
Diagnostic Efficacy of Voxel-Mirrored Homotopic Connectivity in Vascular Dementia as Compared to Alzheimer’s Related Neurodegenerative Diseases—A Resting State fMRI Study

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Clinical and Neuropsychological Assessment
2.3. Data Acquisition
2.3.1. T1W Images
2.3.2. Resting State Functional Images
2.3.3. Pre-Processing of Resting State Functional Images
2.3.4. Voxel-Mirrored Homotopic Connectivity VMHC
2.3.5. Leukoaraiosis and Brain Regional Volume Segmentation
2.4. Statistical Analysis
3. Result
3.1. Demographics, Clinical and Neuropsychological Assessments
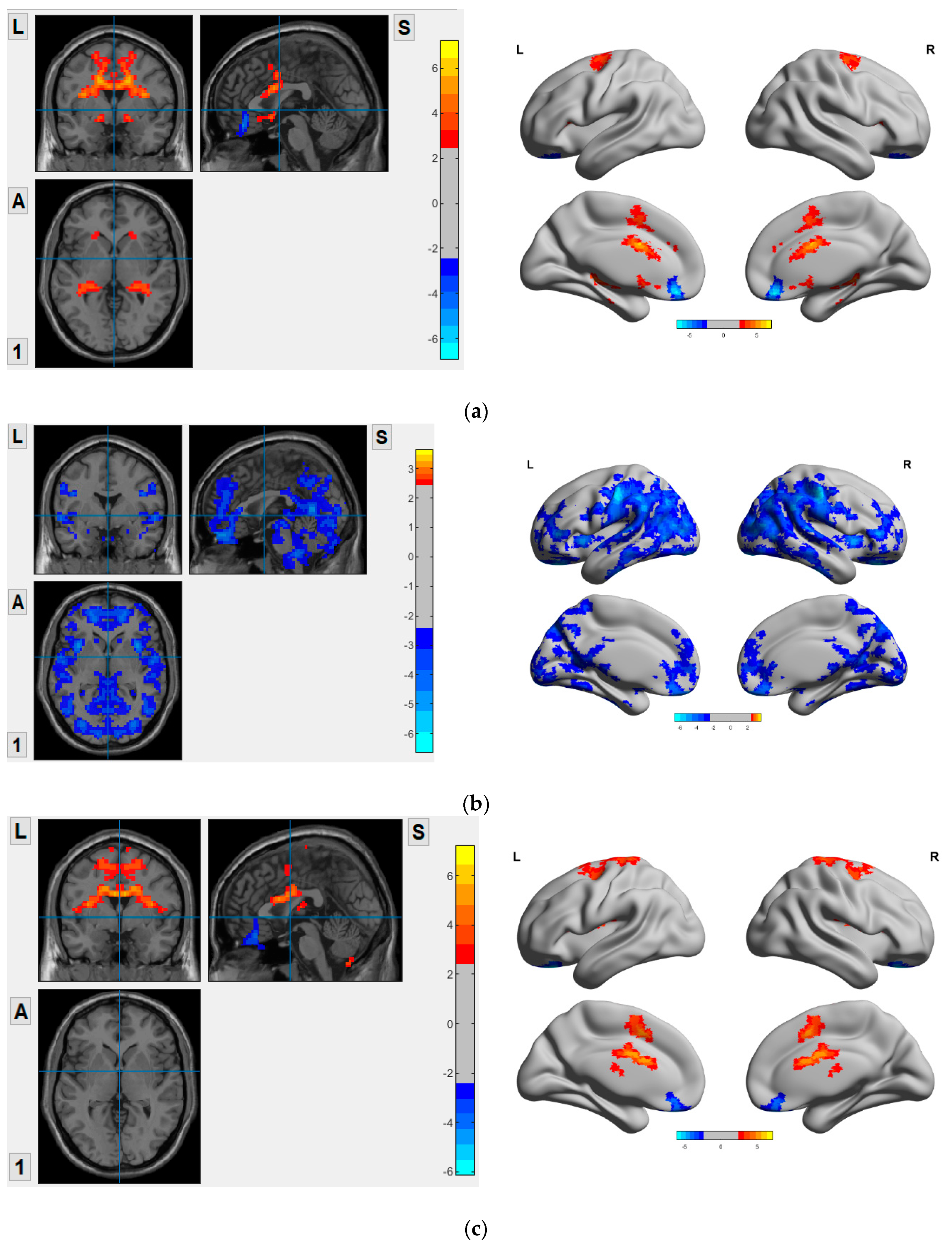
3.2. VMHC Map in VD, AD and MCI Compared to HC
3.3. VMHC Analysis
3.4. Correlation between VMHC Values and Their Corresponding Brain Regional Volumes
3.5. Diagnostic Accuracy of VMHC in Cognitive Impaired Groups
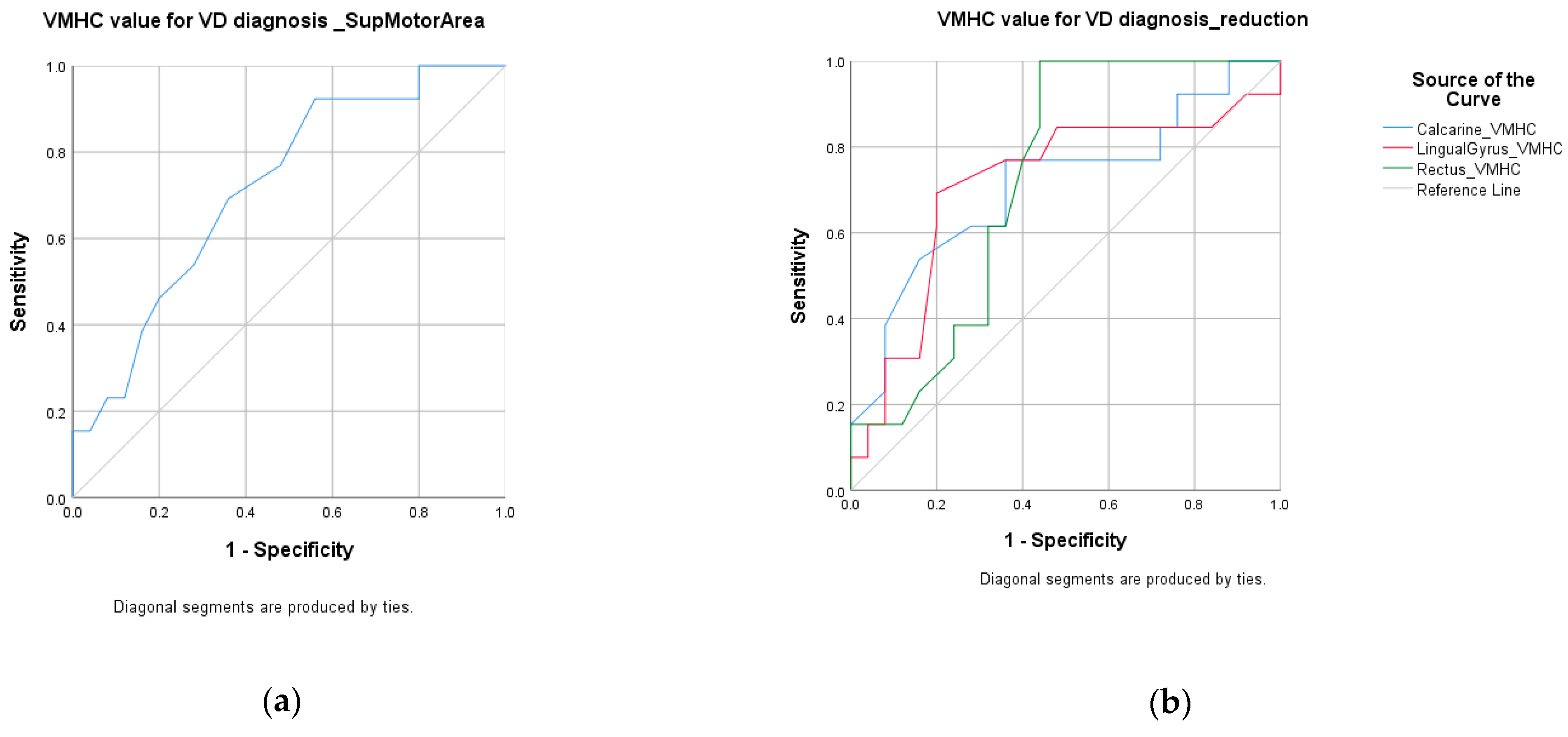
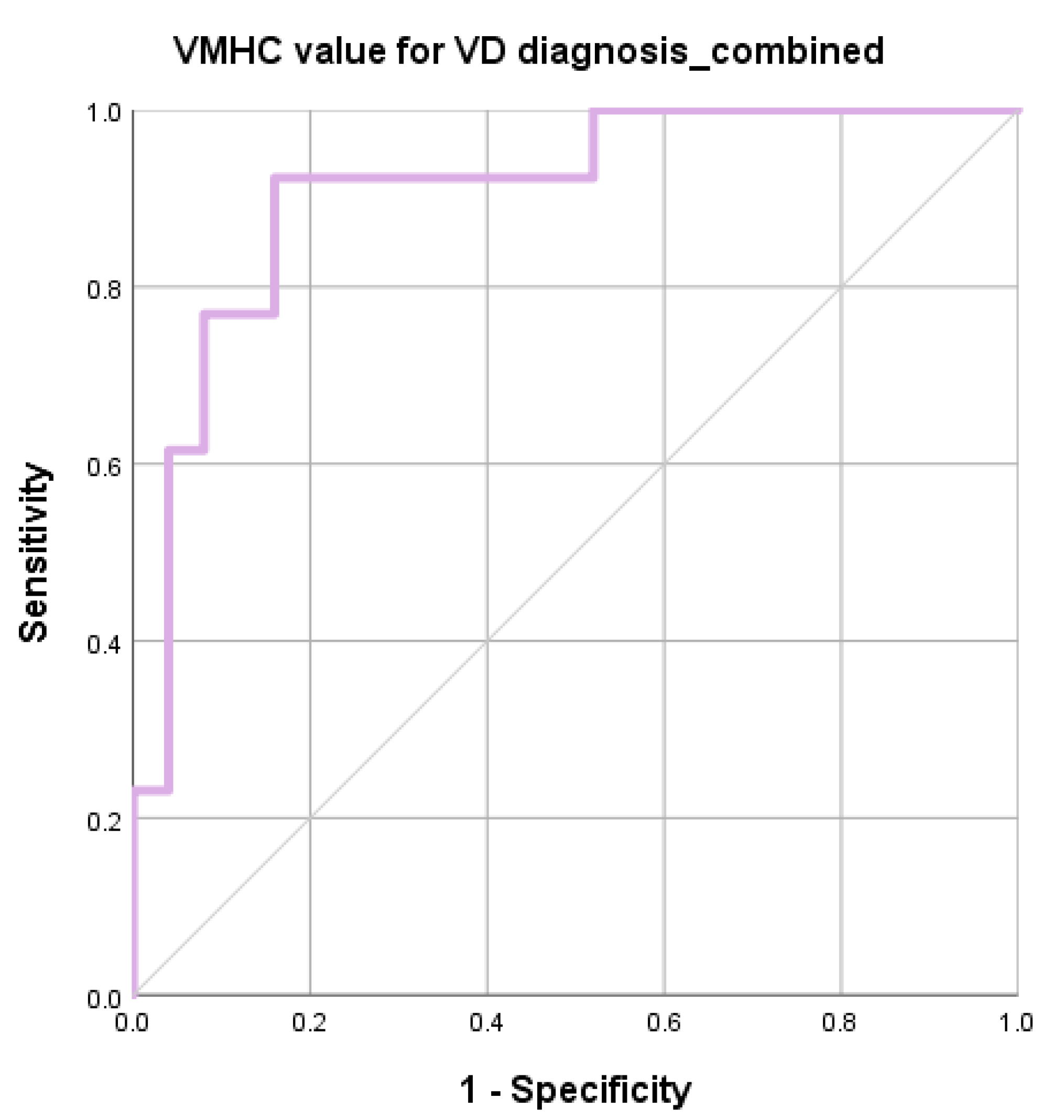
3.5.1. ROC for VD vs. HC
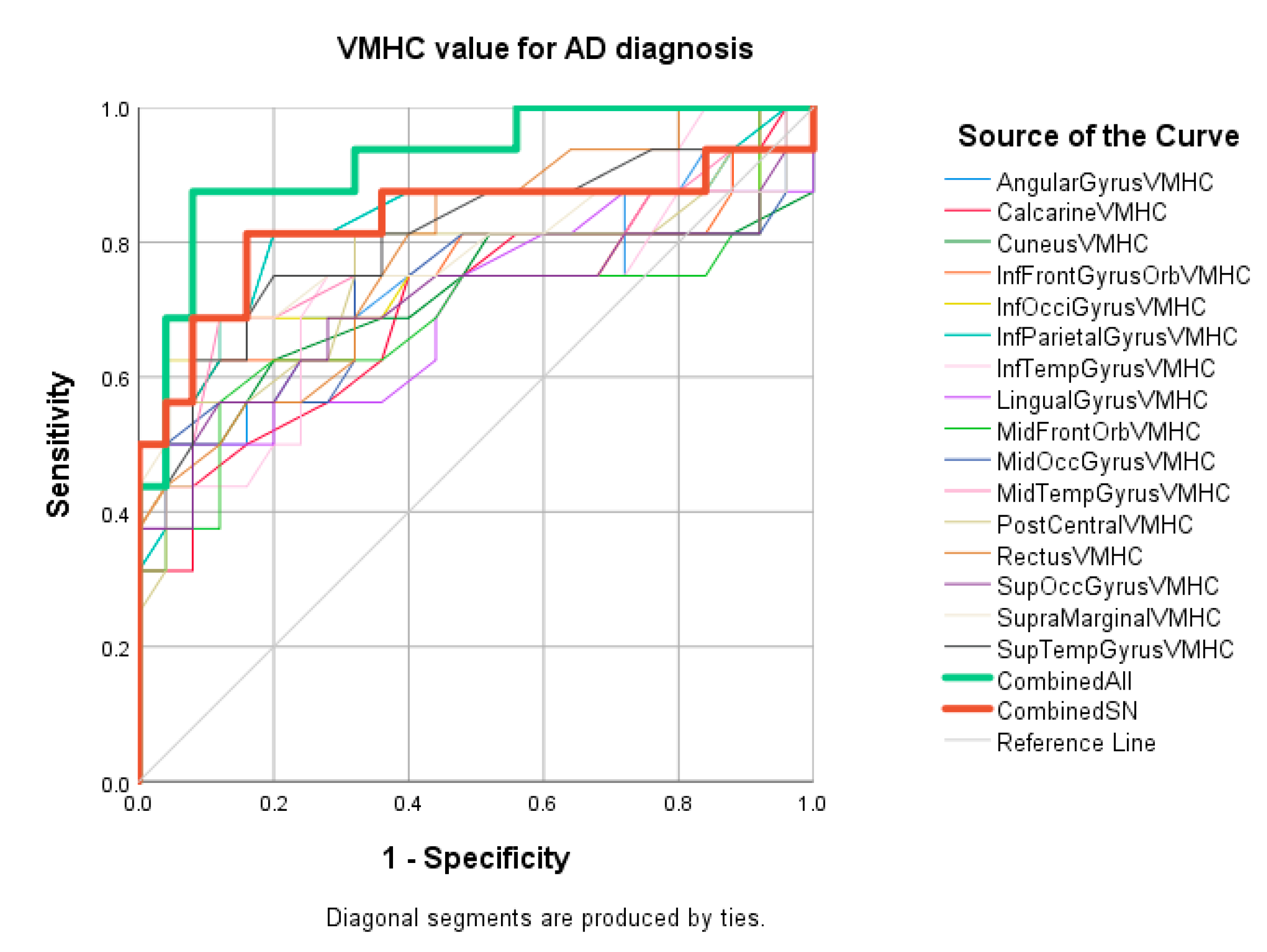
3.5.2. ROC for AD vs. HC
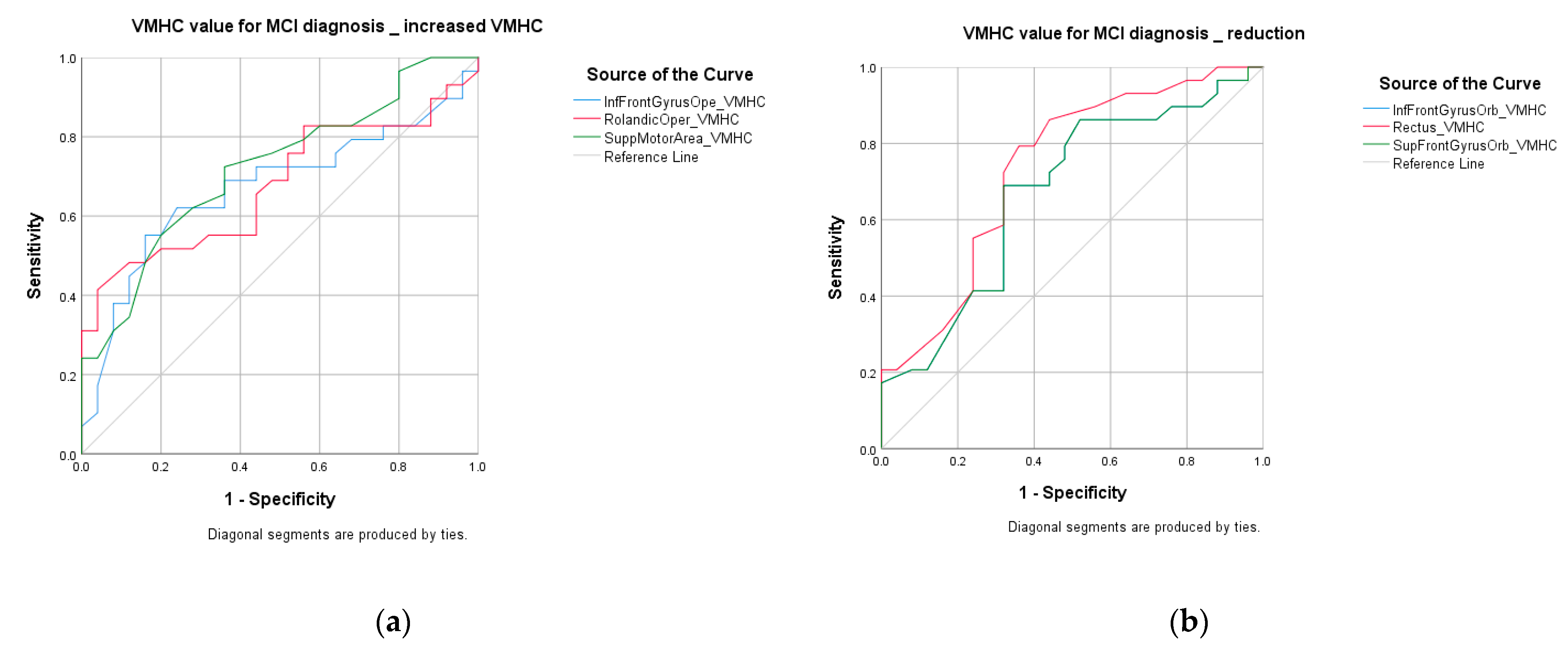
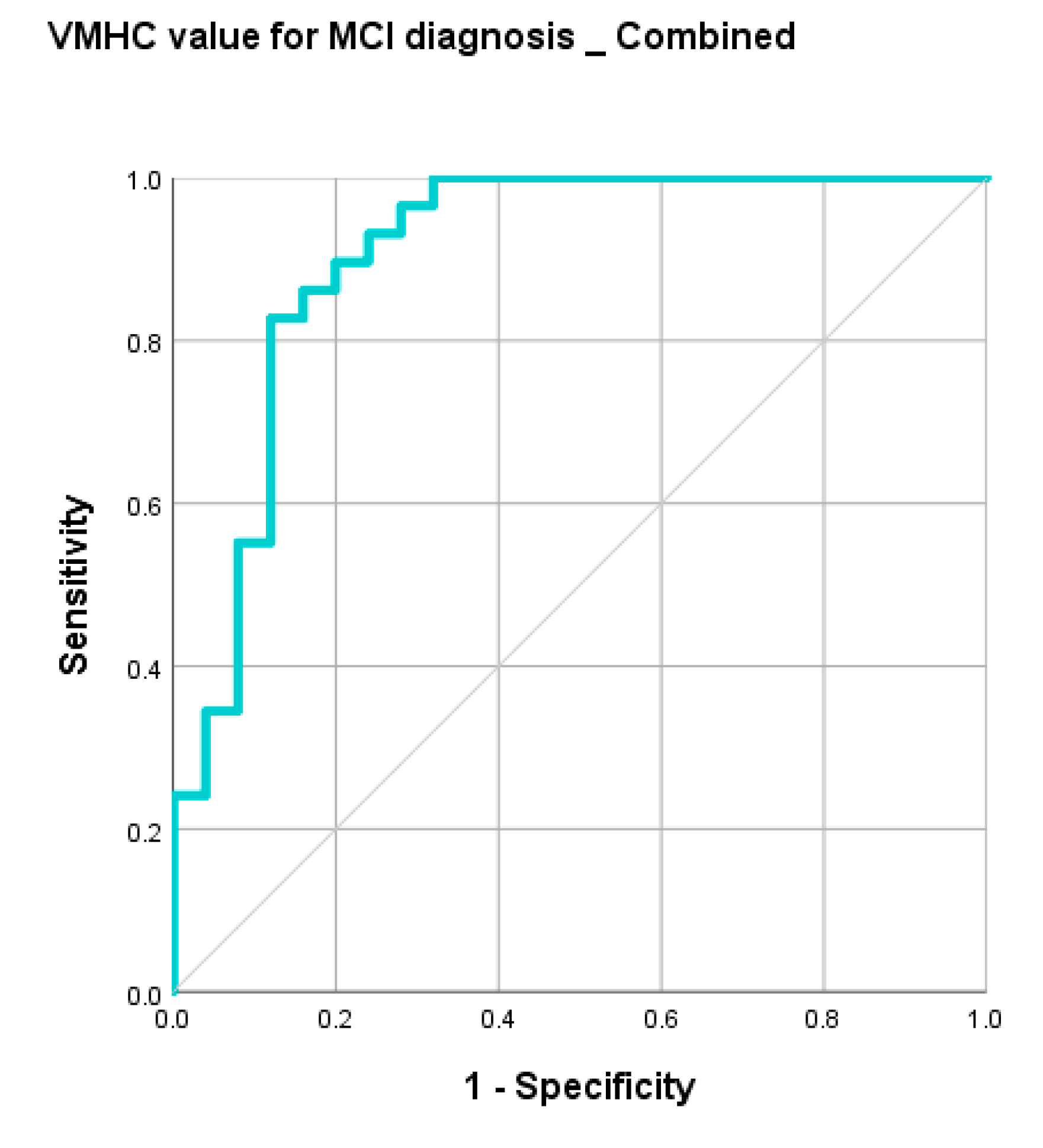
3.5.3. ROC for MCI vs. HC
4. Discussion
4.1. VMHC and Brain Regional Volume Change Are Two Independent Metrics
4.2. Aberrant VMHC in the Cognitive Impaired Groups and Its Diagnostic Accuracy
4.2.1. VD vs. HC
4.2.2. AD vs. HC
4.2.3. MCI vs. HC
4.3. VMHC at Olfactory Network and Salient Network
4.4. Limitations and Future Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prince, M.; Comas-Herrera, A.; Knapp, M.; Guerchet, M.; Karagiannidou, M. World Alzheimer Report 2016; Alzheimer’s Disease International (ADI): London, UK, 2016. [Google Scholar]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current Concepts in Mild Cognitive Impairment. Arch. Neurol. 2001, 58, 1985. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, K.A. Pathology and pathogenesis of vascular cognitive impairment—A critical update. Front. Aging Neurosci. 2013, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devanand, D.P.; Pradhaban, G.; Liu, X.; Khandji, A.; De Santi, S.; Segal, S.; Rusinek, H.; Pelton, G.H.; Honig, L.S.; Mayeux, R.; et al. Hippocampal and entorhinal atrophy in mild cognitive impairment: Prediction of Alzheimer disease. Neurology 2007, 68, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Cherbuin, N.; Anstey, K.J.; Réglade-Meslin, C.; Sachdev, P.S. In Vivo Hippocampal Measurement and Memory: A Comparison of Manual Tracing and Automated Segmentation in a Large Community-Based Sample. PLoS ONE 2009, 4, e5265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Flores, R.; La Joie, R.; Chételat, G. Structural imaging of hippocampal subfields in healthy aging and Alzheimer’s disease. Neuroscience 2015, 309, 29–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moodley, K.K.; Chan, D. The hippocampus in neurodegenerative disease. Front. Neurol. Neurosci. 2014, 34, 95–108. [Google Scholar]
- Chételat, G.; Arbizu, J.; Barthel, H.; Garibotto, V.; Law, I.; Morbelli, S.; van de Giessen, E.; Agosta, F.; Barkhof, F.; Brooks, D.J.; et al. Amyloid-PET and 18F-FDG-PET in the diagnostic investigation of Alzheimer’s disease and other dementias. Lancet Neurol. 2020, 19, 951–962. [Google Scholar] [CrossRef]
