
Mechanism Design and Performance Analysis of a Wearable Hand Rehabilitation Robot
 ,
,
Abstract
:1. Introduction
2. Design Requirements
2.1. Metacarpophalangeal Joint Offset Analysis
2.2. Hand Rehabilitation Exoskeleton Design Requirements
3. Mechanical System
3.1. Mechanical Design
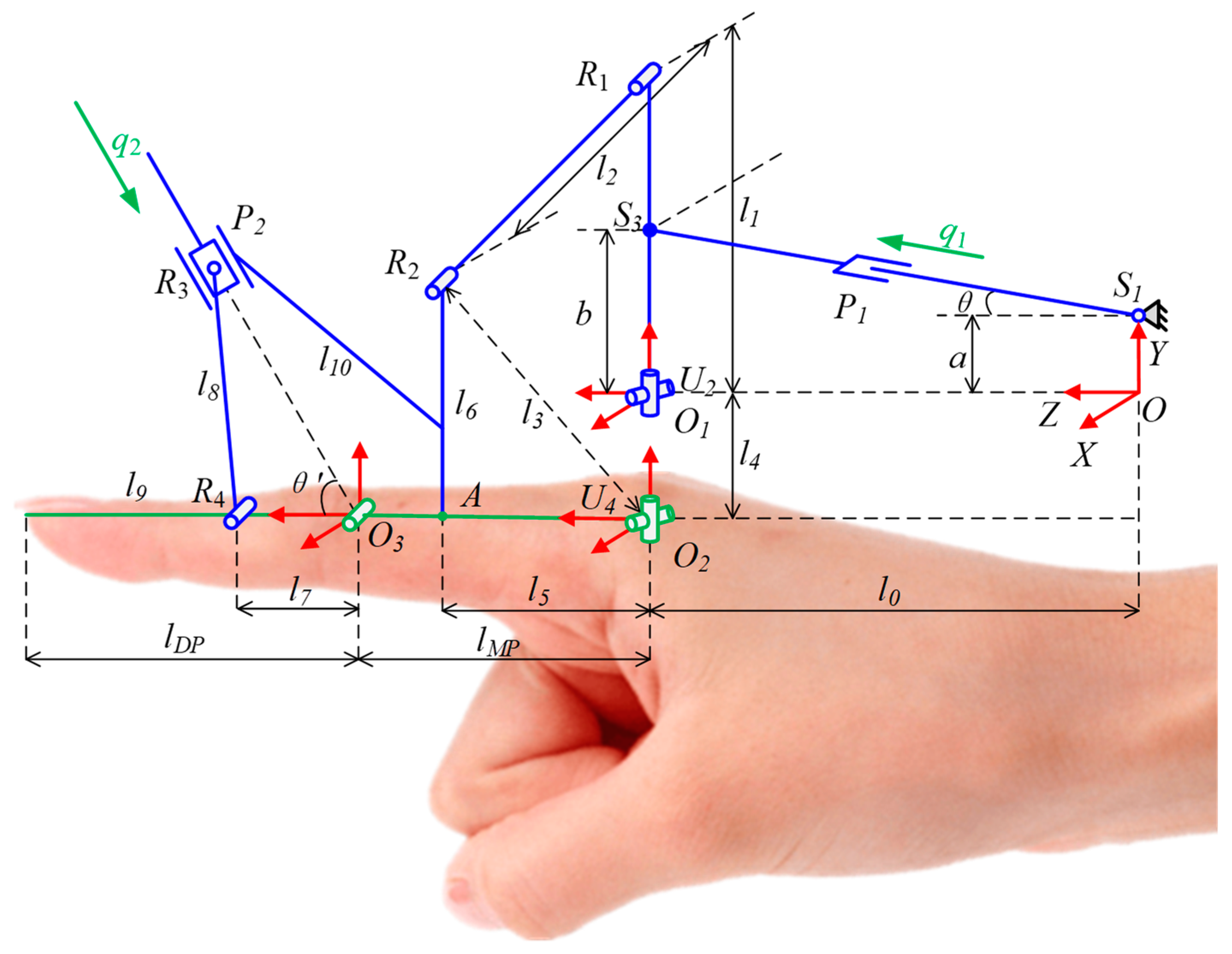
