christian Heiss, and et al. 2021. "Large Animal Model of Osteoporotic Defect Healing: An Alternative to Metaphyseal Defect Model" Life 11, no. 3: 254. https://doi.org/10.3390/life11030254