Numerical Investigation on the Role of Mechanical Factors Contributing to Globe Flattening in States of Elevated Intracranial Pressure


Abstract
:1. Introduction
2. Materials and Methods
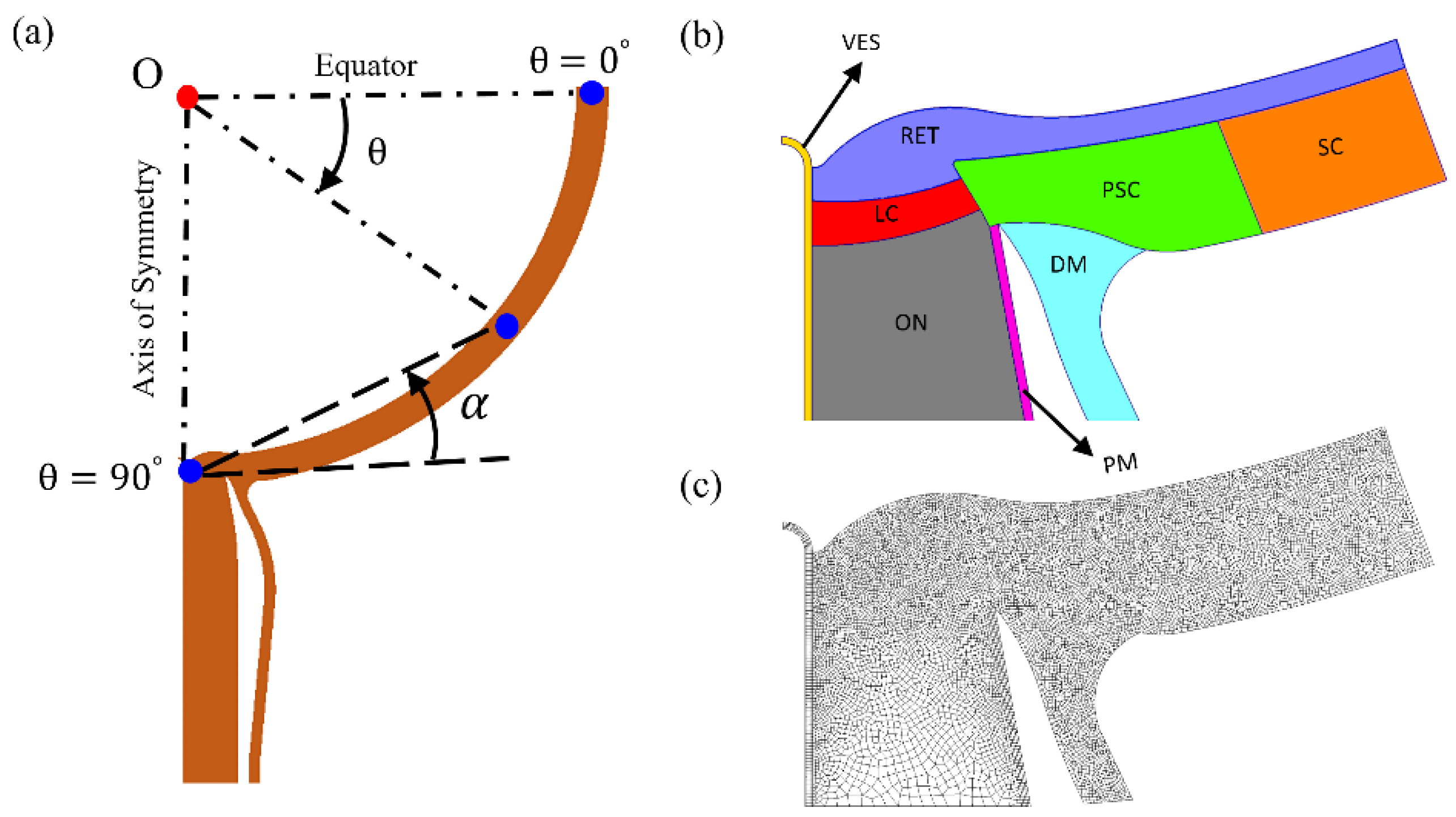
2.1. Model
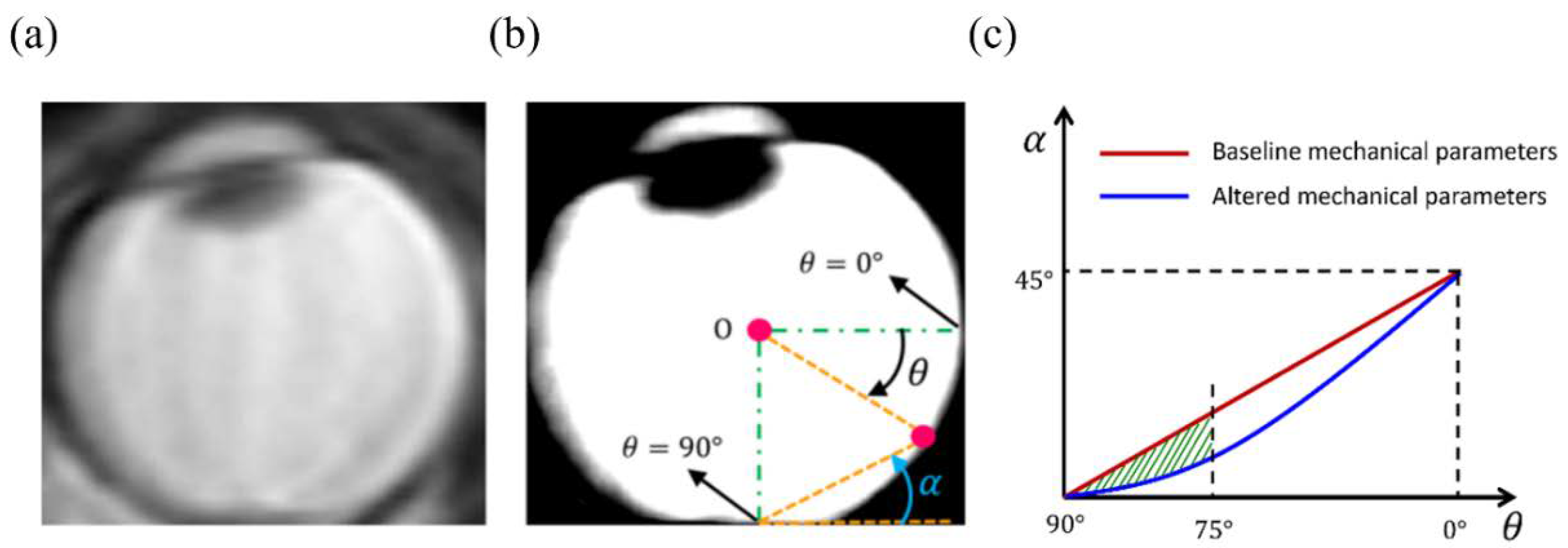
2.2. Assessment of Globe Flattening and Model Comparison
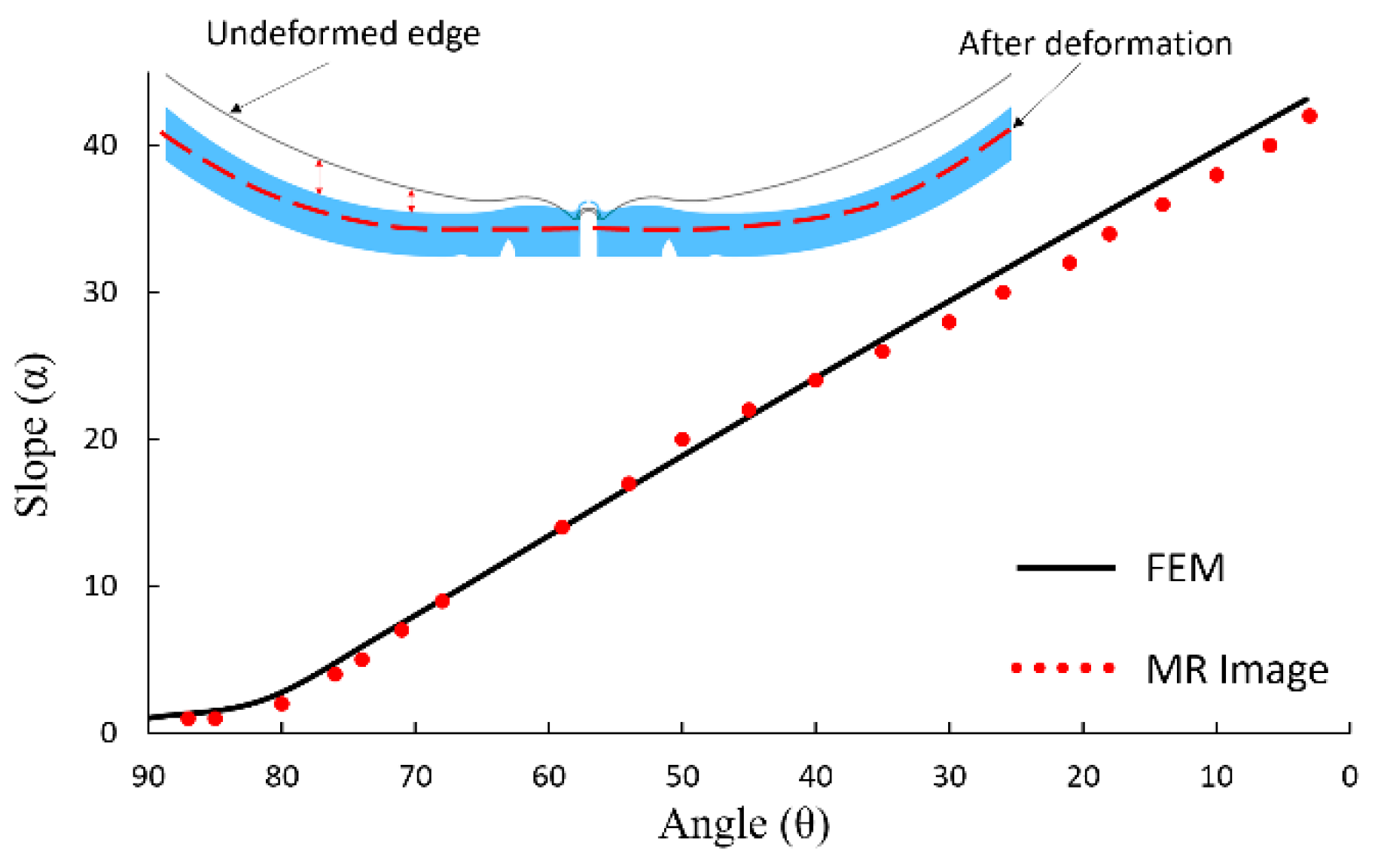
2.3. Tuning of Models to Human Images
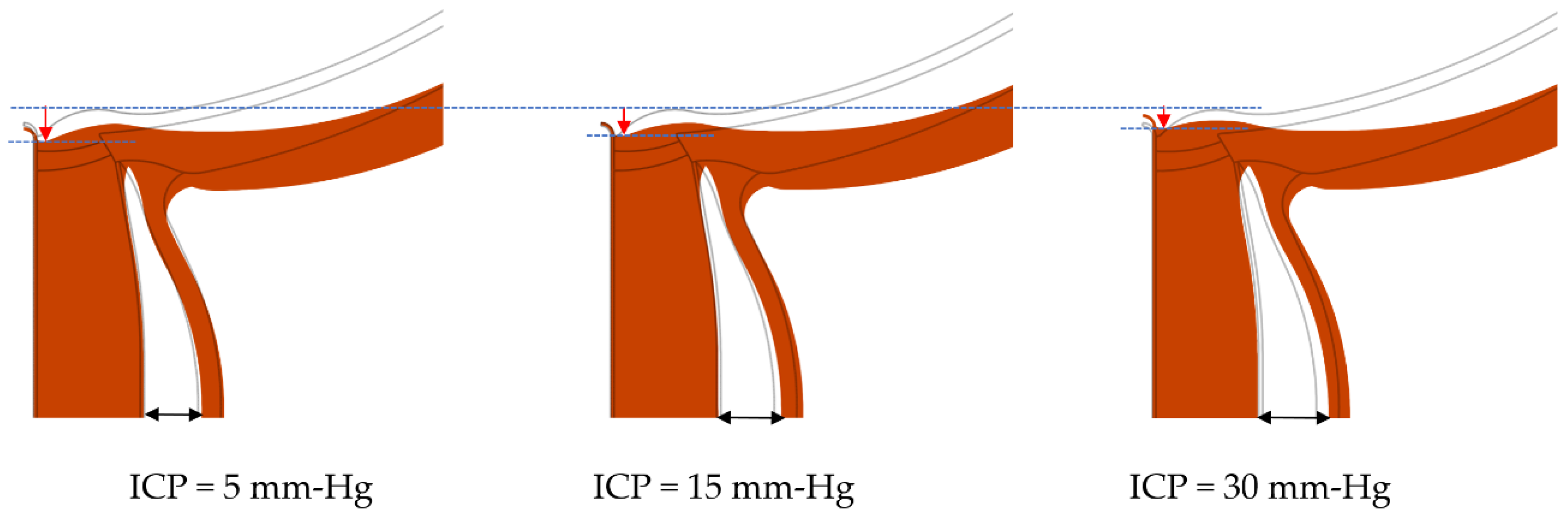
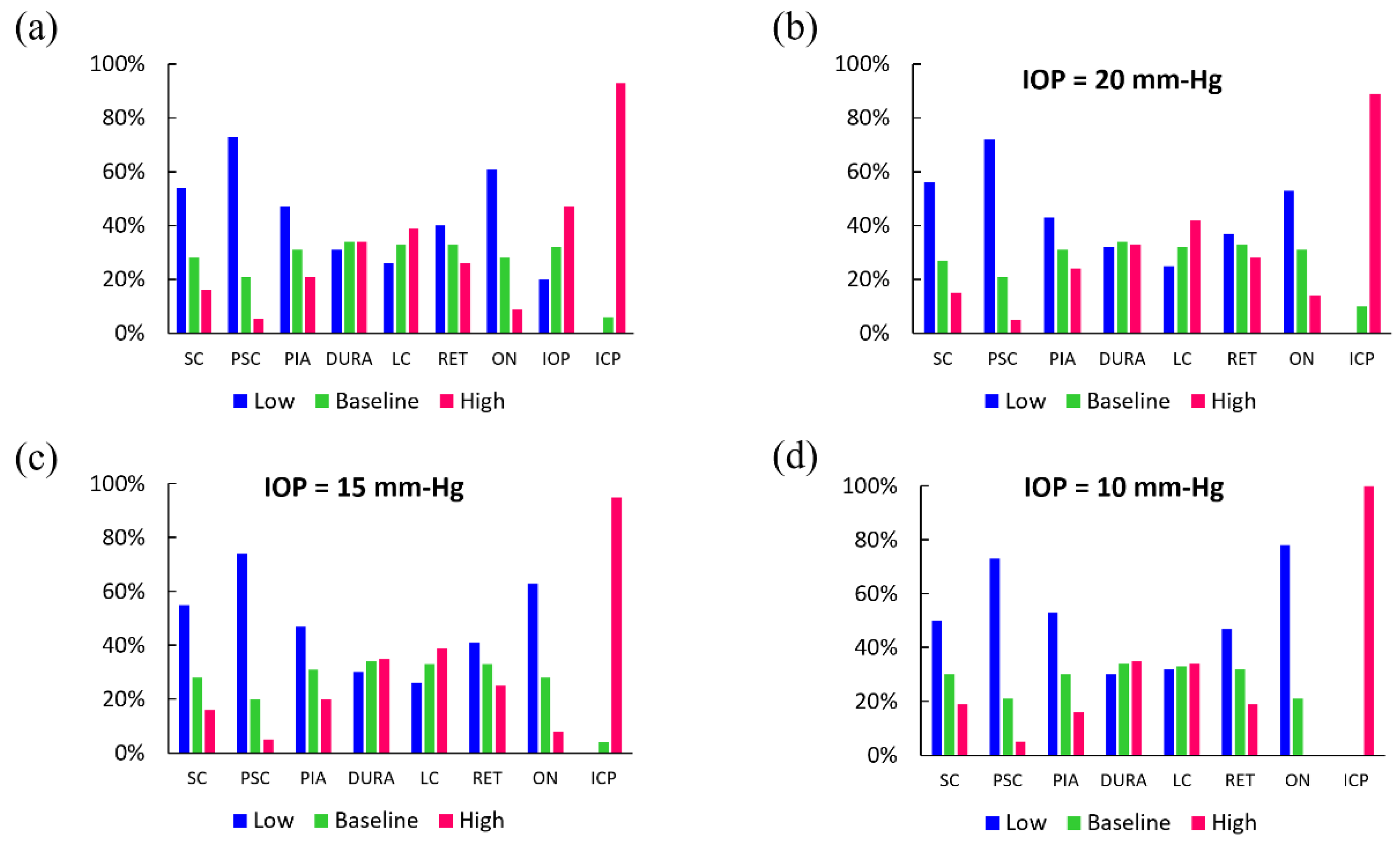
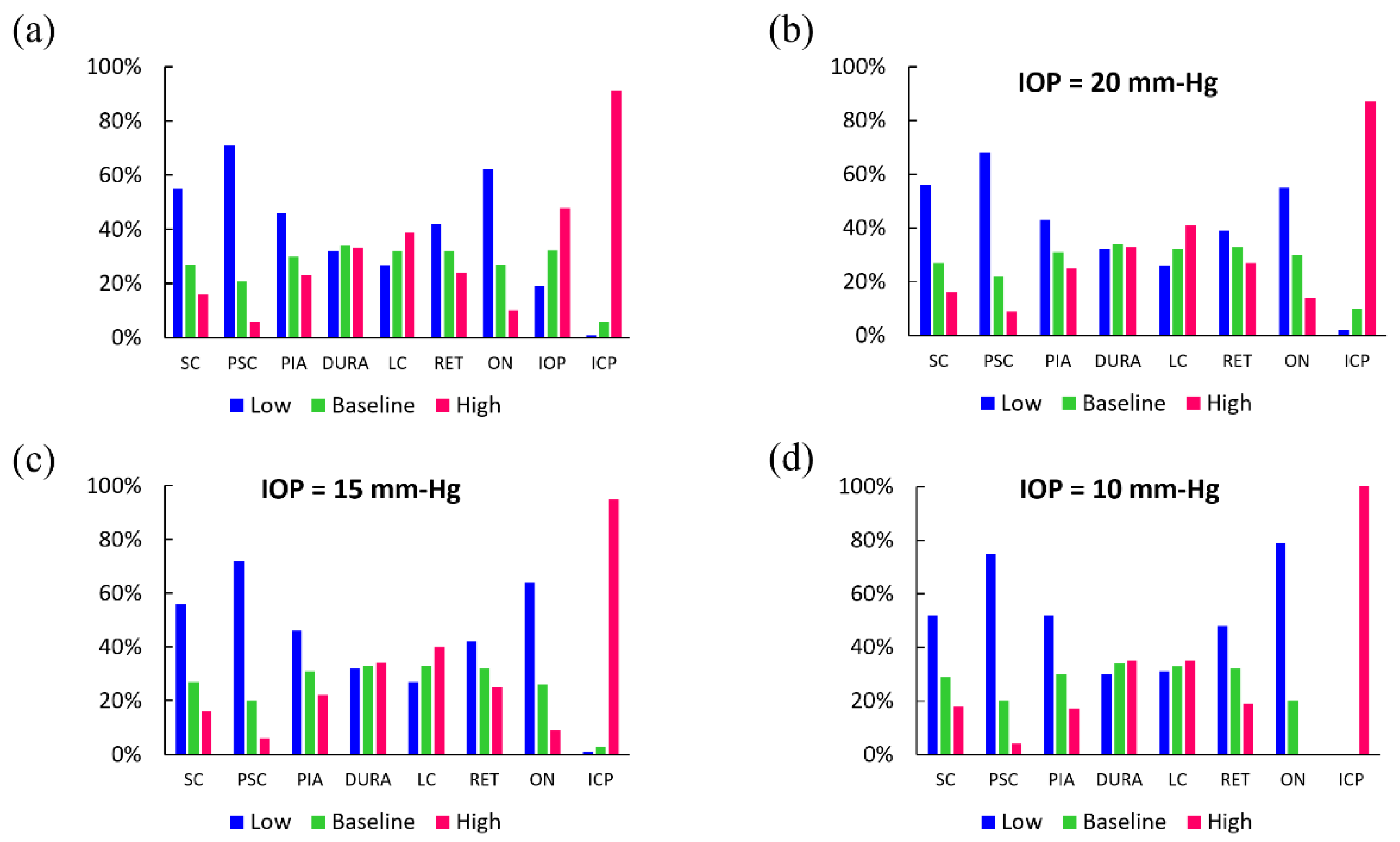
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dandy, W.E. Intracranial pressure without brain tumor: Diagnosis and treatment. Ann. Surg. 1937, 106, 492. [Google Scholar] [CrossRef] [PubMed]
- Skau, M.; Brennum, J.; Gjerris, F.; Jensen, R. What is new about idiopathic intracranial hypertension? An updated review of mechanism and treatment. Cephalalgia 2006, 26, 384–399. [Google Scholar] [CrossRef] [PubMed]
- Wall, M. Idiopathic intracranial hypertension. Neurol. Clin. 2010, 28, 593–617. [Google Scholar] [CrossRef] [PubMed]
- Alperin, N.; Bagci, A.; Lam, B.; Sklar, E. Automated quantitation of the posterior scleral flattening and optic nerve protrusion by MRI in idiopathic intracranial hypertension. Am. J. Neuroradiol. 2013, 34, 2354–2359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holbrook, J.; Saindane, A.M. Imaging of intracranial pressure disorders. Neurosurgery 2017, 80, 341–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, L.A.; Sargsyan, A.E.; Hasan, K.M.; Polk, J.D.; Hamilton, D.R. Orbital and intracranial effects of microgravity: Findings at 3-T MR imaging. Radiology 2012, 263, 819–827. [Google Scholar] [CrossRef]
