
Cardiovascular Surgical Emergencies in France, before, during and after the First Lockdown for COVID-19 in 2020: A Comparative Nationwide Retrospective Cohort Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Hospitalization Data
2.2. Study Design
2.3. Statistical Analysis
2.4. Patient and Public Involvement
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hartnett, K.P.; Kite-Powell, A.; DeVies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; National Syndromic Surveillance Program Community of Practice. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, 1 January 2019–30 May 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Pasea, L.; Harris, S.; Gonzalez-Izquierdo, A.; Torralbo, A.; Shallcross, L.; Noursadeghi, M.; Pillay, D.; Sebire, N.; Holmes, C.; et al. Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: A population-based cohort study. Lancet 2020, 395, 1715–1725. [Google Scholar] [CrossRef]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. COVID-19 and Cardiovascular Disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gong, F.F.; Vaitenas, I.; Malaisrie, S.C.; Maganti, K. Mechanical Complications of Acute Myocardial Infarction: A Review. JAMA Cardiol. 2021, 6, 341–349. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.F.; Czerny, M.; De Carlo, M.; Debus, S.; et al. Editor’s Choice—2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2018, 55, 305–368. [Google Scholar] [CrossRef] [Green Version]
- Riambau, V.; Böckler, D.; Brunkwall, J.; Cao, P.; Chiesa, R.; Coppi, G.; Czerny, M.; Fraedrich, G.; Haulon, S.; Jacobs, M.J.; et al. Editor’s Choice—Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 4–52. [Google Scholar] [CrossRef] [Green Version]
- Fried Justin, A.; Ramasubbu Kumudha Bhatt Reema Topkara Veli, K.; Clerkin Kevin, J.; Horn, E.; Rabbani, L.; Brodie, D.; Jain, S.S.; Kirtane, A.J.; Masoumi, A. The Variety of Cardiovascular Presentations of COVID-19. Circulation 2020, 141, 1930–1936. [Google Scholar] [CrossRef] [Green Version]
- Cano-Valderrama, O.; Morales, X.; Ferrigni, C.J.; Martín-Antona, E.; Turrado, V.; García, A.; Cuñarro-López, Y.; Zarain-Obrador, L.; Duran-Poveda, M.; Balibrea, J.M.; et al. Acute Care Surgery during the COVID-19 pandemic in Spain: Changes in volume, causes and complications. A multicentre retrospective cohort study. Int. J. Surg. 2020, 80, 157–161. [Google Scholar] [CrossRef]
- Bhatt, A.S.; Moscone, A.; McElrath, E.E.; Varshney, A.S.; Claggett, B.L.; Bhatt, D.L.; Januzzi, J.L.; Butler, J.; Adler, D.S.; Solomon, S.D.; et al. Fewer Hospitalizations for Acute Cardiovascular Conditions During the COVID-19 Pandemic. J. Am. Coll. Cardiol. 2020, 76, 280–288. [Google Scholar] [CrossRef]
- Nef, H.M.; Elsässer, A.; Möllmann, H.; Abdel-Hadi, M.; Bauer, T.; Brück, M.; Eggebrecht, H.; Ehrlich, J.R.; Ferrari, M.W.; Fichtlscherer, S.; et al. Impact of the COVID-19 pandemic on cardiovascular mortality and catherization activity during the lockdown in central Germany: An observational study. Clin. Res. Cardiol. 2021, 110, 292–301. [Google Scholar] [CrossRef]
