
Innovative CODAS Algorithm for q-Rung Orthopair Fuzzy Information and Cancer Risk Assessment



Abstract
:1. Introduction
- Diagnosis: Healthcare professionals must consider a range of factors when making a diagnosis, including the patient’s symptoms, medical history, and test results. Making an accurate diagnosis is crucial for determining the most appropriate course of treatment.
- Treatment: Healthcare professionals must consider the potential benefits and risks of different treatment options and choose the one that is most likely to be effective and safe for the patient. This can involve weighing the potential benefits and risks of different medications, therapies, or procedures.
- Management of chronic conditions: For patients with chronic conditions, such as diabetes or heart disease, healthcare professionals must make ongoing decisions about the management of the condition. This can involve determining the most appropriate treatment plan, adjusting the treatment plan as needed, and monitoring the patient’s progress.
- Palliative care: Healthcare professionals working in palliative care must make decisions about the care of patients who are nearing the end of life. This can involve determining the most appropriate treatment and care options, as well as addressing issues related to end-of-life planning, such as advance care directives.
1.1. Motivation and Objectives
- 1.
- An improved q-rung orthopair fuzzy CODAS is discussed in detail. The CODAS technique integrates two separate approaches, namely the “simple additive weighting” (SAW) method and the “weighted product method (WPM)”.
- 2.
- A case study related to cancer risk assessment is provided as an application of the q-rung orthopair fuzzy CODAS approach.
- 3.
- The optimal decision for cancer risk assessment is carried out by a comparison analysis of the suggested model with some existing models.
1.2. Organization of Paper
2. Preliminaries
3. q-Rung Fuzzy CODAS Approach
| Algorithm 1: Q-Rung CODAS |
   |
4. Case Study
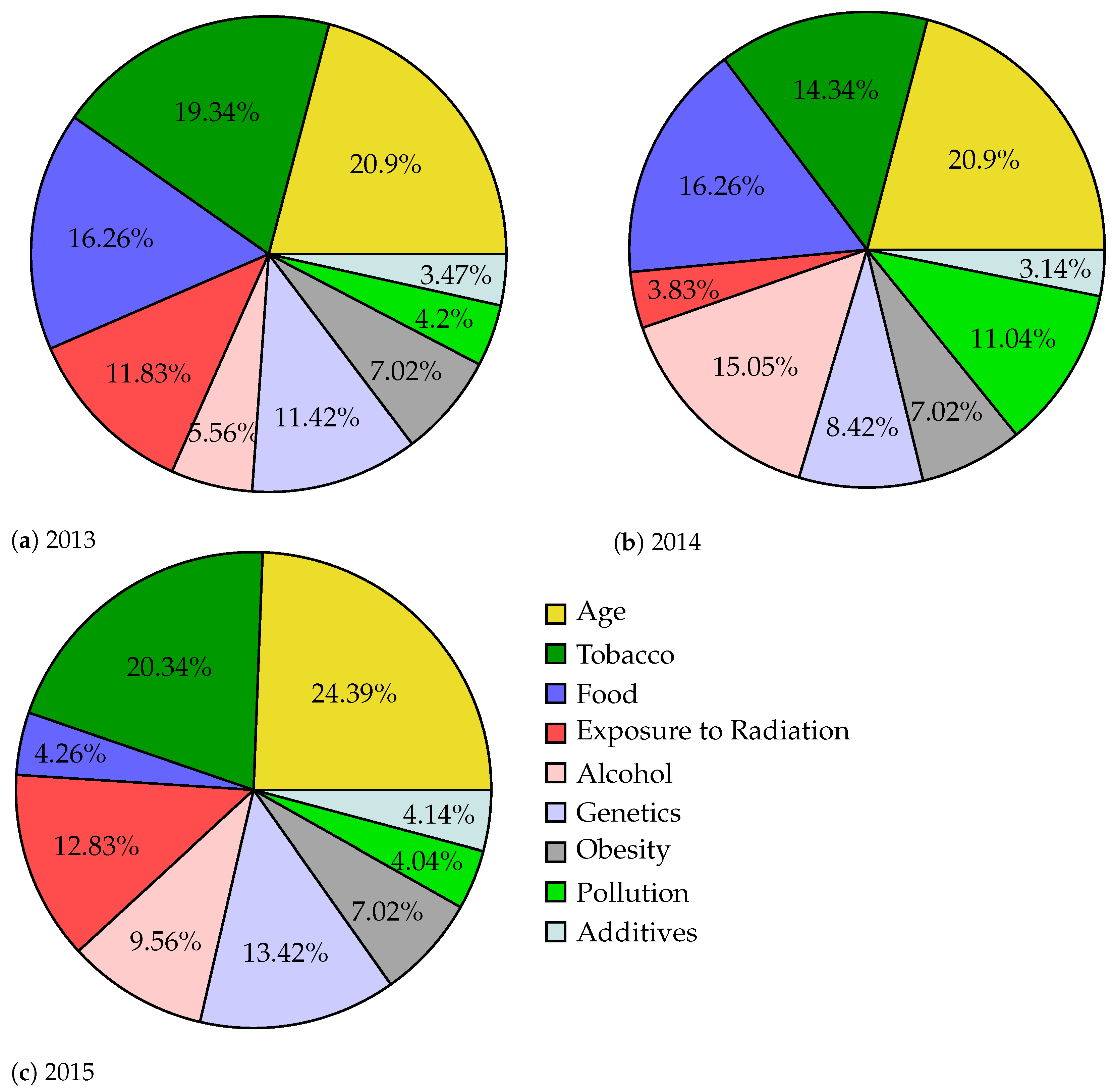
4.1. Risk Factors for Cancer
4.2. Using Tobacco
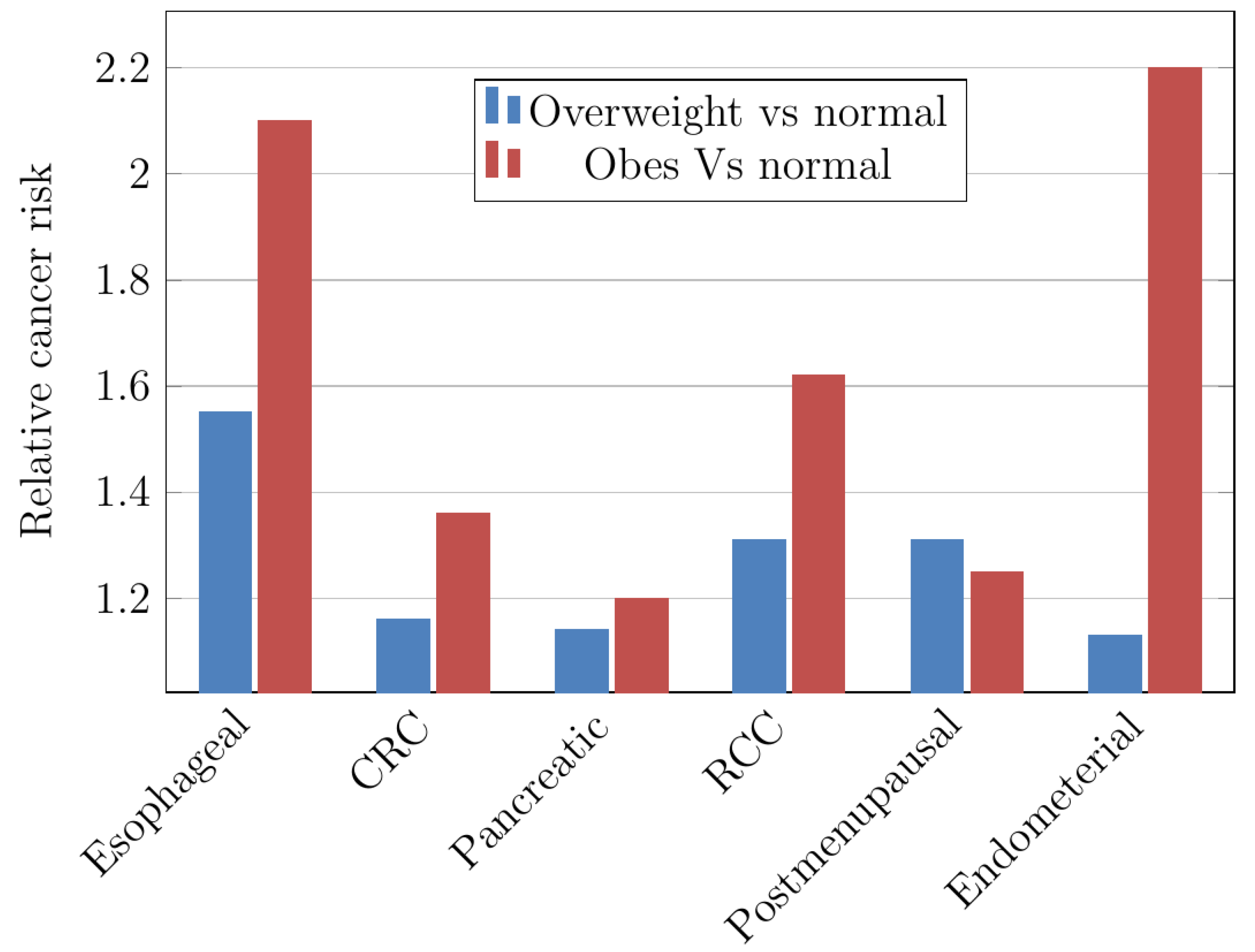
4.3. Obesity
- 1:
- Hyperinsulinemia/IR and abnormalities of the insulin-like development determinant-I (IGF-I) system and indicators;
- 2:
- Sex hormones’ biogenesis and pathway;
- 3:
- Subclinical chronic inferior swelling and oxidative stress;
- 4:
- Changes in the pathophysiology of adipocytokine synthesis;
- 5:
- Determinants of fat deposition;
- 6:
- Microenvironment and natural perturbations;
- 7:
- Determinants of obesity and malignancy such as digestive minerals;
- 8:
- Altered intestinal microbiome; and
- 9:
- Mechanistic determinants of obesity.
