
Cardiac Transplantation and the Use of Cannabis

 , , and
, , and
Abstract
:1. Introduction
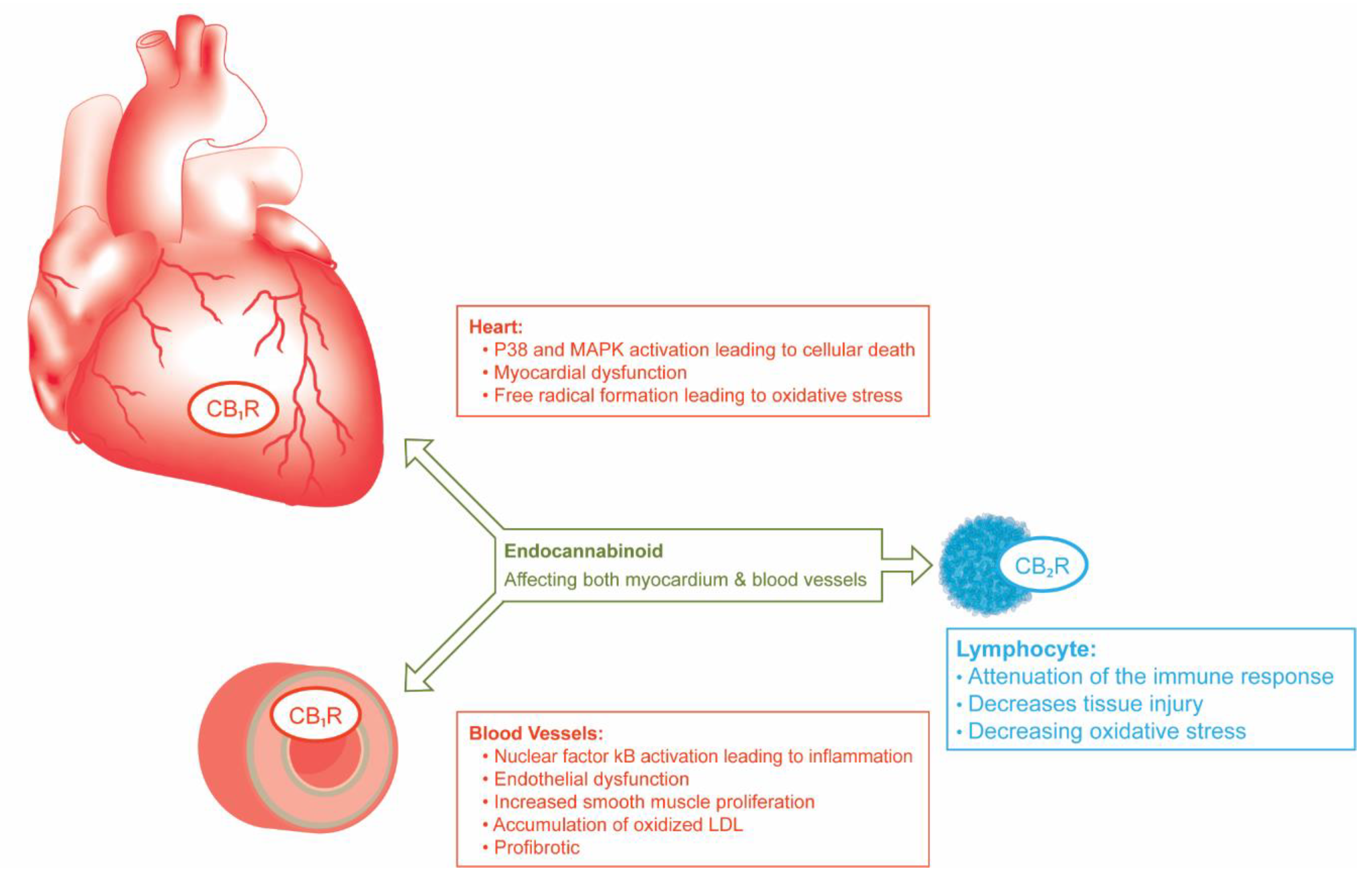
2. Physiology of the Endocannabinoid System (ECS)
3. Activation of CB1R (THC) May Provoke Detrimental Cardiovascular Effects While CB2R Activation May Be Cardioprotective
4. Route of Administration and Pharmacokinetics of Cannabis
5. Medical Uses of Tetrahydrocannabinol (THC) and Cannabidiol (CBD)
6. Cardiovascular Effects of Cannabis
