
The SQEIRP Mathematical Model for the COVID-19 Epidemic in Thailand


Abstract
:1. Introduction
2. Materials and Methods
2.1. Model Development for COVID-19
2.2. The Preconditions and Boundedness of the SQEIRP Model Solutions
3. Stability Analysis of Development for COVID-19
3.1. Equilibrium Point of the SQEIRP Model
3.1.1. Disease-Free Equilibrium Point of the SQEIRP Model
3.1.2. Epidemic Equilibrium Point of the SQEIRP Model
3.2. Basic Reproduction Numbers () of the SQEIRP Model
Global Stability Analysis of Disease-free Equilibrium Point of the SQEIRP Model When
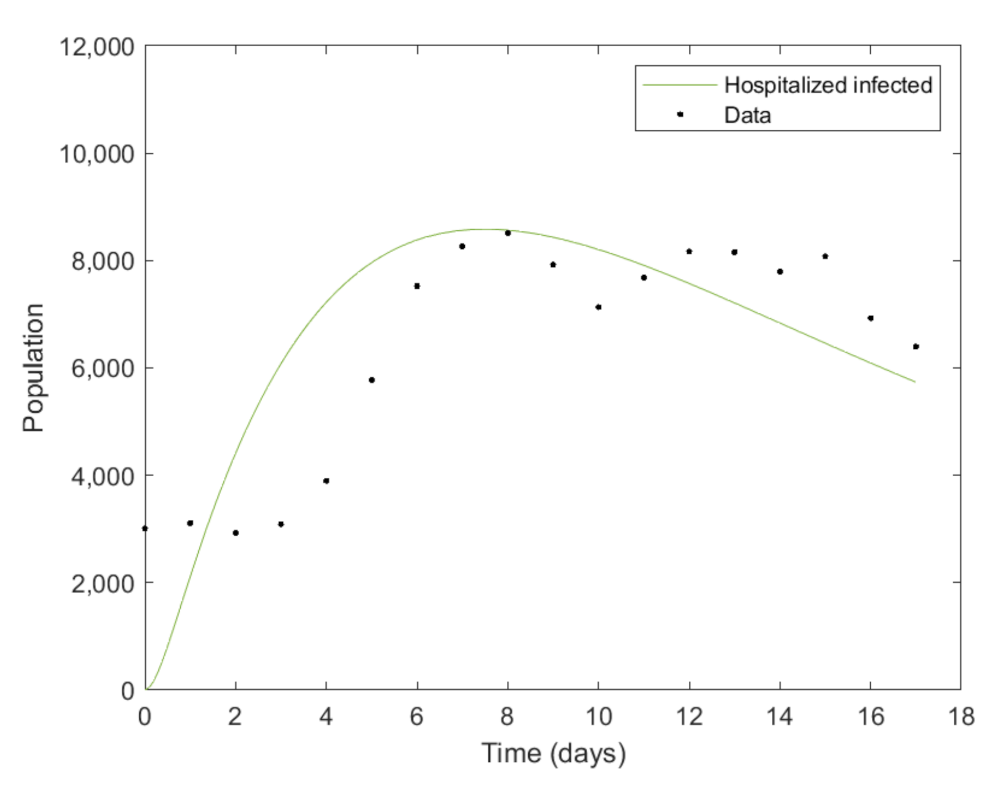
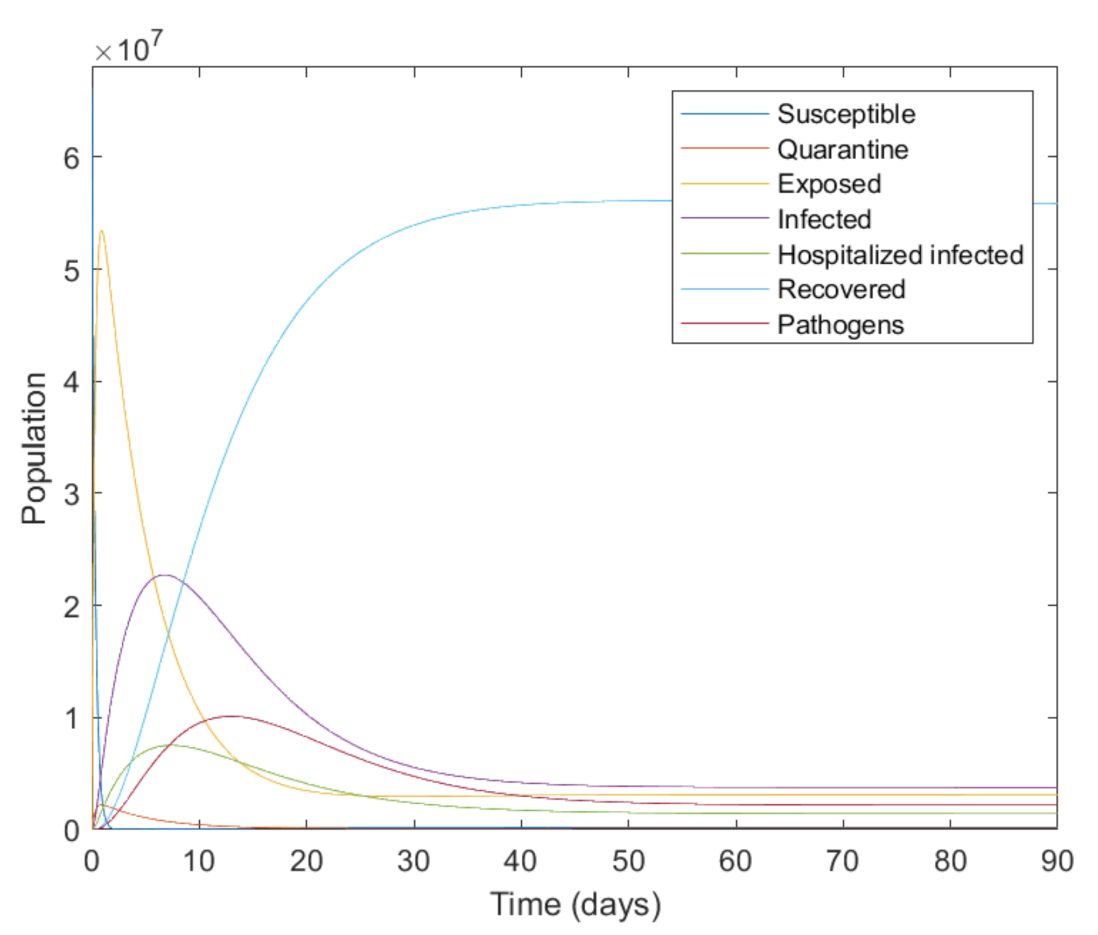
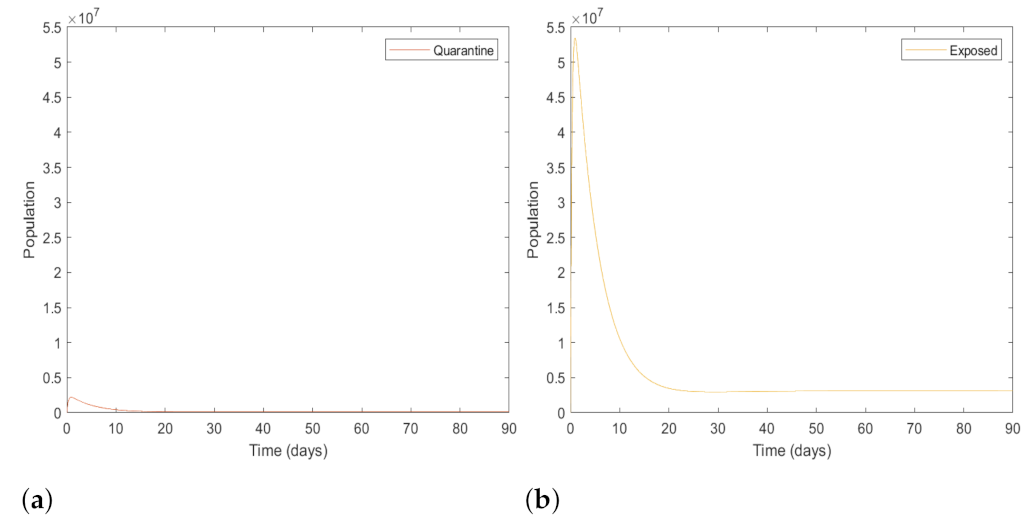
4. Results
4.1. The Numerical Analysis of the SQEIRP Model
4.2. The Value of Basic Reproduction Numbers ()
5. Discussions
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saladino, V.; Algeri, D.; Auriemma, V. The Psychological and Social Impact of Covid-19: New Perspectives of Well-Being. Front. Psychol. 2020, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Reperant, L.A.; Osterhaus, A.D.M.E. AIDS, Avian flu, SARS, MERS, Ebola, Zika… what next? Vaccine 2017, 35, 4470–4474. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, S.M.; Yu, X.H.; Tang, S.L.; Tang, C.K. Coronavirus disease 2019 (COVID-19): Current status and future perspectives. Int. J. Antimicrob. Agents 2020, 55, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Jha, N.K.; Jeyaraman, M.; Rachamalla, M.; Ojha, S.; Dua, K.; Chellappan, D.K.; Muthu, S.; Sharma, A.; Jha, S.K.; Jain, R.; et al. Current Understanding of Novel Coronavirus: Molecular Pathogenesis, Diagnosis, and Treatment Approaches. Immuno 2021, 1, 30–66. [Google Scholar] [CrossRef]
- Thompson, H.A.; Mousa, A.; Dighe, A.; Fu, H.; Arnedo-Pena, A.; Barrett, P.; Bellido-Blasco, J.; Bi, Q.; Caputi, A.; Chaw, L.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARSCoV-2) Setting-specific Transmission Rates: A Systematic Review and Meta-analysis. Clin. Infected Dis. 2021, 73, 754–764. [Google Scholar] [CrossRef]
- Arenas, A.; Cota, W.; Gómez-Gardeñes, J.; Gómez, S.; Granell, C; Matamalas, J. T.; Soriano-Paños, D.; Steinegger, B. Modeling the Spatiotemporal Epidemic Spreading of COVID-19 and the Impact of Mobility and Social Distancing Interventions. Phys. Rev. X 2020, 10, 1–21. [Google Scholar]