- Mesnier, J.; Cottin, Y.; Coste, P.; Ferrari, E.; Schiele, F.; Lemesle, G.; Thuaire, C.; Angoulvant, D.; Cayla, G.; Bouleti, C.; et al. Hospital admissions for acute myocardial infarction before and after lockdown according to regional prevalence of COVID-19 and patient profile in France: A registry study. Lancet Public Health 2020, 5, e536–e542. [Google Scholar] [CrossRef]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; Mamas, M.A.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Ball, S.; Banerjee, A.; Berry, C.; Boyle, J.R.; Bray, B.; Bradlow, W.; Chaudhry, A.; Crawley, R.; Danesh, J.; Denniston, A.; et al. Monitoring indirect impact of COVID-19 pandemic on services for cardiovascular diseases in the UK. Heart 2020, 106, 1890–1897. [Google Scholar] [CrossRef]
- Stabile, E.; Piccolo, R.; Franzese, M.; Accarino, G.; Bracale, U.M.; Cappello, E.; Cioffi, G.; Cioppa, A.; Crinisio, A.; Flora, L.; et al. A cross-sectional study evaluating hospitalization rates for chronic limb-threatening ischemia during the COVID-19 outbreak in Campania, Italy. Vasc. Med. 2020, 26, 174–179. [Google Scholar] [CrossRef]
- Aljarrah, Q.; Allouh, M.; Hallak, A.; Al-Omari, M.; Mesmar, Z.; Kamel, A.; Husein, A.; Manasreh, T.; Bakkar, S.; Jarboa, H. Impact of the COVID-19 pandemic on the management of chronic limb-threatening ischemia in Northern Jordan: Case series and literature review. Int. J. Surg. Case Rep. 2021, 80, 105631. [Google Scholar] [CrossRef]
- Mariet, A.-S.; Giroud, M.; Benzenine, E.; Cottenet, J.; Roussot, A.; Aho-Glélé, L.S.; Tubert-Bitter, P.; Béjot, Y.; Quantin, C. Hospitalizations for Stroke in France During the COVID-19 Pandemic Before, During, and After the National Lockdown. Stroke 2021, 52, 1362–1369. [Google Scholar] [CrossRef]
- Ho, V.T.; Eberhard, A.V.; Asch, S.M.; Leeper, N.J.; Fukaya, E.; Arya, S.; Gyang Ross, E. US National Trends in Vascular Surgical Practice During the COVID-19 Pandemic. JAMA Surg. 2021, 156, 681. [Google Scholar] [CrossRef]
- McLean, R.C.; Young, J.; Musbahi, A.; Lee, J.X.; Hidayat, H.; Abdalla, N.; Chowdhury, S.; Baker, E.A.; Etherson, K.J. A single-centre observational cohort study to evaluate volume and severity of emergency general surgery admissions during the COVID-19 pandemic: Is there a «lockdown» effect? Int. J. Surg. 2020, 83, 259–266. [Google Scholar] [CrossRef]
- El-Hamamsy, I.; Brinster, D.R.; DeRose, J.J.; Girardi, L.N.; Hisamoto, K.; Imam, M.N.; Itagaki, S.; Kurlansky, P.A.; Lau, C.; Nemeth, S.; et al. The COVID-19 Pandemic and Acute Aortic Dissections in New York. J. Am. Coll. Cardiol. 2020, 76, 227–229. [Google Scholar] [CrossRef]
- Murana, G.; Folesani, G.; Botta, L.; Marco, L.; Leone, A.; Loforte, A.; Pacini, D. The effect of COVID-19 lockdown on acute type A aortic dissection: Insights from Bologna. JTCVS Tech. 2020, 4, 50–54. [Google Scholar] [CrossRef]
- Kasdi, R.; Corbineau, H.; Harmouche, M.; Langanay, T.; De Latour, B.R.; Leguerrier, A.; Flecher, E.; Verhoye, J.P. Influence des Saisons et des Pressions Atmosphériques sur la Survenue de Dissections Aortiques et de Ruptures D’anévrismes Aortiques. Étude Rétrospective et Revue de la Littérature. JCTCV:22(1)2018. Available online: http://journal.sfctcv.org/2018/05/influence-des-saisons-et-des-pressions-atmospheriques-sur-la-survenue-de-dissections-aortiques-et-de-ruptures-danevrismes-aortiques-etude-retrospective-et-revue-de-la-litterature/ (accessed on 21 April 2021).