7. Cannabis Use and Outcomes in Organ Transplantation
8. Transplant Listing and Other Illicit Substance Use
9. Similarities between Prescription Opiates and Prescription (Medical) Cannabis
10. Current Views on Cannabis Use and Transplantation
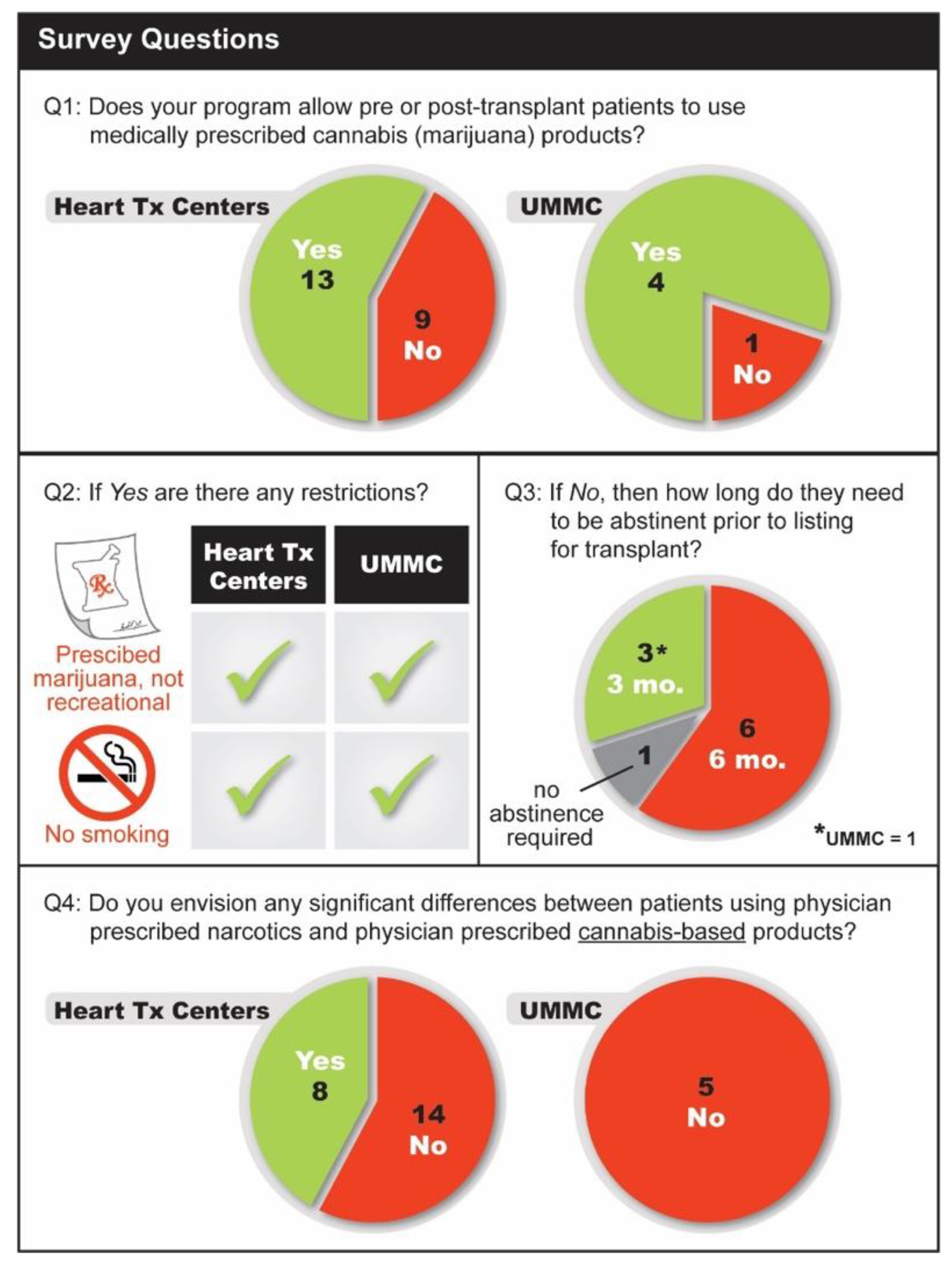
11. Multicenter Survey on Cannabis Use and Cardiac Transplantation Practices
11.1. Methods
11.2. Results
11.3. Survey of Other Organ Transplant Programs
12. Possible Approach to Cannabis Use in Heart Transplant Patients