4.4. Genetic
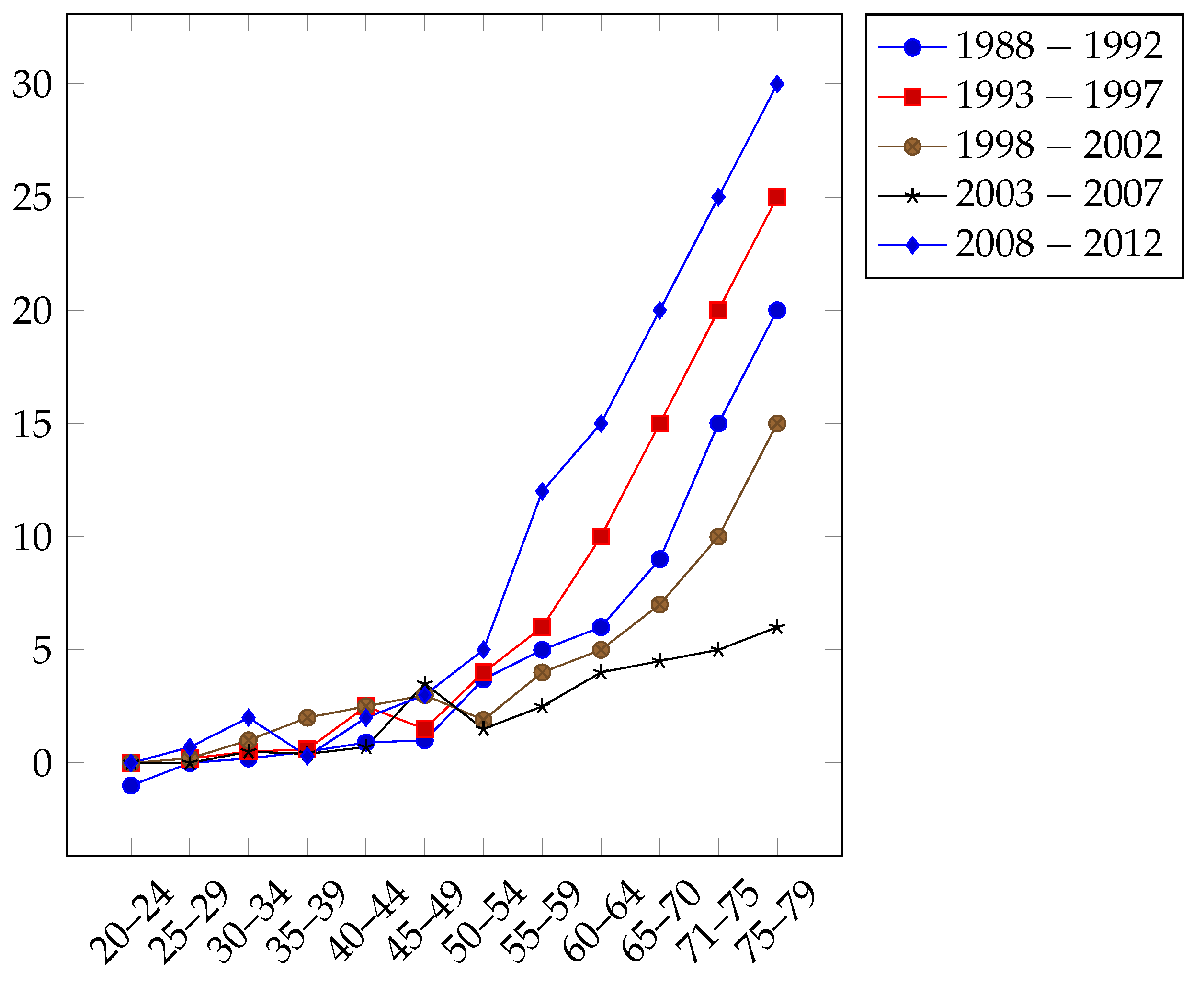
4.5. Older Age
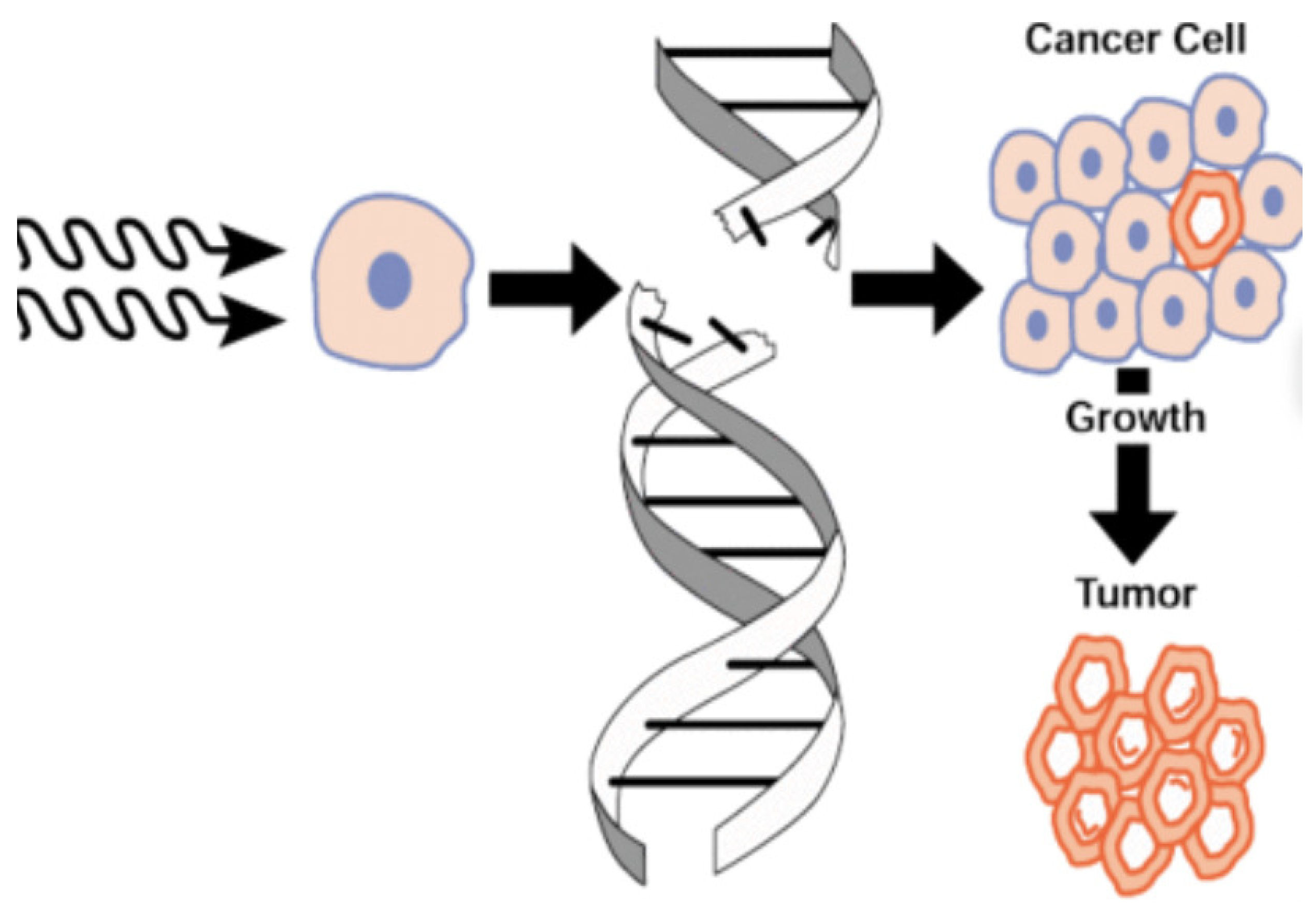
4.6. Exposure to Radiation
4.7. Decision-Making Process
- Step 2: The q-ROF average reputations of the DMs were normalized using Equation (2). Because a DM cannot have a negative reputation value, the positive score algorithm was employed to obtain a crisp average result. The obtained reputation vector of the DMs was
- Step 3: The DMs examined the predefined factors that estimate the risk of cancer. Table 6 contains the DMs’ evaluations of each criterion in terms of the corresponding q-ROFNs.
- Step 5: Now, the q-ROF aggregated significance of the criterion was normalized. Due to the fact that a criterion cannot have negative significance, the positive score function was used to evaluate crisp aggregated values. The normalized values are given in Table 7.
- Step 6: The three decision matrices shown in Table 8 were aggregated using the q-ROFWG operator specified in Equation (4), taking the DMs’ reputational vectors into consideration. Table 9 contains the derived q-rung aggregated assessments of the alternatives in relation to the criteria specified by the three DMs.
- Step 7: Table contains the normalized decision matrix. Equation (5) was used to determine it based on the aggregated decision matrix. The complement operation is used solely for the cost type attributes. Here, we had no such attributes; therefore, the values in Table 9 were used for further evaluations.
- Step 8: To begin, the values of the q-ROF normalized assessments’ score functions were determined using the formulation of the q-ROFNs’ score function. Then, the q-ROFNIS was calculated and provided as {(0.3145, 0.9714) (0.3538, 0.7410) (0.5026, 0.9344) (0.1966, 0.9797) (0.0.4359, 0.8685)}.
- Step 10 and Step 11: We constructed the relative assessment matrix, which is given in Table 11. In the base case scenario, the threshold parameter was set to 0.40.
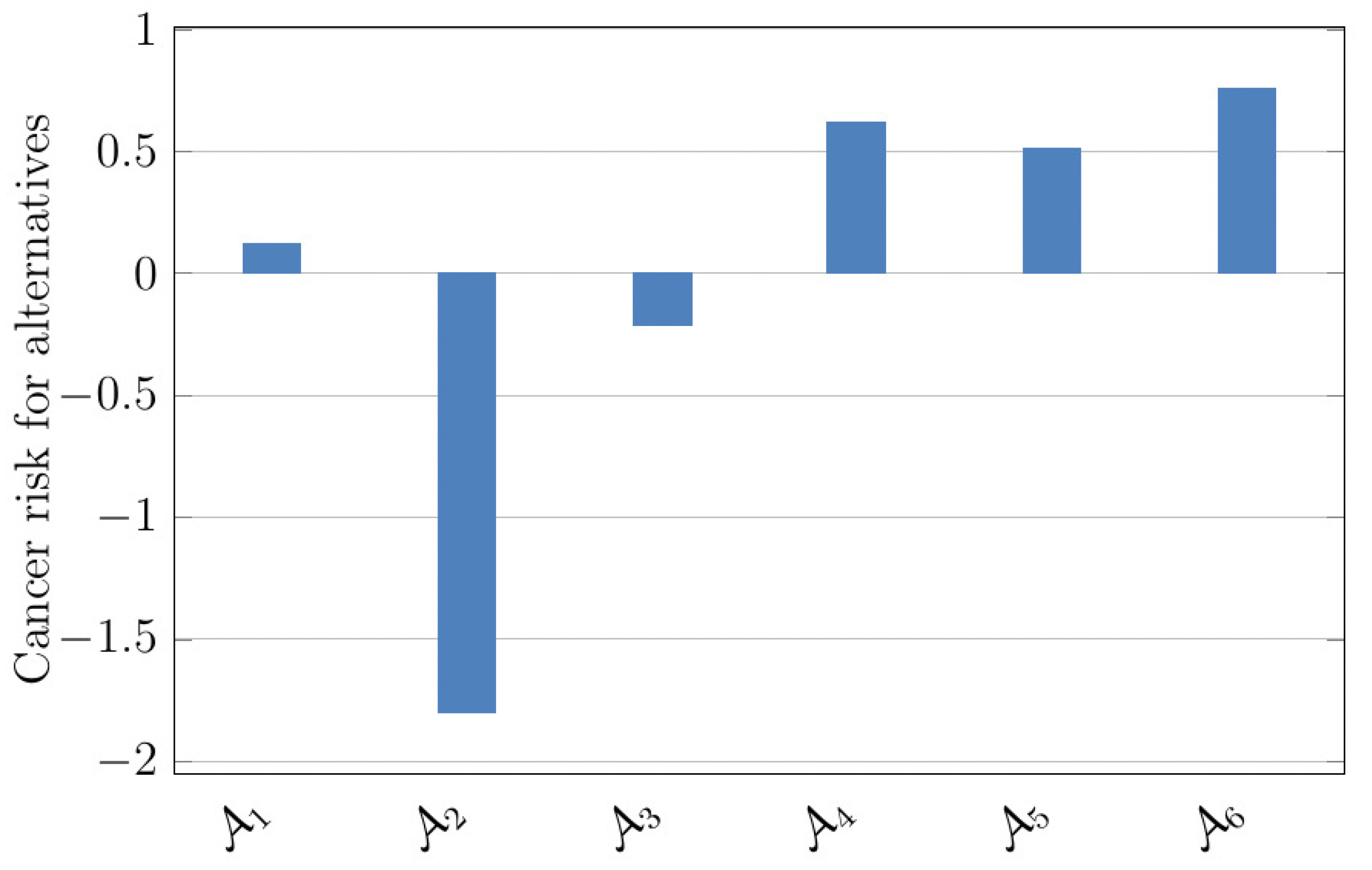
- Step 12: We calculated the assessment scores and ranked the alternatives using Equation (9).
4.8. Comparison Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goff, B.A.; Mandel, L.S.; Drescher, C.W.; Urban, N.; Gough, S.; Schurman, K.M.; Andersen, M.R. Development of an ovarian cancer symptom index: Possibilities for earlier detection. Cancer 2007, 109, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Condron, D.J.; Roscigno, V.J. Disparities within: Unequal Spending and Achievement in an Urban School District. Sociol. Educ. 2003, 76, 18–36. [Google Scholar] [CrossRef]
- Yang, C.; Yang, J.; Liu, Y.; Geng, X. Cancer Risk Analysis Based on Improved Probabilistic Neural Network. Front. Comput. Neurosci. 2020, 14, 58. [Google Scholar] [CrossRef] [PubMed]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