3.2. Robot Kinematics Analysis and Optimization
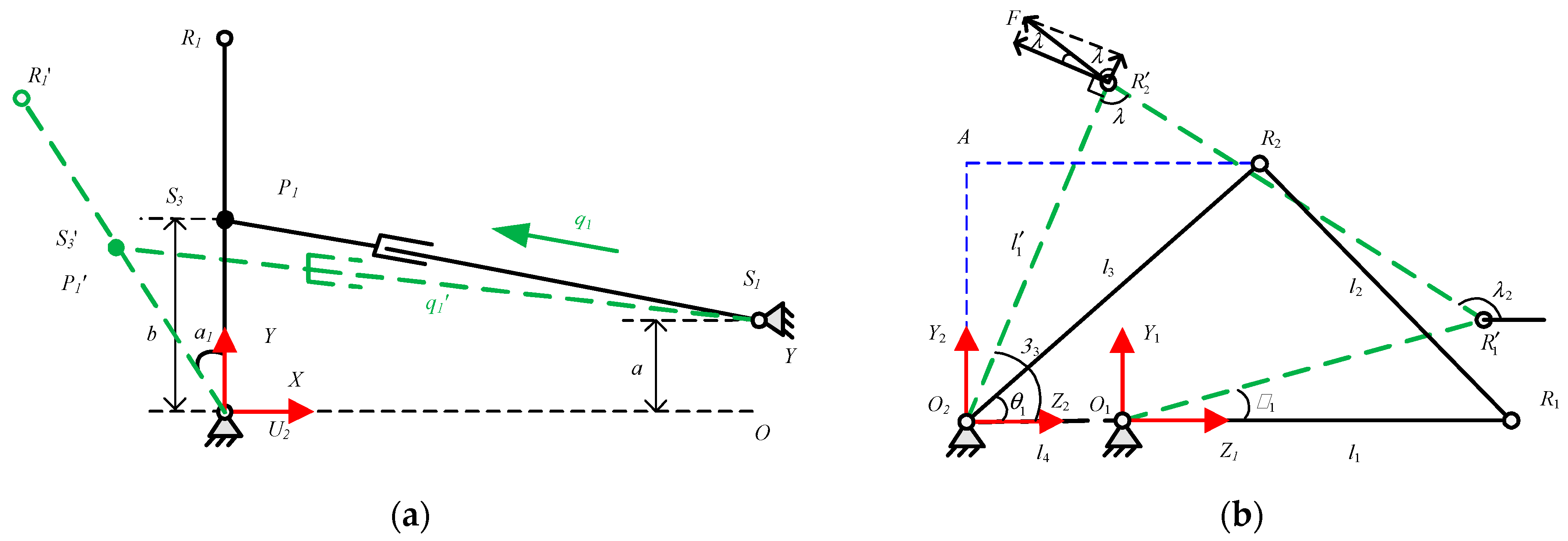
3.2.1. Kinematics
3.2.2. Rod Length Optimization Based on Genetic Algorithm
- Conditions for the establishment of the four-bar mechanism;
- 2.
- Angle magnification factor;
- 3.
- Transmission angle requirements.