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- ElSohly, M.A.; Mehmedic, Z.; Foster, S.; Gon, C.; Chandra, S.; Church, J.C. Changes in cannabis potency over the last 2 decades (1995–2014): Analysis of current data in the United States. Biol. Psychiatry 2016, 79, 613–619. [Google Scholar] [CrossRef] [Green Version]
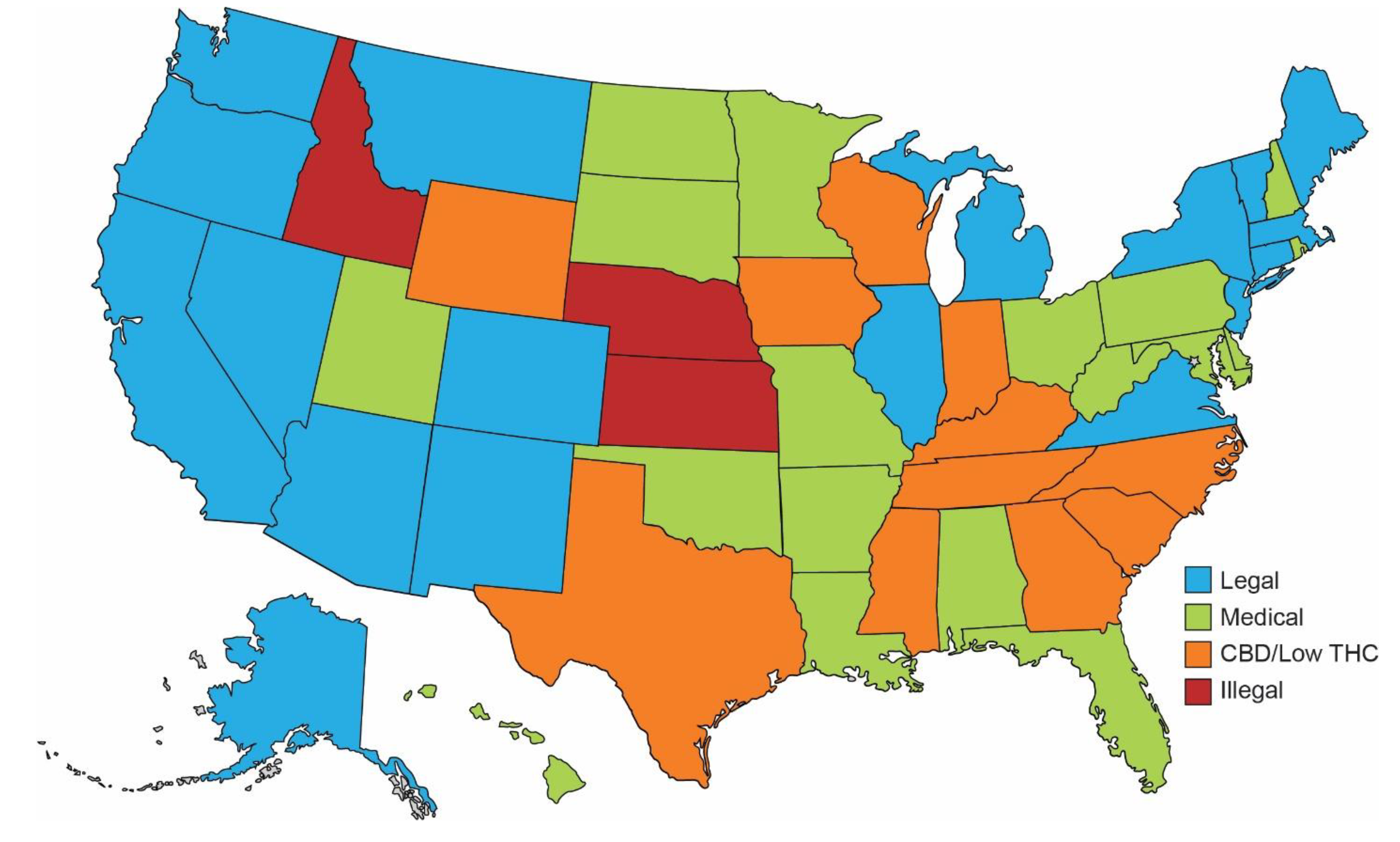
- Solutions, D.G. Map of Marijuana Legality by State. Available online: https://disa.com/map-of-marijuana-legality-by-state (accessed on 31 August 2021).
