Effects of Kinesiology Taping on Shoulder Posture and Peak Torque in Junior Baseball Players with Rounded Shoulder Posture: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
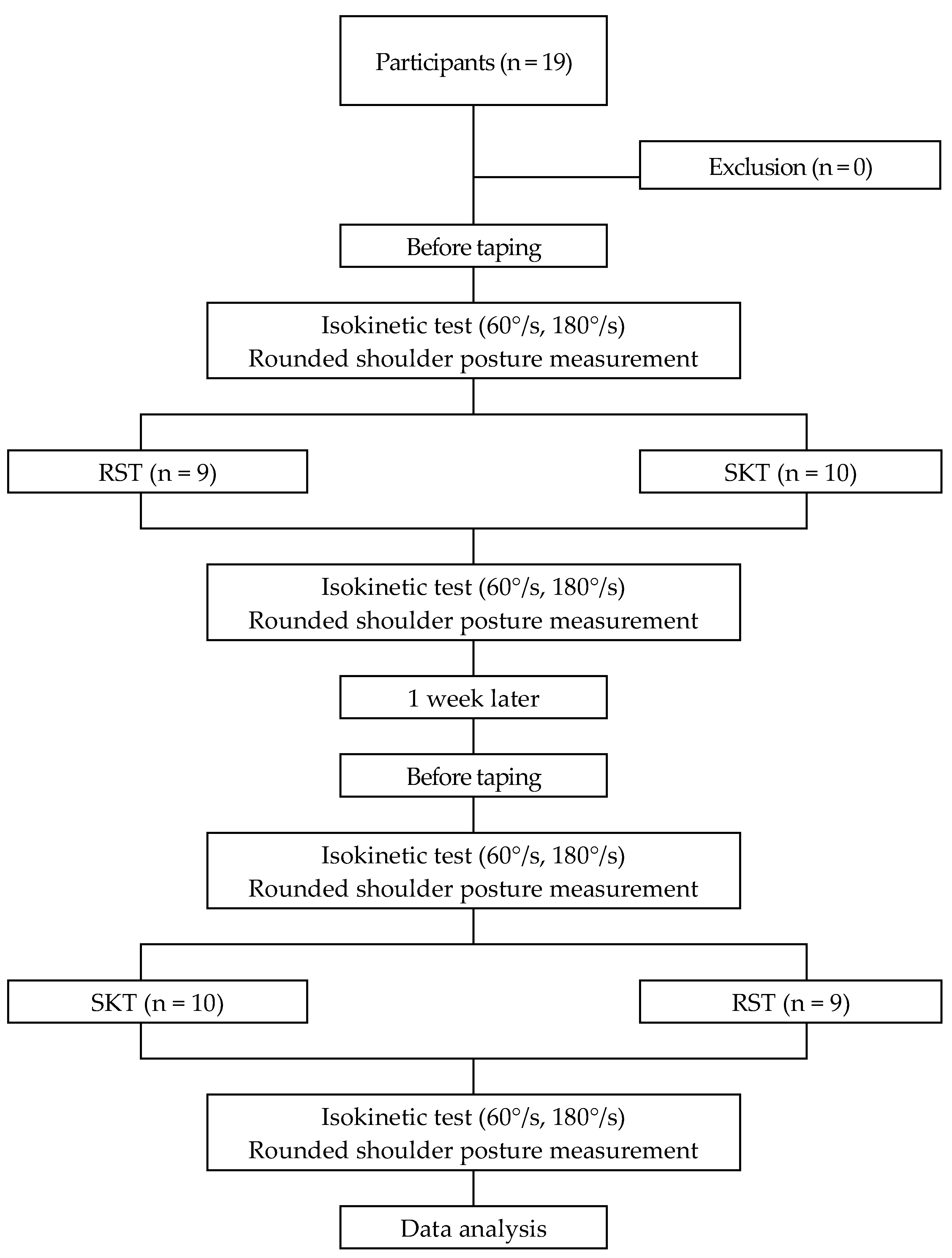
2.1. Study Design
2.2. Participants
2.3. Sample Size
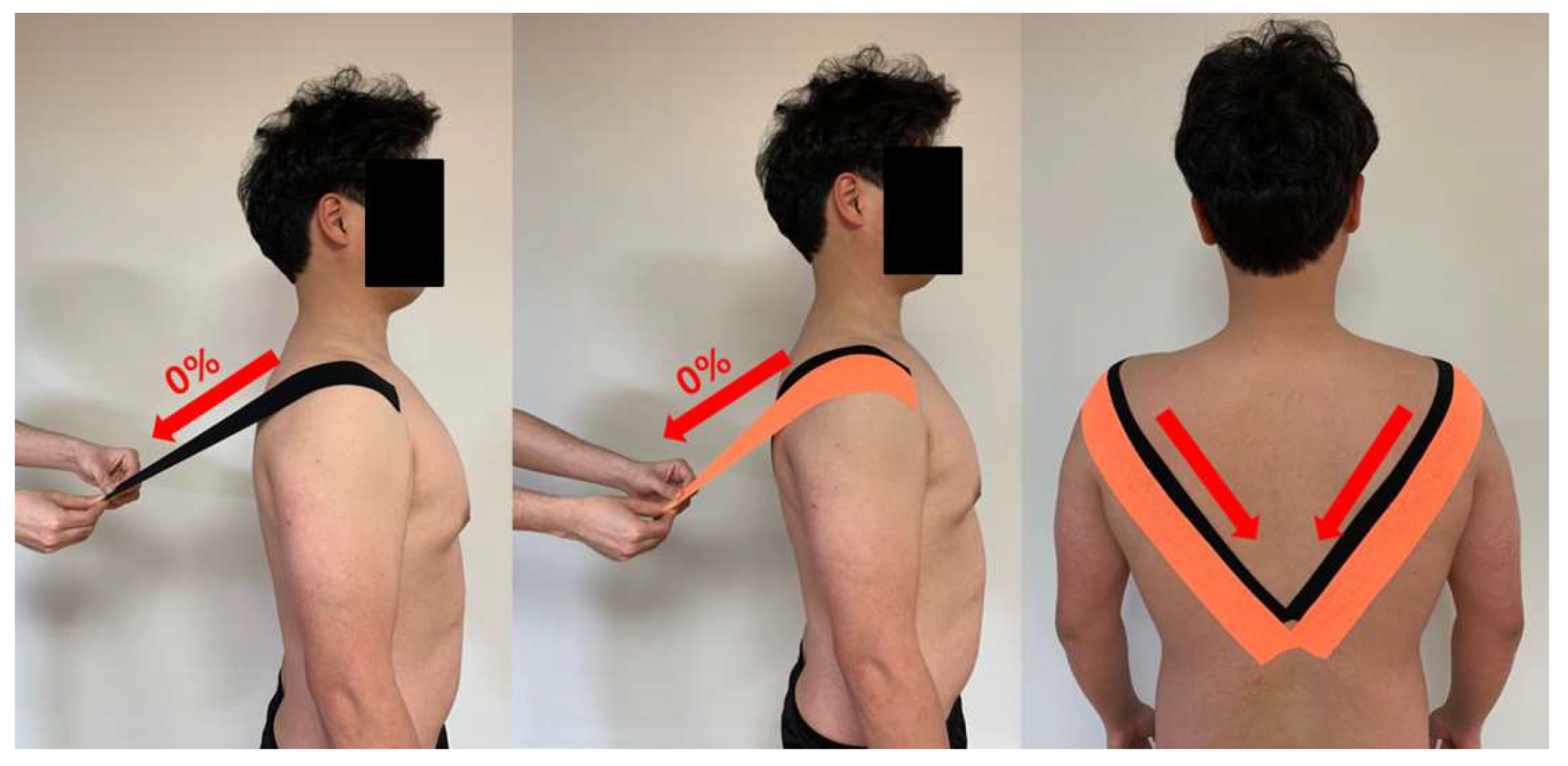
2.4. Kinesiology Tape Application
2.4.1. Rounded Shoulder Taping
2.4.2. Sham Kinesiology Taping
2.5. Measurement
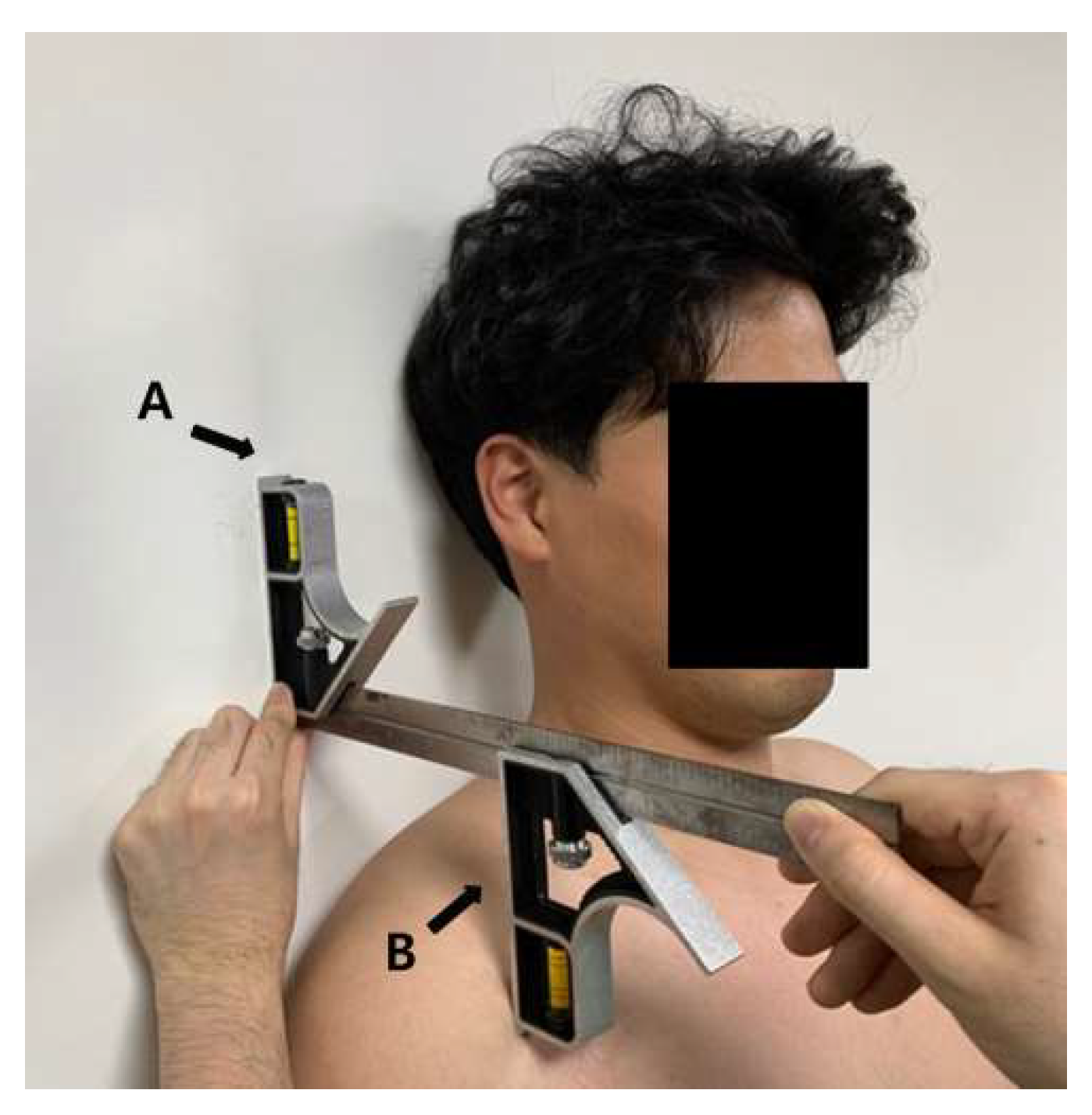
2.5.1. Two 12-in Combination Square
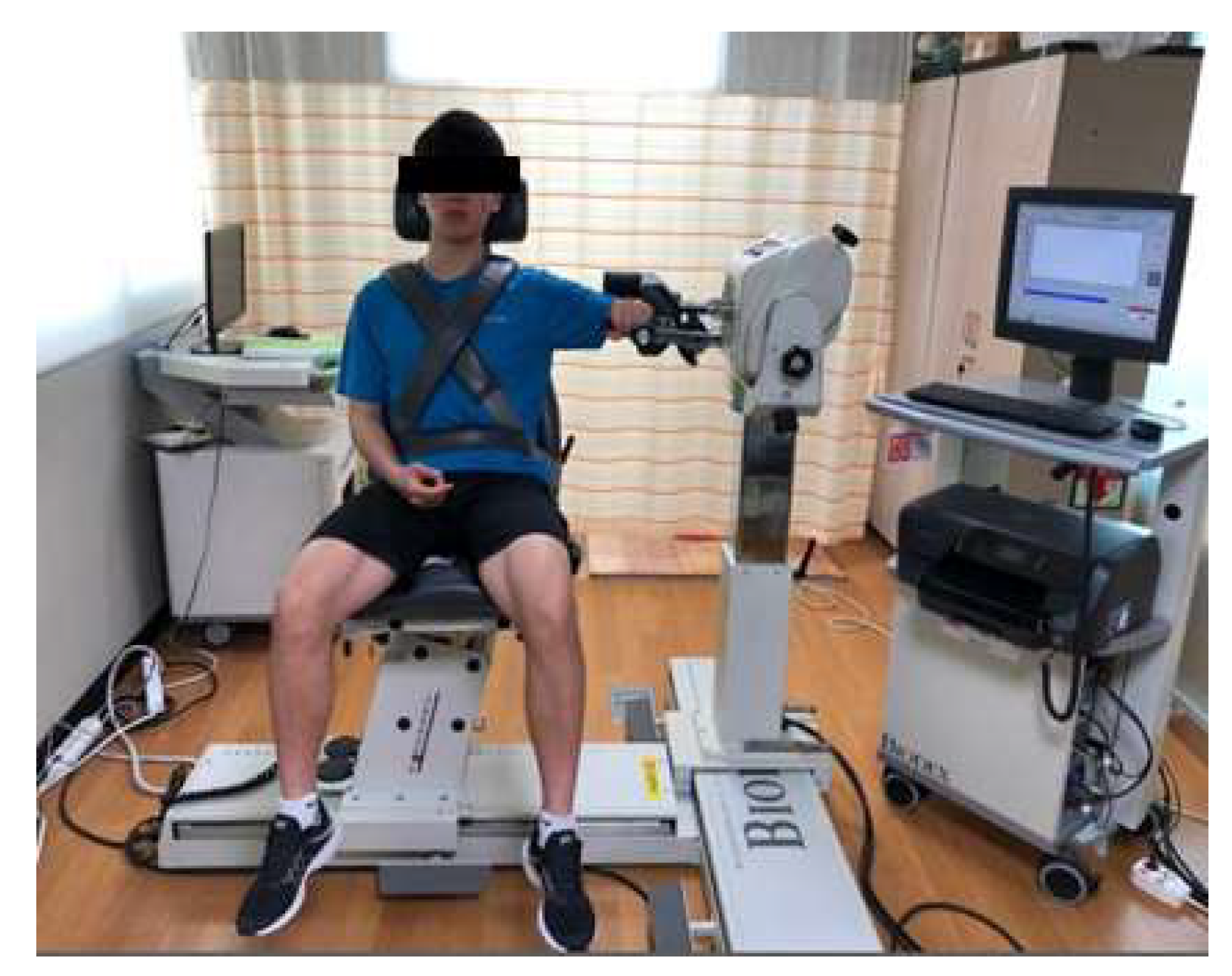
2.5.2. Isokinetic Equipment
2.6. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Changes in Shoulder Posture
3.3. Changes in Shoulder Peak Torque
4. Discussion
4.1. Relationship between Kinesiology Taping and RSP
4.2. Relationship between Kinesiology Taping and Shoulder Peak Torque
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alizadehkhaiyat, O.; Hawkes, D.H.; Kemp, G.J.; Frostick, S.P. Electromyographic analysis of the shoulder girdle musculature during external rotation exercises. Orthop. J. Sports Med. 2015, 3, 2325967115613988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escamilla, R.F.; Andrews, J.R. Shoulder muscle recruitment patterns and related biomechanics during upper extremity sports. Sports Med. 2009, 39, 569–590. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.B.; Laudner, K.G.; Pasquale, M.R.; Bradley, J.P.; Lephart, S.M. Scapular position and orientation in throwing athletes. Am. J. Sports Med. 2005, 33, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B. The role of the scapula in athletic shoulder function. Am. J. Sports Med. 1998, 26, 325–337. [Google Scholar] [CrossRef]
