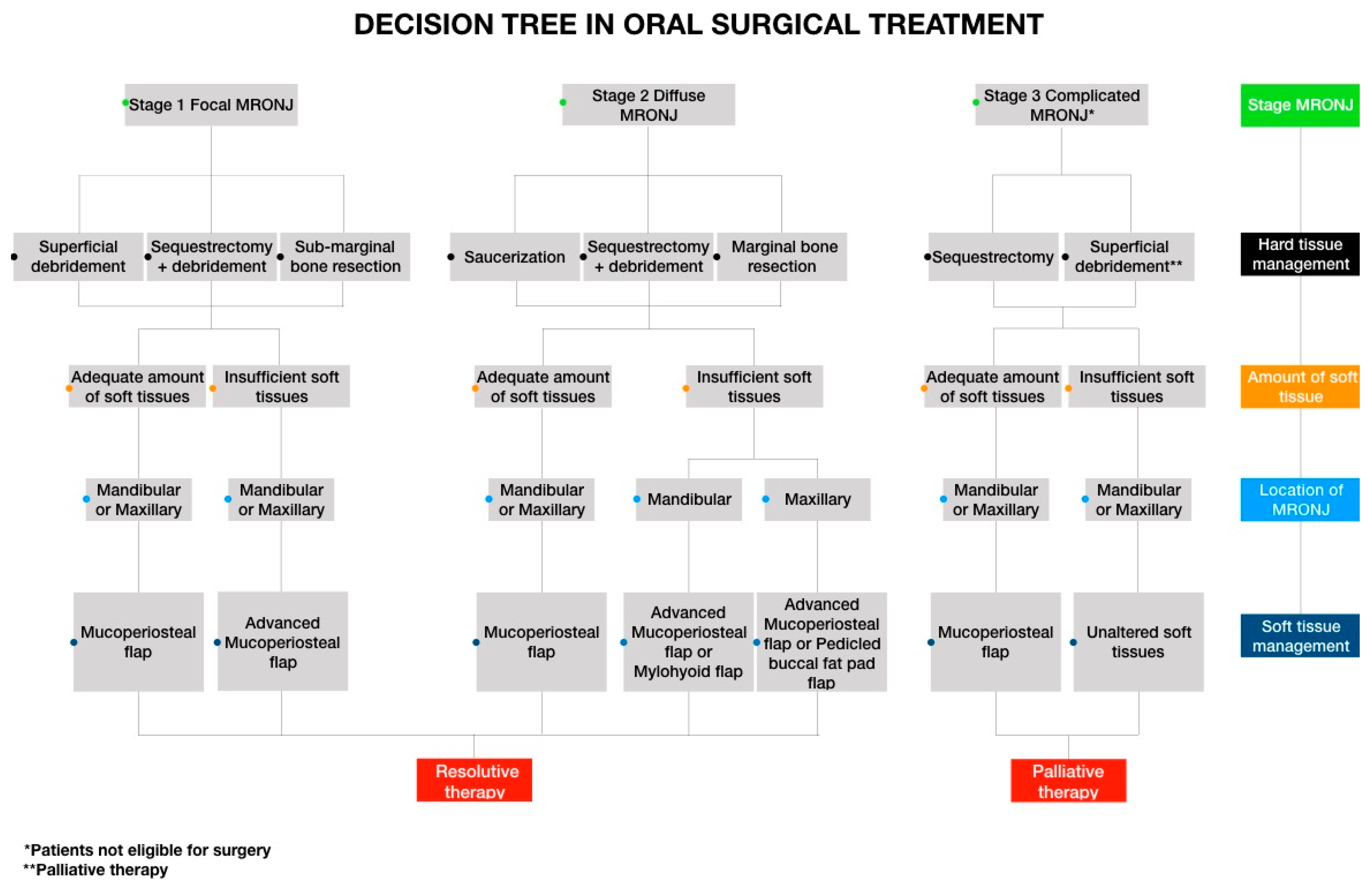
Oral Surgical Management of Bone and Soft Tissues in MRONJ Treatment: A Decisional Tree


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| MRONJ | Medication-related osteonecrosis of the jaws |
| BP | Bisphosphonates |
| SICMF | Italian Society of Maxillofacial Surgery |
| SIPMO | Italian Society of Oral Pathology and Oral Medicine |
References
- Yoneda, T.; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; Shibahara, T.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position paper 2017 of the Japanese allied committee on osteonecrosis of the jaw. J. Bone Miner. Metab. 2016, 35, 6–19. [Google Scholar] [CrossRef]
- Kim, H.Y.; Lee, S.-J.; Kim, S.-M.; Myoung, H.; Hwang, S.J.; Choi, J.-Y.; Lee, J.-H.; Choung, P.-H.; Kim, M.-J.; Seo, B.-M. Extensive surgical procedures result in better treatment outcomes for bisphosphonate-related osteonecrosis of the jaw in patients with osteoporosis. J. Oral Maxillofac. Surg. 2017, 75, 1404–1413. [Google Scholar] [CrossRef] [Green Version]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-related osteonecrosis of the jaw: MASCC/ISOO/ASCO clinical practice guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef]
- Beth-Tasdogan, N.H.; Mayer, B.; Hussein, H. Interventions for managing medication-related osteonecrosis of the jaw (MRONJ). Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Wilde, F.; Heufelder, M.; Winter, K.; Hendricks, J.; Frerich, B.; Schramm, A.; Hemprich, A. The role of surgical therapy in the management of intravenous bisphosphonates-related osteonecrosis of the jaw. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 111, 153–163. [Google Scholar] [CrossRef]
- Marcianò, A.; Peditto, M.; Cicciù, M.; Rubino, E.; Oteri, G. Role of local flaps to achieve primary wound closure in medication-related osteonecrosis of the jaws osseous-resective surgery. J. Craniofacial Surg. 2020, 31, e347–e352. [Google Scholar] [CrossRef]
- Ministero Della Salute, Agenzia Italiana del Farmaco (AIFA). Circolare AIFA del 3 Agosto 2007. Linee Guida per la Classificazione e Conduzione Degli Studi Osservazionali Sui Farmaci. Available online: http://xoomer.virgilio.it/pgiuff/osservazionali.pdf (accessed on 27 March 2017).
- Bedogni, A.; Fusco, V.; Agrillo, A.; Campisi, G. Learning from experience. Proposal of a refined definition and staging system for bisphosphonate-related osteonecrosis of the jaw (BRONJ). Oral Dis. 2012, 18, 621–623. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, A.; Fedele, S.; Bedogni, G.; Scoletta, M.; Favia, G.; Colella, G.; Agrillo, A.; Bettini, G.; Di Fede, O.; Oteri, G.; et al. Staging of osteonecrosis of the jaw requires computed tomography for accurate definition of the extent of bony disease. Br. J. Oral Maxillofac. Surg. 2014, 52, 603–608. [Google Scholar] [CrossRef]
