
Chondral and Soft Tissue Injuries Associated to Acute Patellar Dislocation: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Search Strategy
- Problem: first time patellar dislocation;
- Outcome: soft tissue injuries.
2.2. Literature Search
2.3. Eligibility Criteria
2.4. Outcomes of Interest
2.5. Methodology Quality Assessment
2.6. Statistical Analysis
3. Results
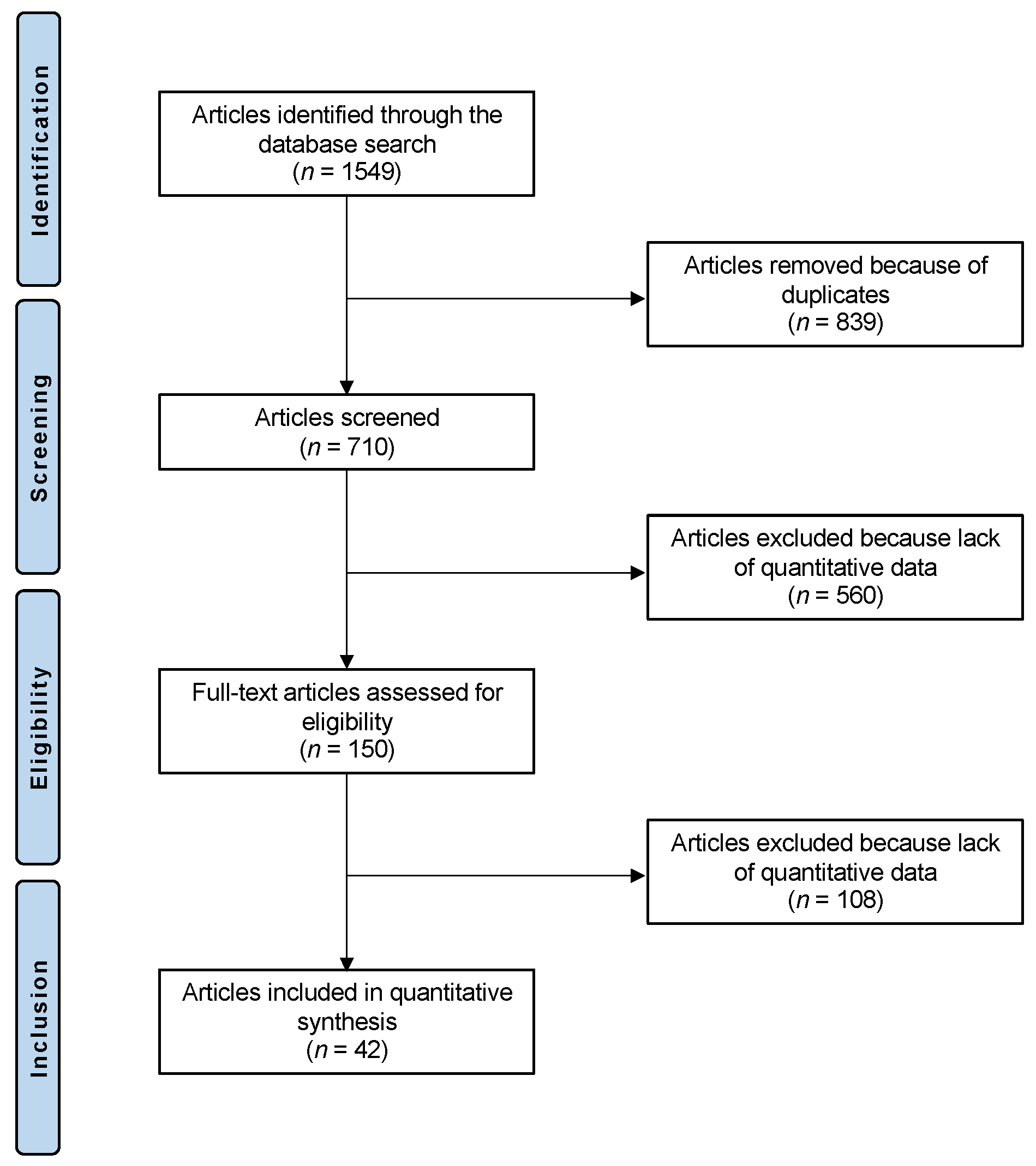
3.1. Search Result
3.2. Methodological Quality Assessment
3.3. Patient Demographics
3.4. MRI Findings
3.5. Arthroscopic Findings
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waterman, B.R.; Belmont, P.J., Jr.; Owens, B.D. Patellar dislocation in the United States: Role of sex, age, race, and athletic participation. J. Knee Surg. 2012, 25, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendt, E.A.; Fithian, D.C.; Cohen, E. Current concepts of lateral patella dislocation. Clin. Sports Med. 2002, 21, 499–519. [Google Scholar] [CrossRef]
- Hoetzel, J.; Preiss, A.; Heitmann, M.A.; Frosch, K.H. Knee injuries in children and adolescents. Eur. J. Trauma Emerg. Surg. 2014, 40, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Cash, J.D.; Hughston, J.C. Treatment of acute patellar dislocation. Am. J. Sports Med. 1988, 16, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.J.; Bell, R.H.; Anisette, G. Acute patellar dislocations. The natural history. Am. J. Sports Med. 1986, 14, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Aicale, R.; D’Addona, A.; Young, D.A.; Kader, D.F.; Oliva, F. Combined medial patellofemoral and patellotibial reconstruction with soft tissue fixation in recurrent patellar dislocation. Injury 2020, 51, 1867–1873. [Google Scholar] [CrossRef] [PubMed]
- Steensen, R.N.; Bentley, J.C.; Trinh, T.Q.; Backes, J.R.; Wiltfong, R.E. The prevalence and combined prevalences of anatomic factors associated with recurrent patellar dislocation: A magnetic resonance imaging study. Am. J. Sports Med. 2015, 43, 921–927. [Google Scholar] [CrossRef]
- Hiemstra, L.A.; Kerslake, S.; Lafave, M. Assessment of demographic and pathoanatomic risk factors in recurrent patellofemoral instability. Knee Surg. Sports Traumatol. Arthrosc. 2016, 25, 3849–3855. [Google Scholar] [CrossRef]
- Boling, M.C.; Padua, D.A.; Marshall, S.W.; Guskiewicz, K.; Pyne, S.; Beutler, A. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: The Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am. J. Sports Med. 2009, 37, 2108–2116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, D.; Pfalzer, F.; Hingelbaum, S.; Huth, J.; Mauch, F.; Bauer, G. The influence of risk factors on clinical outcomes following anatomical medial patellofemoral ligament (MPFL) reconstruction using the gracilis tendon. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 318–324. [Google Scholar] [CrossRef]
- Palmu, S.; Kallio, P.E.; Donell, S.T.; Helenius, I.; Nietosvaara, Y. Acute patellar dislocation in children and adolescents: A randomized clinical trial. J. Bone Jt. Surg. Am. 2008, 90, 463–470. [Google Scholar] [CrossRef]
- Beasley, L.S.; Vidal, A.F. Traumatic patellar dislocation in children and adolescents: Treatment update and literature review. Curr. Opin. Pediatr. 2004, 16, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Buchner, M.; Baudendistel, B.; Sabo, D.; Schmitt, H. Acute traumatic primary patellar dislocation: Long-term results comparing conservative and surgical treatment. Clin. J. Sport Med. 2005, 15, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, P.; Li, X.; Patel, K.; Brown, M.; Busconi, B. Medial patellofemoral ligament injury patterns and associated pathology in lateral patella dislocation: An MRI study. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2009, 1, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nomura, E.; Inoue, M.; Kurimura, M. Chondral and osteochondral injuries associated with acute patellar dislocation. Arthroscopy 2003, 19, 717–721. [Google Scholar] [CrossRef]
- Sanders, T.G.; Paruchuri, N.B.; Zlatkin, M.B. MRI of osteochondral defects of the lateral femoral condyle: Incidence and pattern of injury after transient lateral dislocation of the patella. AJR Am. J. Roentgenol. 2006, 187, 1332–1337. [Google Scholar] [CrossRef]