- Borich, M.R.; Bright, J.M.; Lorello, D.J.; Cieminski, C.J.; Buisman, T.; Ludewig, P.M. Scapular angular positioning at end range internal rotation in cases of glenohumeral internal rotation deficit. J. Orthop. Sports Phys. Ther. 2006, 36, 926–934. [Google Scholar] [CrossRef]
- Macrina, L.C.; Wilk, K.E.; Geus, J.J.; Porterfield, R. The effects of throwing on scapula position in professional baseball pitchers. J. Orthop. Sports Phys. Ther. 2007, 37, A69. [Google Scholar]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G. Muscles. Testing and Function, 4th ed.; Williams &Wilkins: Baltimore, MD, USA, 1993. [Google Scholar]
- Sahrmann, S. Diagnosis and Treatment of Movement Impairment Syndromes, 1st ed.; Mosby: St. Louis, MO, USA, 2002. [Google Scholar]
- Wong, C.K.; Coleman, D.; diPersia, V.; Song, J.; Wright, D. The effects of manual treatment on rounded-shoulder posture, and associated muscle strength. J. Bodyw. Mov. Ther. 2010, 14, 326–333. [Google Scholar] [CrossRef]
- Phillip, P.; Clare, F.; Robert, L. Assessment and Treatment of Muscle Imbalance: The Janda Approach; Human Kinetics: Windsor, ON, Canada, 2009. [Google Scholar]
- Roddey, T.S.; Olson, S.L.; Grant, S.E. The effects of pectoralis muscle stretching on the resting position of the scapula in persons with varying degrees of forward head/rounded shoulder posture. J. Man. Manip. Ther. 2013, 10, 124–128. [Google Scholar] [CrossRef]