- Oteri, G.; Trifirò, G.; Peditto, M.; Presti, L.L.; Marcianó, A.; Giorgianni, F.; Sultana, J. Treatment of medication-related osteonecrosis of the jaw and its impact on a patient’s quality of life: A single-center, 10-year experience from southern Italy. Drug Saf. 2017, 41, 111–123. [Google Scholar] [CrossRef]
- Ramaglia, L.; Guida, A.; Iorio-Siciliano, V.; Cuozzo, A.; Blasi, A.; Sculean, A. Stage-specific therapeutic strategies of medication-related osteonecrosis of the jaws: A systematic review and meta-analysis of the drug suspension protocol. Clin. Oral Investig. 2018, 22, 597–615. [Google Scholar] [CrossRef]
- Stanton, D.C.; Balasanian, E. Outcome of surgical management of bisphosphonate-related osteonecrosis of the jaws: Review of 33 surgical cases. J. Oral Maxillofac. Surg. 2009, 67, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Watters, A.L.; Hansen, H.J.; Williams, T.; Chou, J.F.; Riedel, E.; Halpern, J.; Tunick, S.; Bohle, G.; Huryn, J.; Estilo, C. Intravenous bisphosphonate–related osteonecrosis of the jaw: Long-term follow-up of 109 patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 192–200. [Google Scholar] [CrossRef]
- Ristow, O.; Rückschloß, T.; Bodem, J.; Berger, M.; Bodem, E.; Kargus, S.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Double-layer closure techniques after bone surgery of medication-related osteonecrosis of the jaw A single center cohort study. J. Cranio Maxillofac. Surg. 2018, 46, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Carlson, E.R.; Basile, J.D. The role of surgical resection in the management of bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2009, 67 (Suppl. S5), 85–95. [Google Scholar] [CrossRef] [PubMed]
- Pichardo, S.E.; Van Merkesteyn, J. Evaluation of a surgical treatment of denosumab-related osteonecrosis of the jaws. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 272–278. [Google Scholar] [CrossRef]
- Graziani, F.; Vescovi, P.; Campisi, G.; Favia, G.; Gabriele, M.; Gaeta, G.M.; Gennai, S.; Goia, F.; Miccoli, M.; Peluso, F.; et al. Resective surgical approach shows a high performance in the management of advanced cases of bisphosphonate-related osteonecrosis of the jaws: A retrospective survey of 347 cases. J. Oral Maxillofac. Surg. 2012, 70, 2501–2507. [Google Scholar] [CrossRef]