4. Control and Sensing Systems
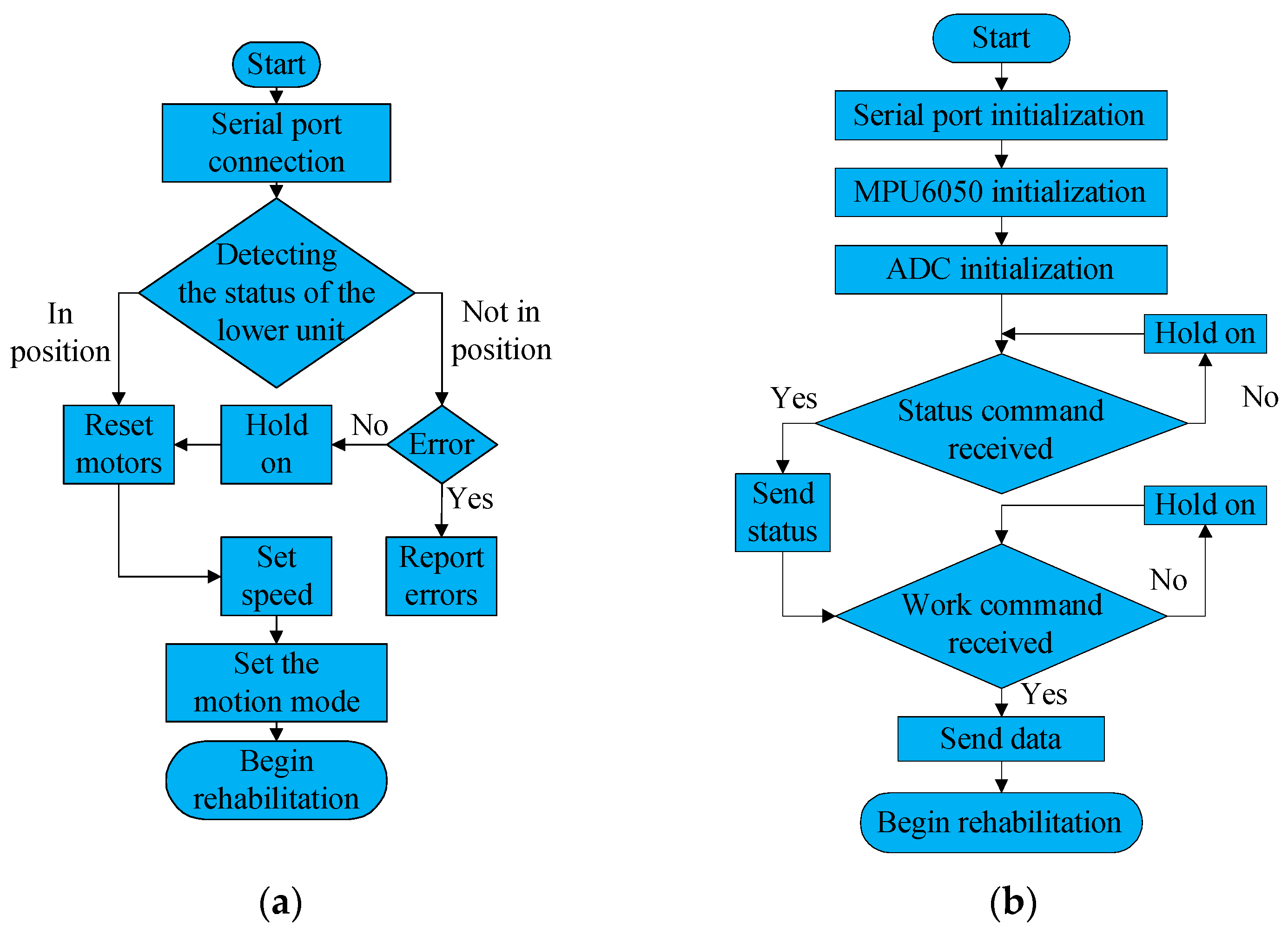
4.1. Software System
4.2. Sensing System
5. Preliminary Experimental Trial of the Robot
5.1. Experimental Platform Construction
5.2. Single Finger Experiment
5.2.1. Passive Rehabilitation Experiment
5.2.2. Active Rehabilitation Experiment
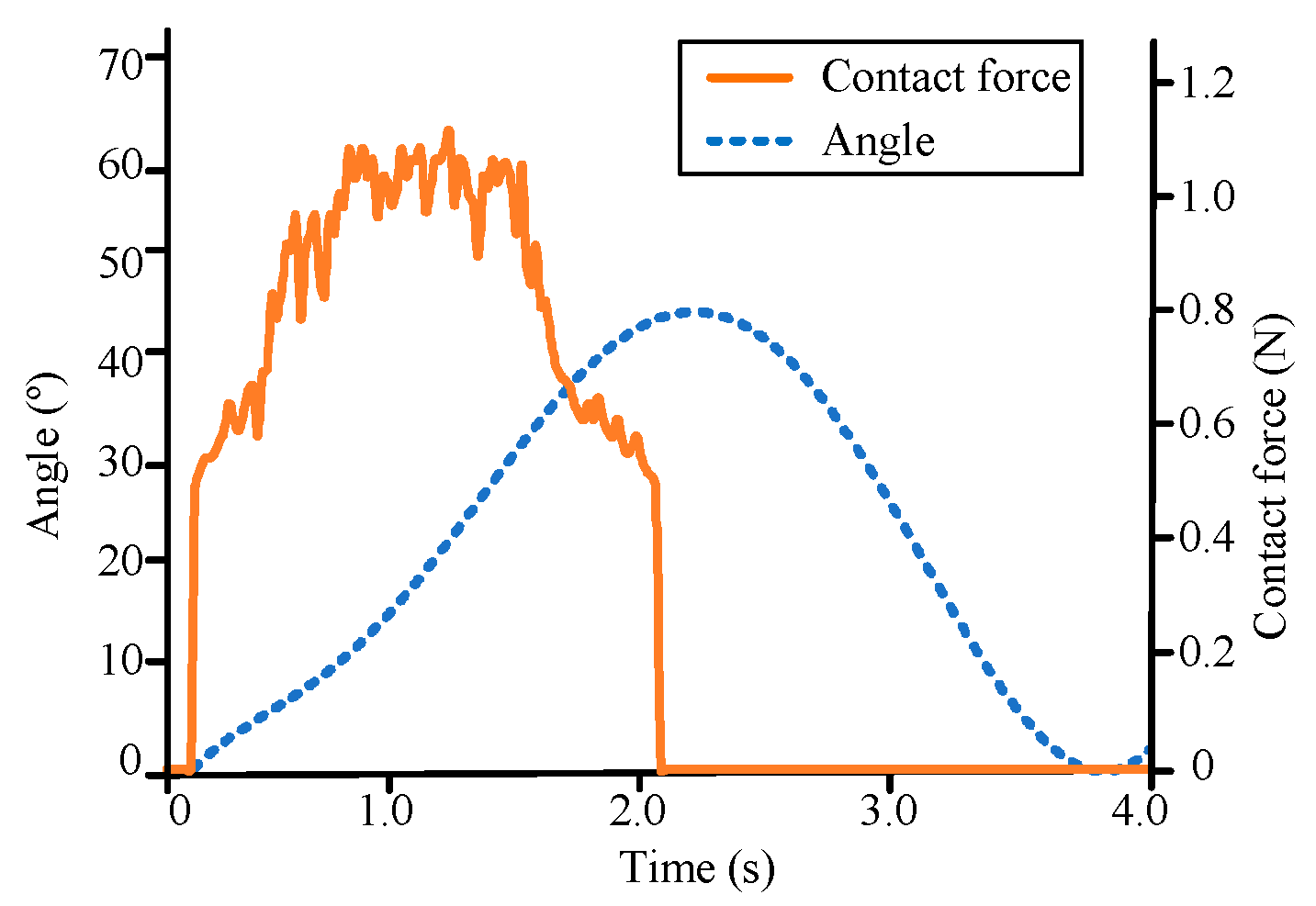
5.3. Grasp Ability Experiment
6. Conclusions and Future Work
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Nguyen, G.; Cercy, K.; Johnson, C.O.; Alam, T.; Parmar, P.G.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abejie, A.N.; et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Health Statistics 2021: Monitoring Health for the SDGs, Sustainable Development Goals; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Jia, J. Hand Function Rehabilitation, 1st ed.; Publishing House of Electronics Industry: Beijing, China, 2019. [Google Scholar]
- Suarez, M.; Rendon-Velez, E. An overview of robotic/mechanical devices for post-stroke thumb rehabilitation. Disabil. Rehabil. Assist. Technol. 2018, 13, 683–703. [Google Scholar] [CrossRef] [PubMed]
- Noronha, B.; Accoto, D. Exoskeletal devices for hand assistance and rehabilitation: A comprehensive analysis of state-of-the-art technologies. IEEE Trans. Med. Robot. Bionics 2021, 3, 525–538. [Google Scholar] [CrossRef]
- Hwang, C.; Seong, J.; Son, D.S. Individual finger synchronized robot-assisted hand rehabilitation in subacute to chronic stroke: A prospective randomized clinical trial of efficacy. Clin. Rehabil. 2021, 26, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Orlando, F.; Behera, L.; Dutta, A.; Saxena, A. Optimal design and redundancy resolution of a novel robotic two-fingered exoskeleton. IEEE Trans. Med. Robot. Bionics 2020, 2, 59–75. [Google Scholar] [CrossRef]
- Kawasaki, H.; Ito, S.; Ishigure, Y.; Nishimoto, Y.; Aoki, T.; Mouri, T.; Sakaeda, H.; Abe, M. Development of a hand motion assist robot for rehabilitation therapy by patient self-motion control. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007. [Google Scholar]