- Potter, H.G.; Linklater, J.M.; Allen, A.A.; Hannafin, J.A.; Haas, S.B. Magnetic resonance imaging of articular cartilage in the knee. An evaluation with use of fast-spin-echo imaging. J. Bone Jt. Surg. Am. 1998, 80, 1276–1284. [Google Scholar] [CrossRef]
- Martin, N.J.; Lustig, S.; Servien, E.; Mangiavini, L.; Luceri, F. Transosseous suture loop technique for MPFL reconstruction. J. Biol. Regul. Homeost. Agents 2020, 34, 133–138. [Google Scholar]
- Bauer, K.L. Osteochondral Injuries of the Knee in Pediatric Patients. J. Knee Surg. 2018, 31, 382–391. [Google Scholar] [CrossRef]
- Chotel, F.; Knorr, G.; Simian, E.; Dubrana, F.; Versier, G.; French Arthroscopy, S. Knee osteochondral fractures in skeletally immature patients: French multicenter study. Orthop. Traumatol. Surg. Res. 2011, 97, S154–S159. [Google Scholar] [CrossRef] [Green Version]
- Lording, T.; Lustig, S.; Servien, E.; Neyret, P. Chondral Injury in Patellofemoral Instability. Cartilage 2014, 5, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Migliorini, F.; Maffulli, N.; Eschweiler, J.; Quack, V.; Tingart, M.; Driessen, A. Lateral retinacular release combined with MPFL reconstruction for patellofemoral instability: A systematic review. Arch. Orthop. Trauma Surg. 2020, 142, 283–292. [Google Scholar] [CrossRef]
- Migliorini, F.; Baroncini, A.; Eschweiler, J.; Tingart, M.; Maffulli, N. Interference screws vs. suture anchors for isolated medial patellofemoral ligament femoral fixation: A systematic review. J. Sport Health Sci. 2020, in press. [Google Scholar] [CrossRef]
- Burnham, J.M.; Howard, J.S.; Hayes, C.B.; Lattermann, C. Medial Patellofemoral Ligament Reconstruction With Concomitant Tibial Tubercle Transfer: A Systematic Review of Outcomes and Complications. Arthroscopy 2016, 32, 1185–1195. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.M.; Joo, Y.B. Patellofemoral osteoarthritis. Knee Surg. Relat. Res. 2012, 24, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, D.; Metcalfe, A.; Wogan, C.; Mandalia, V.; Eldridge, J. Adolescent patellar instability: Current concepts review. Bone Jt. J. 2017, 99-B, 159–170. [Google Scholar] [CrossRef]
- Earl, J.E.; Hoch, A.Z. A proximal strengthening program improves pain, function, and biomechanics in women with patellofemoral pain syndrome. Am. J. Sports Med. 2011, 39, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Maenpaa, H.; Lehto, M.U. Patellar dislocation. The long-term results of nonoperative management in 100 patients. Am. J. Sports Med. 1997, 25, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Moiz, M.; Smith, N.; Smith, T.O.; Chawla, A.; Thompson, P.; Metcalfe, A. Clinical Outcomes After the Nonoperative Management of Lateral Patellar Dislocations: A Systematic Review. Orthop. J. Sports Med. 2018, 6, 2325967118766275. [Google Scholar] [CrossRef]
- Buchanan, G.; Torres, L.; Czarkowski, B.; Giangarra, C.E. Current Concepts in the Treatment of Gross Patellofemoral Instability. Int. J. Sports Phys. Ther. 2016, 11, 867–876. [Google Scholar]
- Migliorini, F.; Driessen, A.; Quack, V.; Gatz, M.; Tingart, M.; Eschweiler, J. Surgical versus conservative treatment for first patellofemoral dislocations: A meta-analysis of clinical trials. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 771–780. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howick, C.I., Jr.; Glasziou, P.; Greenhalgh, T.; Carl, H.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H.; Goddard, O.; Hodgkinson, M. The 2011 Oxford CEBM Levels of Evidence. Oxford Centre for Evidence-Based Medicine. 2011. Available online: https://www.cebm.net/index.aspx?o=5653 (accessed on 22 October 2021).
- Slattery, C.; Kweon, C.Y. Classifications in Brief: Outerbridge Classification of Chondral Lesions. Clin. Orthop. Relat. Res. 2018, 476, 2101–2104. [Google Scholar] [CrossRef]
- Paatela, T.; Vasara, A.; Nurmi, H.; Kautiainen, H.; Kiviranta, I. Assessment of Cartilage Repair Quality With the International Cartilage Repair Society Score and the Oswestry Arthroscopy Score. J. Orthop. Res. 2020, 38, 555–562. [Google Scholar] [CrossRef]