- Seo, S.H.; Jeon, I.H.; Cho, Y.H.; Lee, H.G.; Hwang, Y.T.; Jang, J.H. Surface EMG during the Push-up plus Exercise on a Stable Support or Swiss Ball: Scapular Stabilizer Muscle Exercise. J. Phys. Ther. Sci. 2013, 25, 833–837. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Cynn, H.S.; Yoon, T.L.; Ko, C.H.; Choi, W.J.; Choi, S.A.; Choi, B.S. The effect of scapular posterior tilt exercise, pectoralis minor stretching, and shoulder brace on scapular alignment and muscles activity in subjects with round-shoulder posture. J. Electromyogr. Kinesiol. 2013, 25, 107–114. [Google Scholar] [CrossRef]
- Karlsson, J.; Andreasson, G.O. The effect of external ankle support in chronic lateral ankle joint instability. An electromyographic study. Am. J. Sports Med. 1992, 20, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Hinman, R.S.; Crossley, K.M.; McConnell, J.; Bennell, K.L. Efficacy of knee tape in the management of osteoarthritis of the knee: Blinded randomised controlled trial. BMJ 2003, 327, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Muro, F.; Rodríguez-Fernández, A.L.; Herrero-de-Lucas, A. Treatment of myofascial pain in the shoulder with Kinesio taping. A case report. Man. Ther. 2010, 15, 292–295. [Google Scholar] [CrossRef] [PubMed]
- Grześkowiak, M.; Szulc, P.; Szwedziak, M.; Lewandowski, J. The effect of the Kinesio Taping method on spinal motion and physiological spinal curvatures. Literature review. Ortop. Traumatol. Rehabil. 2014, 16, 221–226. [Google Scholar] [PubMed]
- Richardson, C.A.; Snijders, C.J.; Hides, J.A.; Damen, L.; Pas, M.S.; Storm, J. The relation between the transversus abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine 2002, 27, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yoo, W.G. Effect of scapular elevation taping on scapular depression syndrome: A case report. J. Back Musculoskelet. Rehabil. 