- Wang, L.-J.; Chen, L.-M.; Chen, Y.; Bao, L.-Y.; Zheng, N.-N.; Wang, Y.-Z.; Xing, Y.-Q. Ultrasonography assessments of optic nerve sheath diameter as a noninvasive and dynamic method of detecting changes in intracranial pressure. JAMA Ophthalmol. 2018, 136, 250–256. [Google Scholar] [CrossRef]
- Ossoinig, K.; Cennamo, G.; Frazier-Byrne, S. Echographic differential diagnosis of optic-nerve lesions. In Ultrasonography in Ophthalmology, Documenta Ophthalmologica Proceedings Series; Thijssen, J.M., Verbeek, A.M., Eds.; Springer: Berlin/Heidelberg, Germany, 1981; pp. 327–332. [Google Scholar]
- Rosa, N.; Giamundo, A.; Jura, A.; Iaccarino, G.; Romano, A. Mesalazine-associated benign intracranial hypertension in a patient with ulcerative colitis. Am. J. Ophthalmol. 2003, 136, 212–213. [Google Scholar] [CrossRef]
- Aduayi, O.S.; Asaleye, C.M.; Adetiloye, V.A.; Komolafe, E.O.; Aduayi, V.A. Optic nerve sonography: A noninvasive means of detecting raised intracranial pressure in a resource-limited setting. J. Neurosci. Rural Pract. 2015, 6, 563–567. [Google Scholar] [CrossRef]
- Kitano, T.; Nezu, T.; Mukai, T.; Uemura, J.; Wada, Y.; Yagita, Y. A Case of Hypertensive Encephalopathy with Enlarged Optic Nerve Sheath Measured by Transorbital Sonography. J. Stroke Cereb. Dis. 2017, 26, e20–e21. [Google Scholar] [CrossRef]
