
Postoperative Complications Are Associated with Long-Term Changes in the Gut Microbiota Following Colorectal Cancer Surgery

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Collection and Storage of Stool Samples
2.3. Microbiota Analysis
2.4. Diatery Patterns
2.5. Statistical Analysis
3. Results
3.1. Cohort Demographics and Clinical Differences
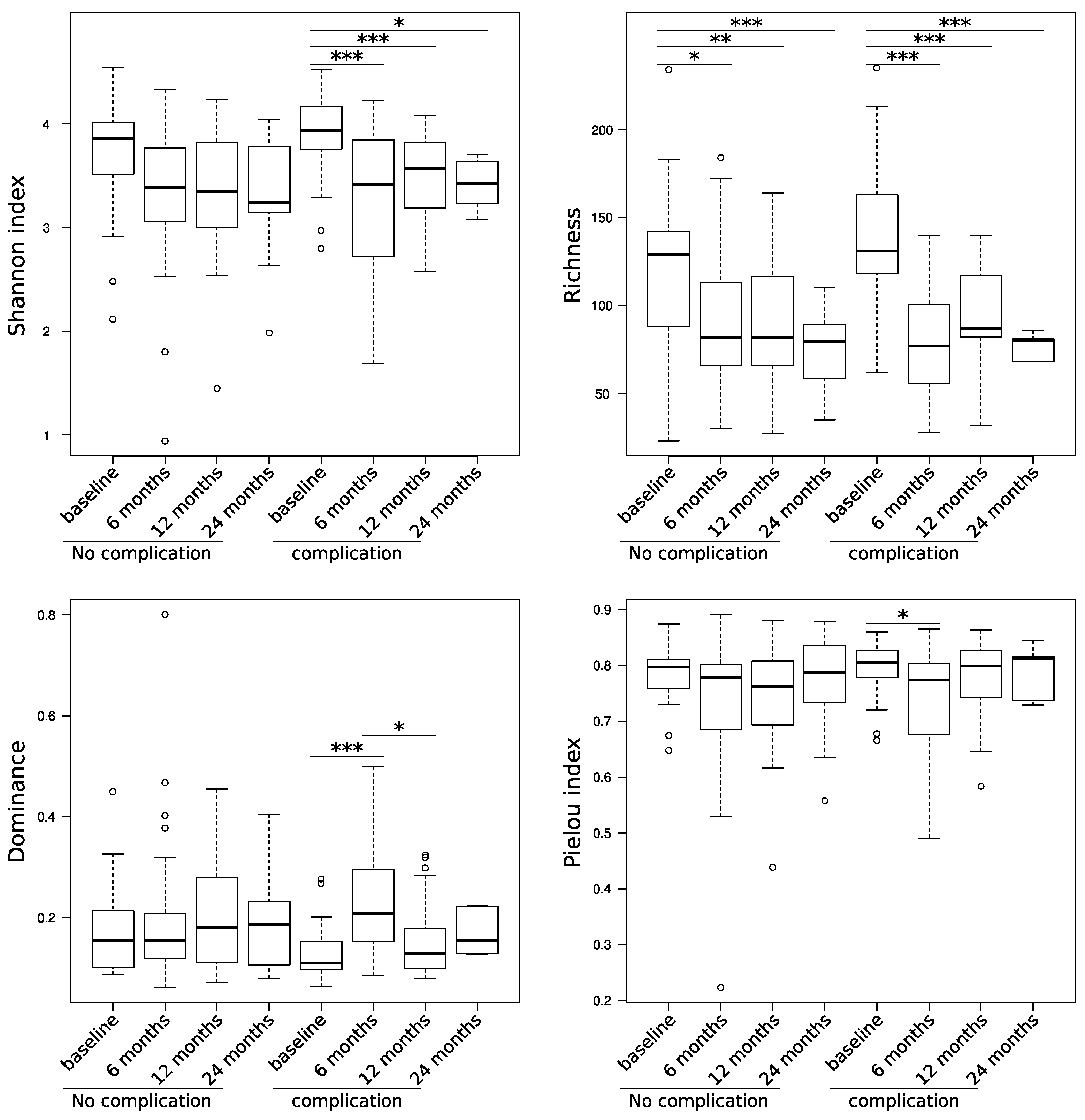
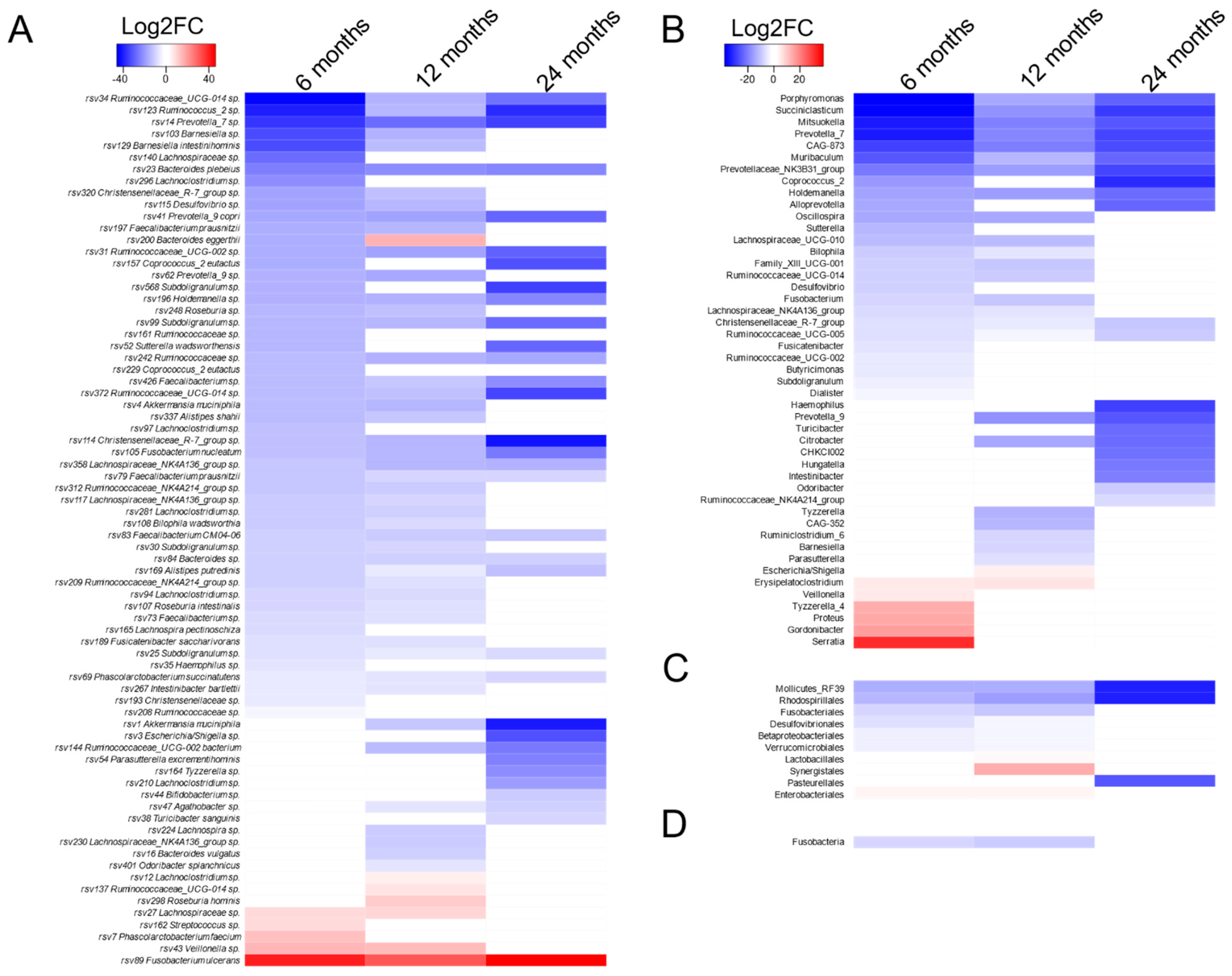
3.2. Associations between Complication and the Microbiota Structure
3.3. Dietary Patterns and BMI
3.4. Tumor Stage and Chemotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Codner, P.A.; Herron, T.J. The shifting microbiome in surgical stress. Curr. Surg. Rep. 2017, 9, 4–5. [Google Scholar] [CrossRef]
- Kamada, N.; Seo, S.-U.; Chen, G.Y.; Núñez, G. Role of the gut microbiota in immunity and inflammatory disease. Nat. Rev. Immunol. 2013, 13, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Ley, R.E.; Turnbaugh, P.J.; Klein, S.; Gordon, J.I. Microbial ecology: Human gut microbes associated with obesity. Nature 2006, 444, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Marteau, P.; Lepage, P.; Mangin, I.; Suau, A.; Dore, J.; Pochart, P.; Seksik, P. Review article: Gut flora and inflammatory bowel disease. Aliment Pharmacol. Ther. 2004, 20, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, F.; Lipinski, A.; Hofer, S.; Uhle, F.; Nusshag, C.; Hackert, T.; Dalpke, A.; Weigand, M.; Brenner, T.; Boutin, S. Pulmonary microbiome patterns correlate with the course of disease in patients with sepsis-induced ARDS following major abdominal surgery. J. Hosp. Infect. 2020, 105, 438–446. [Google Scholar] [CrossRef]
- Bartolini, I.; Risaliti, M.; Ringressi, M.N.; Melli, F.; Nannini, G.; Amedei, A.; Muiesan, P.; Taddei, A. Role of gut microbiota-immunity axis in patients undergoing surgery for colorectal cancer: Focus on short and long-term outcomes. World, J. Gastroenterol. 2020, 26, 2498–2513. [Google Scholar] [CrossRef]
- Koliarakis, I.; Athanasakis, E.; Sgantzos, M.; Mariolis-Sapsakos, T.; Xynos, E.; Chrysos, E.; Souglakos, J.; Tsiaoussis, J. Intestinal Microbiota in Colorectal Cancer Surgery. Cancers 2020, 12, 3011. [Google Scholar] [CrossRef]