2012, 25, 187–191. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.J.; Lee, J.H. Effects of scapula-upward-taping using kinesiology tape in a patient with shoulder pain caused by scapular downward rotation. J. Phys. Ther. Sci. 2015, 27, 547–548. [Google Scholar] [CrossRef] [Green Version]
- Tooth, C.; Schwartz, C.; Colman, D.; Croisier, J.; Bornheim, S.; Brüls, O.; Denoël, V.; Forthomme, B. kinesiotaping for scapular dyskinesis: The influence on scapular kinematics and on the activity of scapular stabilizing muscles. J. Electomyogr. Kinesiol. 2020, 51, 102400. [Google Scholar] [CrossRef]
- Pstaszkowski, K.; Slupska, L.; Paprocka-Borowicz, M.; Kolcz-Trzesicka, A.; Zwierzchowski, K.; Halska, U.; Przestrzelska, M.; Mucha, D.; Rosińczuk, J. Comparison of the short-term outcomes after postisometric muscle relaxation or kinesio taping application for normalization of the upper trapezius muscle tone and the pain relief: A Preliminary Study. Evid. Based Complement. Altern. Med. 2015, 2015, 721938. [Google Scholar]
- Lee, J.H.; Yoo, W.G. Application of posterior pelvic tilt taping for the treatment of chronic low back pain with sacroiliac joint dysfunction and increased sacral horizontal angle. Phys. Ther. Sport. 2012, 13, 279–285. [Google Scholar] [CrossRef]
- Lee, J.H.; Yoo, W.G. The mechanical effect of anterior pelvic tilt taping on slump sitting by seated workers. Ind. Health 2011, 49, 403–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.T.; Lee, J.H.; Yoon, C.H. The mechanical effect of kinesiology tape on rounded shoulder posture in seated male workers: A single-blinded randomized controlled pilot study. Physiother. Theory Pract. 