- De Bernardo, M.; Rosa, N. Transorbital sonography to evaluate optic nerve in hypertensive encephalopathy. J. Stroke Cereb. Dis. 2018, 27, 1124. [Google Scholar] [CrossRef] [PubMed]
- Rosa, N.; De Bernardo, M. Measurement of the optic nerve in a resource-limited setting. J. Neurosci. Rural Pract. 2017, 8, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Passi, N.; Degnan, A.J.; Levy, L.M. MR imaging of papilledema and visual pathways: Effects of increased intracranial pressure and pathophysiologic mechanisms. Am. J. Neuroradiol. 2013, 34, 919–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trobe, J.D. Papilledema: The vexing issues. J. Neur-Ophthalmol. 2011, 31, 175–186. [Google Scholar] [CrossRef] [Green Version]
- Hua, Y.; Tong, J.; Ghate, D.; Kedar, S.; Gu, L. Intracranial pressure influences the behavior of the optic nerve head. J. Biomech. Eng. 2017, 139, 031003. [Google Scholar] [CrossRef]
- Hua, Y.; Voorhees, A.P.; Sigal, I.A. Cerebrospinal Fluid Pressure: Revisiting Factors Influencing Optic Nerve Head Biomechanics. Investig. Ophthalmol. Vis. Sci. 2018, 59, 154–165. [Google Scholar] [CrossRef] [Green Version]
- Sigal, I.A.; Bilonick, R.A.; Kagemann, L.; Wollstein, G.; Ishikawa, H.; Schuman, J.S.; Grimm, J.L. The optic nerve head as a robust biomechanical system. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2658–2667. [Google Scholar] [CrossRef]
- Sigal, I.A.; Ethier, C.R. Biomechanics of the optic nerve head. Exp. Eye Res. 2009, 88, 799–807. [Google Scholar] [CrossRef]
- Sigal, I.A.; Flanagan, J.G.; Ethier, C.R. Factors influencing optic nerve head biomechanics. Investig. Ophthalmol. Vis. Sci. 2005, 46, 4189–4199. [Google Scholar] [CrossRef]
