Health-Related Quality of Life and Frailty in Chronic Liver Diseases

Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Questionnaire
2.3. Our Study
2.4. Statistical Considerations
3. Results
3.1. Patient Baseline Data
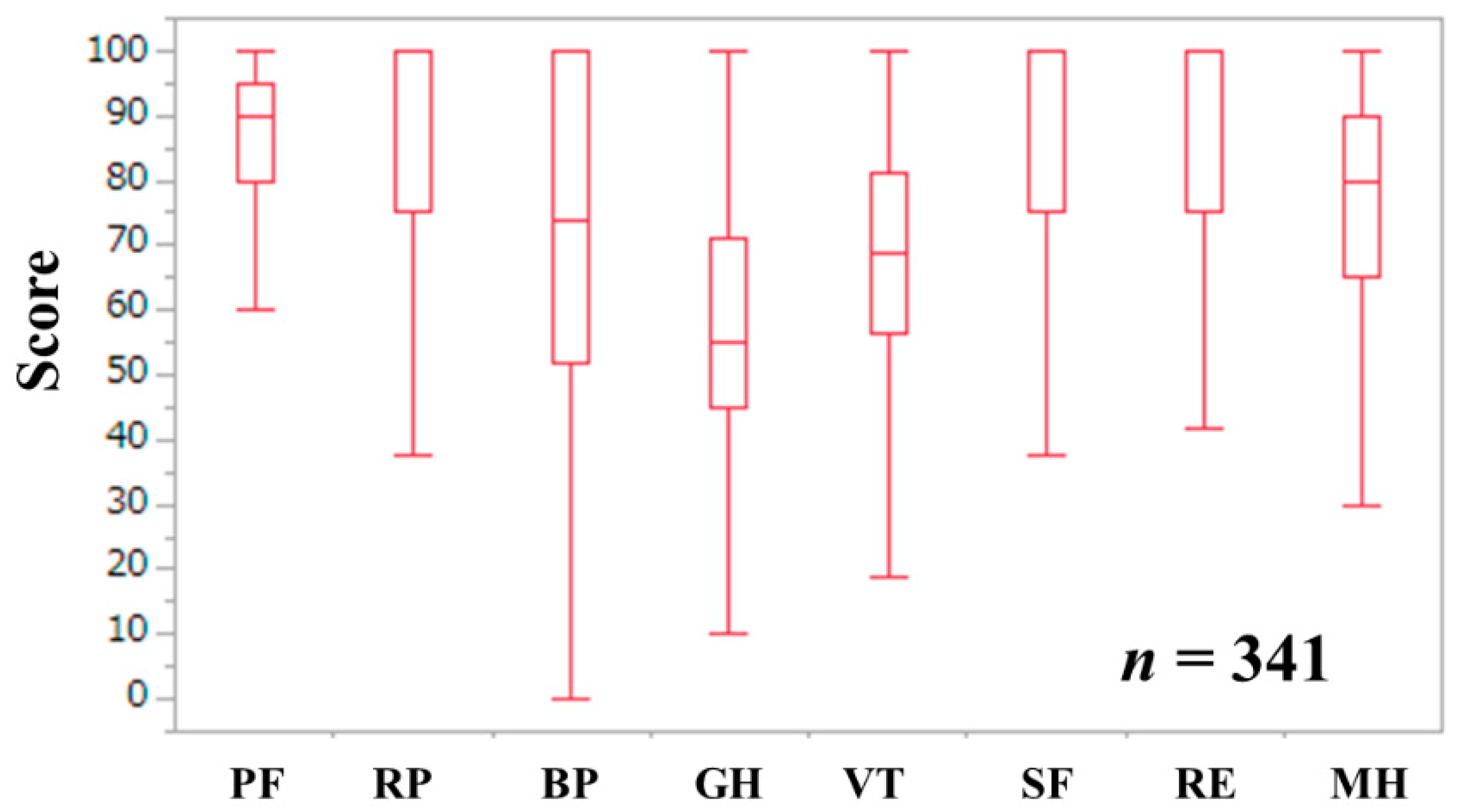
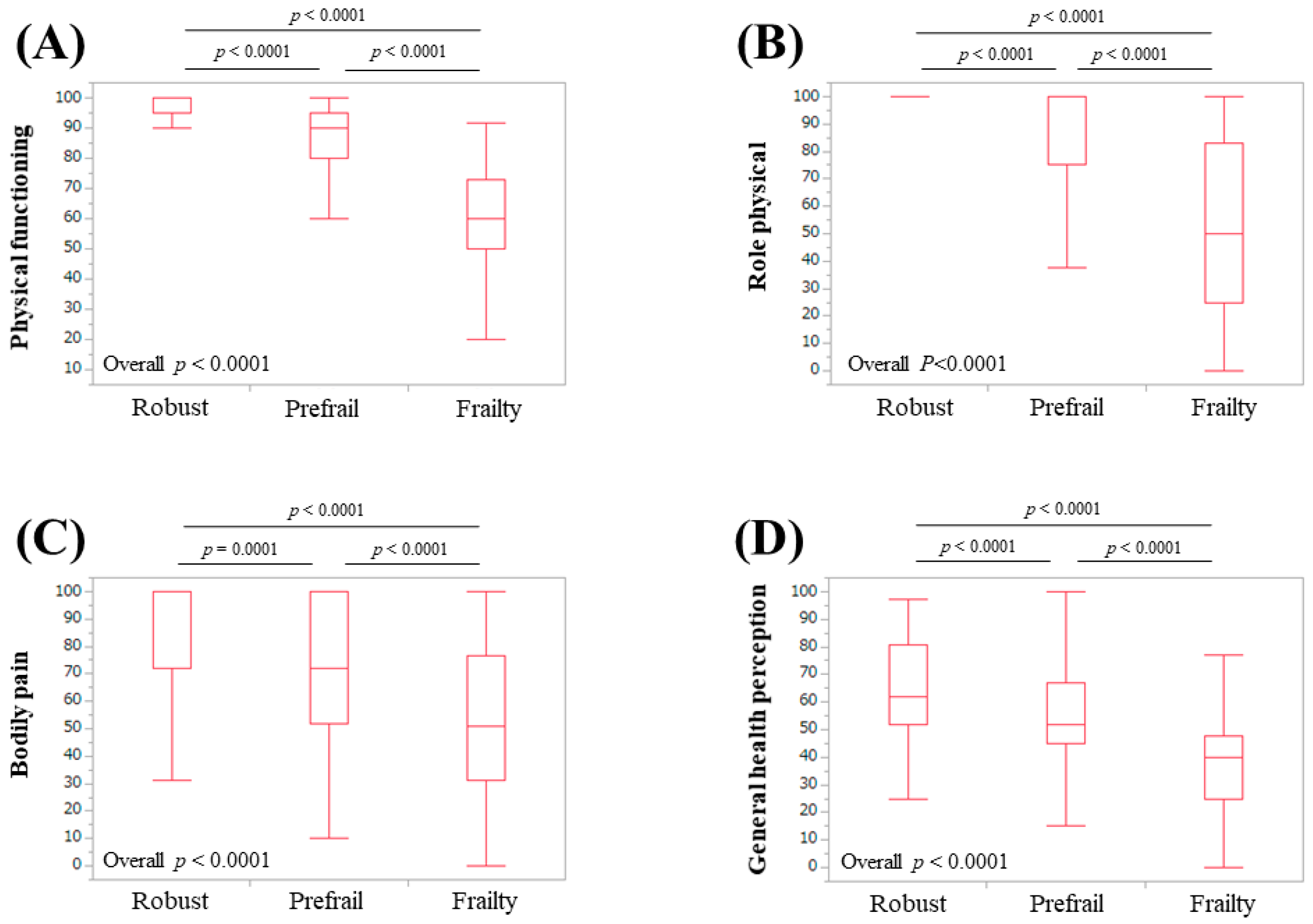
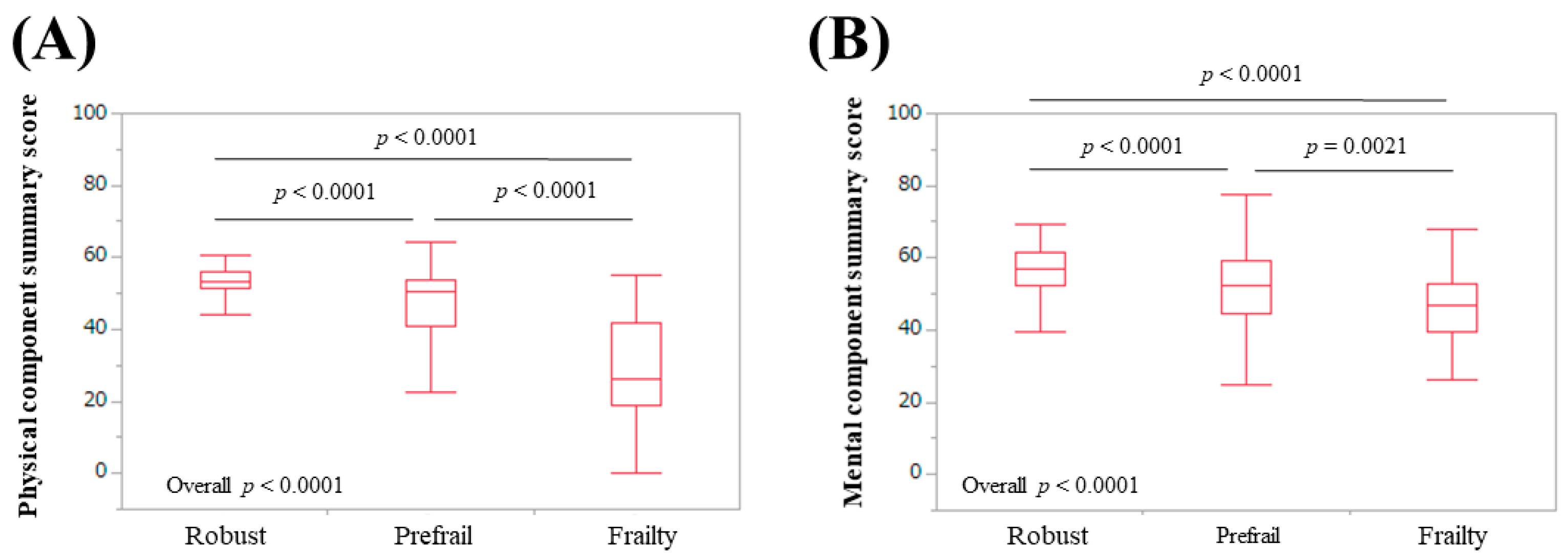
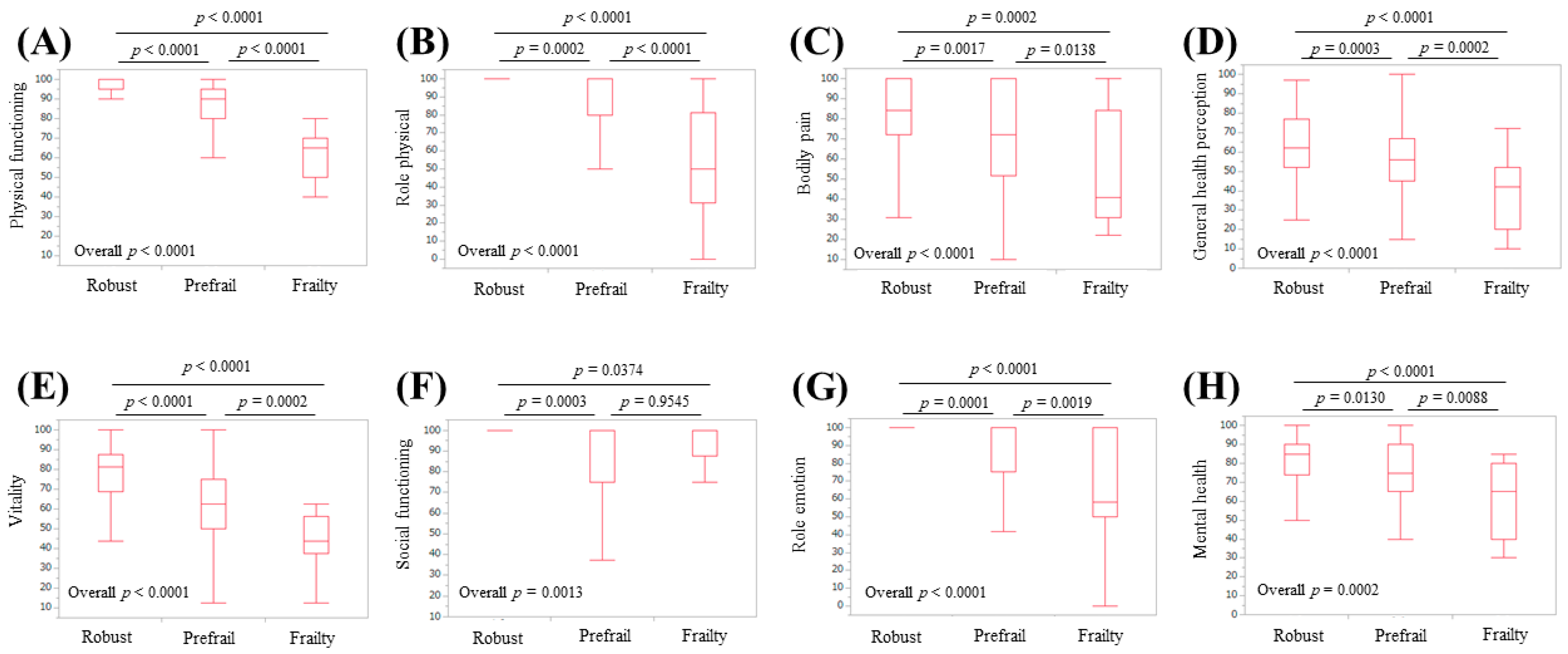
3.2. Scores of the Eight Scales of the SF-36, the PCS, and the MCS Relative to the Frailty Status
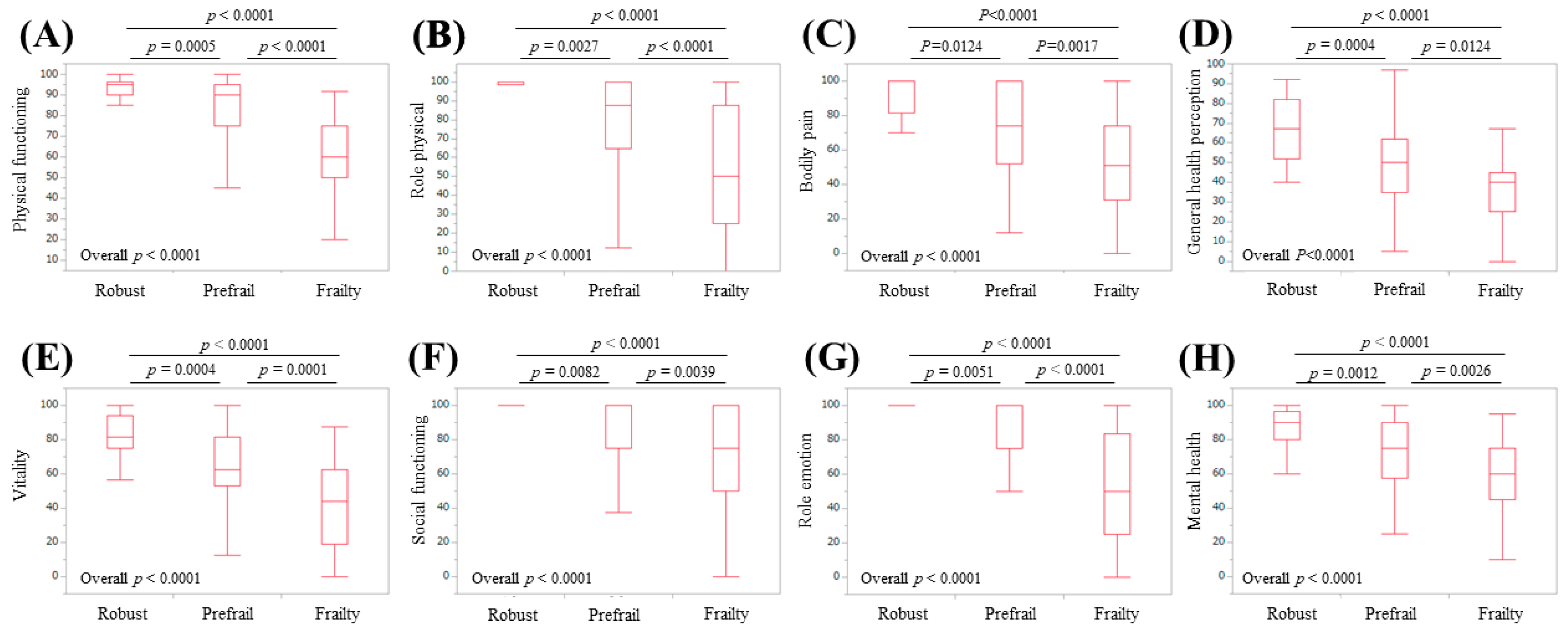
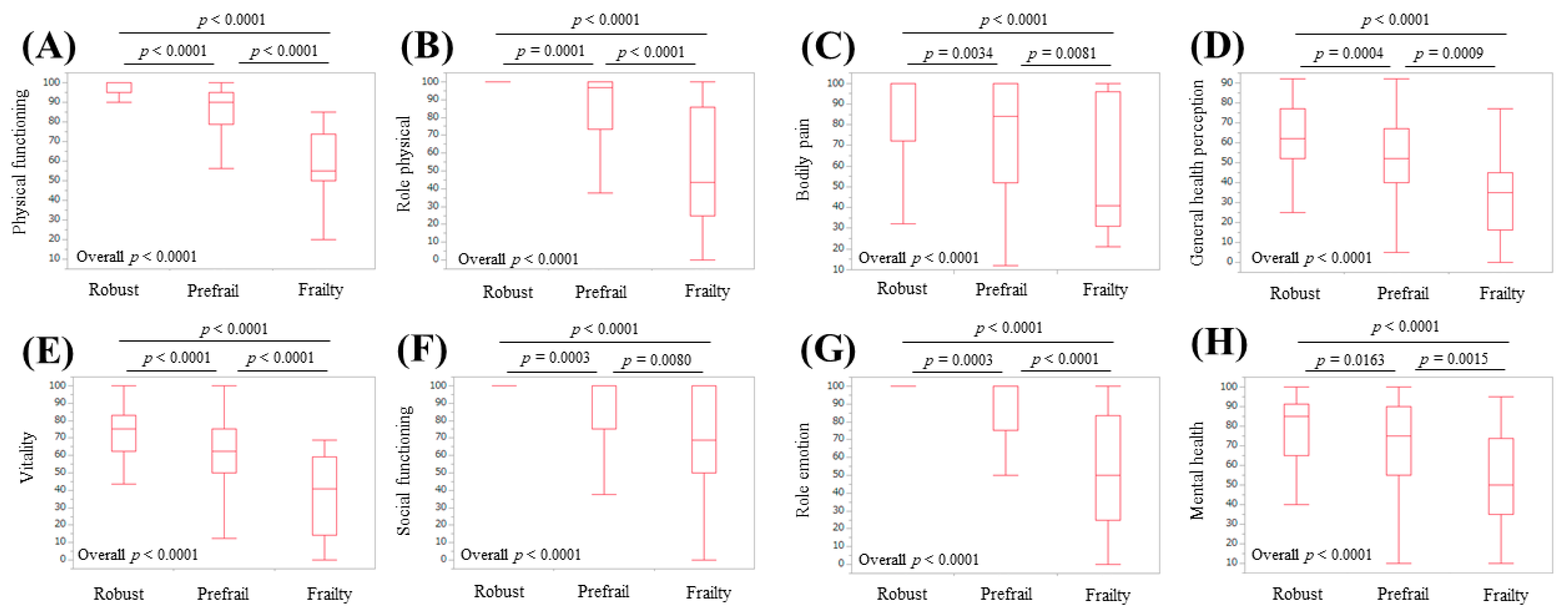
3.3. Subgroup Analysis 1: Scores of the Eight Scales of the SF-36 Relative to the Frailty Status in LC Patients
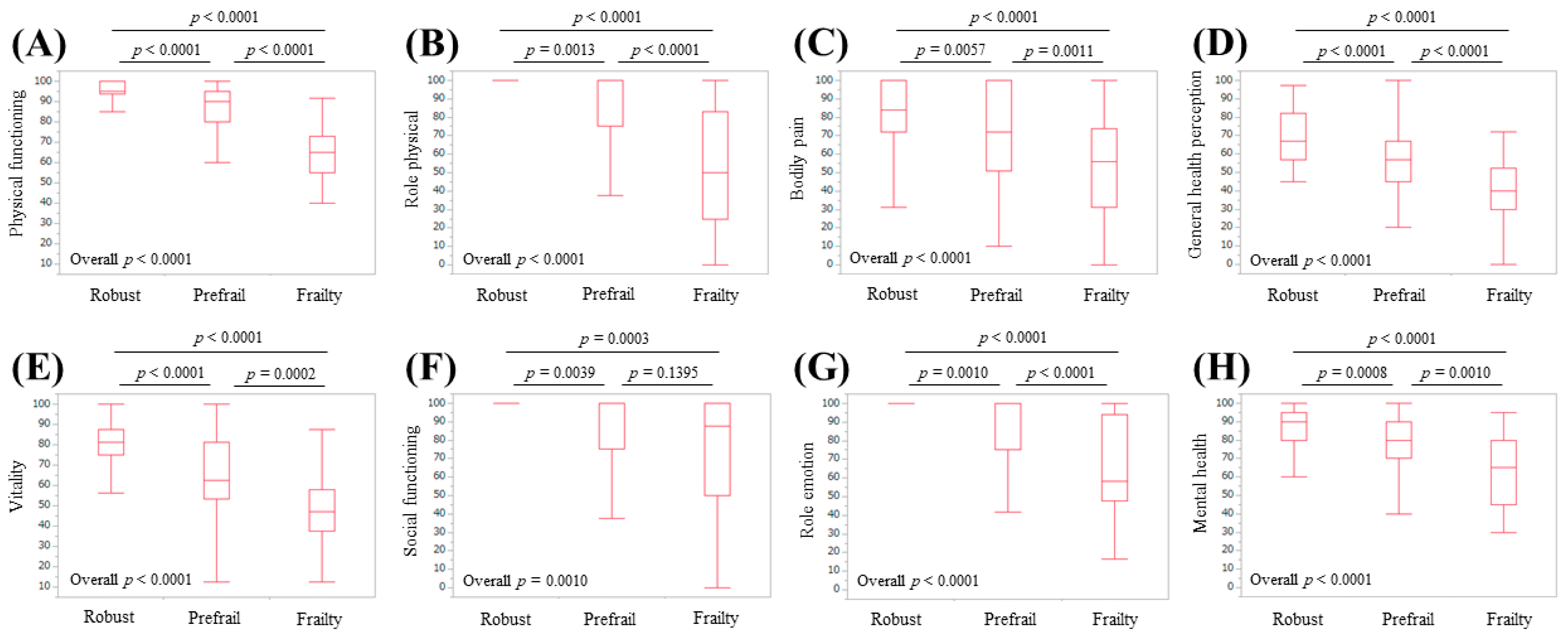
3.4. Subgroup Analysis 2: Scores of the Eight Scales of the SF-36 Relative to the Frailty Status in Non-LC Patients
3.5. Subgroup Analysis 3: Scores of the Eight Scales of the SF-36 Relative to the Frailty Status in Male Patients
3.6. Subgroup Analysis 4: Scores of the Eight Scales of the SF-36 Relative to the Frailty Status in Female Patients
3.7. Univariate and Multivariate Analysis of Factors Linked to Frailty
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviation
| Hr-QOL | health-related quality of life |
| CLDs | chronic liver diseases |
| SF-36 | 36-item Short-Form Health Survey |
| LC | liver cirrhosis |
| BW | body weight |
| GS | grip strength |
| WS | walking speed |
| CHS | Cardiovascular Health Study |
| PCS | physical component summary score |
| MCS | mental component summary score |
| IQR | interquartile range |
| ALBI | albumin-bilirubin |
References