- Singh, N.; Saini, M.; Anand, S.; Kumar, N.; Srivastava, M.V.; Mehndiratta, A. Robotic exoskeleton for wrist and fingers joint in post-stroke neuro-rehabilitation for low-resource settings. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 2369–2377. [Google Scholar] [CrossRef] [PubMed]
- Sandoval-Gonzalez, O.; Jacinto-Villegas, J.; Herrera-Aguilar, I.; Portillo-Rodiguez, O.; Tripicchio, P.; Hernandez-Ramos, M.; Flores-Cuautle, A.; Avizzano, C. Design and development of a hand exoskeleton robot for active and passive rehabilitation. Int. J. Adv. Robot. Syst. 2016, 13, 66. [Google Scholar] [CrossRef] [Green Version]
- Shields, B.L.; Main, J.A.; Peterson, S.W.; Strauss, A.M. An anthropomorphic hand exoskeleton to prevent astronaut hand fatigue during extravehicular activities. IEEE Trans. Syst. Man Cybern. Part A Syst. Hum. 1997, 27, 668–673. [Google Scholar] [CrossRef]
- Hsu, T.H.; Chiang, Y.C.; Chan, W.T.; Chen, S.J. A finger exoskeleton robot for finger movement rehabilitation. Inventions 2017, 2, 12. [Google Scholar] [CrossRef] [Green Version]
- Carbone, G.; Gerding, E.C.; Corves, B.; Cafolla, D.; Russo, M.; Ceccarelli, M. Design of a two-dofs driving mechanism for a motion-assisted finger exoskeleton. Appl. Sci. 2020, 10, 2619. [Google Scholar] [CrossRef]
- Jo, I.; Park, Y.; Lee, J.; Bae, J. A portable and spring-guided hand exoskeleton for exercising flexion/extension of the fingers. Mech. Mach. Theory 2019, 135, 176–191. [Google Scholar] [CrossRef]
- Sun, N.; Li, G.; Cheng, L. Design and validation of a self-aligning index finger exoskeleton for post-stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1513–1523. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Cheng, L.; Sun, N. Design, manipulability analysis and optimization of an index finger exoskeleton for stroke rehabilitation. Mech. Mach. Theory 2022, 167, 104526. [Google Scholar] [CrossRef]