2015, 31, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Hwang-Bo, G.; Lee, J.H.; Kim, H.D. Efficacy of kinesiology taping for recovery of dominant upper back pain in female sedentary worker having a rounded shoulder posture. Technol. Health Care 2013, 21, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Laudner, K.G.; Moline, M.T.; Meister, K. The relationship between forward scapular posture and posterior shoulder tightness among baseball players. Am. J. Sports Med. 2010, 38, 2106–2112. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA; New York, NY, USA, 1988. [Google Scholar]
- Lee, J.H.; Choi, S.W. Balance Taping: Clinical Application of Elastic Therapeutic Tape for Musculoskeletal Disorders; Wetape, Inc.: Paju, Korea, 2016. [Google Scholar]
- Peterson, D.E.; Blankenship, K.R.; Robb, J.B.; Walker, M.J.; Bryan, J.M.; Stetts, D.M.; Mincey, L.M.; Simmons, G.E. Investigation of the validity and reliability of four objective techniques for measuring forward shoulder posture. J. Orthop. Sports Phys. Ther. 1997, 25, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Physical Therapy Association. Guide to Physical Therapist Practice. Second Edition. American Physical Therapy Association. Phys. Ther. 2001, 81, 9–746. [Google Scholar]
- Donald, A.N. Kinesiology of the Musculoskeletal System, 3rd ed.; Mosby: St. Louis, MO, USA, 2018. [Google Scholar]
- Sim, Y.J.; Byun, Y.H.; Yoo, J. Comparison of isokinetic muscle strength and muscle power by types of warm-up. J. Phys. Ther. Sci. 2015, 27, 1491–1494. [Google Scholar] [CrossRef] [Green Version]