- Lloyd, A.; Sawyer, W.; Hopkinson, P. Impact of long-term complications on quality of life in patients with type 2 diabetes not using insulin. Value Health 2001, 4, 392–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambroski, C.H.; Moser, D.K.; Bhat, G.; Ziegler, C. Impact of symptom prevalence and symptom burden on quality of life in patients with heart failure. Eur. J. Cardiovasc. Nurs. 2005, 4, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Rebollo, P.; Ortega, F.; Baltar, J.M.; Díaz-Corte, C.; Navascués, R.A.; Naves, M.; Ureña, A.; Badía, X.; Alvarez-Ude, F.; Alvarez-Grande, J. Health-related quality of life (HRQOL) in end stage renal disease (ESRD) patients over 65 years. Geriatr. Nephrol. Urol. 1998, 8, 85–94. [Google Scholar] [CrossRef]
- Bottomley, A.; Pe, M.; Sloan, J.; Basch, E.; Bonnetain, F.; Calvert, M.; Campbell, A.; Cleeland, C.; Cocks, K.; Collette, L.; et al. Setting International Standards in Analyzing Patient-Reported Outcomes and Quality of Life Endpoints Data (SISAQOL) consortium. Analysing data from patient-reported outcome and quality of life endpoints for cancer clinical trials: A start in setting international standards. Lancet Oncol. 2016, 17, e510–e514. [Google Scholar] [PubMed]
- Gao, F.; Gao, R.; Li, G.; Shang, Z.M.; Hao, J.Y. Health-related quality of life and survival in Chinese patients with chronic liver disease. Health Qual. Life Outcomes 2013, 11, 131. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Yeo, W. Value of quality of life analysis in liver cancer: A clinician’s perspective. World J. Hepatol. 2017, 9, 867–883. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, B.M.; Younossi, Z.M.; Hays, R.D.; Revicki, D.; Robbins, S.; Kanwal, F. Impact of hepatitis C on health-related quality of life: A systematic review and quantitative assessment. Hepatology 2005, 41, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Stepanova, M.; Younossi, I.; Pan, C.Q.; Janssen, H.L.A.; Papatheodoridis, G.; Nader, F. Long-term Effects of Treatment for Chronic HBV Infection on Patient-Reported Outcomes. Clin. Gastroenterol. Hepatol. 