- Berke, J.; Gould, S. Legal marijuana just went on sale in Illinois. Here are all the states where cannabis is legal. Business Insider, 1 January 2020. [Google Scholar]
- Neyer, J.; Uberoi, A.; Hamilton, M.; Kobashigawa, J.A. Marijuana and listing for heart transplant: A survey of transplant providers. Circ. Heart Fail. 2016, 9, e002851. [Google Scholar] [CrossRef]
- Mehra, M.R.; Canter, C.E.; Hannan, M.M.; Semigran, M.J.; Uber, P.A.; Baran, D.A.; Verschuuren, E.A.M.; Zuckermann, A. The 2016 International Society for Heart Lung Transplantation listing criteria for heart transplantation: A 10-year update. J. Heart Lung Transplant. 2016, 35, 1–23. [Google Scholar] [CrossRef]
- Ghosh, M.; Naderi, S. Cannabis and cardiovascular disease. Curr. Atheroscler. Rep. 2019, 21, 1–6. [Google Scholar] [CrossRef]
- Ananth, P.; Reed-Weston, A.; Wolfe, J. Medical marijuana in pediatric oncology: A review of the evidence and implications for practice. Pediatric Blood Cancer 2018, 65, e26826. [Google Scholar] [CrossRef] [PubMed]
- Zou, S.; Kumar, U. Cannabinoid receptors and the endocannabinoid system: Signaling and function in the central nervous system. Int. J. Mol. Sci. 2018, 19, 833. [Google Scholar] [CrossRef] [Green Version]
- Mackie, K. Distribution of cannabinoid receptors in the central and peripheral nervous system. In Cannabinoids; Springer: Berlin/Heidelberg, Germany, 2005; pp. 299–325. [Google Scholar]
- Pacher, P.; Bátkai, S.; Kunos, G. The endocannabinoid system as an emerging target of pharmacotherapy. Pharmacol. Rev. 2006, 58, 389–462. [Google Scholar] [CrossRef] [Green Version]
- Galiègue, S.; Mary, S.; Marchand, J.; Dussossoy, D.; Carriere, D.; Carayon, P.; Bouaboula, M.; Shire, D.; Le Fur, G.; Casellas, P. Expression of central and peripheral cannabinoid receptors in human immune tissues and leukocyte subpopulations. Eur. J. Biochem. 1995, 232, 54–61. [Google Scholar] [CrossRef]
- Ofek, O.; Karsak, M.; Leclerc, N.; Fogel, M.; Frenkel, B.; Wright, K.; Tam, J.; Attar-Namdar, M.; Kram, V.; Shohami, E.; et al. Peripheral cannabinoid receptor, CB2, regulates bone mass. Proc. Natl. Acad. Sci. USA 2006, 103, 696–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffens, S.; Pacher, P. The activated endocannabinoid system in atherosclerosis: Driving force or protective mechanism? Curr. Drug Targets 2015, 16, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Borges, R.S.; Batista, J., Jr.; Viana, R.B.; Baetas, A.C.; Orestes, E.; Andrade, M.A.; Honorio, K.M.; Da Silva, A.F. Understanding the molecular aspects of tetrahydrocannabinol and cannabidiol as antioxidants. Molecules 2013, 18, 12663–12674. [Google Scholar] [CrossRef] [Green Version]
- Pan, H.; Mukhopadhyay, P.; Rajesh, M.; Patel, V.; Mukhopadhyay, B.; Gao, B.; Haskó, G.; Pacher, P. Cannabidiol attenuates cisplatin-induced nephrotoxicity by decreasing oxidative/nitrosative stress, inflammation, and cell death. J. Pharmacol. Exp. Ther. 2009, 328, 708–714. [Google Scholar] [CrossRef] [Green Version]
- Rajesh, M.; Mukhopadhyay, P.; Batkai, S.; Hasko, G.; Liaudet, L.; Drel, V.R.; Obrosova, I.G.; Pacher, P. Cannabidiol attenuates high glucose-induced endothelial cell inflammatory response and barrier disruption. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H610–H619. [Google Scholar] [CrossRef] [Green Version]
- Hamelink, C.; Hampson, A.; Wink, D.A.; Eiden, L.E.; Eskay, R.L. Comparison of cannabidiol, antioxidants, and diuretics in reversing binge ethanol-induced neurotoxicity. J. Pharmacol. Exp. Ther. 2005, 314, 780–788. [Google Scholar] [CrossRef] [Green Version]