- Schubert, M.; Klatte, I.; Linek, W.; Müller, B.; Döring, K.; Eckelt, U.; Hemprich, A.; Berger, U.; Hendricks, J. The saxon bisphosphonate register—Therapy and prevention of bisphosphonate-related osteonecrosis of the jaws. Oral Oncol. 2012, 48, 349–354. [Google Scholar] [CrossRef]
- Bedogni, A.; Saia, G.; Bettini, G.; Tronchet, A.; Totola, A.; Bedogni, G.; Ferronato, G.; Nocini, P.F.; Blandamura, S. Long-term outcomes of surgical resection of the jaws in cancer patients with bisphosphonate-related osteonecrosis. Oral Oncol. 2011, 47, 420–424. [Google Scholar] [CrossRef]
- Stockmann, P.; Vairaktaris, E.; Wehrhan, F.; Seiss, M.; Schwarz, S.; Spriewald, B.; Neukam, F.-W.; Nkenke, E. Osteotomy and primary wound closure in bisphosphonate-associated osteonecrosis of the jaw: A prospective clinical study with 12 months follow-up. Support. Care Cancer 2009, 18, 449–460. [Google Scholar] [CrossRef]
- Lemound, J.; Eckardt, A.M.; Kokemüller, H.; Von See, C.; Voss, P.J.; Tavassol, F.; Rücker, M.; Rana, M.; Gellrich, N.-C. Bisphosphonate-associated osteonecrosis of the mandible: Reliable soft tissue reconstruction using a local myofascial flap. Clin. Oral Investig. 2011, 16, 1143–1152. [Google Scholar] [CrossRef]
- Favaloro, A.; Siniscalchi, E.N.; Cutroneo, G.; Catalfamo, L.; Santoro, G.; Allegra, A.; Oteri, G.; Cicciù, D.; Alonci, A.; Penna, G.; et al. Immunohistochemial evaluation of sarcoglycans and integrins in gingival epithelium of multiple myeloma patients with bisphosphonate-induced osteonecrosis of the jaw. Oncol. Rep. 2010, 24, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Adamo, V.; Ferraro, G.; Adamo, B.; Franchina, T.; Garipoli, C. Impact of integrated treatments on patient management in solid tumors: From diagnosis to palliative care. Forum 2006, 14, E1. [Google Scholar] [PubMed]
- Hinson, A.; Siegel, E.R.; Stack, B.C., Jr. Temporal correlation between bisphosphonate termination and symptom resolution in osteonecrosis of the jaw: A pooled case report analysis. J. Oral Maxillofac. Surg. 2015, 73, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Hoefert, S.; Yuan, A.; Munz, A.; Grimm, M.; ElAyouti, A.; Reinert, S. Clinical course and therapeutic outcomes of operatively and non-operatively managed patients with denosumab-related osteonecrosis of the jaw (DRONJ). J. Cranio Maxillofac. Surg. 2017, 45, 570–578. [Google Scholar] [CrossRef]
- Banca Dati Farmaci Dell’AIFA. Available online: https://farmaci.agenziafarmaco.gov.it/aifa/servlet/PdfDownloadServlet?pdfFileName=footer_002317_040108_RCP.pdf&retry=0&sys=m0b1l3 (accessed on 27 May 2020).