- Chaudhry, S.-P.; Salerno, C.T.; Ravichandran, A.K.; Walsh, M.N. Shared Decision Making in Cardiac Transplantation During the COVID-19 Pandemic: Patient Refusal of Transplantation. JACC Case Rep. 2020, 2, 1365–1367. [Google Scholar] [CrossRef]
- Legeai, C.; Malaquin, G.; Lamotte, C.; Antoine, C.; Averland, B.; Jasseron, C.; Bayer, F.; Bastien, O.; Kerbaul, F. Impact of coronavirus disease 2019 on organ donation and transplantation in France. Transpl. Int. 2021, 34, 204–206. [Google Scholar] [CrossRef]
- Baril, D.T.; Ghosh, K.; Rosen, A.B. Trends in the incidence, treatment, and outcomes of acute lower extremity ischemia in the United States Medicare population. J. Vasc. Surg. 2014, 60, 669–677.e2. [Google Scholar] [CrossRef] [Green Version]
- Grip, O.; Wanhainen, A.; Michaëlsson, K.; Lindhagen, L.; Björck, M. Open or endovascular revascularization in the treatment of acute lower limb ischaemia. Br. J. Surg. 2018, 105, 1598–1606. [Google Scholar] [CrossRef] [Green Version]
- Napoli, C.; Tritto, I.; Benincasa, G.; Mansueto, G.; Ambrosio, G. Cardiovascular involvement during COVID-19 and clinical implications in elderly patients. A review. Ann. Med. Surg. 2020, 57, 236–243. [Google Scholar] [CrossRef]
- Ramanathan, K.; Antognini, D.; Combes, A.; Paden, M.; Zakhary, B.; Ogino, M.; MacLaren, G.; Brodie, D.; Shekar, K. Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir. Med. 2020, 8, 518–526. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, B.; Troncone, M.; James, L.P.; Bisch, S.P.; Iyer, V. Reassessing the operative threshold for abdominal aortic aneurysm repair in the context of COVID-19. J. Vasc. Surg. 2021, 73, 780–788. [Google Scholar] [CrossRef]
- Tomasoni, D.; Adamo, M.; Italia, L.; Branca, L.; Chizzola, G.; Fiorina, C.; Lupi, L.; Inciardi, R.M.; Cani, D.S.; Lombardi, C.M.; et al. Impact of COVID-2019 outbreak on prevalence, clinical presentation and outcomes of ST-elevation myocardial infarction. J. Cardiovasc. Med. 2020, 21, 874–881. [Google Scholar] [CrossRef]