- Costa, B.; Trovato, A.E.; Comelli, F.; Giagnoni, G.; Colleoni, M. The non-psychoactive cannabis constituent cannabidiol is an orally effective therapeutic agent in rat chronic inflammatory and neuropathic pain. Eur. J. Pharmacol. 2007, 556, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Pacher, P.; Steffens, S.; Haskó, G.; Schindler, T.H.; Kunos, G. Cardiovascular effects of marijuana and synthetic cannabinoids: The good, the bad, and the ugly. Nat. Rev. Cardiol. 2018, 15, 151. [Google Scholar] [CrossRef]
- Rajesh, M.; Bátkai, S.; Kechrid, M.; Mukhopadhyay, P.; Lee, W.S.; Horváth, B.; Holovac, E.; Cinar, R.; Liaudet, L.; Mackie, K.; et al. Cannabinoid 1 receptor promotes cardiac dysfunction, oxidative stress, inflammation, and fibrosis in diabetic cardiomyopathy. Diabetes 2012, 61, 716–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajesh, M.; Mukhopadhyay, P.; Haskó, G.; Liaudet, L.; Mackie, K.; Pacher, P. Cannabinoid-1 receptor activation induces reactive oxygen species-dependent and-independent mitogen-activated protein kinase activation and cell death in human coronary artery endothelial cells. Br. J. Pharmacol. 2010, 160, 688–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singla, S.; Sachdeva, R.; Mehta, J.L. Cannabinoids and atherosclerotic coronary heart disease. Clin. Cardiol. 2012, 35, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, P.; Bátkai, S.; Rajesh, M.; Czifra, N.; Harvey-White, J.; Haskó, G.; Zsengeller, Z.; Gerard, N.P.; Liaudet, L.; Kunos, G.; et al. Pharmacological inhibition of CB1cannabinoid receptor protects against doxorubicin-induced cardiotoxicity. J. Am. Coll. Cardiol. 2007, 50, 528–536. [Google Scholar] [CrossRef] [Green Version]
- Tiyerili, V.; Zimmer, S.; Jung, S.; Wassmann, K.; Naehle, C.P.; Lütjohann, D.; Zimmer, A.; Nickenig, G.; Wassmann, S. CB1 receptor inhibition leads to decreased vascular AT1 receptor expression, inhibition of oxidative stress and improved endothelial function. Basic Res. Cardiol. 2010, 105, 465–477. [Google Scholar] [CrossRef]
- Klein, T.W.; Newton, C.; Larsen, K.; Lu, L.; Perkins, I.; Nong, L.; Friedman, H. The cannabinoid system and immune modulation. J. Leukoc. Biol. 2003, 74, 486–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouaboul, M.; Rinaldi, M.; Carayon, P.; Carillon, C.; Delpech, B.; Shire, D.; Le Fur, G.; Casellas, P. Cannabinoid-receptor expression in human leukocytes. Eur. J. Biochem. 1993, 214, 173–180. [Google Scholar] [CrossRef]
- Parlar, A.; Arslan, S.O.; Doğan, M.F.; Çam, S.A.; Yalçin, A.; Elibol, E.; Özer, M.K.; Üçkardeş, F.; Kara, H. The exogenous administration of CB2 specific agonist, GW405833, inhibits inflammation by reducing cytokine production and oxidative stress. Exp. Ther. Med. 2018, 16, 4900–4908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Filippo, C.; Rossi, F.; Rossi, S.; D’amico, M. Cannabinoid CB2 receptor activation reduces nouse myocardial ischemia-reperfusion injury: Involvement of cytokine/chemokines and PMN. J. Leukoc. Biol. 2004, 75, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Montecucco, F.; Lenglet, S.; Braunersreuther, V.; Burger, F.; Pelli, G.; Bertolotto, M.; Mach, F.; Steffens, S. CB(2) cannabinoid receptor activation is cardioprotective in a mouse model of ischemia/reperfusion. J. Mol. Cell. Cardiol. 2009, 46, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Krylatov, A.V.; Ugdyzhekova, D.S.; Bernatskaya, N.A.; Maslov, L.N.; Mekhoulam, R.; Pertwee, R.G.; Stephano, G.B. Activation of type II cannabinoid receptor improves myocardial tolerance to arrhythmogenic effects of coronary occlusion and reperfusion. Bull. Exp. Biol. Med. 2001, 131, 523–525. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Han, D.; Tian, Z.; Gao, B.; Fan, M.; Li, C.; Li, X.; Wang, Y.; Ma, S.; Cao, F.; et al. Activation of cannabinoid receptor type II by AM1241 ameliorates myocardial fibrosis via Nrf2-mediated inhibition of TGF-β1/Smad3 Pathway in Myocardial Infarction Mice. Cell. Physiol. Biochem. 2016, 39, 1521–1536. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.; Rueda, S.; Room, R.; Tyndall, M.; Fischer, B. Routes of administration for cannabis use–basic prevalence and related health outcomes: A scoping review and synthesis. Int. J. Drug Policy 2018, 52, 87–96. [Google Scholar] [CrossRef]