- Villemagne, V.L.; Burnham, S.; Bourgeat, P.; Brown, B.; Ellis, K.A.; Salvado, O.; Szoeke, C.; Macaulay, S.L.; Martins, R.; Maruff, P.; et al. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: A prospective cohort study. Lancet Neurol. 2013, 12, 357–367. [Google Scholar] [CrossRef]
- Thal, D.R.; Beach, T.G.; Zanette, M.; Heurling, K.; Chakrabarty, A.; Ismail, A.; Smith, A.P.L.; Buckley, C. Flutemetamol amyloid positron emission tomography in preclinical and symptomatic Alzheimer’s disease: Specific detection of advanced phases of amyloid-β pathology. Alzheimer. Dement. 2015, 11, 975–985. [Google Scholar] [CrossRef]
- Hattori, N.; Sherwin, P.; Farrar, G. Initial Physician Experience with Flutemetamol Amyloid PET Imaging Following Availability for Routine Clinical Use in Japan. J. Alzheimer’s Dis. Rep. 2020, 4, 165–174. [Google Scholar] [CrossRef]
- Kalaria, R.N. The pathology and pathophysiology of vascular dementia. Neuropharmacology 2018, 134, 226–239. [Google Scholar] [CrossRef]
- Koikkalainen, J.; Rhodius-Meester, H.; Tolonen, A.; Barkhof, F.; Tijms, B.; Lemstra, A.W.; Tong, T.; Guerrero, R.; Schuh, A.; Ledig, C.; et al. Differential diagnosis of neurodegenerative diseases using structural MRI data. Neuroimage Clin. 2016, 11, 435–449. [Google Scholar] [CrossRef] [Green Version]
- Debette, S.; Markus, H.S. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: Systematic review and meta-analysis. BMJ 2010, 341, c3666. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Ogbole, G.; Aribisala, B.; Affini, M.; Yaria, J.; Kehinde, I.; Rahman, M.; Adekunle, F.; Banjo, R.; Faniyan, M.; et al. Association between white matter hyperintensities and stroke in a West African patient population: Evidence from the Stroke Investigative Research and Educational Network study. NeuroImage 2020, 215, 116789. [Google Scholar] [CrossRef]
- Zuo, X.-N.; Kelly, C.; Di Martino, A.; Mennes, M.; Margulies, D.S.; Bangaru, S.; Grzadzinski, R.; Evans, A.C.; Zang, Y.-F.; Castellanos, F.X.; et al. Growing Together and Growing Apart: Regional and Sex Differences in the Lifespan Developmental Trajectories of Functional Homotopy. J. Neurosci. 2010, 30, 15034–15043. [Google Scholar] [CrossRef]
- Kelly, C.; Zuo, X.-N.; Gotimer, K.; Cox, C.L.; Lynch, L.; Brock, D.; Imperati, D.; Garavan, H.; Rotrosen, J.; Castellanos, F.X.; et al. Reduced interhemispheric resting state functional connectivity in cocaine addiction. Biol. Psychiatry 2011, 69, 684–692. [Google Scholar] [CrossRef] [Green Version]
- Yuan, K.; Qin, W.; Liu, P.; Zhao, L.; Yu, D.; Zhao, L.; Dong, M.; Liu, J.; Yang, X.; von Deneen, K.M.; et al. Reduced Fractional Anisotropy of Corpus Callosum Modulates Inter-Hemispheric Resting State Functional Connectivity in Migraine Patients without Aura. PLoS ONE 2012, 7, e45476. [Google Scholar] [CrossRef]
- Su, Q.; Yao, D.; Jiang, M.; Liu, F.; Long, L.; Dai, Y.; Yu, M.; Zhang, Z.; Zhang, J.; Liu, J.; et al. Decreased interhemispheric functional connectivity in insula and angular gyrus/supramarginal gyrus: Significant findings in first-episode, drug-naive somatization disorder. Psychiatry Res. Neuroimaging 2016, 248, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Yang, X.; Zhang, J.; Chen, Y.; Li, T.; Ma, X. Analysis of voxel-mirrored homotopic connectivity in medication-free, current major depressive disorder. J. Affect. Disord. 2018, 240, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Wang, C.; Ji, G.; Feng, Z.; Duan, J.; Chen, F.; Zhou, X.J.; Shi, Y.; Xie, H. Aberrant interhemispheric functional connectivity in first-episode, drug-naïve major depressive disorder. Brain Imaging Behav. 2019, 13, 1302–1310. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wang, Y.; Jia, Y.; Zhong, S.; Sun, Y.; Qi, Z.; Zhang, Z.; Huang, L. Altered interhemispheric functional connectivity in remitted bipolar disorder: A Resting State fMRI Study. Sci. Rep. 2017, 7, 4698. [Google Scholar] [CrossRef] [Green Version]