- Bui, K.L.; Ilaslan, H.; Parker, R.D.; Sundaram, M. Knee dislocations: A magnetic resonance imaging study correlated with clinical and operative findings. Skeletal Radiol. 2008, 37, 653–661. [Google Scholar] [CrossRef]
- Callewier, A.; Monsaert, A.; Lamraski, G. Lateral femoral condyle osteochondral fracture combined to patellar dislocation: A case report. Orthop. Traumatol. Surg. Res. 2009, 95, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Cavalheiro, C.M.; Gobbi, R.G.; Hinckel, B.B.; Demange, M.K.; Pecora, J.R.; Camanho, G.L. Femoral condyle osteochondral fracture treated with bone suture after acute patellar dislocation: A case report. Rev. Bras. Ortop. 2018, 53, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.C.; Haun, D.W.; Morrell, A.P.; Kettner, N.W. Patellar dislocation in a 16-year-old athlete with femoral trochlear dysplasia. J. Manip. Physiol. Ther. 2009, 32, 687–694. [Google Scholar] [CrossRef]
- Elias, D.A.; White, L.M.; Fithian, D.C. Acute lateral patellar dislocation at MR imaging: Injury patterns of medial patellar soft-tissue restraints and osteochondral injuries of the inferomedial patella. Radiology 2002, 225, 736–743. [Google Scholar] [CrossRef]
- Felus, J.; Kowalczyk, B.; Lejman, T. Sonographic evaluation of the injuries after traumatic patellar dislocation in adolescents. J. Pediatr. Orthop. 2008, 28, 397–402. [Google Scholar] [CrossRef]
- Gesslein, M.; Merkl, C.; Bail, H.J.; Krutsch, V.; Biber, R.; Schuster, P. Refixation of Large Osteochondral Fractures After Patella Dislocation Shows Better Mid- to Long-Term Outcome Compared With Debridement. Cartilage 2019, 1947603519886637. [Google Scholar] [CrossRef]
- Gormeli, G.; Gormeli, C.A.; Karakaplan, M.; Gurbuz, S.; Ozdemir, Z.; Ozer, M. Acute patellar dislocation with multiple ligament injuries after knee dislocation and single session reconstruction. J. Pak. Med. Assoc. 2016, 66, 757–760. [Google Scholar]
- Jabalameli, M.; Bagherifard, A.; Hadi, H.; Ghaffari, S. Osteochondral fracture in weight-bearing portion of lateral femoral condyle associated with patellar dislocation. J. Surg. Case Rep. 2017, 2017, rjx150. [Google Scholar] [CrossRef]
- Jalan, D.; Morey, V.M.; Mittal, R.; Pannu, C.D. Transient patellar dislocation resulting in simultaneous osteochondral fractures of patella and lateral femoral condyle—A case report. J. Clin. Diagn. Res. 2014, 8, LD04–LD06. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.; Li, J.; Chen, X.X.; Wang, T.; Liu, S.C.; Li, H.C. Fixation versus Excision of Osteochondral Fractures after Patellar Dislocations in Adolescent Patients: A Retrospective Cohort Study. Chin. Med. J. 2018, 131, 1296–1301. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.J.; Christino, M.A.; Daniels, A.H.; Hulstyn, M.J.; Eberson, C.P. Adolescent patellar osteochondral fracture following patellar dislocation. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1856–1861. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Yang, B.S.; Kim, T.W.; Choi, N.H. Ring-shaped lateral meniscus combined with an accessory meniscus: A rare anatomical variant. J. Orthop. Surg. 2020, 28, 2309499019893059. [Google Scholar] [CrossRef] [Green Version]
- Malecki, K.; Pruchnik-Witoslawska, K.; Gwizdala, D.; Grzelak, P.; Flont, P.; Niedzielski, K.R. Clinical Results and MRI Evaluation of Patellar Osteochondral Fracture Fixation following Patellar Dislocation. Biomed. Res. Int. 2019, 2019, 7943636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maletius, W.; Lundberg, M. Refixation of large chondral fragments on the weight-bearing area of the knee joint: A report of two cases. Arthroscopy 1994, 10, 630–633. [Google Scholar] [CrossRef]
- Mashoof, A.A.; Scholl, M.D.; Lahav, A.; Greis, P.E.; Burks, R.T. Osteochondral injury to the mid-lateral weight-bearing portion of the lateral femoral condyle associated with patella dislocation. Arthroscopy 2005, 21, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Megremis, P.; Megremis, O.; Margariti, R. Late Repair, One Year After a Knee Twisting Injury, of a Missed Femoral Trochlea Osteochondral Fragment, With Bioabsorbable Nails, in a 14-Year-Old Boy. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2019, 3, e040. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Arai, Y.; Inoue, H.; Atsumi, S.; Ichimaru, S.; Ikoma, K.; Fujiwara, H.; Kubo, T. Two patients with osteochondral injury of the weight-bearing portion of the lateral femoral condyle associated with lateral dislocation of the patella. Case Rep. Orthop. 2014, 2014, 876410. [Google Scholar] [CrossRef] [Green Version]