- Huestis, M.A.; Henningfield, J.E.; Cone, E.J. Blood cannabinoids. I. Absorption of THC and formation of 11-OH-THC and THCCOOH during and after smoking marijuana. J. Anal. Toxicol. 1992, 16, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Huestis, M.A.; Sampson, A.H.; Holicky, B.J.; Henningfield, J.E.; Cone, E.J. Characterization of the absorption phase of marijuana smoking. Clin. Pharmacol. Ther. 1992, 52, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Lemberger, L.; Weiss, J.L.; Watanabe, A.M.; Galanter, I.M.; Wyatt, R.J.; Cardon, P.V. Delta-9-tetrahydrocannabinol: Temporal correlation of the psychologic effects and blood levels after various routes of administration. N. Engl. J. Med. 1972, 286, 685–688. [Google Scholar] [CrossRef] [PubMed]
- Abrams, D.I.; Vizoso, H.P.; Shade, S.B.; Jay, C.; Kelly, M.E.; Benowitz, N.L. Vaporization as a smokeless cannabis delivery system: A pilot study. Clin. Pharmacol. Ther. 2007, 82, 572–578. [Google Scholar] [CrossRef] [PubMed]
- He, T.; Oks, M.; Esposito, M.; Steinberg, H.; Makaryus, M. “Tree-in-bloom”: Severe acute lung injury induced by vaping cannabis oil. Ann. Am. Thorac. Soc. 2017, 14, 468–470. [Google Scholar] [CrossRef]
- Blount, B.C.; Karwowski, M.P.; Shields, P.G.; Morel-Espinosa, M.; Valentin-Blasini, L.; Gardner, M.; Braselton, M.; Brosius, C.R.; Caron, K.T.; Chambers, D.; et al. Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N. Engl. J. Med. 2020, 382, 697–705. [Google Scholar] [CrossRef]
- Barrus, D.G.; Capogrossi, K.L.; Cates, S.C.; Gourdet, C.K.; Peiper, N.C.; Novak, S.P.; Lefever, T.W.; Wiley, J.L. Tasty THC: Promises and challenges of cannabis edibles. Methods Rep. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Rog, D.J.; Nurmikko, T.J.; Friede, T.; Young, C.A. Randomized, controlled trial on cannabis based medicine in central pain in multiple sclerosis. Neurology 2005, 65, 812–819. [Google Scholar] [CrossRef]
- Wright, S.; Ware, M.; Guy, G. The use of cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology 2006, 45, 781. [Google Scholar] [CrossRef] [Green Version]
- Blake, D.R.; Robson, P.; Ho, M.; Jubb, R.W.; McCabe, C.S. Preliminary assessment of the efficacy, toelrability, and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis. Rheumatology. 2005, 45, 50–52. [Google Scholar] [CrossRef] [Green Version]
- Ben-Zeev, B. Medical cannabis for intractable epilepsy in childhood: A review. Rambam Maimonides Med. J. 2020, 11, e0004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plasse, T.F.; Gorter, R.W.; Krasnow, S.H.; Lane, M.; Shepard, K.V.; Wadleigh, R.G. Recent clinical experience with dronabinol. Pharmacol. Biochem. Behav. 1991, 40, 695–700. [Google Scholar] [CrossRef]
- VanDolah, H.J.; Bauer, B.A.; Mauck, K.F. Clinicians’ guide to cannabidiol and hemp oils. Mayo Clin Proc. 2019, 94, 1840–1851. [Google Scholar] [CrossRef] [Green Version]
- Mazzarisi, E.L.; Swartzwelder, K.; Clements, P.T. Marijuana for Medical Use: Implications for Health Care Providers; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Jouanjus, E.; Raymond, V.; Lapeyre-Mestre, M.; Wolff, V. What is the current knowledge about the cardiovascular risk for users of cannabis-based products? A systematic review. Curr. Atheroscler. Rep. 2017, 19, 26. [Google Scholar] [CrossRef]
- DeFilippis, E.M.; Bajaj, N.S.; Singh, A.; Malloy, R.; Givertz, M.M.; Blankstein, R.; Bhatt, D.L.; Vaduganathan, M. Marijuana use in patients with cardiovascular disease: JACC review topic of the week. J. Am. Coll. Cardiol. 2020, 75, 320–332. [Google Scholar] [CrossRef]