- Li, C.; Yan, Y.; Ren, H. Compliant finger exoskeleton with telescoping super-elastic transmissions. J. Intell. Robot. Syst. 2020, 100, 435–444. [Google Scholar] [CrossRef]
- Agarwal, P.; Deshpande, A. Subject-specific assist-as-needed controllers for a hand exoskeleton for rehabilitation. IEEE Robot. Autom. Lett. 2018, 3, 508–515. [Google Scholar] [CrossRef]
- Li, J.; Wang, S.; Wang, J.; Zheng, R.; Zhang, Y.; Chen, Z. Development of a hand exoskeleton system for index finger rehabilitation. Chin. J. Mech. Eng. 2012, 25, 223–233. [Google Scholar] [CrossRef]
- Cheng, L.; Chen, M.; Li, Z. Design and control of a wearable hand rehabilitation robot. IEEE Access 2018, 6, 74039–74050. [Google Scholar] [CrossRef]
- Zhang, F.; Yang, L.; Fu, Y. Design of a novel elastic torque sensor for hand injuries rehabilitation based on bowden cable. IEEE Trans. Instrum. Meas. 2018, 68, 3184–3192. [Google Scholar] [CrossRef]
- Pu, S.W.; Pei, Y.C.; Chang, J.Y. Decoupling finger joint motion in an exoskeletal hand: A design for robot-assisted rehabilitation. IEEE Trans. Ind. Electron. 2020, 67, 686–697. [Google Scholar] [CrossRef]
- Marconi, D.; Baldoni, A.; McKinney, Z.; Cempini, M.; Crea, S.; Vitiello, N. A novel hand exoskeleton with series elastic actuation for modulated torque transfer. Mechatronics 2019, 61, 69–82. [Google Scholar] [CrossRef]
- Jo, I.; Bae, J. A force-controllable compact actuator module for a wearable hand exoskeleton. In Proceedings of the 19th World Congress the International Federation of Automatic Control, Cape Town, South Africa, 24–29 August 2014. [Google Scholar]
- Tran, P.; Jeong, S.; Wolf, S.L.; Desai, J.P. Patient-specific, voice-controlled, robotic flexotendon glove-ii system for spinal cord injury. IEEE Robot. Autom. Lett. 2020, 5, 898–905. [Google Scholar] [CrossRef]
- Wang, J.; Liu, Z.; Fei, Y. Design and testing of a soft rehabilitation glove integrating finger and wrist function. J. Mech. Robot. 2019, 11, 011015. [Google Scholar] [CrossRef]