- Nietosvaara, Y.; Aalto, K.; Kallio, P.E. Acute patellar dislocation in children: Incidence and associated osteochondral fractures. J. Pediatr. Orthop. 1994, 14, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Nomura, E.; Inoue, M. Second-look arthroscopy of cartilage changes of the patellofemoral joint, especially the patella, following acute and recurrent patellar dislocation. Osteoarthritis Cartilage 2005, 13, 1029–1036. [Google Scholar] [CrossRef] [Green Version]
- Paakkala, A.; Sillanpaa, P.; Huhtala, H.; Paakkala, T.; Maenpaa, H. Bone bruise in acute traumatic patellar dislocation: Volumetric magnetic resonance imaging analysis with follow-up mean of 12 months. Skeletal Radiol. 2010, 39, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Yoo, J.H.; Yoon, H.K.; Chung, K. Osteochondral Fracture of Posterior Aspect of Lateral Femoral Condyle After Lateral Patella Dislocation: A Case Report. JBJS Case Connect. 2020, 10, e1800366. [Google Scholar] [CrossRef]
- Pedowitz, J.M.; Edmonds, E.W.; Chambers, H.G.; Dennis, M.M.; Bastrom, T.; Pennock, A.T. Recurrence of Patellar Instability in Adolescents Undergoing Surgery for Osteochondral Defects Without Concomitant Ligament Reconstruction. Am. J. Sports Med. 2019, 47, 66–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinn, S.F.; Brown, T.R.; Demlow, T.A. MR imaging of patellar retinacular ligament injuries. J. Magn. Reson. Imaging 1993, 3, 843–847. [Google Scholar] [CrossRef]
- Sallay, P.I.; Poggi, J.; Speer, K.P.; Garrett, W.E. Acute dislocation of the patella. A correlative pathoanatomic study. Am. J. Sports Med. 1996, 24, 52–60. [Google Scholar] [CrossRef]
- Sanders, T.L.; Pareek, A.; Johnson, N.R.; Stuart, M.J.; Dahm, D.L.; Krych, A.J. Patellofemoral Arthritis After Lateral Patellar Dislocation: A Matched Population-Based Analysis. Am. J. Sports Med. 2017, 45, 1012–1017. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.L.; Pareek, A.; Hewett, T.E.; Stuart, M.J.; Dahm, D.L.; Krych, A.J. High rate of recurrent patellar dislocation in skeletally immature patients: A long-term population-based study. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Saragaglia, D.; Banihachemi, J.J.; Refaie, R. Acute instability of the patella: Is magnetic resonance imaging mandatory? Int. Orthop. 2020, 44, 2299–2303. [Google Scholar] [CrossRef] [PubMed]
- Seeley, M.; Bowman, K.F.; Walsh, C.; Sabb, B.J.; Vanderhave, K.L. Magnetic resonance imaging of acute patellar dislocation in children: Patterns of injury and risk factors for recurrence. J. Pediatr. Orthop. 2012, 32, 145–155. [Google Scholar] [CrossRef]
- Seeley, M.A.; Knesek, M.; Vanderhave, K.L. Osteochondral injury after acute patellar dislocation in children and adolescents. J. Pediatr. Orthop. 2013, 33, 511–518. [Google Scholar] [CrossRef]
- Stanitski, C.L. Articular hypermobility and chondral injury in patients with acute patellar dislocation. Am. J. Sports Med. 1995, 23, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Stanitski, C.L.; Paletta, G.A., Jr. Articular cartilage injury with acute patellar dislocation in adolescents. Arthroscopic and radiographic correlation. Am. J. Sports Med. 1998, 26, 52–55. [Google Scholar] [CrossRef] [PubMed]
- von Engelhardt, L.V.; Raddatz, M.; Bouillon, B.; Spahn, G.; David, A.; Haage, P.; Lichtinger, T.K. How reliable is MRI in diagnosing cartilaginous lesions in patients with first and recurrent lateral patellar dislocations? BMC Musculoskelet. Disord. 2010, 11, 149. [Google Scholar] [CrossRef] [PubMed]
- Vollnberg, B.; Koehlitz, T.; Jung, T.; Scheffler, S.; Hoburg, A.; Khandker, D.; Hamm, B.; Wiener, E.; Diederichs, G. Prevalence of cartilage lesions and early osteoarthritis in patients with patellar dislocation. Eur. Radiol. 2012, 22, 2347–2356. [Google Scholar] [CrossRef] [PubMed]