- Franz, C.A.; Frishman, W.H. Marijuana use and cardiovascular disease. Cardiol. Rev. 2016, 24, 158–162. [Google Scholar] [CrossRef]
- Beaconsfield, P.; Ginsburg, J.; Rainsbury, R. Marihuana smoking: Cardiovascular effects in man and possible mechanisms. N. Engl. J. Med. 1972, 287, 209–212. [Google Scholar] [CrossRef]
- Mittleman, M.A.; Lewis, R.A.; Maclure, M.; Sherwood, J.B.; Muller, J.E. Triggering myocardial infarction by marijuana. Circulation 2001, 103, 2805–2809. [Google Scholar] [CrossRef] [Green Version]
- Nawrot, T.S.; Perez, L.; Künzli, N.; Munters, E.; Nemery, B. Public health importance of triggers of myocardial infarction: A comparative risk assessment. Lancet 2011, 377, 732–740. [Google Scholar] [CrossRef]
- DeFilippis, E.M.; Singh, A.; Divakaran, S.; Gupta, A.; Collins, B.L.; Biery, D.; Qamar, A.; Fatima, A.; Ramsis, M.; Pipilas, D.; et al. Cocaine and marijuana use among young adults with myocardial infarction. J. Am. Coll. Cardiol. 2018, 71, 2540–2551. [Google Scholar] [CrossRef] [PubMed]
- Rumalla, K.; Reddy, A.Y.; Mittal, M.K. Recreational marijuana use and acute ischemic stroke: A population-based analysis of hospitalized patients in the United States. J. Neurol. Sci. 2016, 364, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Desbois, A.C.; Cacoub, P. Cannabis-associated arterial disease. Ann. Vasc. Surg. 2013, 27, 996–1005. [Google Scholar] [CrossRef] [PubMed]
- Raheemullah, A.; Laurence, T.N. Repeated thrombosis after synthetic cannabinoid use. J. Emerg. Med. 2016, 51, 540–543. [Google Scholar] [CrossRef] [PubMed]
- Korantzopoulos, P.; Liu, T.; Papaioannides, D.; Li, G.; Goudevenos, J. Atrial fibrillation and marijuana smoking. Int. J. Clin. Pract. 2008, 62, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Rezkalla, S.; Kloner, R.A. Cardiovascular effects of marijuana. Trends Cardiovasc. Med. 2019, 29, 403–407. [Google Scholar] [CrossRef]
- Rezkalla, S.H.; Sharma, P.; Kloner, R.A. Coronary no-flow and ventricular tachycardia associated with habitual marijuana use. Ann. Emerg. Med. 2003, 42, 365–369. [Google Scholar] [CrossRef]
- Akins, D.; Awdeh, M. Marijuana and second-degree AV block. South. Med. J. 1981, 74, 371–373. [Google Scholar] [CrossRef]
- Rodondi, N.; Pletcher, M.J.; Liu, K.; Hulley, S.B.; Sidney, S. Marijuana use, diet, body mass index, and cardiovascular risk factors (from the CARDIA study). Am. J. Cardiol. 2006, 98, 478–484. [Google Scholar] [CrossRef]
- Greenan, G.; Ahmad, S.B.; Anders, M.G.; Leeser, A.; Bromberg, J.S.; Niederhaus, S.V. Recreational marijuana use is not associated with worse outcomes after renal transplantation. Clin. Transplant. 2016, 30, 1340–1346. [Google Scholar] [CrossRef]
- Nickels, M.; Jain, A.; Sharma, R.; Orloff, M.; Tsoulfas, G.; Kashyap, R.; Bozorgzadeh, A. Polysubstance abuse in liver transplant patients and its impact on survival outcome. Exp. Clin. Transplant. 2007, 5, 680. [Google Scholar]
- Mohite, P.N.; Zeriouh, M.; Sáez, D.G.; Popov, A.F.; Sabashnikov, A.; Zych, B.; Padukone, A.; Fazekas, L.; Ananiadou, O.; De Robertis, F.; et al. Influence of history of cannabis smoking in selected donors on the outcomes of lung transplantation. Eur. J. Cardio Thorac. Surg. 2017, 51, 142–147. [Google Scholar] [CrossRef]
- Xu, D.S.; Hartman, D.; Ludrosky, K.; Campbell, J.; Starling, R.C.; Taylor, D.O.; Smedira, N.O.; Gonzales-Stawinski, G.V. Impact of donor high-risk social behaviors on recipient survival in cardiac transplantation. Transplantation. 2010, 89, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Hauser, N.; Sahai, T.; Richards, R.; Roberts, T. High on cannabis and calcineurin inhibitors: A word of warning in an era of legalized marijuana. Case Rep. Transplant. 2016, 2016, 4028492. [Google Scholar] [CrossRef] [Green Version]