- Atanassov, K.T. Intuitionistic fuzzy sets. Fuzzy Sets Ans Syst. 1986, 20, 87–96. [Google Scholar] [CrossRef]
- Yager, R.R.; Abbasov, A.M. Pythagorean membership grades, complex numbers, and decision making. Int. J. Intell. Syst. 2013, 28, 436–452. [Google Scholar] [CrossRef]
- Yager, R.R. Pythagorean fuzzy subsets. In Proceedings of the 2013 Joint IFSA World Congress and NAFIPS Annual Meeting (IFSA/NAFIPS), Edmonton, AB, Canada, 24–28 June 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 57–61. [Google Scholar]
- Yager, R.R. Generalized orthopair fuzzy sets. IEEE Trans. Fuzzy Syst. 2017, 25, 1222–1230. [Google Scholar] [CrossRef]
- Ghorabaee, M.K.; Zavadskas, E.K.; Turskis, Z.; Antucheviciene, J. A new combinative distance-based assessment (CODAS) method for multi-criteria decision-making. Econ. Comput. Econ. Cybern. Stud. Res. 2016, 50, 25–44. [Google Scholar]
- Ghorabaee, M.K.; Amiri, M.; Zavadskas, E.K.; Hooshmand, R.; Antuchevièiene, J. Fuzzy extension of the CODAS method for multi-criteria market segment evaluation. J. Bus. Econ. Manag. 2017, 18, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Badi, I.A.; Abdulshahed, A.M.; Shetwan, A.G. A case study of supplier selection for steelmaking company in Libya by using Combinative Distance-based Assessment (CODAS) model. Decis. Mak. Appl. Manag. Eng. 2018, 1, 1–11. [Google Scholar] [CrossRef]
- Bolturk, E. Pythagorean fuzzy CODAS and its application to supplier selection in a manufacturing firm. J. Enterp. Inf. Manag. 2018, 31, 550–564. [Google Scholar] [CrossRef]
- Bolturk, E.; Kahraman, C. Interval-valued intuitionistic fuzzy CODAS method and its application to wave energy facility location selection problem. J. Intell. Fuzzy Syst. 2018, 35, 4865–4877. [Google Scholar] [CrossRef]
- Mathew, M.; Sahu, S. Comparison of new multi-criteria decision-making methods for material handling equipment selection. Manag. Sci. Lett. 2018, 8, 139–150. [Google Scholar] [CrossRef]
- Pamucar, D.; Badi, I.; Sanja, K.; Obradovic, R. A Novel Approach for the Selection of Power-Generation Technology Using a Linguistic Neutrosophic CODAS Method: A Case Study in Libya. Energies 2018, 11, 2489. [Google Scholar] [CrossRef] [Green Version]
- Peng, X.; Garg, H. Algorithms for interval-valued fuzzy soft sets in emergency decision making based on WDBA and CODAS with new information measure. Comput. Ind. Eng. 2018, 119, 439–452. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.; Das, S.; Kar, S.; Pamucar, D. An Extension of the CODAS Approach Using Interval-Valued Intuitionistic Fuzzy Set for Sustainable Material Selection in Construction Projects with Incomplete Weight Information. Symmetry 2019, 11, 393. [Google Scholar] [CrossRef] [Green Version]