- Alam, S.; Malhotra, D.; Munjal, J.; Chachra, A. Immediate effect of Kinesio taping on shoulder muscle strength and range of motion in healthy individuals: A randomised trial. Hong Kong Physiother. J. 2015, 33, 80–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feiring, D.C.; Ellenbecker, T.S.; Derscheid, G.L. Test-retest reliability of the biodex isokinetic dynamometer. J. Orthop. Sports Phys. Ther. 1990, 11, 298–300. [Google Scholar] [CrossRef]
- Sole, G.; Hamrén, J.; Milosavljevic, S.; Nicholson, H.; Sullivan, S.J. Test-retest reliability of isokinetic knee extension and flexion. Arch. Phys. Med. Rehabil. 2007, 88, 626–631. [Google Scholar] [CrossRef]
- Van Herzeele, M.; van Cingel, R.; Maenhout, A.; De Mey, K.; Cools, A. Does the application of kinesiotape change scapular kinematics in healthy female handball players? Int. J. Sports Med. 2013, 34, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Ozer, S.T.; Karabay, D.; Yesilyaprak, S.S. Taping to improve scapular dyskinesis, scapular upward rotation, and pectoralis minor length in overhead athletes. J. Athl. Train. 2018, 53, 1063–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, D.L.; Brockett, C.L.; Gregory, J.E.; Proske, U. The role of the length-tension curve in the control of movement. Adv. Exp. Med. Biol. 2002, 508, 489–494. [Google Scholar] [PubMed]
- Borstad, J.D.; Ludewig, P.M. Comparison of three stretches for the pectoralis minor muscle. J. Shoulder Elbow Surg. 2006, 15, 324–330. [Google Scholar] [CrossRef]