- Sigal, I.A.; Flanagan, J.G.; Tertinegg, I.; Ethier, C.R. Finite element modeling of optic nerve head biomechanics. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4378–4387. [Google Scholar] [CrossRef]
- Sigal, I.A.; Flanagan, J.G.; Tertinegg, I.; Ethier, C.R. 3D morphometry of the human optic nerve head. Exp. Eye Res. 2010, 90, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Feola, A.J.; Myers, J.G.; Raykin, J.; Mulugeta, L.; Nelson, E.S.; Samuels, B.C.; Ethier, C.R. Finite element modeling of factors influencing optic nerve head deformation due to intracranial pressure. Investig. Ophthalmol. Vis. Sci. 2016, 57, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Geuzaine, C.; Remacle, J.F. Gmsh: A 3-D finite element mesh generator with built-in pre-and post-processing facilities. Int. J. Numer. Methods Eng. 2009, 79, 1309–1331. [Google Scholar] [CrossRef]
- Alnæs, M.; Blechta, J.; Hake, J.; Johansson, A.; Kehlet, B.; Logg, A.; Richardson, C.; Ring, J.; Rognes, M.E.; Wells, G.N. The FEniCS project version 1.5. Arch. Numer. Softw. 2015, 3. [Google Scholar] [CrossRef]
- Logg, A.; Mardal, K.-A.; Wells, G. Automated Solution of Differential Equations by the Finite Element Method: The FEniCS Book; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012; Volume 84. [Google Scholar]
- Girard, M.J.; Downs, J.C.; Burgoyne, C.F.; Suh, J.-K.F. Peripapillary and posterior scleral mechanics—part I: Development of an anisotropic hyperelastic constitutive model. J. Biomech. Eng. 2009, 131. [Google Scholar] [CrossRef]