- Lankelma, J.M.; Van Vught, L.A.; Belzer, C.; Schultz, M.J.; Van Der Poll, T.; De Vos, W.M.; Wiersinga, W.J. Critically ill patients demonstrate large interpersonal variation in intestinal microbiota dysregulation: A pilot study. Intensiv. Care Med. 2017, 43, 59–68. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, F.C.F.; Brenner, T.; Uhle, F.; Loesch, S.; Hackert, T.; Ulrich, A.; Hofer, S.; Dalpke, A.H.; Weigand, M.A.; Boutin, S. Gut microbiome patterns correlate with higher postoperative complication rates after pancreatic surgery. BMC Microbiol. 2019, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Pamer, E.G. Resurrecting the intestinal microbiota to combat antibiotic-resistant pathogens. Science 2016, 352, 535–538. [Google Scholar] [CrossRef] [Green Version]
- Blaser, M.J. Antibiotic use and its consequences for the normal microbiome. Science 2016, 352, 544–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ianiro, G.; Tilg, H.; Gasbarrini, A. Antibiotics as deep modulators of gut microbiota: Between good and evil. Gut 2016, 65, 1906–1915. [Google Scholar] [CrossRef]
- Ulrich, C.M.; Gigic, B.; Böhm, J.; Ose, J.; Viskochil, R.; Schneider, M.; Colditz, G.A.; Figueiredo, J.C.; Grady, W.M.; Li, C.I.; et al. The ColoCare Study: A Paradigm of Transdisciplinary Science in Colorectal Cancer Outcomes. Cancer Epidemiol. Biomark. Prev. 2019, 28, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gigic, B.; Boeing, H.; Toth, R.; Böhm, J.; Habermann, N.; Scherer, D. Associations Between Dietary Patterns and Longitudinal Quality of Life Changes in Colorectal Cancer Pa-tients: The ColoCare Study. Nutr. Cancer 2018, 70, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Pettigrew, M.M.; Gent, J.F.; Kong, Y.; Halpin, A.L.; Pineles, L.; Harris, A.D.; Johnson, J.K. Gastrointestinal Microbiota Disruption and Risk of Colonization With Carbapenem-resistant Pseudomonas aeruginosa in Intensive Care Unit Patients. Clin. Infect. Dis. 2019, 69, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Aardema, H.; Lisotto, P.; Kurilshikov, A.; Diepeveen, J.R.J.; Friedrich, A.W.; Sinha, B.; De Smet, A.M.G.A.; Harmsen, H.J.M. Marked Changes in Gut Microbiota in Cardio-Surgical Intensive Care Patients: A Longitudinal Cohort Study. Front. Cell. Infect. Microbiol. 2020, 9, 467. [Google Scholar] [CrossRef] [Green Version]
