
Is There a Role for the Microbiome and Sudden Death? A Systematic Review



Abstract
:1. Introduction
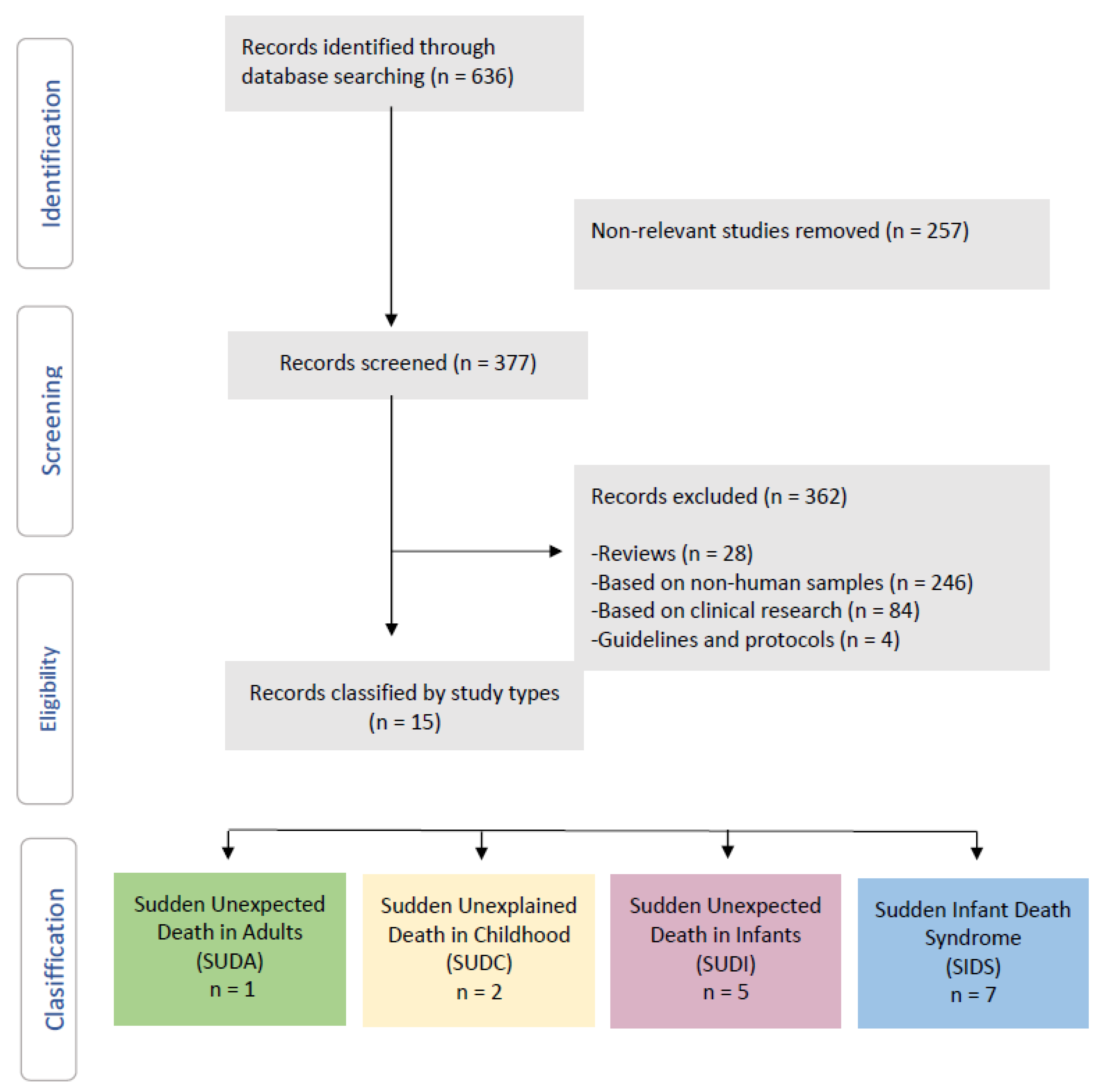
2. Systematic Review
2.1. Inclusion Criteria
2.2. Search Strategy
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Descriptive Studies
2.6. Risk of Bias Assessment
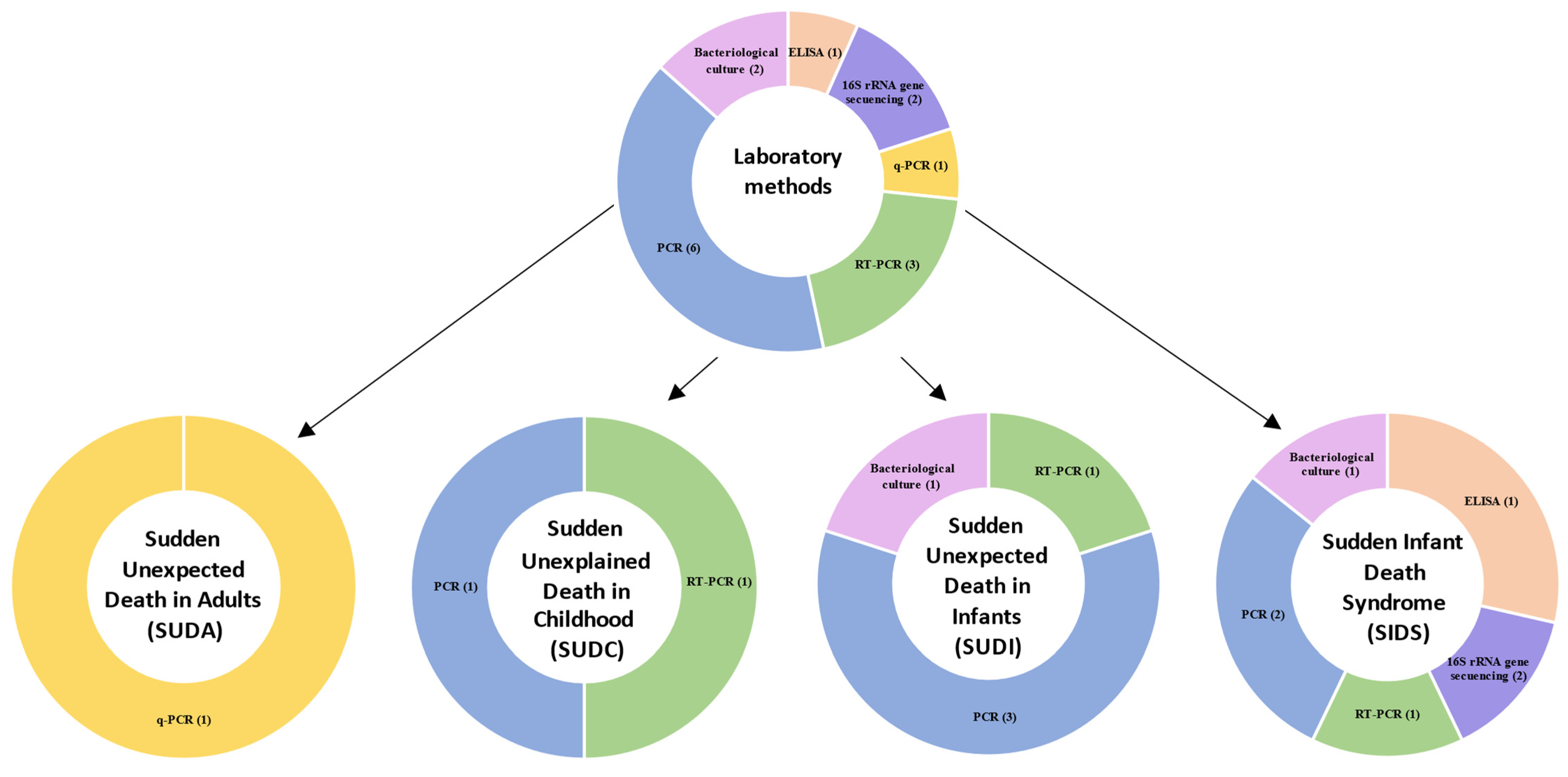
2.7. Laboratory Methods
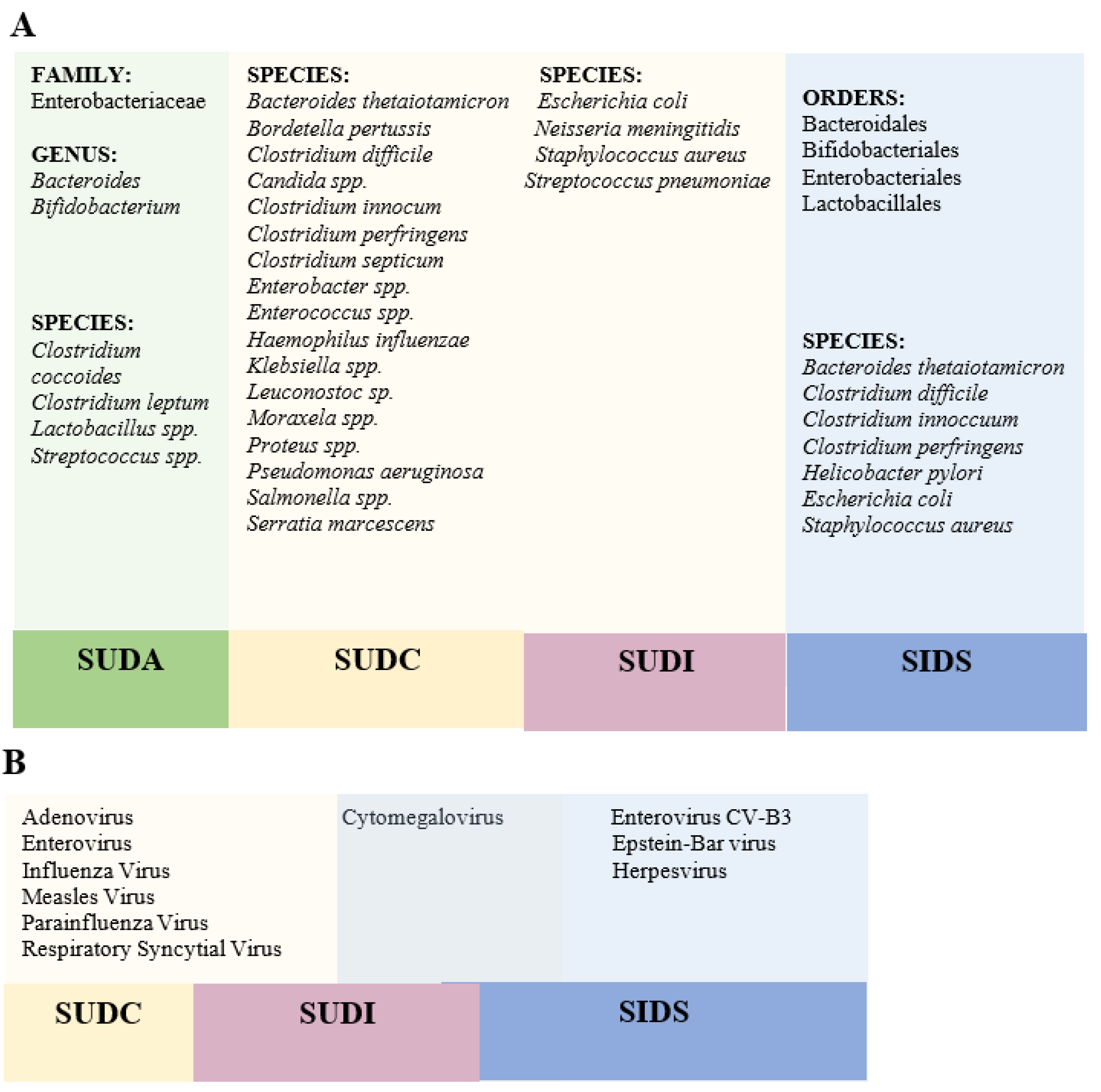
3. Microbiome Analysis in Post-Mortem Forensic Studies of Sudden Death
3.1. Sudden Unexpected Death in Adults
3.2. Sudden Unexplained Death in Childhood
3.3. Sudden Unexpected Death in Infancy
3.4. Sudden Infant Death Syndrome
4. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Madea, B.; Argo, A. Certification of Death: External Postmortem Examination. In Handbook of Forensic Medicine; John Wiley & Sons, Ltd.: Bonn, Germany, 2014; ISBN 9781118570654. [Google Scholar]
- World Health Organization. International Classification of Diseases (ICD-10). Available online: https://icd.who.int/browse10/2019/en#/R96.0 (accessed on 20 November 2021).