2018, 17, 1641–1642. [Google Scholar] [CrossRef] [PubMed]
- Schramm, C.; Wahl, I.; Weiler-Normann, C.; Voigt, K.; Wiegard, C.; Glaubke, C.; Brähler, E.; Löwe, B.; Lohse, A.W.; Rose, M. Health-related quality of life, depression, and anxiety in patients with autoimmune hepatitis. J. Hepatol. 2014, 60, 618–624. [Google Scholar] [CrossRef]
- Dyson, J.K.; Wilkinson, N.; Jopson, L.; Mells, G.; Bathgate, A.; Heneghan, M.A.; Neuberger, J.; Hirschfield, G.M.; Ducker, S.J.; UK-PBC Consortium; et al. The inter-relationship of symptom severity and quality of life in 2055 patients with primary biliary cholangitis. Aliment. Pharmacol. Ther. 2016, 44, 1039–1050. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M. Patient-reported Outcomes and the Economic Effects of Non-Alcoholic Fatty Liver Disease and Non-alcoholic Steatohepatitis-The Value Proposition. Hepatology 2018, 68, 2405–2412. [Google Scholar] [CrossRef] [Green Version]
- Tapper, E.B.; Baki, J.; Parikh, N.D.; Lok, A.S. Frailty, Psychoactive Medications, and Cognitive Dysfunction Are Associated With Poor Patient-Reported Outcomes in Cirrhosis. Hepatology 2019, 69, 1676–1685. [Google Scholar] [CrossRef] [PubMed]
- Kok, B.; Whitlock, R.; Ferguson, T.; Bailey, R.J.; Burak, K.W.; Kowalczewski, J.; Tangri, N.; Tandon, P. Health-Related Quality of Life: A Rapid Predictor of Hospitalization in Patients With Cirrhosis. Am. J. Gastroenterol. 2020, 115, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.R.; Berzigotti, A.; Lord, J.M.; Lai, J.C.; Armstrong, M.J. Impact of exercise on physical frailty in patients with chronic liver disease. Aliment. Pharmacol. Ther. 2019, 50, 988–1000. [Google Scholar] [CrossRef] [PubMed]