- Bryndza, M.A.; Litwinowicz, R.; Bartuś, S.; Nosal, M.; Godlewski, J.; Orzechowska, A.; Wiśniewski, A.; Korpak-Wysocka, R.; Rzeszutko, L.; Kocik, P.; et al. Incidence of mechanical complications following myocardial infarction during the first two months of the COVID-19 pandemic in the Southern Poland region: A multicenter study. Kardiol. Pol. 2020, 79, 66–68. [Google Scholar] [CrossRef]
- Banerjee, A.; Chen, S.; Pasea, L.; Lai, A.G.; Katsoulis, M.; Denaxas, S.; Nafilyan, V.; Williams, B.; Wong, W.K.; Bakhai, A.; et al. Excess deaths in people with cardiovascular diseases during the COVID-19 pandemic. Eur. J. Prev. Cardiol. 2021, zwaa155. [Google Scholar] [CrossRef]
- Committee, T.V.; Ern, E. The COvid-19 Vascular Service (COVER) Study: An International Vascular and Endovascular Research Network (VERN) Collaborative Study Assessing the Provision, Practice, and Outcomes of Vascular Surgery During the COVID-19 Pandemic. Eur. J. Vasc. Endovasc. Surg. 2020, 60, 156–157. [Google Scholar]
- D’Oria, M.; Mills, J.L.; Cohnert, T.; Oderich, G.S.; Hultgren, R.; Lepidi, S. The “Vascular Surgery COVID-19 Collaborative” (VASCC). Eur. J. Vasc. Endovasc. Surg. 2020, 60, 489–490. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Before Lockdown | During Lockdown | After Lockdown | Maximal Variation | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2019 | 2020 | Variation | 2019 | 2020 | Variation | 2019 | 2020 | Variation | % | Week | |
| Cardiac conditions | |||||||||||
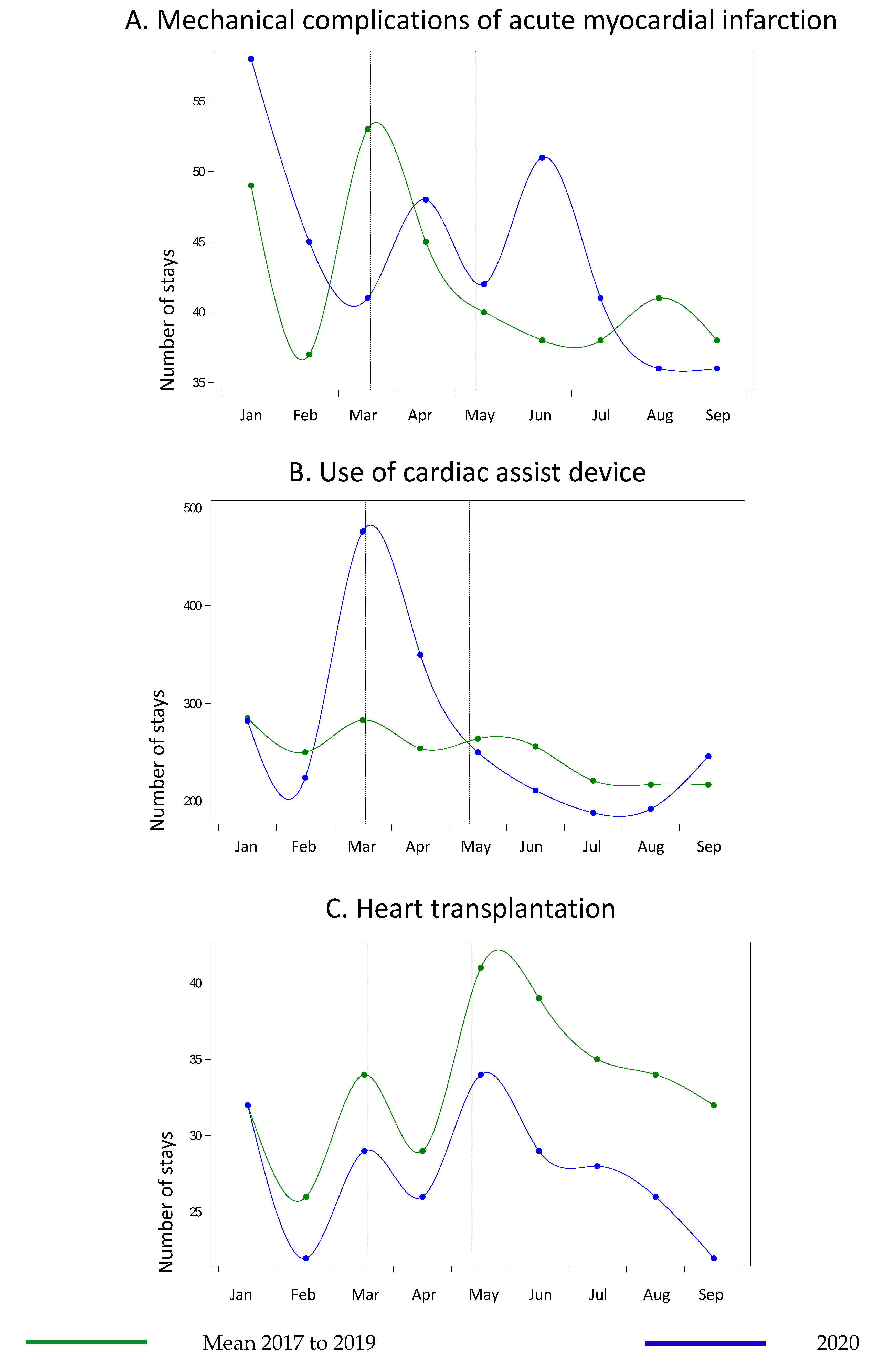
| Complications of myocardial infarction | 104 | 108 | 3.8% | 83 | 83 | 0.0% | 200 | 194 | −3.0% | 171.4% | 20 |
| Use of circulatory assistance | 651 | 634 | −2.6% | 462 | 749 | 62.1% | 1036 | 961 | −7.2% | 138.8% | 13 |