- Menezes, R.G.; Ahmed, S.; Pasha, S.B.; Hussain, S.A.; Fatima, H.; Kharoshah, M.A.; Madadin, M. Gastrointestinal causes of sudden unexpected death: A review. Med. Sci. Law 2018, 58, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Hugar, B.S.; Harish, S.; Girishchandra, Y.P.; Jayanth, S.H. Study of sudden gastrointestinal deaths: An autopsy study. Med. Sci. Law 2014, 54, 63–67. [Google Scholar] [CrossRef] [PubMed]
- De Asmundis, C.; Brugada, P. Epidemiology of Sudden Cardiac Death. Rev. Española Cardiol. Supl. 2013, 13, 2–6. [Google Scholar] [CrossRef]
- Gould, S.J. Sudden unexpected death in infancy. Curr. Diagnostic Pathol. 2001, 7, 69–75. [Google Scholar] [CrossRef]
- Kruger, M.M.; Martin, L.J.; Maistry, S.; Heathfield, L.J. A systematic review exploring the relationship between infection and sudden unexpected death between 2000 and 2016: A forensic perspective. Forensic Sci. Int. 2018, 289, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Willinger, M.; James, L.S.; Catz, C. Defining the sudden infant death syndrome (sids): Deliberations of an expert panel convened by the national institute of child health and human development. Fetal Pediatr. Pathol. 1991, 11, 677–684. [Google Scholar] [CrossRef]
- Goldwater, P.N. Infection: The neglected paradigm in SIDS research. Arch. Dis. Child. 2017, 102, 767–772. [Google Scholar] [CrossRef] [Green Version]
- Kattwinkel, J.; Hauck, F.R.; Keenan, M.E.; Malloy, M.; Moon, R.Y.; Willinger, M.; Couto, J. The changing concept of sudden infant death syndrome: Diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Pediatrics 2005, 116, 1245–1255. [Google Scholar] [CrossRef] [Green Version]
- Ruiz Botia, I.; Cassanello Peñarroya, P.; Díez Izquierdo, A.; Martínez Sánchez, J.M.; Balaguer Santamaria, A. Sudden infant death syndrome: Do the parents follow the recommendations? An. Pediatr. 2020, 92, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Canadian Agency for Drugs and Technologies in Health Interventions for the Prevention of Sudden Infant Death Syndrome: Guidelines; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2020.