- DeFilippis, E.M.; Givertz, M.M. Marijuana use and candidacy for heart transplantation. J. Heart Lung Transplant. 2019, 38, 589–592. [Google Scholar] [CrossRef]
- Hamadeh, R.; Ardehali, A.; Locksley, R.M.; York, M.K. Fatal aspergillosis associated with smoking contaminated marijuana, in a marrow transplant recipient. Chest 1988, 94, 432–433. [Google Scholar] [CrossRef] [Green Version]
- Marks, W.H.; Florence, L.; Lieberman, J.; Chapman, P.; Howard, D.; Roberts, P.; Perkinson, D. Successfully treated invasive pulmonary aspergillosis associated with smoking marijuana in a renal transplant recipient. Transplantation. 1996, 61, 1771–1774. [Google Scholar] [CrossRef]
- Volkow, N.D.; Swanson, J.M.; Evins, A.E.; DeLisi, L.E.; Meier, M.H.; Gonzalez, R.; Bloomfield, M.A.P.; Curran, H.V.; Baller, R. Effects of cannabis use on human behavior, including cognition, motivation, and psychosis: A review. JAMA Psychiatry. 2016, 73, 292–297. [Google Scholar] [CrossRef]
- Zhou, Y.; Leri, F. Neuroscience of opiates for addiction medicine: From stress-responsive systems to behavior. In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2016; Volume 223, pp. 237–251. [Google Scholar]
- Wilson, N. Drug and opioid-involved overdose deaths—United States, 2017–2018. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 290. [Google Scholar] [CrossRef] [Green Version]
- Lentine, K.L.; Shah, K.S.; Kobashigawa, J.A.; Xiao, H.; Zhang, Z.; Axelrod, D.A.; Lam, N.N.; Segev, D.L.; McAdams-de Marco, M.A.; Randall, H.; et al. Prescription opioid use before and after heart transplant: Associations with posttransplant outcomes. Am. J. Transplant. 2019, 19, 3405–3414. [Google Scholar] [CrossRef] [PubMed]
- Lucas, P. Cannabis as an adjunct to or substitute for opiates in the treatment of chronic pain. J. Psychoact. Drugs 2012, 44, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Lucas, P.; Reiman, A.; Earleywine, M.; McGowan, S.K.; Oleson, M.; Coward, M.P.; Thomas, B. Cannabis as a substitute for alcohol and other drugs: A dispensary-based survey of substitution effect in Canadian medical cannabis patients. Addict. Res. Theory 2013, 21, 435–442. [Google Scholar] [CrossRef]
- Dobbels, F.; De Geest, S.; Van Cleemput, J.; Droogne, W.; Vanhaecke, J. Effect of late medication non-compliance on outcome after heart transplantation: A 5-year follow-up. J. Heart Lung Transplant. 2004, 23, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Dew, M.A.; DiMartini, A.F.; Steel, J.; De Vito Dabbs, A.; Myaskovsky, L.; Unruh, M.; Greenhouse, J. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs. Liver Transplant. 2008, 14, 159–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olt, C.; Faulkenberg, K.D.; Hsich, E.M. The growing dilemma of legalized cannabis and heart transplantation. J. Heart Lung Transplant. 2021, 40, 863–871. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| System | Potential Adverse Effects | References |
|---|---|---|
| Cardiovascular |
| [40,41] |
| [46,47,48,49] | |
| [43] | |
| [44,45] | |
| Pulmonary |
| [25] |
| Drug Interaction |
| [55,56] |
| Infectious Disease |
| [57,58] |
| Psychosocial |
| [59] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, H.; Fraser, M.; Agdamag, A.C.; Maharaj, V.; Nzemenoh, B.; Martin, C.M.; Alexy, T.; Garry, D.J. Cardiac Transplantation and the Use of Cannabis. Life 2021, 11, 1063. https://doi.org/10.3390/life11101063
Shah H, Fraser M, Agdamag AC, Maharaj V, Nzemenoh B, Martin CM, Alexy T, Garry DJ. Cardiac Transplantation and the Use of Cannabis. Life. 2021; 11(10):1063. https://doi.org/10.3390/life11101063
Chicago/Turabian StyleShah, Hirak, Meg Fraser, Arianne C. Agdamag, Valmiki Maharaj, Bellony Nzemenoh, Cindy M. Martin, Tamas Alexy, and Daniel J. Garry. 2021. "Cardiac Transplantation and the Use of Cannabis" Life 11, no. 10: 1063. https://doi.org/10.3390/life11101063