- Liao, Z.; Tan, Y.; Qiu, Y.; Zhu, J.; Chen, Y.; Lin, S.; Wu, M.; Mao, Y.; Hu, J.; Ding, Z.; et al. Interhemispheric functional connectivity for Alzheimer’s disease and amnestic mild cognitive impairment based on the triple network model. J. Zhejiang Univ. Sci. B 2018, 19, 924–934. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Zhang, H.; Mchugh, R.; Sun, X.; Li, K.; Yang, Q.X. Interhemispheric Functional and Structural Disconnection in Alzheimer’s Disease: A Combined Resting-State fMRI and DTI Study. PLoS ONE 2015, 10, e0126310. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.; Liao, Z.; Tan, Y.; Qiu, Y.; Zhu, J.; Han, Z.; Wang, J.; Wang, X.; Wang, H.; Chen, Y.; et al. High-sensitivity neuroimaging biomarkers for the identification of amnestic mild cognitive impairment based on resting-state fMRI and a triple network model. Brain Imaging Behav. 2019, 13, 1–14. [Google Scholar] [CrossRef]
- Rubinov, M.; Sporns, O. Complex network measures of brain connectivity: Uses and interpretations. NeuroImage 2010, 52, 1059–1069. [Google Scholar] [CrossRef]
- Chau, A.C.M.; Cheung, E.Y.W.; Chan, K.H.; Chow, W.S.; Shea, Y.F.; Chiu, P.K.C.; Mak, H.K.F. Impaired cerebral blood flow in type 2 diabetes mellitus—A comparative study with subjective cognitive decline, vascular dementia and Alzheimer’s disease subjects. NeuroImage Clin. 2020, 27, 102302. [Google Scholar] [CrossRef]
- Wong, A.; Xiong, Y.Y.; Kwan, P.W.L.; Chan, A.Y.Y.; Lam, W.W.M.; Wang, K.; Chu, W.C.W.; Nyenhuis, D.L.; Nasreddine, Z.; Wong, L.K.S.; et al. The Validity, Reliability and Clinical Utility of the Hong Kong Montreal Cognitive Assessment (HK-MoCA) in Patients with Cerebral Small Vessel Disease. Dement. Geriatr. Cogn. Disord. 2009, 28, 81–87. [Google Scholar] [CrossRef]
- Yan, C.-G.; Craddock, R.C.; Zuo, X.-N.; Zang, Y.-F.; Milham, M.P. Standardizing the intrinsic brain: Towards robust measurement of inter-individual variation in 1000 functional connectomes. NeuroImage 2013, 80, 246–262. [Google Scholar] [CrossRef] [Green Version]
- Hachinski, V.C.; Potter, P.; Merskey, H. Leuko-Araiosis. Arch. Neurol. 1987, 44, 21–23. [Google Scholar] [CrossRef]
- Wei, K.; Tran, T.; Chu, K.; Borzage, M.T.; Braskie, M.N.; Harrington, M.G.; King, K.S. White matter hypointensities and hyperintensities have equivalent correlations with age and CSF β-amyloid in the nondemented elderly. Brain Behav. 2019, 9, e01457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischl, B. FreeSurfer. NeuroImage 2012, 62, 774–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischl, B.; Salat, D.H.; Busa, E.; Albert, M.; Dieterich, M.; Haselgrove, C.; van der Kouwe, A.; Killiany, R.; Kennedy, D.; Klaveness, S.; et al. Whole Brain Segmentation. Neuron 2002, 33, 341–355. [Google Scholar] [CrossRef] [Green Version]