- Seker, S. A novel interval-valued intuitionistic trapezoidal fuzzy combinative distance-based assessment (CODAS) method. Soft Comput 2020, 24, 2287–2300. [Google Scholar] [CrossRef]
- Liu, P.; Liu, J. Some q-rung orthopair fuzzy bonferroni mean operators and their application to multi-attribute group decision making. Int. J. Intell. Syst. 2018, 33, 315–347. [Google Scholar] [CrossRef]
- Liu, Z.; Wang, S.; Liu, P. Multiple attribute group decision making based on q-rung orthopair fuzzy Heronianmean operators. Int. J. Intell. Syst. 2018, 33, 2341–2364. [Google Scholar] [CrossRef]
- Joshi, B.P.; Gegov, A. Confidence levels q-rung orthopair fuzzy aggregation operators and its applications to MCDM problems. Int. J. Intell. Syst. 2020, 35, 125–149. [Google Scholar] [CrossRef]
- Garg, H. CN-ROFS: Connection number-based q-rung orthopair fuzzy set and their application to decision-making process. Int. J. Intell. Syst. 2021, 36, 3106–3143. [Google Scholar] [CrossRef]
- Liu, P.; Wang, P. Some q-rung orthopair fuzzy aggregation operator and their application to multi-attribute decision making. Int. J. Intell. Syst. 2018, 33, 259–280. [Google Scholar] [CrossRef]
- Peng, X.; Dai, J.; Garg, H. Exponential operation and aggregation operator for q-rung orthopair fuzzy set and their decision-making method with a new score function. Int. J. Intell. Syst. 2018, 33, 2255–2282. [Google Scholar] [CrossRef]
- Jana, C.; Muhiuddin, G.; Pal, M. Some Dombi aggregation of q-rung orthopair fuzzy numbers in multiple-attribute decision making. Int. J. Intell. Syst. 2019, 34, 3220–3240. [Google Scholar] [CrossRef]
- Wei, G.; Gao, H.; Wei, Y. Some q-rung orthopair fuzzy Heronian mean operators in multiple attribute decision making. Int. J. Intell. Syst. 2018, 33, 1426–1458. [Google Scholar] [CrossRef]
- Lin, M.; Li, X.; Chen, L. Linguistic q-rung orthopair fuzzy sets and their interactional partitioned Heronian mean aggregation operators. Int. J. Intell. Syst. 2020, 35, 217–249. [Google Scholar] [CrossRef]
- Khan, M.J.; Ali, M.I.; Kumam, P. A new ranking technique for q-rung orthopair fuzzy values. Int. J. Intell. Syst. 2021, 36, 558–592. [Google Scholar] [CrossRef]
- Zeng, S.Z.; Hu, Y.J.; Xie, X.Y. q-Rung orthopair fuzzy weighted induced logarithmic distance measures and their application in multiple attribute decision making. Eng. Appl. Artif. Intell. 2021, 100, 104167. [Google Scholar] [CrossRef]
- Sitara, M.; Akram, M.; Riaz, M. Decision-making analysis based on q-rung picture fuzzy graph structures. J. Appl. Math. Comput. 2021, 67, 541–577. [Google Scholar] [CrossRef]
- Farid, H.M.A.; Riaz, M. Some generalized q-rung orthopair fuzzy Einstein interactive geometric aggregation operators with improved operational laws. Int. J. Intell. Syst. 2021, 36, 7239–7273. [Google Scholar] [CrossRef]