- Zirk, M.; Kreppel, M.; Buller, J.; Pristup, J.; Peters, F.; Dreiseidler, T.; Zinser, M.; Zöller, J.E. The impact of surgical intervention and antibiotics on MRONJ stage II and III—Retrospective study. J. Cranio Maxillofac. Surg. 2017, 45, 1183–1189. [Google Scholar] [CrossRef]
- Mücke, T.; Koschinski, J.; Deppe, H.; Wagenpfeil, S.; Pautke, C.; Mitchell, D.A.; Wolff, K.-D.; Hölzle, F. Outcome of treatment and parameters influencing recurrence in patients with bisphosphonate-related osteonecrosis of the jaws. J. Cancer Res. Clin. Oncol. 2010, 137, 907–913. [Google Scholar] [CrossRef]
- Blus, C.; Giannelli, G.; Szmukler-Moncler, S.; Orrù, G. Treatment of medication-related osteonecrosis of the jaws (MRONJ) with ultrasonic piezoelectric bone surgery. A case series of 20 treated sites. Oral Maxillofac. Surg. 2016, 21, 41–48. [Google Scholar] [CrossRef]
- Silva, L.F.; Curra, C.; Munerato, M.S.; DeAntoni, C.C.; Matsumoto, M.A.; Cardoso, C.L.; Curi, M.M. Surgical management of bisphosphonate-related osteonecrosis of the jaws: Literature review. Oral Maxillofac. Surg. 2015, 20, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Lemound, J.; Muecke, T.; Zeller, A.-N.; Lichtenstein, J.; Eckardt, A.M.; Gellrich, N.-C. Nasolabial flap improves healing in medication-related osteonecrosis of the jaw. J. Oral Maxillofac. Surg. 2018, 76, 877–885. [Google Scholar] [CrossRef]
- Rotaru, A.; Kim, M.-K.; Kim, S.-G.; Park, Y.-W. Pedicled buccal fat pad flap as a reliable surgical strategy for the treatment of medication-related osteonecrosis of the jaw. J. Oral Maxillofac. Surg. 2015, 73, 437–442. [Google Scholar] [CrossRef]
- Mozzati, M.; Gallesio, G.; Arata, V.; Pol, R.; Scoletta, M. Platelet-rich therapies in the treatment of intravenous bisphosphonate-related osteonecrosis of the jaw: A report of 32 cases. Oral Oncol. 2012, 48, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Yoo, H.-Y.; Kim, G.-T.; Lee, J.-W.; Lee, Y.-A.; Kim, K.-I.; Kwon, Y.-D. Short-term teriparatide and recombinant human bone morphogenetic protein-2 for regenerative approach to medication-related osteonecrosis of the jaw: A preliminary study. J. Bone Miner. Res. 2017, 32, 2445–2452. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | # (%) |
| Age Years (Mean) | 70.72 |
| Sex | - |
| Male | 27 (26.21%) |
| Female | 76 (73.78%) |
| Primary Disease | # (%) |
| Breast cancer | 24 (23.30%) |
| Prostate cancer | 16 (15.53%) |
| Kidney cancer | 1 (0.97%) |
| Multiple myeloma | 11 (10.67%) |
| Lung cancer | 1 (0.97%) |
| Gastrointestinal stromal tumors (GISTs) | 1 (0.97%) |
| Rheumatoid arthritis | 3 (2.91%) |
| Osteoporosis | 46 (44.66%) |
| Administered Antiresorptive Drug | # (%) |
| Zoledronate (i.v) | 37 (68.51%) |
| Denosumab 120 mg (subcutaneous) | 13 (24.07%) |
| Denosumab 60 mg (subcutaneous) | 2 (4.08%) |
| Alendronate (per os) | 28 (57.14%) |
| Ibandronate (per os) | 9 (18.36%) |
| Risedronate (per os) | 2 (4.08%) |
| Clodronate (i.m) | 1 (2.04%) |
| Switch Therapy | # (%) |