- Fischl, B.; Salat, D.H.; van der Kouwe, A.J.W.; Makris, N.; Ségonne, F.; Quinn, B.T.; Dale, A.M. Sequence-independent segmentation of magnetic resonance images. NeuroImage 2004, 23, S69–S84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischl, B.; Liu, A.; Dale, A.M. Automated manifold surgery: Constructing geometrically accurate and topologically correct models of the human cerebral cortex. IEEE Trans. Med. Imaging 2001, 20, 70–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ségonne, F.; Pacheco, J.; Fischl, B. Geometrically accurate topology-correction of cortical surfaces using nonseparating loops. IEEE Trans. Med. Imaging 2007, 26, 518–529. [Google Scholar] [CrossRef]
- Dale, A.M.; Fischl, B.; Sereno, M.I. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage 1999, 9, 179–194. [Google Scholar] [CrossRef]
- Dale, A.M.; Sereno, M.I. Improved Localizadon of Cortical Activity by Combining EEG and MEG with MRI Cortical Surface Reconstruction: A Linear Approach. J. Cogn. Neurosci. 1993, 5, 162–176. [Google Scholar] [CrossRef]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef] [Green Version]
- Safari, S.; Baratloo, A.; Elfil, M.; Negida, A. Evidence Based Emergency Medicine; Part 5 Receiver Operating Curve and Area under the Curve. Emergency 2016, 4, 111–113. [Google Scholar]
- Duffy, F.H.; Mcanulty, G.B.; Albert, M.S. Effects of age upon interhemispheric EEG coherence in normal adults. Neurobiol. Aging 1996, 17, 587–599. [Google Scholar] [CrossRef]
- Yi, L.-Y.; Liang, X.; Liu, D.-M.; Sun, B.; Ying, S.; Yang, D.-B.; Li, Q.-B.; Jiang, C.-L.; Han, Y. Disrupted topological organization of resting-state functional brain network in subcortical vascular mild cognitive impairment. CNS Neurosci. Ther. 2015, 21, 846–854. [Google Scholar] [CrossRef]
- Zhou, X.; Hu, X.; Zhang, C.; Wang, H.; Zhu, X.; Xu, L.; Sun, Z.; Yu, Y. Aberrant Functional Connectivity and Structural Atrophy in Subcortical Vascular Cognitive Impairment: Relationship with Cognitive Impairments. Front. Aging Neurosci. 2016, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Liu, B.; Chen, J.; Peng, X.; Liu, X.; Fan, Y.; Liu, M.; Huang, R. Determination of Vascular Dementia Brain in Distinct Frequency Bands with Whole Brain Functional Connectivity Patterns. PLoS ONE 2013, 8, e54512. [Google Scholar]
- Kalaria, R.N.; Akinyemi, R.; Ihara, M. Stroke injury, cognitive impairment and vascular dementia. Biochim. Biophys. Acta Mol. Basis Dis. 2016, 1862, 915–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Overdorp, E.J.; Kessels, R.P.C.; Claassen, J.A.; Oosterman, J.M. Cognitive impairments associated with medial temporal atrophy and white matter hyperintensities: An MRI study in memory clinic patients. Front. Aging Neurosci. 2014, 6, 98. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, Y.; Liu, Q.; Shi, Q.; Wang, J.; Shen, H.; Chen, X.; Ma, J.; Ai, L.; Zhang, Y.M. Abnormal Interactions of the Salience Network, Central Executive Network, and Default-Mode Network in Patients With Different Cognitive Impairment Loads Caused by Leukoaraiosis. Front. Neural Circuits 2019, 13, 42. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W. The Salience Network: A Neural System for Perceiving and Responding to Homeostatic Demands. J. Neurosci. 2019, 39, 9878–9882. [Google Scholar] [CrossRef]
- Uddin, L.Q. Functions of the Salience Network. In Salience Network of the Human Brain; Elsevier: Amsterdam, The Netherlands, 2017; pp. 11–16. ISBN 978-0-12-804593-0. [Google Scholar]