- Saha, A.; Dutta, D.; Kar, S. Some new hybrid hesitant fuzzy weighted aggregation operators based on Archimedean and Dombi operations for multi-attribute decision making. Neural Comput. Appl. 2021, 33, 8753–8776. [Google Scholar] [CrossRef]
- Feng, F.; Zheng, Y.; Sun, B.; Akram, M. Novel score functions of generalized orthopair fuzzy membership grades with application to multiple attribute decision making. Granul. Comput. 2022, 7, 95–111. [Google Scholar] [CrossRef]
- Mahmood, T.; Ullah, K.; Khan, Q.; Jan, N. An approach toward decision-making and medical diagnosis problems using the concept of spherical fuzzy sets. Neural Comput. Appl. 2019, 31, 7041–7053. [Google Scholar] [CrossRef]
- Ashraf, S.; Abdullah, S. Emergency decision support modeling for COVID-19 based on spherical fuzzy information. Int. J. Intell. Syst. 2020, 35, 1601–1645. [Google Scholar] [CrossRef]
- Attaullah, S.; Rehman, N.; Khan, A.; Park, C. A decision making algorithm for wind power plant based on q-rung orthopair hesitant fuzzy rough aggregation information and TOPSIS. AIMS Math. 2022, 7, 5241–5274. [Google Scholar] [CrossRef]
- Riaz, M.; Farid, H.M.A.; Shakeel, H.M.; Almalki, Y. Modernizing Energy Efficiency Improvement With q-Rung Orthopair Fuzzy MULTIMOORA Approach. IEEE Access 2022, 10, 74931–74947. [Google Scholar] [CrossRef]
- Farid, H.M.A.; Kausar, R.; Riaz, M.; Marinkovic, D.; Stankovic, M. Linear Diophantine Fuzzy Fairly Averaging Operator for Suitable Biomedical Material Selection. Axioms 2022, 11, 735. [Google Scholar] [CrossRef]
- Farid, H.M.A.; Riaz, M. Single-valued neutrosophic Einstein interactive aggregation operators with applications for material selection in engineering design: Case study of cryogenic storage tank. Complex Intell. Syst. 2022, 8, 2131–2149. [Google Scholar] [CrossRef]
- Zararsız, Z.; Riaz, M. Bipolar fuzzy metric spaces with application. Comp. Appl. Math. 2022, 41, 49. [Google Scholar] [CrossRef]
- Alcantud, J.C.R. The relationship between fuzzy soft and soft topologies. J. Intell. Fuzzy Syst. 2022, 24, 1653–1668. [Google Scholar] [CrossRef]
- Karaaslan, F.; Ozlu, S. Correlation coefficients of dual type-2 hesitant fuzzy sets and their applications in clustering analysis. Int. J. Intell. Syst. 2020, 35, 1200–1229. [Google Scholar] [CrossRef]
- Senapati, T.; Mesiar, R.; Simic, V.; Iampan, A.; Chinram, R.; Ali, R. Analysis of Interval-Valued Intuitionistic Fuzzy Aczel–Alsina Geometric Aggregation Operators and Their Application to Multiple Attribute Decision-Making. Axioms 2022, 11, 258. [Google Scholar] [CrossRef]
- Schrek, R.; Baker, L.A.; Ballard, G.P.; Dolgoff, S. Tobacco smoking as an etiologic factor in disease. I. Cancer. Cancer Res. 1950, 10, 49–58. [Google Scholar] [PubMed]