- McDonald, D.; Ackermann, G.; Khailova, L.; Baird, C.; Heyland, D.; Kozar, R.; Lemieux, M.; Derenski, K.; King, J.; Vis-Kampen, C.; et al. Extreme Dysbiosis of the Microbiome in Critical Illness. mSphere 2016, 1. [Google Scholar] [CrossRef] [Green Version]
- Ojima, M.; Motooka, D.; Shimizu, K.; Gotoh, K.; Shintani, A.; Yoshiya, K.; Nakamura, S.; Ogura, H.; Iida, T.; Shimazu, T. Metagenomic Analysis Reveals Dynamic Changes of Whole Gut Microbiota in the Acute Phase of Intensive Care Unit Patients. Dig. Dis. Sci. 2016, 61, 1628–1634. [Google Scholar] [CrossRef] [Green Version]
- Zaborin, A.; Smith, D.; Garfield, K.; Quensen, J.; Shakhsheer, B.; Kade, M. Membership and behavior of ultra-low-diversity pathogen communities present in the gut of humans during pro-longed critical illness. mBio 2014, 5, e01361-14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brahe, L.K.; Le Chatelier, E.; Prifti, E.; Pons, N.; Kennedy, S.; Blaedel, T.; Håkansson, J.; Dalsgaard, T.K.; Hansen, T.; Pedersen, O.; et al. Dietary modulation of the gut microbiota—A randomised controlled trial in obese postmenopausal women. Br. J. Nutr. 2015, 114, 406–417. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, T.; Ishikawa, H.; Tateda, K.; Yaeshima, T.; Ishibashi, N.; Yamaguchi, K. Oral administration of Bifidobacterium longum prevents gut-derived Pseudomonas aeruginosa sepsis in mice. J. Appl. Microbiol. 2008, 104, 672–680. [Google Scholar] [CrossRef]
- Buffie, C.G.; Bucci, V.; Stein, R.R.; McKenney, P.T.; Ling, L.; Gobourne, A.; No, D.; Liu, H.; Kinnebrew, M.; Viale, A.; et al. Precision microbiome reconstitution restores bile acid mediated resistance to Clostridium difficile. Nat. Cell Biol. 2015, 517, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Adriaans, B.; Shah, H. Fusobacterium ulcerans sp. nov. from Tropical Ulcers. Int. J. Syst. Bacteriol. 1988, 38, 447–448. [Google Scholar] [CrossRef]
- Claros, M.C.; Papke, Y.; Kleinkauf, N.; Adler, D.; Citron, D.M.; Hunt-Gerardo, S. Characteristics of Fusobacterium ulcerans, a new and unusual species compared with Fusobacterium varium and Fusobacterium mortiferum. Anaerobe 1999, 5, 137–140. [Google Scholar] [CrossRef]