- Algehyne, E.A.; Ud Din, R. On global dynamics of COVID-19 by using SQIR type model under non-linear saturated incidence rate. Alex. Eng. J. 2021, 60, 393–399. [Google Scholar] [CrossRef]
- Yuen, K.S.; Ye, Z.W.; Fung, S.Y.; Chan, C.P.; Dong, Y.J. SARS-CoV-2 and COVID-19: The most important research questions. Cell Biosci. 2020, 10, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Hafeez, A.; Ahmad, S.; Siddqui, S.A.; Ahmad, M.; Mishra, S. A Review of COVID-19 (Coronavirus Disease-2019) Diagnosis, Treatments and Prevention. Eurasian J. Med. Oncol. 2020, 4, 116–125. [Google Scholar]
- Aljadeed, R.; AlRuthia, Y.; Balkhi, B.; Sales, I.; Alwhaibi, M.; Almohammed, O.; Alotaibi, A.J.; Alrumaih, A.M.; Asiri, Y. The Impact of COVID-19 on Essential Medicines and Personal Protective Equipment Availability and Prices in Saudi Arabia. Healthcare 2021, 9, 1–14. [Google Scholar] [CrossRef]
- Ayati, N.; Saiyarsarai, P.; Nikfar, S. Short and long term impacts of COVID-19 on the pharmaceutical sector. DARU J. Pharm. Sci. 2020, 28, 799–805. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 8 December 2022).