- Kringelbach, M.L. The human orbitofrontal cortex: Linking reward to hedonic experience. Nat. Rev. Neurosci. 2005, 6, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Torregrossa, M.M.; Quinn, J.J.; Taylor, J.R. Impulsivity, Compulsivity, and Habit: The Role of Orbitofrontal Cortex Revisited. Biol. Psychiatry 2008, 63, 253–255. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Qin, W.; Zhang, J.; Zhang, X.; Yu, C. Enhanced Interhemispheric Functional Connectivity Compensates for Anatomical Connection Damages in Subcortical Stroke. Stroke 2015, 46, 1045–1051. [Google Scholar] [CrossRef] [Green Version]
- Torisson, G.; van Westen, D.; Stavenow, L.; Minthon, L.; Londos, E. Medial temporal lobe atrophy is underreported and may have important clinical correlates in medical inpatients. BMC Geriatr. 2015, 15, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jack, C.R.; Barkhof, F.; Bernstein, M.A.; Cantillon, M.; Cole, P.E.; DeCarli, C.; Dubois, B.; Duchesne, S.; Fox, N.C.; Frisoni, G.B.; et al. Steps to standardization and validation of hippocampal volumetry as a biomarker in clinical trials and diagnostic criterion for Alzheimer’s disease. Alzheimer. Dement. 2011, 7, 474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.; Kwon, J.-H.; Seo, H.-J. Medial temporal lobe atrophy in vascular dementia: Visual temporal lobe rating scale. Arch. Gerontol. Geriatr. 2009, 48, 415–418. [Google Scholar] [CrossRef]
- Schuff, N.; Matsumoto, S.; Kmiecik, J.; Studholme, C.; Du, A.; Ezekiel, F.; Miller, B.L.; Kramer, J.H.; Jagust, W.J.; Chui, H.C.; et al. Cerebral blood flow in ischemic vascular dementia and Alzheimer’s disease, measured by arterial spin-labeling magnetic resonance imaging. Alzheimer. Dement. 2009, 5, 454–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hachinski, V. Shifts in Thinking About Dementia. JAMA 2008, 300, 2172. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Braak, E.; Bohl, J. Staging of Alzheimer-related cortical destruction. Int. Psychogeriatr. 1993, 33, 403–408. [Google Scholar] [CrossRef]
- Yang, L.; Yan, Y.; Wang, Y.; Hu, X.; Lu, J.; Chan, P.; Yan, T.; Han, Y. Gradual Disturbances of the Amplitude of Low-Frequency Fluctuations (ALFF) and Fractional ALFF in Alzheimer Spectrum. Front. Neurosci. 2018, 12, 975. [Google Scholar] [CrossRef] [Green Version]
- Reisberg, B.; Prichep, L.; Mosconi, L.; John, E.R.; Glodzik-Sobanska, L.; Boksay, I.; Monteiro, I.; Torossian, C.; Vedvyas, A.; Ashraf, N.; et al. The pre–mild cognitive impairment, subjective cognitive impairment stage of Alzheimer’s disease. Alzheimer. Dement. 2008, 4, S98–S108. [Google Scholar] [CrossRef]
- Teipel, S.J.; Wohlert, A.; Metzger, C.; Grimmer, T.; Sorg, C.; Ewers, M.; Meisenzahl, E.; Klöppel, S.; Borchardt, V.; Grothe, M.J.; et al. Multicenter stability of resting state fMRI in the detection of Alzheimer’s disease and amnestic MCI. NeuroImage Clin. 2017, 14, 183–194. [Google Scholar] [CrossRef]
- Petrides, M.; Pandya, D.N. The Frontal Cortex. In The Human Nervous System; Elsevier: Amsterdam, The Netherlands, 2012; pp. 988–1011. ISBN 978-0-12-374236-0. [Google Scholar]
- Seubert, J.; Freiherr, J.; Djordjevic, J.; Lundström, J.N. Statistical localization of human olfactory cortex. NeuroImage 2013, 66, 333–342. [Google Scholar] [CrossRef]