| Heart transplantation | 69 | 68 | −1.4% | 61 | 51 | −16.4% | 165 | 123 | −25.5% | −83.3% | 37 |
| Aortic conditions | |||||||||||
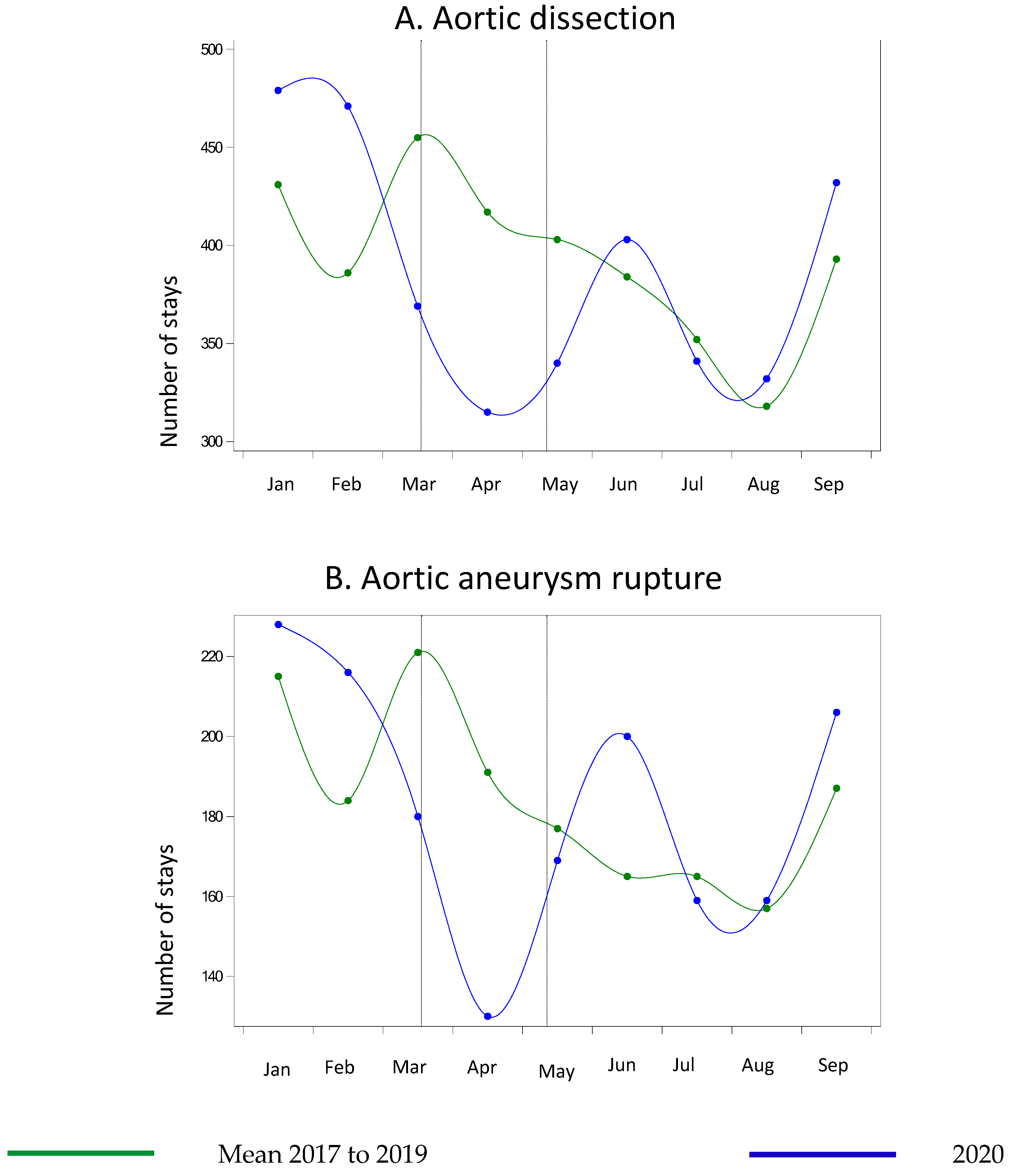
| Aortic dissection | 984 | 1123 | 14.1% | 841 | 556 | −33.9% | 1767 | 1673 | −5.3% | −56.1% | 11 |
| Aortic aneurysm rupture | 475 | 516 | 8.6% | 330 | 265 | −19.7% | 782 | 808 | 3.3% | −42.5% | 14 |
| Peripheral vascular conditions | |||||||||||
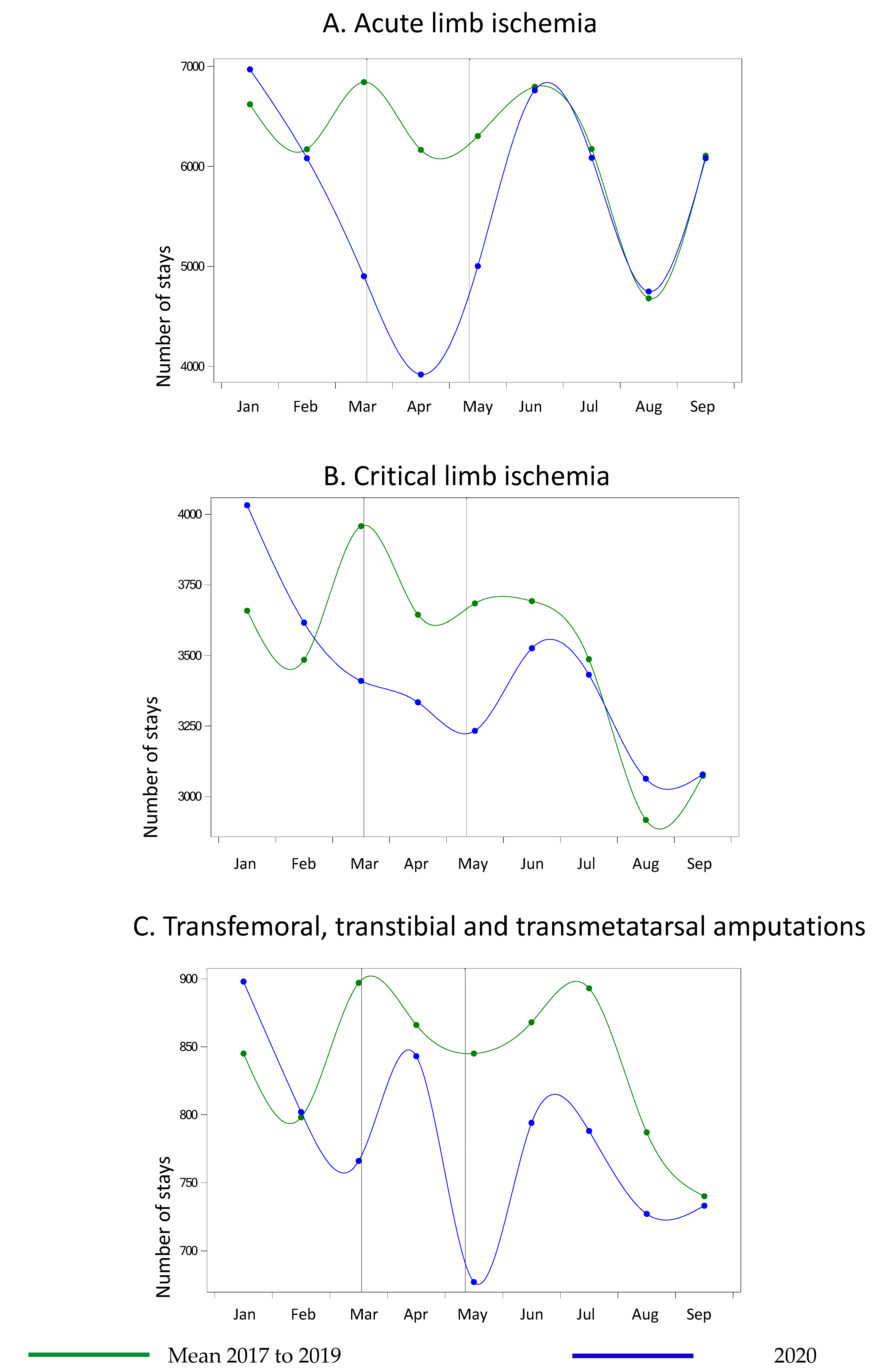
| Acute limb ischemia | 15,828 | 15,348 | −3.0% | 11,729 | 7072 | −39.7% | 27,479 | 26,580 | −3.3% | −50.7% | 12 |
| Critical limb ischemia | 9154 | 8991 | −1.8% | 7006 | 5853 | −16.5% | 15,742 | 14,985 | −4.8% | −34.5% | 12 |
| Amputations | 2012 | 1955 | −2.8% | 1563 | 1439 | −7.9% | 3732 | 3435 | −8.0% | −25.9% | 12 |
| 2017–2019 N (%) or Median [IQR] | 2020 N (%) or Median [IQR] | p Value Univariable Logistic Regression a | p Value Multivariable Logistic Regression | |
|---|---|---|---|---|
| Complications of myocardial infarction | N = 137 | N = 48 | ||
| Age (years): continuous | 71 (60–83) | 67.5 (57.5–77.5) | 0.05 a | |
| Classes: | 0.50 | 0.65 | ||
| [18–65] | 48 (35.0) | 16 (33.3) | ||
| [65–80] | 45 (32.9) | 20 (41.7) | ||
| [80–85] | 18 (13.1) | 7 (14.6) | ||
| ≥85 | 26 (19.0) | 5 (10.4) | ||
| Male | 78 (56.9) | 33 (68.8) | 0.15 | 0.21 |
| Hypertension | 50 (36.5) | 21 (43.8) | 0.37 | 0.23 |
| Diabetes | 20 (14.6) | 4 (8.3) | 0.27 | 0.23 |
| Obesity | 9 (6.6) | 3 (6.3) | 0.94 | 0.93 |
| Atrial fibrillation | 39 (28.5) | 10 (20.8) | 0.30 | 0.36 |
| COVID-19 | 0 (0) | 4 (8.3) | NA | NA |
| Death | 66 (48.2) | 22 (45.8) | 0.78 | 0.99 |
| Use of circulatory assistance | N = 763 | N = 350 | ||
| Age (years): continuous | 58 (47–66) | 55 (46–62) | 0.01 a | |
| Classes: | <0.001 | <0.001 | ||
| [18–65] | 159 (20.8) | 73 (20.9) | ||
| [65–80] | 157 (20.6) | 95 (27.1) | ||