- Schwaner, S.A.; Kight, A.M.; Perry, R.N.; Pazos, M.; Yang, H.; Johnson, E.C.; Morrison, J.C.; Burgoyne, C.F.; Ethier, C.R. A methodology for individual-specific modeling of rat optic nerve head biomechanics in glaucoma. J. Biomech. Eng. 2018, 140. [Google Scholar] [CrossRef]
- Hoffmann, J.; Schmidt, C.; Kunte, H.; Klingebiel, R.; Harms, L.; Huppertz, H.-J.; Lüdemann, L.; Wiener, E. Volumetric assessment of optic nerve sheath and hypophysis in idiopathic intracranial hypertension. Am. J. Neuroradiol. 2014, 35, 513–518. [Google Scholar] [CrossRef] [Green Version]
- Killer, H.; Jaggi, G.; Flammer, J.; Miller, N.R.; Huber, A.; Mironov, A. Cerebrospinal fluid dynamics between the intracranial and the subarachnoid space of the optic nerve. Is it always bidirectional? Brain 2007, 130, 514–520. [Google Scholar] [CrossRef]
- Hansen, H.-C.; Helmke, K. Validation of the optic nerve sheath response to changing cerebrospinal fluid pressure: Ultrasound findings during intrathecal infusion tests. J. Neurosurg. 1997, 87, 34–40. [Google Scholar] [CrossRef]
- Mader, T.H.; Gibson, C.R.; Pass, A.F.; Kramer, L.A.; Lee, A.G.; Fogarty, J.; Tarver, W.J.; Dervay, J.P.; Hamilton, D.R.; Sargsyan, A. Optic disc edema, globe flattening, choroidal folds, and hyperopic shifts observed in astronauts after long-duration space flight. Ophthalmology 2011, 118, 2058–2069. [Google Scholar] [CrossRef] [Green Version]