- Wissman, R.D.; Verma, S.; Kreeger, M.; Robertson, M. Extensor mechanism injuries in tibiofemoral dislocations. J. Comput. Assist. Tomogr. 2009, 33, 145–149. [Google Scholar] [CrossRef]
- Wilson, A.; Afarin, A.; Shaw, C.; Shirley, E.; Pierce, J.; Slakey, J.B. Magnetic Resonance Imaging Findings After Acute Patellar Dislocation in Children. Orthop. J. Sports Med. 2013, 1, 2325967113512460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaidi, A.; Babyn, P.; Astori, I.; White, L.; Doria, A.; Cole, W. MRI of traumatic patellar dislocation in children. Pediatr. Radiol. 2006, 36, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.Y.; Zheng, L.; Shi, H.; Qu, S.H.; Ding, H.Y. Sonography on injury of the medial patellofemoral ligament after acute traumatic lateral patellar dislocation: Injury patterns and correlation analysis with injury of articular cartilage of the inferomedial patella. Injury 2013, 44, 1892–1898. [Google Scholar] [CrossRef]
- Zhang, G.Y.; Zheng, L.; Feng, Y.; Shi, H.; Liu, W.; Ji, B.J.; Sun, B.S.; Ding, H.Y. Injury patterns of medial patellofemoral ligament and correlation analysis with articular cartilage lesions of the lateral femoral condyle after acute lateral patellar dislocation in adults: An MRI evaluation. Injury 2015, 46, 2413–2421. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Shi, H.; Feng, Y.; Sun, B.S.; Ding, H.Y.; Zhang, G.Y. Injury patterns of medial patellofemoral ligament and correlation analysis with articular cartilage lesions of the lateral femoral condyle after acute lateral patellar dislocation in children and adolescents: An MRI evaluation. Injury 2015, 46, 1137–1144. [Google Scholar] [CrossRef]
- Nomura, E.; Horiuchi, Y.; Inoue, M. Correlation of MR imaging findings and open exploration of medial patellofemoral ligament injuries in acute patellar dislocations. Knee 2002, 9, 139–143. [Google Scholar] [CrossRef]
- Hendawi, T.; Godshaw, B.; Flowers, C.; Stephens, I.; Haber, L.; Waldron, S. Autograft vs Allograft Comparison in Pediatric Medial Patellofemoral Ligament Reconstruction. Ochsner J. 2019, 19, 96–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nomura, E.; Inoue, M.; Osada, N. Anatomical analysis of the medial patellofemoral ligament of the knee, especially the femoral attachment. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 510–515. [Google Scholar] [CrossRef]
- Duthon, V.B. Acute traumatic patellar dislocation. Orthop. Traumatol. Surg. Res. 2015, 101, S59–S67. [Google Scholar] [CrossRef]
- Conlan, T.; Garth, W.P., Jr.; Lemons, J.E. Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J. Bone Jt. Surg Am. 1993, 75, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Feller, J.A.; Feagin, J.A., Jr.; Garrett, W.E., Jr. The medial patellofemoral ligament revisited: An anatomical study. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Smirk, C.; Morris, H. The anatomy and reconstruction of the medial patellofemoral ligament. Knee 2003, 10, 221–227. [Google Scholar] [CrossRef]
- Weber-Spickschen, T.S.; Spang, J.; Kohn, L.; Imhoff, A.B.; Schottle, P.B. The relationship between trochlear dysplasia and medial patellofemoral ligament rupture location after patellar dislocation: An MRI evaluation. Knee 2011, 18, 185–188. [Google Scholar] [CrossRef]
- Ahmad, C.S.; Shubin Stein, B.E.; Matuz, D.; Henry, J.H. Immediate surgical repair of the medial patellar stabilizers for acute patellar dislocation. A review of eight cases. Am. J. Sports Med. 2000, 28, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Avikainen, V.J.; Nikku, R.K.; Seppanen-Lehmonen, T.K. Adductor magnus tenodesis for patellar dislocation. Technique and preliminary results. Clin. Orthop. Relat. Res. 1993, 297, 12–16. [Google Scholar]
- Sillanpaa, P.J.; Maenpaa, H.M.; Mattila, V.M.; Visuri, T.; Pihlajamaki, H. Arthroscopic surgery for primary traumatic patellar dislocation: A prospective, nonrandomized study comparing patients treated with and without acute arthroscopic stabilization with a median 7-year follow-up. Am. J. Sports Med. 2008, 36, 2301–2309. [Google Scholar] [CrossRef] [PubMed]