- Haas, E.A. Sudden Unexplained Death in Childhood: An Overview. In SIDS Sudden infant and early childhood death: The past, the present and the future; Duncan, J.R., Byard, R.W., Eds.; University of Adelaide Press: Adelaide, Australia, 2018; pp. 51–71. ISBN 9781925261677. [Google Scholar]
- Molina, P.; Bermejo, M.; Cardona, B.; Giner, S. Clasificación de San Diego y Nuevas Tendencias del Síndrome de Muerte Súbita del Lactante; Asociación Española de Pediatría: Madrid, Spain, 2013. [Google Scholar]
- Goldwater, P.N. SIDS, prone sleep position and infection: An overlooked epidemiological link in current SIDS research? Key evidence for the “Infection Hypothesis.”. Med. Hypotheses 2020, 144, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Marom, T.; Cinamon, U.; Castellanos, P.F.; Cohen, M.C. Otolaryngological aspects of sudden infant death syndrome. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 311–318. [Google Scholar] [CrossRef]
- Thach, B.T. Sudden infant death syndrome: Can gastroesophageal reflux cause sudden infant death? Am. J. Med. 2000, 108, 144–148. [Google Scholar] [CrossRef]
- Vege, Å.; Rognum, T.O. Inflammatory responses in sudden infant death syndrome - Past and present views. FEMS Immunol. Med. Microbiol. 1999, 25, 67–78. [Google Scholar] [CrossRef]
- Hauck, F.R.; Tanabe, K.O. Beyond “back to sleep”: Ways to further reduce the risk of sudden infant death syndrome. Pediatr. Ann. 2017, 46, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Courts, C.; Madea, B. Genetics of the sudden infant death syndrome. Forensic Sci. Int. 2010, 203, 25–33. [Google Scholar] [CrossRef]
- Young, J.; Shipstone, R. Shared Sleeping Surfaces and Dangerous Sleeping Environments. In SIDS Sudden Infant and Early Childhood Death: The Past, the Present and the Future; Duncan, J.R., Byard, R.W., Eds.; University of Adelaide Press: Adelaide, Australia, 2018; pp. 187–216. ISBN 9781925261677. [Google Scholar]
- Filiano, J.J.; Kinney, H.C. A Perspective on Neuropathologic Findings in Victims of the Sudden Infant Death Syndrome: The Triple-Risk Model. Biol Neonate 1994, 65, 194–197. [Google Scholar] [CrossRef]
- García, M.G.; Pérez-Cćrceles, M.D.; Osuna, E.; Legaz, I. Impact of the Human Microbiome in Forensic Sciences: a Systematic Review. Appl. Environ. Microbiol. 2020, 86, 1–20. [Google Scholar] [CrossRef]
- Carlin, R.F.; Moon, R.Y. Risk factors, protective factors, and current recommendations to reduce sudden infant death syndrome a review. JAMA Pediatr. 2017, 171, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.; Amorim, A. Microbial forensics: New breakthroughs and future prospects. Appl. Microbiol. Biotechnol. 2018, 102, 10377–10391. [Google Scholar] [CrossRef]
- Horne, R.S.C. Sudden infant death syndrome: Current perspectives. Intern. Med. J. 2019, 49, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.H. Sudden death in pediatric populations. Korean Circ. J. 2010, 40, 253–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, P.; Blair, P.S. Sudden Infant Death Syndrome and parental smoking. Early Hum. Dev. 2007, 83, 721–725. [Google Scholar] [CrossRef]
- Heron, M. Deaths: Leading causes for 2014. Natl. Vital Stat. Reports 2016, 65, 1–96. [Google Scholar]
- Liebrechts-Akkerman, G.; Lao, O.; Liu, F.; Van Sleuwen, B.E.; Engelberts, A.C.; L’Hoir, M.P.; Tiemeier, H.W.; Kayser, M. Postnatal parental smoking: An important risk factor for SIDS. Eur. J. Pediatr. 2011, 170, 1281–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, R.Y.; Horne, R.S.C.H.; Hauck, F.R. Sudden Infant Death Syndrome. Encycl. Respir. Med. Four-Volume Set 2007, 370, 1578–1587. [Google Scholar] [CrossRef]
- Moon, R.Y.; Oden, R.P.; Joyner, B.L.; Ajao, T.I. Qualitative Analysis of Beliefs and Perceptions about Sudden Infant Death Syndrome in African-American Mothers: Implications for Safe Sleep Recommendations. J. Pediatr. 2010, 157, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Stiffler, D.; Ayres, B.; Fauvergue, C.; Cullen, D. Sudden infant death and sleep practices in the Black community. J. Spec. Pediatr. Nurs. 2018, 23. [Google Scholar] [CrossRef]
- Horne, R.S.C. Autonomic Cardiorespiratory Physiology and Arousal of the Fetus and Infant. In SIDS Sudden Infant and Early Childhood Death: The Past, the Present and the Future; Duncan, J.R., Byard, R.W., Eds.; University of Adelaide Press: Adelaide, Australia, 2018; pp. 449–491. ISBN 9781925261677. [Google Scholar]