- Joo, M.S.; Park, D.S.; Moon, C.T.; Chun, Y.I.; Song, S.W.; Roh, H.G. Relationship between Gyrus Rectus Resection and Cognitive Impairment after Surgery for Ruptured Anterior Communicating Artery Aneurysms. J. Cerebrovasc. Endovasc. Neurosurg. 2016, 18, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Testa, N.; Jordan, R.; Elyan, R.; Kanekar, S.; Wang, J.; Eslinger, P.; Yang, Q.X.; Zhang, B.; Karunanayaka, P.R. Functional Connectivity between the Resting-State Olfactory Network and the Hippocampus in Alzheimer’s Disease. Brain Sci. 2019, 9, 338. [Google Scholar] [CrossRef] [Green Version]
- Menon, V.; Uddin, L.Q. Saliency, switching, attention and control: A network model of insula function. Brain Struct. Funct. 2010, 214, 655–667. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VD | AD | MCI | HC | |
|---|---|---|---|---|
| No of participants | 13 | 16 | 29 | 25 |
| Age | 79.15 ^ ± 4.06 (69–84) | 74.81 ± 7.93 (61–87) | 74.95 @ ± 6.84 (64–88) | 68.84 @^ ± 6.27 (60–84) |
| Gender (M/F) | 9/6 | 8/13 | 7/14 | 9/16 |
| HK-MoCA | 17.00 %* ± 4.69 (7–23) | 13.17 #%* ± 7.11 (3–23) | 21.25 #% ± 3.88 (13–29) | 28.56 %± 1.23 (26–30) |
| leukoaraiosis volume (mm3) | 15,098.7 ^ | 4883.3 ^ | 3309.2 ^ | 4247.4 ^ |
| T2DM | 3(23.1%) | 0 | 6 (20.6%) | 0 |
| Hypertension | 9(69.2%) | 7(43.7%) | 13(44.8%) | 7(28%) |
| Hyperlipidemia | 10(76.9%) | 6(37.5%) | 4(13.8%) | 4(16%) |
| VD vs. HC Brain Regions | Network | Coordinate (MNI) | Peak Intensity | Volume | Correlation Coefficient | ||
|---|---|---|---|---|---|---|---|
| x | y | z | (T Value) | (mm3) | |||
| Precentral gryus | ECN | −23 | −14 | 66 | 3.011 | −316.38 | |
| Sup Frontal | DMN | −19 | −8 | 74 | 3.437 | 603.33 | r = 0.667 |
| Sup Frontal Orb | vSN | −18 | 38 | −20 | −2.711 | 61.50 | |
| Inf Frontal Oper | vSN | −44 | 15 | 11 | 3.464 | 26.45 | |
| Inf Frontal Tri | DMN | −33 | 29 | 4 | 2.857 | −59.58 | |
| Rolandic Oper | dSN | −40 | −13 | 21 | 3.652 | 211.16 | |
| Supp Motor Area | −6 | 7 | 51 | 3.835 | −132.8 | ||
| Olfactory | −12 | 15 | 17 | 3.553 | −69.98 | ||
| Frontal Med Orb | −6 | 38 | −10 | −4.049 | −150.01 | ||
| Gyrus rectus | vSN | −6 | 39 | −18 | −6.866 | −4.40 | |
| Insula | SN | −36 | −14 | 13 | 4.682 | −57.48 | |
| Ant cing | DMN | −5 | 11 | 27 | 4.315 | −165.48 | |
| Mid Cing | DMN | −8 | 8 | 42 | 3.201 | −147.7 | |
| Post Cing | DMN | −12 | −43 | 16 | 2.963 | −85.80 | |
| Hippocampus | −28 | −20 | −10 | 3.391 | −720.79 # | ||
| Parahippocampus | −22 | −34 | −5 | 3.141 | −165.67 | ||
| Amygdala | SN | −18 | −1 | −11 | 3.707 | −385.47 # | |
| Caudate | −15 | 23 | 9 | 3.553 | 118.27 | ||
| AD vs. HC Brain Regions | Network | Coordinate (MNI) | Peak Intensity | Volume | Correlation Coefficient | ||
|---|---|---|---|---|---|---|---|
| x | y | z | (T Value) | (mm3) | |||
| Precentral gryus | ECN | −40 | −21 | 63 | −2.848 | −191.13 | |
| Sup Frontal | DMN | −19 | 55 | 27 | −2.574 | −820.20# | |
| Sup Frontal Orb | vSN | −18 | 34 | −24 | −5.252 | −81.60 | |
| Mid Frontal | DMN | −34 | 52 | 16 | −2.807 | −797.45 | |
| Mid Front Orb | ECN | −32 | 57 | −8 | −2.915 | −241.39 | |
| Inf Frontal Oper | vSN | −52 | 9 | 25 | −4.033 | −303.90 | |
| Inf Frontal Tri | DMN | −45 | 39 | 10 | −4.157 | −291.70 | |
| Inf Frontal orb | vSN | −37 | 29 | −21 | −3.362 | −29.40 | |
| Rolandic Oper | dSN | −45 | −26 | 18 | −2.766 | −136.20 | |
| Olfactory | −6 | 23 | −8 | −2.651 | −72.54 | ||
| Sup Frontal Medial | −6 | 51 | 27 | −2.852 | −533.60 | ||
| Frontal Med Orb | −6 | 39 | −9 | −3.159 | −328.71 | ||
| Gyrus rectus | vSN | −8 | 37 | −19 | −4.997 | −57.56 | |