- Nomura, E.; Inoue, M. Cartilage lesions of the patella in recurrent patellar dislocation. Am. J. Sports Med. 2004, 32, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Migliorini, F.; Rath, B.; Tingart, M.; Niewiera, M.; Eschweiler, J. Distal alignment procedures for patellofemoral instability: Comprehensive review of the literature. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1579–1588. [Google Scholar] [CrossRef]
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L.M. Epidemiology and natural history of acute patellar dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Stefancin, J.J.; Parker, R.D. First-time traumatic patellar dislocation: A systematic review. Clin. Orthop. Relat. Res. 2007, 455, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsen, E.; Lauridsen, F. Conservative treatment of patellar dislocations. Influence of evident factors on the tendency to redislocation and the therapeutic result. Clin. Orthop. Relat. Res. 1982, 171, 131–136. [Google Scholar] [CrossRef]
- Arendt, E.A.; Askenberger, M.; Agel, J.; Tompkins, M.A. Risk of Redislocation After Primary Patellar Dislocation: A Clinical Prediction Model Based on Magnetic Resonance Imaging Variables. Am. J. Sports Med. 2018, 46, 3385–3390. [Google Scholar] [CrossRef] [PubMed]
- Balcarek, P.; Oberthur, S.; Hopfensitz, S.; Frosch, S.; Walde, T.A.; Wachowski, M.M.; Schuttrumpf, J.P.; Sturmer, K.M. Which patellae are likely to redislocate? Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2308–2314. [Google Scholar] [CrossRef] [PubMed]
- Jaquith, B.P.; Parikh, S.N. Predictors of Recurrent Patellar Instability in Children and Adolescents After First-time Dislocation. J. Pediatr. Orthop. 2017, 37, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.Y.; Ding, H.Y.; Li, E.M.; Zheng, L.; Bai, Z.W.; Shi, H.; Fan, F.J.; Guo, D. Incidence of second-time lateral patellar dislocation is associated with anatomic factors, age and injury patterns of medial patellofemoral ligament in first-time lateral patellar dislocation: A prospective magnetic resonance imaging study with 5-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Hevesi, M.; Heidenreich, M.J.; Camp, C.L.; Hewett, T.E.; Stuart, M.J.; Dahm, D.L.; Krych, A.J. The Recurrent Instability of the Patella Score: A Statistically Based Model for Prediction of Long-Term Recurrence Risk After First-Time Dislocation. Arthroscopy 2019, 35, 537–543. [Google Scholar] [CrossRef]
- Christensen, T.C.; Sanders, T.L.; Pareek, A.; Mohan, R.; Dahm, D.L.; Krych, A.J. Risk Factors and Time to Recurrent Ipsilateral and Contralateral Patellar Dislocations. Am. J. Sports Med. 2017, 45, 2105–2110. [Google Scholar] [CrossRef] [PubMed]
- Sillanpaa, P.J.; Peltola, E.; Mattila, V.M.; Kiuru, M.; Visuri, T.; Pihlajamaki, H. Femoral avulsion of the medial patellofemoral ligament after primary traumatic patellar dislocation predicts subsequent instability in men: A mean 7-year nonoperative follow-up study. Am. J. Sports Med. 2009, 37, 1513–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeoh, C.S.; Lam, K.Y. Tibial tubercle to trochlear groove distance and index in children with one-time versus recurrent patellar dislocation: A magnetic resonance imaging study. J. Orthop. Surg. 2016, 24, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Apostolovic, M.; Vukomanovic, B.; Slavkovic, N.; Vuckovic, V.; Vukcevic, M.; Djuricic, G.; Kocev, N. Acute patellar dislocation in adolescents: Operative versus nonoperative treatment. Int. Orthop. 2011, 35, 1483–1487. [Google Scholar] [CrossRef] [Green Version]
- Bitar, A.C.; Demange, M.K.; D’Elia, C.O.; Camanho, G.L. Traumatic patellar dislocation: Nonoperative treatment compared with MPFL reconstruction using patellar tendon. Am. J. Sports Med. 2012, 40, 114–122. [Google Scholar] [CrossRef]