- Calle, E.E.; Thun, M.J. Obesity and cancer. Oncogene 2004, 23, 6365–6378. [Google Scholar] [CrossRef] [PubMed]
- DePinho, R.A. The age of cancer. Nature 2000, 408, 248–254. [Google Scholar] [CrossRef]
- Littlefield, L.G.; Colyer, S.P.; Sayer, A.M. Radiation Emergency Assistance Center/Training Site. In Sister Chromatid Exchanges: 25 Years of Experimental Research Part B Genetic Toxicology and Human Studies; Springer: Cleveland, OH, USA, 2013. [Google Scholar]
- Karagoz, S.; Deveci, M.; Simic, V.; Aydin, N.; Bolukbas, U. A novel intuitionistic fuzzy MCDM-based CODAS approach for locating an authorized dismantling center: A case study of Istanbul. Waste Manag. Res. 2020, 38, 660–672. [Google Scholar] [CrossRef]
- Yeni, F.B.; Özçelik, G. Interval-valued Atanassov intuitionistic Fuzzy CODAS method for multi criteria group decision making problems. Group Decis. Negot. 2019, 28, 433–452. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Qualifications | Experience (Years) | Working in Cancer Hospital | q-ROF |
|---|---|---|---|
| General physician | |||
| Cancer specialist | |||
| Cancer surgeon | |||
| Ph.D. in cancer research |
| Criteria | |
|---|---|
| Age | |
| Genetics | |
| Using tobacco | |
| Obesity | |
| Radiation |
| DMs | Qualifications | Experience (Years) | Experience (Working in Cancer Hospital) |
|---|---|---|---|
| Ph.D. in cancer research | 11 | 10 | |
| Cancer specialist | 9 | 3 | |
| General physician | 7 | 1.5 |
| DMs | Qualifications | Experience (Years) | Experience (Working in Cancer Hospital) | Average |
|---|---|---|---|---|
| (0.450, 0.910) | (0.250, 0.700) | ( 0.250, 0.700) | (0.350, 0.805) | |
| (0.550, 0.970) | (0.500, 0.500) | (0.250, 0.700) | (0.350, 0.980) | |
| (0.900, 0.150 ) | (0.700, 0.250) | (0.700, 0.250) | (0.775, 0.540) |
| DMs | Importance | ||
|---|---|---|---|
| Average q-ROFNs | Positive Score | Normalized | |
| (0.350, 0.805) | 0.6585 | 0.2861 | |
| 0.5360 | 0.2329 | ||
| 1.1070 | 0.4810 | ||
| Criterion | DMs | ||
|---|---|---|---|
| Criterion | Importance | ||
|---|---|---|---|
| Aggregated q-ROFNs | Positive Score | Normalized | |
| (0.7800, 0.4262) | 1.3373 | 0.2500 | |
| (0.5412, 0.5892) | 0.9653 | 0.1805 | |
| (0.5442, 0.5865) | 0.9694 | 0.1812 | |
| (0.6697, 0.4506) | 1.1599 | 0.2169 | |
| (0.6304, 0.7006) | 0.9170 | 0.1714 | |
| Experts | Alternatives | Criterion | ||||
|---|---|---|---|---|---|---|
| (0.3220, 0.9600) | (0.3210, 0.9200) | (0.4130, 0.9600) | (0.5120, 0.6300) | (0.8100, 0.2540) | ||
| (0.1120, 0.9700) | (0.1320, 0.9700) | (0.4320, 0.9400) | (0.5120, 0.6900) | (0.2320, 0.9800) | ||
| (0.2120, 0.9200) | (0.2110, 0.9300 ) | (0.1120, 0.6300) | (0.6120, 0.9500 ) | (0.8120, 0.8600) | ||
| (0.9120, 0.7400) | (0.9820, 0.4000) | (0.9600, 0.6000) | (0.8820, 0.6000 ) | (0.8720, 0.3000 ) | ||