| [80–85] | 227 (29.8) | 128 (36.6) | ||
| ≥85 | 220 (28.8) | 54 (15.4) | ||
| Male | 564 (73.9) | 266 (76.0) | 0.46 | 0.18 |
| Hypertension | 206 (27.0) | 125 (35.7) | 0.003 | 0.05 |
| Diabetes | 148 (19.4) | 77 (22.0) | 0.32 | 0.33 |
| Obesity | 95 (12.5) | 119 (34.0) | <0.001 | <0.001 |
| Atrial fibrillation | 209 (27.4) | 65 (18.6) | 0.002 | <0.001 |
| COVID-19 | 0 (0) | 223 (63.7) | NA | NA |
| Death | 426 (55.8) | 167 (47.7) | 0.01 | 0.10 |
| Heart transplantation | N = 87 | N = 26 | ||
| Age (years): continuous | 54 (43–61) | 52.5 (43–56) | 0.40 a | |
| Classes: | 0.15 | 0.15 | ||
| [18–65] | 30 (34.5) | 8 (30.8) | ||
| [65–80] | 15 (17.2) | 9 (34.6) | ||
| [80–85] | 12 (13.8) | 5 (19.2) | ||
| ≥85 | 30 (34.5) | 4 (15.4) | ||
| Male | 64 (73.6) | 17 (65.4) | 0.42 | 0.31 |
| Hypertension | 24 (27.6) | 5 (19.2) | 0.39 | 0.20 |
| Diabetes | 19 (21.8) | 7 (26.9) | 0.59 | 0.92 |
| Obesity | 7 (8.1) | 5 (19.2) | 0.11 | 0.05 |
| Atrial fibrillation | 29 (33.3) | 9 (34.6) | 0.90 | 0.89 |
| COVID-19 | 0 (0) | 1 (3.9) | NA | NA |
| Death | 19 (21.8) | 5 (19.2) | 0.78 | 0.71 |
| Aortic dissection | N = 1251 | N = 315 | ||
| Age (years): continuous | 69 (59–79) | 71 (60–81) | 0.009 a | |
| Classes: | 0.05 | 0.03 | ||
| [18–65] | 485 (38.8) | 106 (33.6) | ||
| [65–80] | 457 (36.5) | 116 (36.8) | ||
| [80–85] | 128 (10.2) | 49 (15.6) | ||
| ≥85 | 181 (14.5) | 44 (14.0) | ||
| Male | 794 (63.5) | 217 (68.9) | 0.07 | 0.06 |
| Hypertension | 743 (59.4) | 170 (54.0) | 0.08 | 0.03 |
| Diabetes | 95 (7.6) | 42 (13.3) | 0.002 | 0.004 |
| Obesity | 130 (10.4) | 49 (15.6) | 0.01 | 0.007 |
| Atrial fibrillation | 286 (22.9) | 59 (18.7) | 0.11 | 0.04 |
| COVID-19 | 0 (0) | 15 (4.8) | NA | NA |
| Death | 192 (15.4) | 68 (21.6) | 0.008 | 0.03 |
| Aortic aneurysm rupture | N = 574 | N = 130 | ||
| Age (years): continuous | 75 (65–84) | 75 (68–84) | 0.73 a | |
| Classes: | 0.13 | 0.15 | ||