| Insula | SN | −36 | 7 | 3 | −3.783 | −404.75 | |
| Ant cing | DMN | −7 | 47 | 12 | −3.052 | −271.20 | |
| Post Cing | DMN | −6 | −43 | 12 | −3.14 | −245.20 # | |
| Hippocampus | −22 | −37 | 9 | −2.839 | −903.70 # | ||
| Parahippocampus | −22 | −5 | −32 | −3.283 | −407.66 | ||
| Amygdala | SN | −24 | 2 | −17 | −3.465 | −567.81 # | |
| Calcarine | −8 | −63 | 16 | −3.063 | −299.00 | ||
| Cuneus | −8 | −83 | 24 | −3.054 | −139.40 | ||
| Lingual Gyrus | SN | −17 | −66 | 4 | −3.236 | −430.46 # | |
| Sup Occipital | SN | −18 | −84 | 28 | −3.217 | −238.40 | |
| Mid occipital | ECN | −35 | −81 | 35 | −3.726 | −714.76 # | r = 0.692 |
| Inf occipital | −37 | −83 | −4 | −3.42 | −139.90 | ||
| Fusiform | −28 | −50 | −12 | −2.989 | −744.70 # | ||
| Post Central | ECN | −44 | −23 | 49 | −4.312 | −333.39 | |
| Sup Parietal | −24 | −59 | 56 | −3.178 | −298.60 # | ||
| Inf Parietal | DMN | −44 | −36 | 39 | −5.332 | −298.56 | |
| SupraMarginal | ECN | −57 | −44 | 31 | −5.199 | −690.12 | |
| Angular | DMN | −50 | −61 | 29 | −3.166 | −603.50 | |
| Precuneus | DMN | −3 | −55 | 41 | −3.250 | −893.74 # | |
| Caudate | −12 | 22 | −5 | −3.411 | −243.47 | ||
| Thalamus | −10 | −22 | 3 | −3.059 | −700.16 # | ||
| Heschl | −50 | −15 | 9 | −3.824 | −9.20 | ||
| Sup Temp | DMN | −54 | −6 | −2 | −3.853 | −1304.4 # | |
| Sup Temp Pole | −51 | 7 | −6 | −3.311 | −378.75 | ||
| Mid Temp | ECN | −57 | −49 | 6 | −3.105 | −834.24 | |
| Inf Temp | ECN | −51 | −51 | −23 | −3.535 | −1240.70 # | |
| MCI vs. HC Brain Regions | Network | Coordinate (MNI) | Peak Intensity | Volume | Correlation Coefficient | ||
|---|---|---|---|---|---|---|---|
| x | y | z | (T Value) | (mm3) | |||
| Precentral gryus | ECN | −31 | −5 | 50 | 2.728 | +65.00 | |
| Sup Frontal | DMN | −19 | 1 | 59 | 3.839 | 262.16 | |
| p Frontal Orb | vSN | −17 | 33 | −23 | −4.496 | −67.40 | |
| Inf Frontal orb | vSN | −37 | 29 | −21 | −3.362 | −53.90 | |
| Rolandic Oper | dSN | −43 | −8 | 18 | 3.420 | 29.48 | |
| Supp Motor Area | −8 | 8 | 46 | 5.041 | −192.20 | ||
| Olfactory | −9 | 18 | −4 | −2.931 | −43.48 | ||
| Frontal Med Orb | −6 | 37 | −10 | −2.642 | −197.96 | ||
| Gyrus rectus | vSN | −8 | 39 | −20 | −4.386 | 54.37 | |
| Insula | SN | −33 | 7 | 12 | 3.308 | −101.8 | |
| Mid cing | DMN | −8 | 4 | 43 | 3.734 | 0.40 | |
| Post Central | ECN | −21 | −30 | 71 | 3.663 | −133.1 | |
| Paracentral Lobule | −14 | −26 | 76 | 3.567 | 22.34 | ||
| Hippocampus | No sig | −470.56 # | |||||
| Amygdala | SN | No sig | −299.84 # | ||||
| Caudate | −16 | 11 | 20 | 4.122 | 35.72 | ||
| Putamen | −24 | 8 | 10 | 2.825 | −247.9 | ||
| Thalamus | −12 | −14 | 18 | 2.954 | −386.58 # | ||
| Brain Regions | AUC | Sig | Network | Threshold VMHC Value | Sen | Spec | PPV | NPV | Acc | Youden Index | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Calcarine | 0.712 | p = 0.034 | DMN | Reduction | 0.47 | 0.77 | 0.64 | 0.68 | 0.73 | 70% | 0.41 |
| Lingual Gyrus | 0.712 | p = 0.034 | dSN | Reduction | 0.52 | 0.69 | 0.80 | 0.78 | 0.72 | 75% | 0.49 |
| Gyrus Rectus | 0.723 | p = 0.026 | vSN | Reduction | 0.42 | 1.00 | 0.56 | 0.69 | 1.00 | 78% | 0.56 |
| Supp Motor Area | 0.718 | p = 0.029 | Increased | 0.42 | 0.85 | 0.52 | 0.64 | 0.77 | 68% | 0.37 | |
| Combined | 0.908 | p = 0.000 | 0.923 | 0.84 | 0.92 | 0.77 | 87% | 0.76 |
| Brain Regions | AUC | Sig | Network | Threshold VMHC Value | Sensitivity | Specificity | PPV | NPV | Accuracy | Youden Index |