- Clemente, J.C.; Ursell, L.K.; Parfrey, L.W.; Knight, R. Review The Impact of the Gut Microbiota on Human Health: An Integrative View. Cell 2012, 148, 1258–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rautava, S.; Luoto, R.; Salminen, S.; Isolauri, E. Microbial contact during pregnancy, intestinal colonization and human disease. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 565–576. [Google Scholar] [CrossRef]
- Levy, M.; Blacher, E.; Elinav, E. Microbiome, metabolites and host immunity. Curr. Opin. Microbiol. 2017, 35, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Tsang, T.K.; Lee, K.H.; Foxman, B.; Balmaseda, A.; Gresh, L.; Sanchez, N.; Ojeda, S.; Lopez, R.; Yang, Y.; Kuan, G.; et al. Association between the respiratory microbiome and susceptibility to influenza virus infection. Clin. Infect. Dis. 2020, 71, 1195–1203. [Google Scholar] [CrossRef]
- Luoto, R.; Ruuskanen, O.; Waris, M.; Kalliomäki, M.; Salminen, S.; Isolauri, E. Prebiotic and probiotic supplementation prevents rhinovirus infections in preterm infants: A randomized, placebo-controlled trial. J. Allergy Clin. Immunol. 2014, 133, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Ichinohe, T.; Pang, I.K.; Kumamoto, Y.; Peaper, D.R.; Ho, J.H.; Murray, T.S.; Iwasaki, A. Microbiota regulates immune defense against respiratory tract influenza a virus infection. Proc. Natl. Acad. Sci. USA 2011, 108, 5354–5359. [Google Scholar] [CrossRef] [Green Version]
- Panigrahi, P.; Parida, S.; Nanda, N.C.; Satpathy, R.; Pradhan, L.; Chandel, D.S.; Baccaglini, L.; Mohapatra, A.; Mohapatra, S.S.; Misra, P.R.; et al. A randomized synbiotic trial to prevent sepsis among infants in rural India. Nature 2017, 548, 407–412. [Google Scholar] [CrossRef]
- Abt, M.C.; Osborne, L.C.; Monticelli, L.A.; Doering, T.A.; Alenghat, T.; Sonnenberg, G.F.; Paley, M.A.; Antenus, M.; Williams, K.L.; Erikson, J.; et al. Commensal Bacteria Calibrate the Activation Threshold of Innate Antiviral Immunity. Inmunity 2012, 27, 158–170. [Google Scholar] [CrossRef] [Green Version]
- Tremaroli, V.; Bäckhed, F. Functional interactions between the gut microbiota and host metabolism. Nature 2012, 489, 242–249. [Google Scholar] [CrossRef]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F. Preferred reporting items for a systematic review and meta-analysis of individual participant data: The PRISMA-IPD statement. J. Am. Med. Assoc. 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0; Green, S., Ed.; The Cochrane Collaboration: Oxford, UK, 2011. [Google Scholar]
- Armstrong, R.; Jackson, N.; Doyle, J.; Waters, E.; Howes, F. It’s in your hands: The value of handsearching in conducting systematic reviews of public health interventions. J. Public Health (Bangkok). 2005, 27, 388–391. [Google Scholar] [CrossRef] [Green Version]
- de Vet, H.C.W.; Dikmans, R.E.; Eekhout, I. Specific agreement on dichotomous outcomes can be calculated for more than two raters. J. Clin. Epidemiol. 2017, 83, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Critical Appraisal Skills Programme. CASP Checklists; Critical Apraisal Skills Programme: Oxford, UK, 2020. [Google Scholar]
- Oxman, A.D. Grading quality of evidence and strength of recommendations. Br. Med. J. 2004, 328, 1490–1494. [Google Scholar] [CrossRef] [Green Version]
- Tuomisto, S.; Huhtala, H.; Martiskainen, M.; Goebeler, S.; Lehtimäki, T.; Karhunen, P.J. Age-dependent association of gut bacteria with coronary atherosclerosis: Tampere sudden death study. PLoS One 2019, 14, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prtak, L.; Al-Adnani, M.; Fenton, P.; Kudesia, G.; Cohen, M.C. Contribution of bacteriology and virology in sudden unexpected death in infancy. Arch. Dis. Child. 2010, 95, 371–376. [Google Scholar] [CrossRef]
- Burger, M.C.; Dempers, J.J.; De Beer, C. Profiling the approach to the investigation of viral infections in cases of sudden unexpected death in infancy in the Western Cape Province, South Africa. Forensic Sci. Int. 2014, 239, 27–30. [Google Scholar] [CrossRef]
- Weber, M.A.; Klein, N.J.; Hartley, J.C.; Lock, P.E.; Malone, M.; Sebrine, M.J. Infection and sudden unexpected death in infancy: A systematic retrospective case review. Lancet 2008, 371, 1848–1853. [Google Scholar] [CrossRef]
- Weber, M.A.; Hartley, J.C.; Ashworth, M.T.; Malone, M.; Sebire, N.J. Virological investigations in sudden unexpected deaths in infancy (SUDI). Forensic Sci. Med. Pathol. 2010, 6, 261–267. [Google Scholar] [CrossRef]