- Bützer, T.; Lambercy, O.; Arata, J.; Gassert, R. Fully wearable actuated soft exoskeleton for grasping assistance in everyday activities. Soft Robot. 2021, 8, 128–143. [Google Scholar] [CrossRef] [PubMed]
- Cappello, L.; Meyer, J.T.; Galloway, K.C.; Peisner, J.D.; Granberry, R.; Wagner, D.A.; Walsh, C.J. Assisting hand function after spinal cord injury with a fabric-based soft robotic glove. J. NeuroEng. Rehabil. 2018, 15, 59. [Google Scholar] [CrossRef]
- Yap, H.K.; Lim, J.H.; Nasrallah, F.; Goh, J.C.; Yeow, R.C. A soft exoskeleton for hand assistive and rehabilitation application using pneumatic actuators with variable stiffness. In Proceedings of the 2015 IEEE International Conference on Robotics and Automation (ICRA), Seattle, WA, USA, 26–30 May 2015. [Google Scholar]
- Li, J.; Zhang, Z.; Zhang, L.; Tao, C.; Ji, R.; Fan, J. Review of the kinematic compatibility design of hand exoskeletons. J. Shanghai Jiaotong Univ. 2018, 52, 729–742. [Google Scholar] [CrossRef]
- Santos, V.J.; Valero-Cuevas, F.J. Reported anatomical variability naturally leads to multimodal distributions of Denavit-Hartenberg parameters for the human thumb. IEEE Trans. Biomed. Eng. 2006, 53, 155–163. [Google Scholar] [CrossRef]
- Zafar, U.; Rahman, S.U.; Hamid, N.; Ahsan, J.; Zafar, N. Correlation between height and hand size, and predicting height on the basis of age, gender and hand size. J. Med. Sci. 2017, 25, 425–428. [Google Scholar]
- Huo, S.; Fan, S.; Zhao, C. Measurement of fingers’ width and length of every segment in human. Prog. Anat. Sci. 2003, 9, 326–328. [Google Scholar] [CrossRef]
- Katoch, S.; Chauhan, S.S.; Kumar, V. A review on genetic algorithm: Past, present, and future. Multimed. Tools Appl. 2021, 80, 8091–8126. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Type | Active DoF | Transmission | Actuator | Decoupling of Joints |
|---|---|---|---|---|---|
| This paper | Hybrid | 9 | Linkage/cable | Linear motor | Yes |
| Amadeo [6] | Rigid | 5 | Linkage | DC motor | No |