- Citron, D.M. Update on the Taxonomy and Clinical Aspects of the GenusFusobacterium. Clin. Infect. Dis. 2002, 35, S22–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miniet, A.A.; Grunwell, J.R.; Coopersmith, C.M. The microbiome and the immune system in critical illness. Curr. Opin. Crit. Care 2021, 27, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Krezalek, M.A.; DeFazio, J.; Zaborina, O.; Zaborin, A.; Alverdy, J.C. The Shift of an Intestinal “Microbiome” to a “Pathobiome” Governs the Course and Outcome of Sepsis Following Surgical Injury. Shock 2016, 45, 475–482. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Yang, Y.; Wang, H.; Wang, H.; Yu, X.; Lu, Y.; Shen, S.; Teng, L. Gut microbiota shifts in patients with gastric cancer in perioperative period. Medicine 2019, 98, e16626. [Google Scholar] [CrossRef]
- Van Passel, M.W.; Kant, R.; Zoetendal, E.G.; Plugge, C.M.; Derrien, M.; Malfatti, S.A. The genome of Akkermansia muciniphila, a dedicated intestinal mucin degrader, and its use in exploring intes-tinal metagenomes. PLoS ONE 2011, 6, e16876. [Google Scholar]
- Borchers, M.T.; Carty, M.P.; Leikauf, G.D. Regulation of human airway mucins by acrolein and inflammatory mediators. Am. J. Physiol. Content 1999, 276, L549–L555. [Google Scholar] [CrossRef]
- Moal, V.L.-L.; Servin, A.L. Anti-Infective Activities of Lactobacillus Strains in the Human Intestinal Microbiota: From Probiotics to Gastrointestinal Anti-Infectious Biotherapeutic Agents. Clin. Microbiol. Rev. 2014, 27, 167–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derrien, M.; Van Baarlen, P.; Hooiveld, G.; Norin, E.; Müller, M.; De Vos, W.M. Modulation of Mucosal Immune Response, Tolerance, and Proliferation in Mice Colonized by the Mucin-Degrader Akkermansia muciniphila. Front. Microbiol. 2011, 2, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reunanen, J.; Kainulainen, V.; Huuskonen, L.; Ottman, N.; Belzer, C.; Huhtinen, H.; De Vos, W.M.; Satokari, R. Akkermansia muciniphila Adheres to Enterocytes and Strengthens the Integrity of the Epithelial Cell Layer. Appl. Environ. Microbiol. 2015, 81, 3655–3662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blander, J.M.; Longman, R.S.; Iliev, I.D.; Sonnenberg, G.F.; Artis, D. Regulation of inflammation by microbiota interactions with the host. Nat. Immunol. 2017, 18, 851–860. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients’ Characteristics | |