- Weber, M.A.; Hartley, J.C.; Klein, N.J.; Risdon, R.A.; Malone, M.; Sebire, N.J. Staphylococcal toxins in sudden unexpected death in infancy: Experience from a single specialist centre. Forensic Sci. Med. Pathol. 2011, 7, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Vargas, S.L.; Ponce, C.A.; Gallo, M.; Pérez, F.; Astorga, J.F.; Bustamante, R.; Chabé, M.; Durand-Joly, I.; Iturra, P.; Miller, R.F.; et al. Near-universal prevalence of pneumocystis and associated increase in mucus in the lungs of infants with sudden unexpected death. Clin. Infect. Dis. 2013, 56, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Yagmur, G.; Ziyade, N.; Elgormus, N.; Das, T.; Sahin, M.F. Postmortem diagnosis of cytomegalovirus and accompanying other infection agents by real-time PCR in cases of sudden unexpected death in infancy (SUDI). J. Forensic Leg. Med. 2015, 38, 18–23. [Google Scholar] [CrossRef]
- Álvarez-Lafuente, R.; Aguilera, B.; Suárez-Mier, M.P.; Morentin, B.; Vallejo, G.; Gómez, J.; Fernández-Rodríguez, A. Detection of human herpesvirus-6, Epstein-Barr virus and cytomegalovirus in formalin-fixed tissues from sudden infant death: A study with quantitative real-time PCR. Forensic Sci. Int. 2008, 178, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Stray-Pedersen, A.; Vege, Å.; Rognum, T.O. Helicobacter pylori antigen in stool is associated with SIDS and sudden infant deaths due to infectious disease. Pediatr. Res. 2008, 64, 405–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, J.L.; Bettelheim, K.A.; Luke, R.K.J.; Goldwater, P.N. Serotypes of Escherichia coli in Sudden Infant Death Syndrome. J. Appl. Microbiol. 2010, 108, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Highet, A.R.; Goldwater, P.N. Staphylococcal enterotoxin genes are common in Staphylococcus aureus intestinal flora in Sudden infant death syndrome (SIDS) and live comparison infants. FEMS Immunol. Med. Microbiol. 2009, 57, 151–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Highet, A.R.; Berry, A.M.; Bettelheim, K.A.; Goldwater, P.N. Gut microbiome in sudden infant death syndrome (SIDS) differs from that in healthy comparison babies and offers an explanation for the risk factor of prone position. Int. J. Med. Microbiol. 2014, 304, 735–741. [Google Scholar] [CrossRef]
- Gaaloul, I.; Riabi, S.; Evans, M.; Hunter, T.; Huber, S.; Aouni, M. Postmortem diagnosis of infectious heart diseases: A mystifying cause of Sudden Infant Death. Forensic Sci. Int. 2017, 262, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Leong, L.E.X.; Taylor, S.L.; Shivasami, A.; Goldwater, P.N.; Rogers, G.B. Intestinal Microbiota Composition in Sudden Infant Death Syndrome and Age-Matched Controls. J. Pediatr. 2017, 191, 63–68.e1. [Google Scholar] [CrossRef]
- Al Mana, H.; Yassine, H.M.; Younes, N.N.; Al-Mohannadi, A.; Al-Sadeq, D.W.; Alhababi, D.; Nasser, E.A.; Nasrallah, G.K. The current status of cytomegalovirus (CMV) prevalence in the MENA region: A systematic review. Pathogens 2019, 8. [Google Scholar] [CrossRef] [Green Version]
- Gleeson, M.; Clancy, R.L.; Cox, A.J.; Gulliver, S.A.; Hall, S.T.; Cooper, D.M. Mucosal immune responses to infections in infants with acute life threatening events classified as “near-miss” sudden infant death syndrome. FEMS Immunol. Med. Microbiol. 2004, 42, 105–118. [Google Scholar] [CrossRef] [Green Version]
- Aagaard, K.; Ma, J.; Antony, K.M.; Ganu, R.; Petrosino, J.; Versalovic, J. The placenta harbors a unique microbiome. Sci. Transl. Med. 2014, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiGiulio, D.B.; Romero, R.; Amogan, H.P.; Kusanovic, J.P.; Bik, E.M.; Gotsch, F.; Kim, C.J.; Erez, O.; Edwin, S.; Relman, D.A. Microbial prevalence, diversity and abundance in amniotic fluid during preterm labor: A molecular and culture-based investigation. PLoS One 2008, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, E.; Fernández, L.; Marín, M.L.; Martín, R.; Odriozola, J.M.; Nueno-Palop, C.; Narbad, A.; Olivares, M.; Xaus, J.; Rodríguez, J.M. Isolation of commensal bacteria from umbilical cord blood of healthy neonates born by cesarean section. Curr. Microbiol. 2005, 51, 270–274. [Google Scholar] [CrossRef]