- Bunchorntavakul, C.; Reddy, K.R. Malnutrition/sarcopenia and frailty in patients with cirrhosis. Aliment. Pharmacol. Ther. 2020, 51, 64–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aber, A.; Howard, A.; Woods, H.B.; Jones, G.; Michaels, J. Impact of Carotid Artery Stenosis on Quality of Life: A Systematic Review. Patient 2019, 12, 213–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikdashi, J. Measuring and monitoring health-related quality of life responsiveness in systemic lupus erythematosus patients: Current perspectives. Patient Relat. Outcome Meas. 2018, 9, 339–343. [Google Scholar] [CrossRef] [Green Version]
- Gerth, A.M.J.; Hatch, R.A.; Young, J.D.; Watkinson, P.J. Changes in health-related quality of life after discharge from an intensive care unit: A systematic review. Anaesthesia 2019, 74, 100–108. [Google Scholar] [CrossRef]
- Paracha, N.; Abdulla, A.; MacGilchrist, K.S. Systematic review of health state utility values in metastatic non-small cell lung cancer with a focus on previously treated patients. Health Qual. Life Outcomes 2018, 16, 179. [Google Scholar] [CrossRef] [Green Version]
- Behboodi Moghadam, Z.; Fereidooni, B.; Saffari, M.; Montazeri, A. Measures of health-related quality of life in PCOS women: A systematic review. Int. J. Womens Health 2018, 10, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, A.R.; Howlett, S.E.; Fernandes, A. Frailty-A promising concept to evaluate disease vulnerability. Mech. Ageing Dev. 2020, 187, 111217. [Google Scholar] [CrossRef] [PubMed]