- Shinojima, A.; Kakeya, I.; Tada, S. Association of space flight with Problems of the brain and eyes. JAMA Ophthalmol. 2018, 136, 1075–1076. [Google Scholar] [CrossRef] [PubMed]
- Wall, M.; GEORGE, D. Idiopathic intracranial hypertension: A prospective study of 50 patients. Brain 1991, 114, 155–180. [Google Scholar] [PubMed]
- Moss, H.E.; Park, J.C.; McAnany, J.J. The photopic negative response in idiopathic intracranial hypertension. Investig. Ophthalmol. Vis. Sci. 2015, 56, 3709–3714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, H.; Mehr, J.A.; Hatami-Marbini, H. Effect of posterior optic nerve and sheath boundary conditions on globe deformation in high intracranial pressure (ICP) states. Investig. Ophthalmol. Vis. Sci. 2019, 60, 5228. [Google Scholar]
- Nguyen, B.A.; Roberts, C.J.; Reilly, M.A. Biomechanical impact of the sclera on corneal deformation response to an air-puff: A finite-element study. Front. Bioeng. Biotechnol. 2019, 6, 210. [Google Scholar] [CrossRef]
- Girard, M.J.; Suh, J.-K.F.; Bottlang, M.; Burgoyne, C.F.; Downs, J.C. Scleral biomechanics in the aging monkey eye. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5226–5237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jan, N.-J.; Gomez, C.; Moed, S.; Voorhees, A.P.; Schuman, J.S.; Bilonick, R.A.; Sigal, I.A. Microstructural crimp of the lamina cribrosa and peripapillary sclera collagen fibers. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3378–3388. [Google Scholar]
- Jan, N.-J.; Lathrop, K.; Sigal, I.A. Collagen architecture of the posterior pole: High-resolution wide field of view visualization and analysis using polarized light microscopy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 735–744. [Google Scholar] [CrossRef]