| [18–65] | 139 (24.2) | 21 (16.2) | ||
| [65–80] | 202 (35.2) | 58 (44.6) | ||
| [80–85] | 93 (16.2) | 19 (14.6) | ||
| ≥85 | 140 (24.4) | 32 (24.6) | ||
| Male | 434 (75.6) | 97 (74.6) | 0.81 | 0.72 |
| Hypertension | 265 (46.2) | 61 (46.9) | 0.88 | 0.55 |
| Diabetes | 56 (9.8) | 14 (10.8) | 0.73 | 0.80 |
| Obesity | 44 (7.7) | 6 (4.6) | 0.23 | 0.26 |
| Atrial fibrillation | 120 (20.9) | 24 (18.5) | 0.53 | 0.48 |
| COVID-19 | 0 (0) | 8 (6.2) | NA | NA |
| Death | 203 (35.4) | 54 (41.5) | 0.18 | 0.25 |
| Acute limb ischemia | N = 18,496 | N = 3919 | ||
| Age (years): continuous | 71 (62–81) | 72 (63–83) | <0.001 a | |
| Classes: | <0.001 | 0.01 | ||
| [18–65] | 5938 (32.1) | 1131 (28.9) | ||
| [65–80] | 7204 (39.0) | 1527 (38.9) | ||
| [80–85] | 2165 (11.7) | 478 (12.2) | ||
| ≥85 | 3189 (17.2) | 783 (20.0) | ||
| Male | 12,842 (69.4) | 2669 (68.1) | 0.10 | 0.74 |
| Hypertension | 8094 (43.8) | 1641 (41.9) | 0.03 | <0.001 |
| Diabetes | 4786 (25.9) | 1127 (28.8) | <0.001 | <0.001 |
| Obesity | 1567 (8.5) | 298 (7.6) | 0.07 | 0.14 |
| Atrial fibrillation | 2565 (13.9) | 629 (16.1) | <0.001 | 0.13 |
| COVID-19 | 0 (0) | 198 (5.1) | NA | NA |
| Death | 1073 (5.8) | 366 (9.3) | <0.001 | <0.001 |
| Critical limb ischemia | N = 10,934 | N = 3334 | ||
| Age (years): continuous | 77 (67–85) | 76 (67–85) | 0.02 a | |
| Classes: | 0.13 | 0.24 | ||
| [18–65] | 2122 (19.4) | 632 (19.0) | ||
| [65–80] | 4089 (37.4) | 1322 (39.6) | ||
| [80–85] | 1754 (16.0) | 507 (15.2) | ||
| ≥85 | 2969 (27.2) | 873 (26.2) | ||
| Male | 7465 (68.3) | 2331 (69.9) | 0.07 | 0.16 |
| Hypertension | 5542 (50.7) | 1762 (50.2) | 0.59 | 0.24 |
| Diabetes | 5387 (49.3) | 1700 (51.0) | 0.08 | 0.23 |
| Obesity | 948 (8.7) | 333 (10.0) | 0.02 | 0.03 |
| Atrial fibrillation | 2460 (22.5) | 774 (23.2) | 0.38 | 0.51 |
| COVID–19 | 0 (0) | 177 (5.3) | NA | NA |
| Death | 915 (8.4) | 336 (10.1) | 0.002 | 0.001 |