- Camanho, G.L.; Viegas Ade, C.; Bitar, A.C.; Demange, M.K.; Hernandez, A.J. Conservative versus surgical treatment for repair of the medial patellofemoral ligament in acute dislocations of the patella. Arthroscopy 2009, 25, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, S.E.; Jakobsen, B.W.; Lund, B.; Lind, M. Isolated repair of the medial patellofemoral ligament in primary dislocation of the patella: A prospective randomized study. Arthroscopy 2008, 24, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Ji, G.; Wang, S.; Wang, X.; Liu, J.; Niu, J.; Wang, F. Surgical versus Nonsurgical Treatments of Acute Primary Patellar Dislocation with Special Emphasis on the MPFL Injury Patterns. J. Knee Surg. 2017, 30, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.L.; Yau, W.P. Management of traumatic patellar dislocation in a regional hospital in Hong Kong. Hong Kong Med. J. 2017, 23, 122–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petri, M.; Liodakis, E.; Hofmeister, M.; Despang, F.J.; Maier, M.; Balcarek, P.; Voigt, C.; Haasper, C.; Zeichen, J.; Stengel, D.; et al. Operative vs conservative treatment of traumatic patellar dislocation: Results of a prospective randomized controlled clinical trial. Arch. Orthop. Trauma Surg. 2013, 133, 209–213. [Google Scholar] [CrossRef]
- Regalado, G.; Lintula, H.; Kokki, H.; Kroger, H.; Vaatainen, U.; Eskelinen, M. Six-year outcome after non-surgical versus surgical treatment of acute primary patellar dislocation in adolescents: A prospective randomized trial. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Sillanpaa, P.J.; Mattila, V.M.; Maenpaa, H.; Kiuru, M.; Visuri, T.; Pihlajamaki, H. Treatment with and without initial stabilizing surgery for primary traumatic patellar dislocation. A prospective randomized study. J. Bone Jt. Surg. Am. 2009, 91, 263–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sillanpää, P.; Mattila, V.M.; Iivonen, T.; Visuri, T.; Pihlajamäki, H.M. Incidence and risk factors of acute traumatic primary patellar dislocation. Med. Sci. Sports Exerc. 2008, 40, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Bollier, M.; Fulkerson, J.; Cosgarea, A.; Tanaka, M. Technical failure of medial patellofemoral ligament reconstruction. Arthroscopy 2011, 27, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.H.; Kim, H.K.; Shiraj, S.; Anton, C.; Kim, D.H.; Horn, P.S. Patellofemoral instability in children: T2 relaxation times of the patellar cartilage in patients with and without patellofemoral instability and correlation with morphological grading of cartilage damage. Pediatr. Radiol. 2016, 46, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Horaguchi, T.; Okano, T.; Yoshimatsu, T.; Saito, A.; Ryu, J. Patellar dislocation: Arthroscopic patellar stabilization with anchor sutures. Arthroscopy 2004, 20, 761–764. [Google Scholar] [CrossRef]
- Hing, C.B.; Smith, T.O.; Donell, S.; Song, F. Surgical versus non-surgical interventions for treating patellar dislocation. Cochrane Database Syst Rev. 2011. [Google Scholar] [CrossRef] [Green Version]
- Reagan, J.; Kullar, R.; Burks, R. MPFL reconstruction: Technique and results. Orthop. Clin. N. Am. 2015, 46, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Stupay, K.L.; Swart, E.; Shubin Stein, B.E. Widespread Implementation of Medial Patellofemoral Ligament Reconstruction for Recurrent Patellar Instability Maintains Functional Outcomes at Midterm to Long-Term Follow-up While Decreasing Complication Rates: A Systematic Review. Arthroscopy 2015, 31, 1372–1380. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PEDro Score | |
|---|---|
| 1. Eligibility criteria | 98% (41 of 42) |
| 2. Random allocation | 0% (0 of 42) |
| 3. Concealed allocation | 43% (18 of 42) |
| 4. Baseline comparability | 86% (36 of 42) |
| 5. Blind subject | 43% (18 of 42) |
| 6. Blind clinician | 0% (0 of 42) |
| 7. Blind assessor | 21% (9 of 42) |
| 8. Adequate follow-up | 93% (39 of 42) |
| 9. Intention-to-treat analysis | 95% (40 of 42) |
| 10. Between-group analysis | 90% (38 of 42) |
| 11. Point estimates and variability | 74% (31 of 42) |
| Author, Year | Journal Name | Design | Knees (n) | Mean Age (Mean) |
|---|---|---|---|---|
| Bui et al., 2008 [36] | Skeletal Radiol | RCS | 20 | 31 |
| Callewier et al., 2009 [37] | Orthop Traumatol Surg Res | CR | 1 | 23 |
| Cavalheiro et al., 2018 [38] | Rev Bras Ortop | CR | 1 | 13 |
| Cho et al., 2009 [39] | J Manipulative Physiol Ter | CR | 1 | 16 |
| Elias et al., 2002 [40] | Radiology | RCS | 82 | 20 |
| Felus et al., 2008 [41] | J Pediatr Orthop | PCS | 22 | 14 |
| Gesslein et al., 2019 [42] | Cartilage | RCS | 53 | 19.5 |