- Wang, S.; Hatami-Marbini, H. Constitutive Modelling of Cornea Tissue; Influence of Three-Dimensional Collagen Fiber Microstructure. J. Biomech. Eng. 2020. [Google Scholar] [CrossRef]
- Feola, A.J.; Nelson, E.S.; Myers, J.; Ethier, C.R.; Samuels, B.C. The impact of choroidal swelling on optic nerve head deformation. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4172–4181. [Google Scholar] [CrossRef]
- Hatami-Marbini, H.; Maulik, R. A biphasic transversely isotropic poroviscoelastic model for the unconfined compression of hydrated soft tissue. J. Biomech. Eng. 2016, 138. [Google Scholar] [CrossRef] [PubMed]
- Moss, H.E.; Treadwell, G.; Wanek, J.; DeLeon, S.; Shahidi, M. Retinal vessel diameter assessment in papilledema by semi-automated analysis of SLO images: Feasibility and reliability. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2049–2054. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Abbreviation | Unit | Value | ||
|---|---|---|---|---|---|
| Low | Baseline | High | |||
| Pressure | |||||
| Intraocular pressure | IOP | mm-Hg | 10 | 15 | 20 |
| Intracranial pressure | ICP | mm-Hg | 5 | 15 | 30 |
| Young’s modulus (E) | |||||
| Sclera | SC | MPa | 0.6 | 1.2 | 1.8 |
| Peripapillary sclera | PSC | MPa | 0.6 | 1.2 | 1.8 |
| Pia mater | PM | MPa | 0.6 | 1.2 | 1.8 |
| Dura mater | DM | MPa | 0.6 | 1.2 | 1.8 |
| Lamina cribrosa | LC | MPa | 0.3 | 0.6 | 0.9 |
| Retina | RET | MPa | 0.03 | 0.06 | 0.09 |