- Satake, S.; Arai, H. Implications of frailty screening in clinical practice. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 4–10. [Google Scholar] [CrossRef]
- Sewo Sampaio, P.Y.; Sampaio, R.A.; Yamada, M.; Arai, H. Systematic review of the Kihon Checklist: Is it a reliable assessment of frailty? Geriatr. Gerontol. Int. 2016, 16, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.A.; Rogal, S.S.; Duarte-Rojo, A.; Lai, J.C. Physical Function, Physical Activity, and Quality of Life after Liver Transplantation. Liver Transpl. 2020, 26, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Dodge, J.L.; Kappus, M.R.; Dunn, M.A.; Volk, M.L.; Duarte-Rojo, A.; Ganger, D.R.; Rahimi, R.S.; McCulloch, C.E.; Haugen, C.E.; et al. Changes in frailty are associated with waitlist mortality in patients with cirrhosis. J. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Dodge, J.L.; McCulloch, C.E.; Covinsky, K.E.; Singer, J.P. Frailty and the Burden of Concurrent and Incident Disability in Patients with Cirrhosis: A Prospective Cohort Study. Hepatol. Commun. 2019, 4, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between frailty and quality of life among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef]
- Derck, J.E.; Thelen, A.E.; Cron, D.C.; Friedman, J.F.; Gerebics, A.D.; Englesbe, M.J.; Sonnenday, C.J. In ESLD patient referred for liver transplant, diminished QoL appears to be significantly negatively associated with frailty and not with severity of liver disease as measured MELD. Transplantation 2015, 99, 340–344. [Google Scholar] [CrossRef] [Green Version]