| (0.3000, 0.8000 ) | (0.4000, 0.6500) | (0.8000, 0.3000) | (0.9000, 0.2000) | (0.5500, 0.5000) | ||
| (0.6500, 0.4000) | (0.1000, 0.9750) | (0.8000, 0.3000) | (0.4000, 0.6500 ) | (0.5500, 0.5000 ) | ||
| (0.9920, 0.3400) | (0.3310, 0.2410) | (0.7720, 0.3680) | (0.9820, 0.4400) | (0.3400, 0.9120) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.9920, 0.3400) | (0.3310, 0.2410) | (0.7720, 0.3680) | (0.9820, 0.4400) | (0.3400, 0.9120) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| (0.5340, 0.9720) | (0.8720, 0.5140) | (0.5340, 0.9320) | (0.1340, 0.9920) | (0.7820, 0.4130) | ||
| Criterion | Alternatives | |||||
|---|---|---|---|---|---|---|
| (0.7189, 0.8068) | (0.3415, 0.9714) | (0.1883, 0.9170) | (0.8785, 0.7637) | (0.3186, 0.9572) | (0.6903, 0.3573) | |
| (0.3281, 0.7428) | (0.5081, 0.8362) | (0.2605, 0.8343) | (0.6447, 0.7076) | (0.3538, 0.7410) | (0.2986, 0.9158) | |
| (0.6455, 0.8078) | (0.5026, 0.9344) | (0.4772, 0.4860 ) | (0.6784, 0.6371) | (0.7615, 0.4660) | (0.7903, 0.7763) | |
| (0.8150, 0.5206) | (0.1966, 0.9797) | (0.7524, 0.7995) | (0.6364, 0.6000) | (0.9096, 0.3714) | (0.4703, 0.6278) | |
| (0.4359, 0.8685) | (0.5523, 0.8527) | (0.7092, 0.6846) | (0.7056, 0.4757) | (0.4886, 0.7266) | (0.6903, 0.5958) | |
| Distance Measure | Alternatives | |||||
|---|---|---|---|---|---|---|
| Weighted Euclidean | 0.3818 | 0.0618 | 0.3263 | 0.4639 | 0.4466 | 0.4871 |
| Weighted Hamming | 0.2712 | 0.0304 | 0.2453 | 0.3943 | 0.2945 | 0.4036 |
| Alternatives | ||||||
|---|---|---|---|---|---|---|
| 0 | −0.3200 | −0.0555 | 0.0821 | 0.0648 | 0.1053 | |
| 0.3200 | 0 | 0.2645 | 0.4020 | 0.3848 | 0.4253 | |
| 0.0554 | −0.2645 | 0 | 0.1375 | 0.1203 | 0.1607 | |
| −0.0821 | −0.4020 | −0.1375 | 0 | −0.0172 | 0.0232 | |
| −0.0648 | −0.3848 | −0.1203 | 0.0172 | 0 | 0.0405 | |
| −0.1053 | −0.4253 | −0.1607 | −0.0232 | −0.0405 | 0 |
| Alternatives | Assessment Score | Rank |
|---|---|---|
| 0.1232 | 4 | |
| −1.7966 | 6 | |
| −0.2095 | 5 | |
| 0.6156 | 2 | |
| 0.5123 | 3 | |
| 0.7550 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kausar, R.; Farid, H.M.A.; Riaz, M.; Gonul Bilgin, N. Innovative CODAS Algorithm for q-Rung Orthopair Fuzzy Information and Cancer Risk Assessment. Symmetry 2023, 15, 205. https://doi.org/10.3390/sym15010205
Kausar R, Farid HMA, Riaz M, Gonul Bilgin N. Innovative CODAS Algorithm for q-Rung Orthopair Fuzzy Information and Cancer Risk Assessment. Symmetry. 2023; 15(1):205. https://doi.org/10.3390/sym15010205
Chicago/Turabian StyleKausar, Rukhsana, Hafiz Muhammad Athar Farid, Muhammad Riaz, and Nazmiye Gonul Bilgin. 2023. "Innovative CODAS Algorithm for q-Rung Orthopair Fuzzy Information and Cancer Risk Assessment" Symmetry 15, no. 1: 205. https://doi.org/10.3390/sym15010205