| Optic nerve | ON | MPa | 0.03 | 0.06 | 0.09 |
| Retinal vessel | VES | MPa | 0.1 | ||
| Parameters | Abbreviation | Unit | Value | ||
|---|---|---|---|---|---|
| Low | Baseline | High | |||
| Pressure | |||||
| Intraocular pressure | IOP | mm-Hg | 10 | 15 | 20 |
| Intracranial pressure | ICP | mm-Hg | 5 | 15 | 30 |
| Nonlinear material constant (c1) | |||||
| Sclera | SC | MPa | 0.1 | 0.2 | 0.3 |
| Peripapillary Sclera | PSC | MPa | 0.1 | 0.2 | 0.3 |
| Pia Mater | PM | MPa | 0.1 | 0.2 | 0.3 |
| Dura Mater | DM | MPa | 0.1 | 0.2 | 0.3 |
| Young’s modulus (E) | |||||
| Lamina Cribrosa | LC | MPa | 0.3 | 0.6 | 0.9 |
| Optic Nerve | ON | MPa | 0.03 | 0.06 | 0.09 |
| Retina | RT | MPa | 0.03 | 0.06 | 0.09 |
| Vessel | VES | MPa | 0.1 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehr, J.A.; Moss, H.E.; Hatami-Marbini, H. Numerical Investigation on the Role of Mechanical Factors Contributing to Globe Flattening in States of Elevated Intracranial Pressure. Life 2020, 10, 316. https://doi.org/10.3390/life10120316
Mehr JA, Moss HE, Hatami-Marbini H. Numerical Investigation on the Role of Mechanical Factors Contributing to Globe Flattening in States of Elevated Intracranial Pressure. Life. 2020; 10(12):316. https://doi.org/10.3390/life10120316
Chicago/Turabian StyleMehr, Jafar A., Heather E. Moss, and Hamed Hatami-Marbini. 2020. "Numerical Investigation on the Role of Mechanical Factors Contributing to Globe Flattening in States of Elevated Intracranial Pressure" Life 10, no. 12: 316. https://doi.org/10.3390/life10120316