- Ekstrom, R.A.; Donatelli, R.A.; Soderberg, G.L. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J. Orthop. Sports Phys. Ther. 2003, 33, 247–258. [Google Scholar] [CrossRef]
- Harput, G.; Guney, H.; Toprak, U.; Colakoglu, F.; Baltaci, G. Acute effects of scapular Kinesio Taping® on shoulder rotator strength, ROM and acromiohumeral distance in asymptomatic overhead athletes. J. Sports Med. Phys. Fit. 2017, 57, 1479–1485. [Google Scholar]
- McQuade, K.J.; Smidt, G.L. Dynamic scapulohumeral rhythm: The effects of external resistance during elevation of the arm in the scapular plane. J. Orthop. Sports Phys. Ther. 1998, 27, 125–133. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Participant (n = 19) |
|---|---|
| Gender (male/female) | 19 (100%)/0 (0%) |
| Dominant (right/left) | 16 (84%)/3 (16%) |
| Age (years) | 17.42 ± 1.46 † |
| Height (cm) | 175.10 ± 4.45 |
| Weight (kg) | 80.05 ± 11.98 |
| Variables | Pre-Taping | Post-Taping | p |
|---|---|---|---|
| RST (cm) | 14.88 ± 1.63 † (15.25, 1.75) | 14.19 ± 1.63 (13.00, 2.25) | 0.00 * |
| SKT (cm) | 14.88 ± 1.63 (15.25, 1.75) | 14.81 ± 1.62 (15.25, 2.00) | 0.09 |
| Variable | RST | SKT | p |
|---|---|---|---|
| Distance (cm) | 0.68 ± 0.18 † (0.75, 0.25) | 0.06 ± 0.16 (0.00, 0.25) | 0.00 * |
| Variables | Pre-Taping | Post-Taping | p | |
|---|---|---|---|---|
| External rotation (Nm) | 60°/s | 27.70 ± 9.09 † (26.90, 16.80) | 29.26 ± 8.63 (28.90, 15.00) | 0.00 * |
| 180°/s | 23.93 ± 8.17 (23.20, 14.90) | 25.25 ± 8.30 (24.60, 12.70) | 0.02 * | |
| Internal rotation (Nm) | 60°/s | 39.57 ± 11.95 (39.70, 15.00) | 42.10 ± 10.80 (41.30, 13.30) | 0.02 * |
| 180°/s | 36.80 ± 10.29 (38.20, 19.70) | 39.05 ± 10.65 (41.70, 18.80) | 0.01 * | |