| Gormeli et al., 2016 [43] | J Pak Med Assoc | CR | 1 | 41 |
| Guerrero et al., 2009 [14] | Sports Med Arthrosc Rehabil Ther Technol | RCS | 195 | 23 |
| Jabalameli et al., 2017 [44] | J Surg Case Rep | CR | 3 | 17 |
| Jalan et al., 2014 [45] | J Clin Diagn Res | CR | 1 | 30 |
| Kang et al., 2018 [46] | Chin Med J (Engl) | RCS | 43 | 14.1 |
| Lee et al., 2013 [47] | Knee Surg Sports Traumatol Arthrosc | RCS | 9 | 14.6 |
| Lee et al., 2020 [48] | J Orthop Surg (Hong Kong) | CR | 1 | 16 |
| Maleki et al., 2019 [49] | Biomed Res Int | CS | 17 | 14.1 |
| Maletius et al., 1994 [50] | Arthroscopy | CR | 2 | 19.5 |
| Mashoof et al., 2005 [51] | Arthroscopy | RCS | 7 | 24 |
| Megremis et al., 2019 [52] | J Am Acad Orthop Surg Glob Res Rev | CR | 1 | 14 |
| Nakagawa et al., 2014 [53] | Case Rep Orthop | CR | 2 | 14.5 |
| Nietosvaara et al., 1994 [54] | J Pediatr Orthop | PCS | 72 | 13.3 |
| Nomura et al., 2003 [15] | Arthroscopy | CS | 39 | 18 |
| Nomura et al., 2005 [55] | Osteoarthritis Cartilage | RCS | 30 | 17.2 |
| Paakkala et al., 2010 [56] | Skeletal Radiol | CS | 23 | 19–45 |
| Park et al., 2020 [57] | JBJS Case Connect | CR | 1 | 15 |
| Pedowitz et al., 2019 [58] | Am J Sports Med | RCS | 41 | 13.8 |
| Quinn et al., 1993 [59] | J Magn Reson Imaging | CS | 8 | |
| Sallay et al., 1996 [60] | Am J Sports Med | RCS | 12 | 25 |
| Sanders et al., 2017 [61] | Am J Sports Med | PCS | 609 | 21.4 |
| Sanders et al., 2018 [62] | Knee Surg Sports Traumatol Arthrosc | PCS | 232 | 14.1 |
| Saragaglia et al., 2020 [63] | Int Orthop | PCS | 39 | 23 |
| Seeley et al., 2012 [64] | J Pediatr Orthop | RCS | 111 | 14.9 |
| Seeley et al., 2013 [65] | J Pediatr Orthop | RCS | 46 | 14.6 |
| Stanitski 1995 [66] | Am J Sports Med | CS | 17 | 13.8 |
| Stanitski et al., 1998 [67] | Am J Sports Med | CS | 48 | 14 |
| von Engelhardt et al., 2010 [68] | BMC Muskuloskelet Disord | CS | 40 | 21.5 |
| Vollnberg et al., 2012 [69] | Eur Radiol | RCS | 51 | 22.4 |
| Wissmann et al., 2009 [70] | J Comput Assist Tomogr | RCS | 14 | 33 |
| Wilson et al., 2013 [71] | Orthop J Sports Med | CS | 36 | 14.5 |
| Zaidi et al., 2006 [72] | Pediatr Radiol | RCS | 26 | 13.9 |
| Zhang et al., 2013 [73] | Injury | RCS | 49 | 24.5 |
| Zhang et al., 2015 [74] | Injury | PCS | 121 | 25 |
| Zheng et al., 2015 [75] | Injury | PCS | 127 | 14.1 |
| First Time Patellar Dislocation—MRI Findings | |
|---|---|
| Evidence of lateral trochlea damage (Outerbridge) | 47% (191 of 410) |
| I (6.2%) | |
| II (17.5%) | |
| III (9.3%) | |
| IV (10.3%) | |
| V (11.3%) | |
| Evidence of patellar damage (Outerbridge) | 85% (85 of 100) |
| I (17.6%) | |
| II (32.4%) | |
| III (20.3%) | |
| IV (31.1%) | |
| V (0%) | |
| Free loose bodies | 11.5% (183 of 1589) |
| MPFL tear | 98% (1031 of 1052) |
| patellar site | 48.0% (315 of 656) |
| femoral site | 33.7% (268 of 402) |
| midportion | 18.2% (73 of 402) |
| First Time Patellar Dislocation—Arthroscopic Findings | |
|---|---|
| Lateral patellar facet (ICRS) | I (2.8%) |
| II (2.8%) | |
| III (2.8%) | |
| IV (0%) | |
| Medial patellar facet (ICRS) | I (2.8%) |
| II (18.3%) | |
| III (15.5%) | |
| IV (29.6%) | |
| Median crest lesions (ICRS) | I (7.0%) |
| II (19.7%) | |
| III (8.5%) | |
| IV (18.3%) | |
| Trochlea (ICRS) | I (9.7%) |
| II (13.9%) | |
| III (3.2%) | |
| IV (0%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorini, F.; Marsilio, E.; Cuozzo, F.; Oliva, F.; Eschweiler, J.; Hildebrand, F.; Maffulli, N. Chondral and Soft Tissue Injuries Associated to Acute Patellar Dislocation: A Systematic Review. Life 2021, 11, 1360. https://doi.org/10.3390/life11121360
Migliorini F, Marsilio E, Cuozzo F, Oliva F, Eschweiler J, Hildebrand F, Maffulli N. Chondral and Soft Tissue Injuries Associated to Acute Patellar Dislocation: A Systematic Review. Life. 2021; 11(12):1360. https://doi.org/10.3390/life11121360
Chicago/Turabian StyleMigliorini, Filippo, Emanuela Marsilio, Francesco Cuozzo, Francesco Oliva, Jörg Eschweiler, Frank Hildebrand, and Nicola Maffulli. 2021. "Chondral and Soft Tissue Injuries Associated to Acute Patellar Dislocation: A Systematic Review" Life 11, no. 12: 1360. https://doi.org/10.3390/life11121360