- Nixon, A.C.; Bampouras, T.M.; Pendleton, N.; Mitra, S.; Brady, M.E.; Dhaygude, A.P. Frailty is independently associated with worse health-related quality of life in chronic kidney disease: A secondary analysis of the Frailty Assessment in Chronic Kidney Disease study. Clin. Kidney J. 2019, 13, 85–94. [Google Scholar] [CrossRef]
- Satake, S.; Arai, H. Chapter 1 Frailty: Definition, diagnosis, epidemiology. Geriatr. Gerontol. Int. 2020, 20 (Suppl. 1), 7–13. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- Mchorney, C.A.; Ware, J.E.; Raczek, A.E. The MOS 36-item Short-Form Health Survey (SF-36): Ⅱ. Psychometric and Clinical Tests of Validity in Measuring Physical and Mental Health Constructs. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mchorney, C.A.; Ware, J.E.; Raczek, A.E. The MOS 36-item Short-Form Health Survey (SF-36): Ⅲ. Tests of Data Quality, scaling Assumptions, and Reliability across Diverse Patient Groups. Med. Care 1994, 32, 40–66. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, S.; Bito, S.; Green, J.; Hsiao, A.; Kurokawa, K. Translation, adaptation, and validation of the SF-36 Health Survey for use in Japan. J. Clin. Epidemiol. 1998, 51, 1037–1044. [Google Scholar] [CrossRef]
- Fukuhara, S.; Ware, J.E.; Kosinski, M.; Wada, S.; Gandek, B. Psychometric and clinical tests of validity of the Japanese SF-36 Health Survey. J. Clin. Epidemiol. 1998, 51, 1045–1053. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Bunt, S.; Steverink, N.; Olthof, J.; van der Schans, C.P.; Hobbelen, J.S.M. Social frailty in older adults: A scoping review. Eur. J. Ageing 2017, 14, 323–334. [Google Scholar] [CrossRef]
- Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; Takata, R.; et al. Health-Related Quality of Life in Chronic Liver Diseases: A Strong Impact of Hand Grip Strength. J. Clin. Med. 2018, 7, 553. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, H.; Osaki, Y. Clinical significance of therapy using branched-chain amino acid granules in patients with liver cirrhosis and hepatocellular carcinoma. Hepatol. Res. 2014, 44, 149–158. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Cases (n = 341) |
|---|---|
| Age (years) | 66 (55, 72) |
| Gender, male/female | 164/177 |
| Liver disease etiology HCV-related/HBV-related/HBV- and HCV-related/NBNC-related | 174/61/7/99 |
| Presence of frailty, yes/no | 46/295 |
| Presence of LC, yes/no | 122/219 |
| Body mass index (kg/m2) | 22.7 (20.5, 25.65) |
| Walking speed (m/s) | 1.303 (1.1005, 1.4445) |
| Grip strength (kg), male | 33.3 (27.925, 38.925) |
| Grip strength (kg), female | 20.8 (17.6, 24.45) |
| Total bilirubin (mg/dL) | 0.8 (0.6, 1.1) |
| Serum albumin (g/dL) | 4.3 (4.0, 4.5) |
| ALBI score | −2.9 (−3.12, −2.6) |
| ALBI grade, 1/2/3 | 256/78/7 |
| Prothrombin time (%) | 91.2 (80.55, 99.05) |
| Platelet count (×104/mm3) | 17.5 (12.6, 22.0) |
| AST (IU/L) | 25 (19, 34) |
| ALT (IU/L) | 19 (14, 33) |
| Total cholesterol (mg/dL) | 181 (151.25, 213) |
| HbA1c (NGSP) | 5.7 (5.4, 6.1) |
| Scales of SF-36 | |
| Physical functioning | 90 (80, 95) |
| Role physical | 100 (75, 100) |
| Bodily pain | 74 (52, 100) |
| General health perception | 55 (45, 71) |
| Vitality | 68.8 (56.2, 81.3) |
| Social functioning | 100 (75, 100) |
| Role emotion | 100 (75, 100) |
| Mental health | 80 (65, 90) |
| Physical component summary score | 51.1 (41.2, 54.3) |
| Mental component summary score | 53.6 (46.0, 59.2) |
| Variables | Univariate Analysis p-Value | Multivariate Analysis | ||
|---|---|---|---|---|
| Estimates | SE | p-Value | ||
| Age (years) | 0.0002 | −0.0499 | 0.020 | 0.0126 |