| Variables | Pre-Taping | Post-Taping | p | |
|---|---|---|---|---|
| External rotation (Nm) | 60°/s | 27.95 ± 8.81 † (24.90, 15.00) | 28.13 ± 9.21 (25.90, 13.40) | 0.72 |
| 180°/s | 24.36 ± 7.92 (23.80, 14.50) | 24.21 ± 8.04 (22.40, 12.00) | 0.38 | |
| Internal rotation (Nm) | 60°/s | 38.88 ± 11.77 (39.10, 17.60) | 37.77 ± 9.22 (39.30, 13.20) | 0.60 |
| 180°/s | 35.92 ± 9.91 (37.40, 15.50) | 35.46 ± 9.65 (36.90, 18.60) | 0.55 | |
| Variables | RST | SKT | p | |
|---|---|---|---|---|
| External rotation (Nm) | 60°/s | 1.56 ± 1.66 † (1.50, 2.40) | 0.18 ± 2.21 (0.30, 2.80) | 0.03 * |
| 180°/s | 1.31 ± 2.36 (1.70, 2.10) | −0.15 ± 1.26 (0.50, 2.30) | 0.02 * | |
| Internal rotation (Nm) | 60°/s | 2.52 ± 4.56 (2.00, 6.60) | −1.10 ± 5.42 (0.30, 7.90) | 0.03 * |
| 180°/s | 2.25 ± 3.54 (2.40, 2.60) | −0.45 ± 3.29 (1.70, 4.30) | 0.02 * | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, H.-g.; Lee, J.-H.; Choi, I.-R. Effects of Kinesiology Taping on Shoulder Posture and Peak Torque in Junior Baseball Players with Rounded Shoulder Posture: A Pilot Study. Life 2020, 10, 139. https://doi.org/10.3390/life10080139
Yun H-g, Lee J-H, Choi I-R. Effects of Kinesiology Taping on Shoulder Posture and Peak Torque in Junior Baseball Players with Rounded Shoulder Posture: A Pilot Study. Life. 2020; 10(8):139. https://doi.org/10.3390/life10080139
Chicago/Turabian StyleYun, Hyeong-geun, Jung-Hoon Lee, and Im-Rak Choi. 2020. "Effects of Kinesiology Taping on Shoulder Posture and Peak Torque in Junior Baseball Players with Rounded Shoulder Posture: A Pilot Study" Life 10, no. 8: 139. https://doi.org/10.3390/life10080139