- World Health Organization. Coronavirus Disease (COVID-19): How Is It Transmitted? Available online: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-covid-19-how-is-it-transmitted (accessed on 14 August 2021).
- Cheng, V.C.C.; Wong, S.K.; Chen, J.H.K.; Yip, C.C.Y.; Chuang, V.W.M.; Tsang, O.T.Y.; Sridhar, S.; Chan, J.F.W.; Ho, P.L.; Yuen, K.Y. Escalating infection control response to the rapidly evolving epidemiology of the coronavirus disease 2019 (COVID-19) due to SARS-CoV-2 in Hong Kong. Soc. Healthc. Epidemiol. Am. 2020, 41, 493–498. [Google Scholar] [CrossRef]
- Ong, S.W.X.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA 2020, 323, 1610–1612. [Google Scholar] [CrossRef] [Green Version]
- Biancolella, M.; Colona, V.L.; Mehrian-Shai, R.; Watt, J.L.; Luzzatto, L.; Novelli, G.; Reichardt, J.K.V. COVID-19 2022 update: Transition of the pandemic to the endemic phase. Hum. Genom. 2022, 16, 1–12. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19—Tests. Available online: https://www.who.int/westernpacific/emergencies/covid-19/information/covid-19-testing (accessed on 14 August 2021).
- De Walque, D.; Friedman, J.; Gatti, R.; Aaditya, M. How Two Tests Can Help Contain COVID-19 and Revive the Economy; World Bank: Washington, DC, USA, 2020; pp. 1–5. [Google Scholar]
- Elliott, J.; Whitaker, M.; Bodinier, B.; Eales, O.; Riley, S.; Ward, H.; Cooke, G.; Darzi, A.; Chadeau-Hyam, M.; Elliott, P. Predictive symptoms for COVID-19 in the community: REACT-1 study of over 1 million people. PLoS Med. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Özdemir, Ö. Coronavirus Disease 2019 (COVID-19): Diagnosis and Management. Erciyes Med. J. 2020, 42, 242–247. [Google Scholar]
- Shrestha, N.; Muhammad, Y.S.; Ulvi, O.; Khan, M.H.; Karamehic-Muratovic, A.; Nguyen, U.S.D.T.; Baghbanzadeh, M.; Wardrup, R.; Aghamohammadi, N.; Cervantes, D.; et al. The impact of COVID-19 on globalization. One Health 2020, 11, 100180. [Google Scholar] [CrossRef]
- Banerjee, S. Mathematical Modeling; Chapman and Hall Book: London, UK; New York, NY, USA, 2014; p. 1. [Google Scholar]
- Mwalili, S.; Kimathi, M.; Ojiambo, V.; Gathungu, D.; Mbogo, R. SEIR model for COVID-19 dynamics incorporating the environment and social distancing. BMC Res. Notes 2020, 13, 1–5. [Google Scholar] [CrossRef]
- Kerr, C.C.; Stuart, R.M.; Mistry, D.; Abeysuriya, R.G.; Rosenfeld, K.; Hart, G.R.; Núñez, R.C.; Cohen, J.A.; Selvaraj, P.; Hagedorn, B.; et al. Covasim: An agent-based model of COVID-19 dynamics and interventions. PLoS Comput. Biol. 2021, 17, e1009149. [Google Scholar] [CrossRef]
- Lozano, M.A.; Garibo i Orts, O.; Piñol, E.; Rebollo, M.; Polotskaya, K.; Garcia-March, M.A.; Conejero, J.A.; Escolano, F.; Oliver, N. Machine Learning and Knowledge Discovery in Databases, Applied Data Science TrackOpen Data Science to Fight COVID-19: Winning the 500k XPRIZE Pandemic Response Challenge; Springer: Berlin/Heidelberg, Germany, 2021; Volume 12978, pp. 384–399. [Google Scholar]
- LANL COVID-19 Cases and Deaths Forecasts, Los Alamos. Available online: https://covid-19.bsvgateway.org/ (accessed on 30 December 2022).