- Lauder, A.P.; Roche, A.M.; Sherrill-Mix, S.; Bailey, A.; Laughlin, A.L.; Bittinger, K.; Leite, R.; Elovitz, M.A.; Parry, S.; Bushman, F.D. Comparison of placenta samples with contamination controls does not provide evidence for a distinct placenta microbiota. Microbiome 2016, 4, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salter, S.J.; Cox, M.J.; Turek, E.M.; Calus, S.T.; Cookson, W.O.; Moffatt, M.F.; Turner, P.; Parkhill, J.; Loman, N.J.; Walker, A.W. Reagent and laboratory contamination can critically impact sequence-based microbiome analyses. BMC Biol. 2014, 12, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Perez-Muñoz, M.E.; Arrieta, M.C.; Ramer-Tait, A.E.; Walter, J. A critical assessment of the “sterile womb” and “in utero colonization” hypotheses: Implications for research on the pioneer infant microbiome. Microbiome 2017, 5, 1–19. [Google Scholar] [CrossRef]
- Doré, J.; Schir, A.; Hannequart-Gramet, G.; Corthier, G.; Pochart, P. Design and evaluation of a 16S rRNA-Targeted oligonucleotide probe for specific detection and quantitation of human faecal Bacteroides populations. Syst. Appl. Microbiol. 1998, 21, 65–71. [Google Scholar] [CrossRef]
- Milani, C.; Duranti, S.; Bottacini, F.; Casey, E.; Turroni, F.; Mahony, J.; Belzer, C.; Delgado Palacio, S.; Arboleya Montes, S.; Mancabelli, L.; et al. The First Microbial Colonizers of the Human Gut: Composition, Activities, and Health Implications of the Infant Gut Microbiota. Microbiol. Mol. Biol. Rev. 2017, 81, 1–67. [Google Scholar] [CrossRef] [Green Version]
- Harmsen, H.J.M.; Wildeboer–Veloo, A.C.M.; Raangs, G.C.; Wagendorp, A.A.; Klijn, N.; Bindels, J.G.; Welling, G.W. Analysis of Intestinal Flora Development in Breast-Fed and Formula-Fed Infants by Using Molecular Identification and Detection Methods. J. Pediatr. Gastroenterol. Nutr. 2000, 30, 61–67. [Google Scholar] [CrossRef]
- Stark, P.L.; Lee, A. The microbial ecology of the large bowel of breast-fed and formula-fed infants during the first year of life. J. Med. Microbiol. 1982, 15, 189–203. [Google Scholar] [CrossRef]
- Lundgren, S.N.; Madan, J.C.; Emond, J.A.; Morrison, H.G.; Christensen, B.C.; Karagas, M.R.; Hoen, A.G. Maternal diet during pregnancy is related with the infant stool microbiome in a delivery mode-dependent manner. Microbiome 2018, 6, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bezirtzoglou, E.; Tsiotsias, A.; Welling, G.W. Microbiota profile in feces of breast- and formula-fed newborns by using fluorescence in situ hybridization (FISH). Anaerobe 2011, 17, 478–482. [Google Scholar] [CrossRef]
- Goldwater, P.N. Gut microbiota and immunity: Possible role in sudden infant death syndrome. Front. Immunol. 2015, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saegeman, V.; Cohen, M.C.; Alberola, J.; Ziyade, N.; Farina, C.; Achour, W.; Andréoletti, L.; Arribi, A.; Bazaj, A.; Elgormüs, N.; et al. How is post-mortem microbiology appraised by pathologists? Results from a practice survey conducted by ESGFOR. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1381–1385. [Google Scholar] [CrossRef] [PubMed]
- Fernández-rodríguez, A.; Alberola, J.; Cecilia, M. Análisis microbiológico post mórtem. Enferm. Infecc. Y Microbiol. Clínica 2013, 31, 685–691. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| . | SUDA | SUDC | SUDI | SIDS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tuomisto et al. [50]] | Prtak et al. [51] | Burger et al. [52] | Weber et al. [53] | Weber et al. [54] | Weber et al. [55] | Vargas et al. [56] | Yagmur et al. [57] | Álvarez-Lafuente et al. [58] | Stray-Pedersen et al. [59] | Pearce et al. [60] | Highet and Goldwater [61] | Highet et al. [62] | Gaaloul et al. [63] | Leong et al. [64] | |
| Address a clearly focused issue |  | | | | | | | | | | | | | | |
| Acceptable cohort recruitment | | | | | | | | |  | | | | | | |
| Exposure accurately measured | | | | | | | | | | | | | | | |
| Outcome accurately measured | | | | | | | | | | | | | | | |
| Important confounding factors identified | | | | | | | | | | | | | | | |
| Important confounding factors accounted for | | | | | | | | | | | | | | | |
| Precise results | | | | | | | | | | | | | | | |
| Believable results | | | | | | | | | | | | | | | |
| Results fit with other available data | | | | | | | | | | | | | | | |
| Overall quality score | | | | | | | | |  | | | | | | |
| References | Analysis Techniques | |||||
|---|---|---|---|---|---|---|
| Bacteriological Culture | PCR | RT-PCR | q-PCR | ELISA | 16S rRNA Gene Sequencing | |
| Sudden Unexpected Death in Adults (SUDA) | ||||||
| Tuomisto et al. [50] | ✓ | |||||
| Sudden Unexplained Death in Childhood (SUDIC) | ||||||
| Prtak et al. [51] | ✓ | |||||
| Burger et al. [52] | ✓ | |||||
| Sudden Unexpected Death in Infants (SUDI) | ||||||
| Weber et al. [53] | ✓ | |||||