| Zoledronate (i.v) + Risedronate (per os) | 1 (2.04%) |
| Zoledronate (i.v) + Pamidronate (i.v) | 2 (3.70%) |
| Zoledronate (i.v) + Ibandronate (per os) | 1 (1.85%) |
| Alendronate (per os) + Risedronate (per os) | 2 (4.08%) |
| Alendronate (per os) + Ibandronate (per os) | 2 (4.08%) |
| Neridronate (i.v) + Ibandronate (per os) | 1 (2.04%) |
| Zoledronate (i.v) + Denosumab 120 mg (subcutaneous) | 1 (1.85%) |
| Zoledronate (i.v) + Denosumab 60 mg (subcutaneous) | 1 (2.04%) |
| Average Duration of Therapy | Months |
| Zoledronate (i.v) | 28.70 |
| Denosumab 120 mg (subcutaneous) | 26.92 |
| Denosumab 60 mg (subcutaneous) | 33.5 |
| Alendronate (per os) | 66.14 |
| Ibandronate (per os) | 95.11 |
| Risedronate (per os) | 78.5 |
| Clodronate (i.m) | 24 |
| Zoledronate (i.v) + Risedronate (per os) | 113 |
| Zoledronate (i.v) + Pamidronate (i.v) | 52.5 |
| Zoledronate (i.v) + Ibandronate (per os) | 65 |
| Alendronate (per os) + Risedronate (per os) | 85.5 |
| Alendronate (per os) + Ibandronate (per os) | 164.5 |
| Neridronate (i.v) + Ibandronate (per os) | 70 |
| Zoledronate (i.v) + Denosumab 120 mg (subcutaneous) | 24 |
| Zoledronate (i.v) + Denosumab 60 mg (subcutaneous) | 99 |
| Items | # (%) |
|---|---|
| Anatomic Location | - |
| Lower jaw | 74 (71.84%) |
| Upper jaw | 21 (20.38%) |
| Both jaws | 8 (7.76%) |
| SICMF-SIPMO Staging | Total (n = 111) (%) |
| Stage 1a Stage 1b | 13 (11.71%) 27 (24.32%) |
| Stage 2a Stage 2b | 11 (9.90%) 45 (40.54%) |
| Stage 3 | 15 (13.51%) |
| Stage and Location of MRONJ | Bone Surgery | Flap Management | Surgeries # (%) | Success # (%) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SD | SQ | SAU | SMBR | MBR | MPF | CAF | MYF | FPF | |||
| Stage I Mandibular bone | ✓ | - | - | - | - | ✓ | - | - | - | 5 (4.42%) | 4 (80%) |
| ✓ | - | - | - | - | - | ✓ | - | - | 8 (7.07%) | 8 (100%) | |
| - | - | - | ✓ | - | ✓ | - | - | - | 7 (6.19%) | 6 (85.71%) | |
| - | - | - | ✓ | - | - | ✓ | - | - | 15 (3.27%) | 13 (86.66%) | |
| ✓ | ✓ | - | - | - | ✓ | - | - | - | 1 (0.88%) | 1 (100%) | |
| Stage II Mandibular bone | - | - | ✓ | - | - | ✓ | - | - | - | 5 (4.42%) | 2 (40%) |
| - | - | ✓ | - | - | - | ✓ | - | - | 7 (6.19%) | 6 (85.71%) | |
| - | - | ✓ | - | - | - | - | ✓ | - | 4 (3.53%) | 4 (100%) | |
| - | - | - | - | ✓ | ✓ | - | - | - | 5 (4.42%) | 2 (60%) | |
| - | - | - | - | ✓ | - | ✓ | - | - | 14 (12.38%) | 11 (78.57%) | |
| - | - | - | - | ✓ | - | - | ✓ | - | 19 (16.81%) | 19 (100%) | |
| ✓ | ✓ | - | - | - | - | ✓ | - | - | 1 (0.88%) | 1 (100%) | |
| Stage I Maxillary bone | ✓ | - | - | - | - | ✓ | - | - | - | 1 (0.88%) | 1 (100%) |
| ✓ | - | - | - | - | - | ✓ | - | - | 2 (1.76%) | 2 (100%) | |
| - | - | - | ✓ | - | ✓ | - | - | - | 1 (0.88%) | 1 (100%) | |
| - | - | - | ✓ | - | - | ✓ | - | - | 2 (1.76%) | 2 (100%) | |
| ✓ | ✓ | - | - | - | ✓ | - | - | - | 1 (0.88%) | 1 (100%) | |
| Stage II Maxillary bone | - | - | ✓ | - | - | ✓ | - | - | - | 1 (0.88%) | 0 (0%) |
| - | - | ✓ | - | - | - | ✓ | - | - | 3 (2.65%) | 3 (100%) | |