|---|---|
| Age (years) | 64 (54.3–72.8) |
| Gender | |
| Female | 34 (54.8%) |
| Male | 28 (45.2%) |
| Body Mass Index | 26.4 (24.3–30.0) |
| Site of Surgery | |
| Colon | 27 (58.7%) |
| Rectum | 35 (41.3%) |
| Chemotherapy | |
| Neo–Adjuvant | 15 (24.2%) |
| Adjuvant | 19 (30.6%) |
| Tumor Staging | |
| Carcinoma In Situ | 1 (1.6%) |
| Grade I | 12 (19.4%) |
| Grade II | 18 (29.0%) |
| Grade III | 17 (27.4%) |
| Grade IV | 14 (22.6%) |
| Complications (Number of Patients; Double Naming Feasible) | |
| Surgical | 22 (35.5%) |
| Medical | 20 (32.3%) |
| Both | 14 (22.6%) |
| Complication Grade (According to the Clavien–Dindo Classification) | |
| Grade I | 10 (16.1%) |
| Grade II | 11 (17.7%) |
| Grade III | 7 (11.3%) |
| Grade IV | 2 (3.2%) |
| Survivor (After 24-months) | 58 (93.5%) |
| Data are presented by median and interquartile range (Q1–Q3) or quantity and percentage. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmitt, F.C.F.; Schneider, M.; Mathejczyk, W.; Weigand, M.A.; Figueiredo, J.C.; Li, C.I.; Shibata, D.; Siegel, E.M.; Toriola, A.T.; Ulrich, C.M.; et al. Postoperative Complications Are Associated with Long-Term Changes in the Gut Microbiota Following Colorectal Cancer Surgery. Life 2021, 11, 246. https://doi.org/10.3390/life11030246
Schmitt FCF, Schneider M, Mathejczyk W, Weigand MA, Figueiredo JC, Li CI, Shibata D, Siegel EM, Toriola AT, Ulrich CM, et al. Postoperative Complications Are Associated with Long-Term Changes in the Gut Microbiota Following Colorectal Cancer Surgery. Life. 2021; 11(3):246. https://doi.org/10.3390/life11030246
Chicago/Turabian StyleSchmitt, Felix C. F., Martin Schneider, William Mathejczyk, Markus A. Weigand, Jane C. Figueiredo, Christopher I. Li, David Shibata, Erin M. Siegel, Adetunji T. Toriola, Cornelia M. Ulrich, and et al. 2021. "Postoperative Complications Are Associated with Long-Term Changes in the Gut Microbiota Following Colorectal Cancer Surgery" Life 11, no. 3: 246. https://doi.org/10.3390/life11030246