| Two-Fingered Exoskeleton [7] | Rigid | 7 | Linkage | Servo motor | Yes |
| Hand motion assist robot [8] | Rigid | 18 | Linkage/gear | Servo motor | Yes |
| Robotic Exoskeleton [9] | Rigid | 1 | Linkage/gear | DC motor | No |
| ExoK’ab [10] | Rigid | 8 | Linkage/gear | DC motor | Yes |
| Spring-guided exoskeleton [14] | Hybrid | 1 | Linkage/spring | Linear motor | No |
| WIFRE [15,16] | Hybrid | 3 | Linkage/cable | DC motor | Yes |
| Two-finger exoskeleton [17] | Hybrid | 5 | Linkage/cable | Servo motor | Yes |
| Maestro [18] | Hybrid | 7 | Linkage/cable | DC motor | Yes |
| Hand exoskeleton [23,24] | Hybrid | 7 | Linkage/SEA | DC motor | Yes |
| FLEXotendon Glove-II [25] | Soft | 4 | Cable | Biomimetic tendon | No |
| Soft glove [26] | Soft | 6 | - | Pneumatic actuator | No |
| RELab tenoexo [27] | Soft | 5 | Spring | DC motor | No |
| Soft robotic glove [28] | Soft | 5 | Bladder | Air Pump | No |
| ExoGlove [29] | Soft | 5 | - | Pneumatic actuator | No |
| Requirements | Ranges |
|---|---|
| Link length of the proximal phalange | 37.07–51.48 mm |
| Link length of the middle phalange | 18.09–24.64 mm |
| Motion range of the active MCP f/e | 70° |
| Motion range of the passive MCP a/a | 15° |
| Motion range of the active PIP f/e | 80° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, J.; Tian, Y.; Zhang, D.; Wang, H.; Zhang, Y.; Cheng, B.; Niu, J. Mechanism Design and Performance Analysis of a Wearable Hand Rehabilitation Robot. Machines 2022, 10, 1211. https://doi.org/10.3390/machines10121211
Du J, Tian Y, Zhang D, Wang H, Zhang Y, Cheng B, Niu J. Mechanism Design and Performance Analysis of a Wearable Hand Rehabilitation Robot. Machines. 2022; 10(12):1211. https://doi.org/10.3390/machines10121211
Chicago/Turabian StyleDu, Jiazheng, Yu Tian, Dagan Zhang, Hongbo Wang, Yongshun Zhang, Bo Cheng, and Jianye Niu. 2022. "Mechanism Design and Performance Analysis of a Wearable Hand Rehabilitation Robot" Machines 10, no. 12: 1211. https://doi.org/10.3390/machines10121211