| - | - | ✓ | - | - | - | - | - | ✓ | 2 (1.76%) | 2 (100%) | |
| - | - | - | - | ✓ | ✓ | - | - | - | 2 (1.76%) | 1 (50%) | |
| - | - | - | - | ✓ | - | ✓ | - | - | 4 (3.53%) | 3 (75%) | |
| - | - | - | - | ✓ | - | - | - | ✓ | 2 (1.76%) | 2 (100%) | |
| ✓ | ✓ | - | - | - | - | ✓ | - | - | 1 (0.88%) | 1 (100%) | |
| Patient # | 1st Procedure | Re-Entry Procedure | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bone Surgery | Flap Management | Bone Surgery | Flap Management | ||||||||||
| SD | SAU | SMBR | MBR | MPF | CAF | SD | SAU | SMBR | MBR | CAF | MYF | FPF | |
| 1 | - | ✓ | - | - | ✓ | - | - | - | - | ✓ | - | ✓ | - |
| 2 | - | ✓ | - | - | ✓ | - | - | - | - | ✓ | - | ✓ | - |
| 3 | - | ✓ | - | - | ✓ | - | - | - | - | ✓ | - | ✓ | - |
| 4 | - | - | - | ✓ | ✓ | - | - | - | - | ✓ | - | ✓ | - |
| 5 | - | - | - | ✓ | - | ✓ | - | - | - | ✓ | - | ✓ | - |
| 6 | - | ✓ | - | - | ✓ | - | - | ✓ | - | - | ✓ | - | - |
| 7 | - | - | - | ✓ | ✓ | - | - | - | - | ✓ | - | ✓ | - |
| 8 | ✓ | - | - | - | ✓ | - | ✓ | - | - | - | ✓ | - | - |
| 9 | ✓ | - | - | - | ✓ | - | - | - | ✓ | - | ✓ | - | - |
| 10 | - | - | - | ✓ | - | ✓ | - | - | - | ✓ | - | ✓ | - |
| 11 | - | - | - | ✓ | - | ✓ | - | - | - | ✓ | - | ✓ | - |
| 12 | - | - | - | ✓ | ✓ | - | - | - | - | ✓ | ✓ | - | - |
| 13 | - | - | - | ✓ | - | ✓ | - | - | - | ✓ | - | - | ✓ |
| 14 | - | - | ✓ | - | ✓ | - | - | - | ✓ | - | ✓ | - | - |
| 15 | - | - | - | ✓ | ✓ | - | - | - | - | ✓ | ✓ | - | - |
| 16 | - | - | ✓ | - | - | ✓ | - | - | - | ✓ | ✓ | - | - |
| Patient | Localization | Surgical Techniques | Outcome | ||
|---|---|---|---|---|---|
| SD | SQ | MPF | |||
| 1 | Maxillary | ✓ | - | ✓ | Partial Healing |
| Mandibular | ✓ | - | - | Unchanged | |
| 2 | Maxillary | ✓ | - | - | Unchanged |
| 3 | Mandibular | ✓ | - | ✓ | Worsened |
| 4 | Maxillary | - | ✓ | ✓ | Partial Healing |
| 5 | Maxillary | ✓ | - | - | Worsened |
| 6 | Mandibular | ✓ | - | ✓ | Partial Healing |
| 7 | Maxillary | ✓ | - | ✓ | Partial Healing |
| 8 | Maxillary | - | ✓ | ✓ | Partial Healing |
| 9 | Mandibular | ✓ | - | - | Unchanged |
| 10 | Mandibular | ✓ | - | ✓ | Partial Healing |
| 11 | Maxillary | ✓ | - | ✓ | Partial Healing |
| 12 | Maxillary | ✓ | - | - | Unchanged |
| 13 | Maxillary | ✓ | - | ✓ | Partial Healing |
| 14 | Maxillary | ✓ | - | - | Unchanged |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcianò, A.; Rubino, E.; Peditto, M.; Mauceri, R.; Oteri, G. Oral Surgical Management of Bone and Soft Tissues in MRONJ Treatment: A Decisional Tree. Life 2020, 10, 99. https://doi.org/10.3390/life10070099
Marcianò A, Rubino E, Peditto M, Mauceri R, Oteri G. Oral Surgical Management of Bone and Soft Tissues in MRONJ Treatment: A Decisional Tree. Life. 2020; 10(7):99. https://doi.org/10.3390/life10070099
Chicago/Turabian StyleMarcianò, Antonia, Erasmo Rubino, Matteo Peditto, Rodolfo Mauceri, and Giacomo Oteri. 2020. "Oral Surgical Management of Bone and Soft Tissues in MRONJ Treatment: A Decisional Tree" Life 10, no. 7: 99. https://doi.org/10.3390/life10070099