- BOI: The Board of Investment of Thailand, Demographic. Available online: https://www.boi.go.th/ (accessed on 14 October 2022).
- Jankhonkhan, J.; Sawangtong, S. Model Predictive Control of COVID-19 Pandemic with Social Isolation and Vaccination Policies in Thailand. Axioms 2021, 10, 1–17. [Google Scholar] [CrossRef]
- Brauer, F.; Castillo-Chavez, C. A Global Asymptotic Stability Result. In Mathematical Models in Population Biology and Epidemiology; Springer: London, UK; New York, NY, USA, 2012; p. 403. [Google Scholar]
- Buskermolen, M.; Te Paske, K.; van Beek, J.; Kortbeek, T.; Götz, H.; Fanoy, E.; Feenstra, S.; Richardus, J.H.; Vollaard, A. Relapse in the first 8 weeks after onset of COVID-19 disease in outpatients: Viral reactivation or inflammatory rebound? J. Infect. 2021, 83, e6–e8. [Google Scholar] [CrossRef] [PubMed]
- Department Of Disease Control. COVID-19 Infected Situation Reports. Available online: https://ddc.moph.go.th/covid19-daily-dashboard/ (accessed on 28 October 2022).
- Department Of Disease Control. COVID-19 Infected Situation Reports. Available online: https://ddc.moph.go.th/viralpneumonia/eng/index.php (accessed on 28 October 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter Description | Symbol | Value | Source |
|---|---|---|---|
| Birth rate of the human population | A | 0.000028 | [27] |
| Natural human death rate | d | 0.000021 | [27] |
| Probability of the population of | 0.0397 | [28] | |
| the susceptible class that has been quarantined | |||
| Probability of the exposed population | 0.8 | [28] | |
| changing to the infected population | |||
| Rate of transmission from susceptible class | 0.00414 | [23] | |
| to exposed class due to the pathogens | |||
| Rate of transmission from susceptible class | 0.333333 | [Assume] | |
| to exposed class due to the infected | |||
| Proportion of interaction with an infected environment | 0.1 | [23] | |
| Proportion of interaction with an infected individual | 0.1 | [23] | |
| Rate of transmission from quarantine class | 1/5.2 | [28] | |
| to hospitalized infected class | |||
| Rate of transmission from exposed class to infected class | 1/5.2 | [28] | |
| Rate of recovery of the hospitalized infected population | 1/10 | [28] | |
| Rate of recovery of the infected population | 1/8 | [28] | |
| Death rate due to the coronavirus | 0.00011 | [28] | |
| Rate of virus spread to environment by infected class | 0.1 | [23] | |
| Natural death rate of pathogens in the environment | 0.1724 | [23] | |
| Rate of recovered population transferring into a susceptible class | m | 1/90 | [Assume] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jitsinchayakul, S.; Humphries, U.W.; Khan, A. The SQEIRP Mathematical Model for the COVID-19 Epidemic in Thailand. Axioms 2023, 12, 75. https://doi.org/10.3390/axioms12010075
Jitsinchayakul S, Humphries UW, Khan A. The SQEIRP Mathematical Model for the COVID-19 Epidemic in Thailand. Axioms. 2023; 12(1):75. https://doi.org/10.3390/axioms12010075
Chicago/Turabian StyleJitsinchayakul, Sowwanee, Usa Wannasingha Humphries, and Amir Khan. 2023. "The SQEIRP Mathematical Model for the COVID-19 Epidemic in Thailand" Axioms 12, no. 1: 75. https://doi.org/10.3390/axioms12010075