|---|---|---|---|---|---|---|---|---|---|---|
| Angular Gyrus | 0.735 | p = 0.012 | DMN | 0.47 | 0.69 | 0.76 | 0.74 | 0.71 | 72% | 0.45 |
| Calcarine | 0.709 | p = 0.026 | DMN | 0.47 | 0.75 | 0.64 | 0.68 | 0.72 | 70% | 0.39 |
| Cuneus | 0.716 | p = 0.021 | DMN | 0.44 | 0.50 | 0.96 | 0.93 | 0.66 | 73% | 0.46 |
| Inf Parietal | 0.82 | p = 0.001 | DMN | 0.42 | 0.81 | 0.80 | 0.80 | 0.81 | 81% | 0.61 |
| Sup Temp | 0.708 | p = 0.001 | DMN | 0.37 | 0.75 | 0.84 | 0.82 | 0.77 | 80% | 0.59 |
| Inf Temp | 0.73 | p = 0.014 | ECN | 0.32 | 0.75 | 0.72 | 0.73 | 0.74 | 74% | 0.47 |
| Mid Occi | 0.725 | p = 0.016 | ECN | 0.33 | 0.50 | 0.96 | 0.93 | 0.66 | 73% | 0.46 |
| Mid Temp | 0.755 | p = 0.006 | ECN | 0.29 | 0.69 | 0.88 | 0.85 | 0.74 | 78% | 0.57 |
| Post Central | 0.747 | p = 0.008 | ECN | 0.29 | 0.56 | 0.92 | 0.88 | 0.68 | 74% | 0.48 |
| SupraMarginal | 0.781 | p = 0.003 | ECN | 0.29 | 0.63 | 0.96 | 0.94 | 0.72 | 79% | 0.59 |
| Inf Front Orb | 0.754 | p = 0.007 | SN | 0.29 | 0.63 | 0.88 | 0.84 | 0.70 | 75% | 0.51 |
| Inf Occi | 0.741 | p = 0.010 | SN | 0.37 | 0.69 | 0.92 | 0.90 | 0.75 | 80% | 0.61 |
| Lingual Gyrus | 0.7 | p = 0.033 | SN | 0.45 | 0.50 | 0.96 | 0.93 | 0.66 | 73% | 0.46 |
| Gyrus rectus | 0.787 | p = 0.002 | vSN | 0.32 | 0.56 | 0.88 | 0.82 | 0.67 | 72% | 0.44 |
| Sup Occi | 0.708 | p = 0.002 | SN | 0.38 | 0.56 | 0.88 | 0.82 | 0.67 | 72% | 0.44 |
| Combined SN | 0.83 | p = 0.000 | 0.81 | 0.84 | 0.63 | 0.96 | 83% | 0.65 | ||
| Combined all | 0.92 | p = 0.000 | 0.92 | 0.88 | 0.88 | 0.92 | 92% | 0.76 |
| Brain Regions | AUC | Sig | Network | Threshold VMHC Value | Sens | Spec | PPV | NPV | Acc | Youden Index | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Inf Front Oper | 0.671 | p = 0.031 | vSN | Increased | 0.4 | 0.55 | 0.84 | 0.78 | 0.65 | 70% | 0.39 |
| Rolandic Oper | 0.677 | p = 0.026 | dSN | Increased | 0.46 | 0.48 | 0.88 | 0.80 | 0.63 | 68% | 0.36 |
| Supp Motor Area | 0.721 | p = 0.006 | Increased | 0.47 | 0.52 | 0.84 | 0.76 | 0.64 | 68% | 0.36 | |
| Inf Front Orb | 0.672 | p = 0.031 | vSN | Reduction | 0.35 | 0.69 | 0.68 | 0.68 | 0.69 | 68% | 0.37 |
| Gyrus rectus | 0.736 | p = 0.003 | vSN | Reduction | 0.39 | 0.76 | 0.68 | 0.70 | 0.74 | 72% | 0.44 |
| Sup Front Orb | 0.672 | p = 0.03 | vSN | Reduction | 0.35 | 0.69 | 0.68 | 0.68 | 0.69 | 68% | 0.37 |
| Combined | 0.905 | p = 0.000 | 0.88 | 0.83 | 0.80 | 0.86 | 83% | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, E.Y.W.; Shea, Y.F.; Chiu, P.K.C.; Kwan, J.S.K.; Mak, H.K.F. Diagnostic Efficacy of Voxel-Mirrored Homotopic Connectivity in Vascular Dementia as Compared to Alzheimer’s Related Neurodegenerative Diseases—A Resting State fMRI Study. Life 2021, 11, 1108. https://doi.org/10.3390/life11101108
Cheung EYW, Shea YF, Chiu PKC, Kwan JSK, Mak HKF. Diagnostic Efficacy of Voxel-Mirrored Homotopic Connectivity in Vascular Dementia as Compared to Alzheimer’s Related Neurodegenerative Diseases—A Resting State fMRI Study. Life. 2021; 11(10):1108. https://doi.org/10.3390/life11101108
Chicago/Turabian StyleCheung, Eva Y. W., Y. F. Shea, Patrick K. C. Chiu, Joseph S. K. Kwan, and Henry K. F. Mak. 2021. "Diagnostic Efficacy of Voxel-Mirrored Homotopic Connectivity in Vascular Dementia as Compared to Alzheimer’s Related Neurodegenerative Diseases—A Resting State fMRI Study" Life 11, no. 10: 1108. https://doi.org/10.3390/life11101108