| Amputations | N = 2600 | N = 843 | ||
| Age (years): continuous | 72 (63–82) | 73 (64–82) | 0.04 a | |
| Classes: | 0.49 | 0.41 | ||
| [18–5] | 736 (28.3) | 226 (26.8) | ||
| [65–80] | 1054 (40.5) | 351 (41.6) | ||
| [80–85] | 372 (14.3) | 110 (13.1) | ||
| ≥85 | 438 (16.9) | 156 (18.5) | ||
| Male | 1955 (75.2) | 643 (76.3) | 0.53 | 0.43 |
| Hypertension | 1218 (46.9) | 399 (47.3) | 0.81 | 0.80 |
| Diabetes | 1422 (54.7) | 472 (56.0) | 0.51 | 0.62 |
| Obesity | 244 (9.4) | 94 (11.2) | 0.13 | 0.13 |
| Atrial fibrillation | 529 (20.4) | 177 (21.0) | 0.68 | 0.99 |
| COVID-19 | 0 (0) | 49 (5.8) | NA | NA |
| Death | 221 (8.5) | 79 (9.4) | 0.44 | 0.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baudry, A.; Mariet, A.-S.; Benzenine, E.; Crespy, V.; Bernard, C.; Morgant, M.-C.; Bejot, Y.; Giroud, M.; Bouchot, O.; Steinmetz, E.; et al. Cardiovascular Surgical Emergencies in France, before, during and after the First Lockdown for COVID-19 in 2020: A Comparative Nationwide Retrospective Cohort Study. Life 2021, 11, 1245. https://doi.org/10.3390/life11111245
Baudry A, Mariet A-S, Benzenine E, Crespy V, Bernard C, Morgant M-C, Bejot Y, Giroud M, Bouchot O, Steinmetz E, et al. Cardiovascular Surgical Emergencies in France, before, during and after the First Lockdown for COVID-19 in 2020: A Comparative Nationwide Retrospective Cohort Study. Life. 2021; 11(11):1245. https://doi.org/10.3390/life11111245
Chicago/Turabian StyleBaudry, Anna, Anne-Sophie Mariet, Eric Benzenine, Valentin Crespy, Chloé Bernard, Marie-Catherine Morgant, Yannick Bejot, Maurice Giroud, Olivier Bouchot, Eric Steinmetz, and et al. 2021. "Cardiovascular Surgical Emergencies in France, before, during and after the First Lockdown for COVID-19 in 2020: A Comparative Nationwide Retrospective Cohort Study" Life 11, no. 11: 1245. https://doi.org/10.3390/life11111245