| Weber et al. [54] | ✓ | |||||
| Weber et al. [55] | ✓ | |||||
| Vargas et al. [56] | ✓ | |||||
| Yagmur et al. [57] | ✓ | |||||
| Sudden Infant Death Syndrome (SIDS) | ||||||
| Álvarez-Lafuente et al. [58] | ✓ | |||||
| Stray Pedersen et al. [59] | ✓ | |||||
| Pearce et al. [60] | ✓ | |||||
| Highet and Goldwater [61] | ✓ | |||||
| Highet et al. [62] | ✓ | |||||
| Gaaloul et al. [63] | ✓ | |||||
| Leong et al. [64] | ✓ | |||||
| References | n | Age (Range) * | Sex (M/F) | Clinical Variables | Population Analyzed | Type of Sample | Microbiota Detected |
|---|---|---|---|---|---|---|---|
| Sudden Unexpected Death in Adults (SUDA) | |||||||
| Tuomisto et al. [50] | 67 | 18–95 | M | No signs of bacterial infections or drug addiction. | Finland | Feces and coronary plaques | Bacteroides spp., Bifidobacterium spp., Clostridium leptum group, Clostridium coccoides group, Enterobacteriaceae, Streptococcus spp., and Lactobacillus spp. |
| Sudden Unexplained Death in Childhood (SUDC) | |||||||
| Prtak et al. [51] | 116 | 0–24 | n.i. | n.i. | United Kingdom | Blood cardiac, cerebrospinal fluid (CSF), bronchial swab, lung swab, lung tissue, nasopharyngeal aspirate | Streptococcus pneumoniae, Haemophilus sp., S. aureus, Escherichia coli, Beta-haemolytic streptococcus group A, Beta-haemolytic streptococcus group B, Haemolyticstreptococcus, Moraxella sp., Leuconostoc sp., Pseudomonas sp., Bordetella pertussis, Mycobacterium bovis (BCG), Neisseria meningitidis, Clostridium septicum, Ureaplasma and Candida sp. |
| Burger et al. [52] | 82 | 0–13 | M/F | Bed-sharing (65%); smoke parents (29%); prematurity (27%); alcohol parents and prone position (24%) | South Africa | Lung tissue | Adenovirus, Cytomegalovirus, Respiratory syncytial virus. |
| Sudden Unexpected Death in Infants (SUDI) | |||||||
| Weber et al. [53] | 507 | 0–12 | n.i. | n.i. | United Kingdom | Cardiac blood, cerebrospinal fluid (CSF), lung and spleen | Staphylococcus aureus, Escherichia coli, Beta-haemolytic streptococcus group A Beta-hemolytic streptococcus group B, Streptococcus pneumoniae, Neisseria meningitidis |
| Weber et al. [54] | 490 | 0–12 | n.i. | n.i. | United Kingdom | Lung tissue | Adenovirus, Influenza Virus, Parainfluenza Virus, Respiratory Syncytial Virus, Measles Virus, Cytomegalovirus, and Enterovirus |
| Weber et al. [55] | 507 | 0–12 | n.i. | n.i. | United Kingdom | n.i. | Staphylococcus aureus toxins |
| Vargas et al. [56] | 128 | 0–12 | n.i. | n.i. | Chile | Lung tissue | Pneumocystis jirovecii |
| Yagmur et al. [57] | 39 | 0–12 | M/F | n.i. | Turkey | Blood, cerebrospinal fluid (CSF), lung, spleen, stool, and tracheal swab. | Cytomegalovirus |
| Sudden Infant Death Syndrome (SIDS) | |||||||
| Álvarez-Lafuente et al., [58] | 11 | 1–5 | n.i. | No previous infections | Spain | Lung, brain, kidney, and spleen tissues | Herpesvirus-6, Epstein-Bar virus, and Cytomegalovirus |
| Stray Pedersen et al. [59] | 160 | 0–12 | M/F | n.i. | Norway | Fecal, cerebrospinal fluid, and gastric antrum tissue | Helicobacter pilory |
| Pearce et al. [60] | 231 | n.i. | n.i. | n.i. | Australia | Fecal | Different serotypes of Escherichia coli |
| Highet and Goldwater [61] | 57 | 0–12 | M/F | Anybody used antibiotics before death. | Australia | Intestine | Staphylococcus aureus |
| Highet et al. [62] | 52 | 3–52 | M/F | Anybody used antibiotics before death. | Australia | Intestine | Clostridium perfringens, Clostridium difficile, Clostridium innocuum, Bacteroides thetaiotamicron, and Staphylococcus aureus |
| Gaaloul et al. [63] | 39 | 3–9 | M/F | Mild fever and insomnia for a few days before death. | Tunisia | Heart and pericardial fluids | Enterovirus CV-B3 |
| Leong et al. [64] | 44 | 0–12 | M/F | n.i. | Australia | Fecal | Bacteria to the orders Clostridiales, Bacteroidales, Lactobacillales, Enterobacteriales, Bifidobacteriales |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collados-Ros, A.; Pérez-Cárceles, M.D.; Legaz, I. Is There a Role for the Microbiome and Sudden Death? A Systematic Review. Life 2021, 11, 1345. https://doi.org/10.3390/life11121345
Collados-Ros A, Pérez-Cárceles MD, Legaz I. Is There a Role for the Microbiome and Sudden Death? A Systematic Review. Life. 2021; 11(12):1345. https://doi.org/10.3390/life11121345
Chicago/Turabian StyleCollados-Ros, Aurelia, María D. Pérez-Cárceles, and Isabel Legaz. 2021. "Is There a Role for the Microbiome and Sudden Death? A Systematic Review" Life 11, no. 12: 1345. https://doi.org/10.3390/life11121345