| Gender | 0.5292 | |||
| Presence of LC | <0.0001 | −0.484 | 0.265 | 0.0685 |
| Body mass index | 0.3701 | |||
| Total bilirubin | 0.9042 | |||
| Serum albumin | <0.0001 | 0.259 | 0.413 | 0.5308 |
| Prothrombin time | 0.2037 | |||
| Platelet count | 0.0543 | |||
| AST | 0.0992 | |||
| ALT | 0.6717 | |||
| Total cholesterol | 0.0815 | |||
| HbA1c (NGSP) | 0.1741 | |||
| Physical functioning | <0.0001 | 0.0434 | 0.0125 | 0.0005 |
| Role physical | <0.0001 | 0.00769 | 0.0102 | 0.4531 |
| Bodily pain | <0.0001 | −0.000804 | 0.0095 | 0.9327 |
| General health perception | <0.0001 | 0.00357 | 0.0139 | 0.7976 |
| Vitality | <0.0001 | 0.0349 | 0.0155 | 0.0246 |
| Social functioning | <0.0001 | −0.0169 | 0.0117 | 0.1481 |
| Role emotion | <0.0001 | 0.0158 | 0.0106 | 0.1384 |
| Mental health | <0.0001 | −0.00394 | 0.0146 | 0.7877 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, H.; Yoh, K.; Enomoto, H.; Iwata, Y.; Sakai, Y.; Kishino, K.; Shimono, Y.; Ikeda, N.; Takashima, T.; Aizawa, N.; et al. Health-Related Quality of Life and Frailty in Chronic Liver Diseases. Life 2020, 10, 76. https://doi.org/10.3390/life10050076
Nishikawa H, Yoh K, Enomoto H, Iwata Y, Sakai Y, Kishino K, Shimono Y, Ikeda N, Takashima T, Aizawa N, et al. Health-Related Quality of Life and Frailty in Chronic Liver Diseases. Life. 2020; 10(5):76. https://doi.org/10.3390/life10050076
Chicago/Turabian StyleNishikawa, Hiroki, Kazunori Yoh, Hirayuki Enomoto, Yoshinori Iwata, Yoshiyuki Sakai, Kyohei Kishino, Yoshihiro Shimono, Naoto Ikeda, Tomoyuki Takashima, Nobuhiro Aizawa, and et al. 2020. "Health-Related Quality of Life and Frailty in Chronic Liver Diseases" Life 10, no. 5: 76. https://doi.org/10.3390/life10050076