1. Introduction
Spondylolisthesis is defined as a pathological condition of the spine in which the ventral to the ventrocaudal displacement of the cranial vertebra relative to the more caudal vertebra occurs. A specific type of spondylolistheses is dysplastic spondylolisthesis, which is based on dysplastic changes most commonly in the lumbosacral junction (further referred to as LS). According to the degree of dysplastic changes and the extent of the slip, dysplastic spondylolisthesis is further divided into high dysplastic and low dysplastic types. As a result of the pathological shift, anatomical changes lead to the asymmetry of the lumbosacral junction and decompensation of the sagittal profile of the entire spine, which affects the posture when standing and walking [
1].
Several classification systems have been developed to divide spondylolisthesis into subtypes. In 1974, a classification was created in Montreal by the team of Wiltse, Newman, and MacNab, which divided spondylolisthesis into six types according to the etiology of the disability, namely dysplastic, isthmic, degenerative, traumatic, pathological, and iatrogenic spondylolisthesis [
2]. Another classification was developed by Marchetti and Bartolozzi in 1997 [
3]. This classification includes two basic types: developmental and acquired spondylolisthesis. Acquired spondylolisthesis is divided into traumatic, pathologic, degenerative, and postsurgical. Developmental spondylolisthesis is further divided into the subgroups of low dysplastic and high dysplastic types.
The division into low dysplastic and high dysplastic spondylolisthesis is an important prognostic factor and indicator of subsequent treatment. In low dysplastic spondylolisthesis (further referred to as LDDS), the slip is up to 50% and the parallel position of the endplates of the vertebral body and the sacrum is maintained. There is no significant kyphotisation of the LS junction. The upper edge of the sacrum is usually without a defect in the front of the vertebral body. The risk of deformity progression is low. Due to the low risk of progression, patients may be treated conservatively. In the case of asymptomatic patients, clinical and radiological conditions are checked at regular intervals and surgical treatment is indicated by worsening subjective difficulties and by the increasing extent of the slip as seen on X-ray scans.
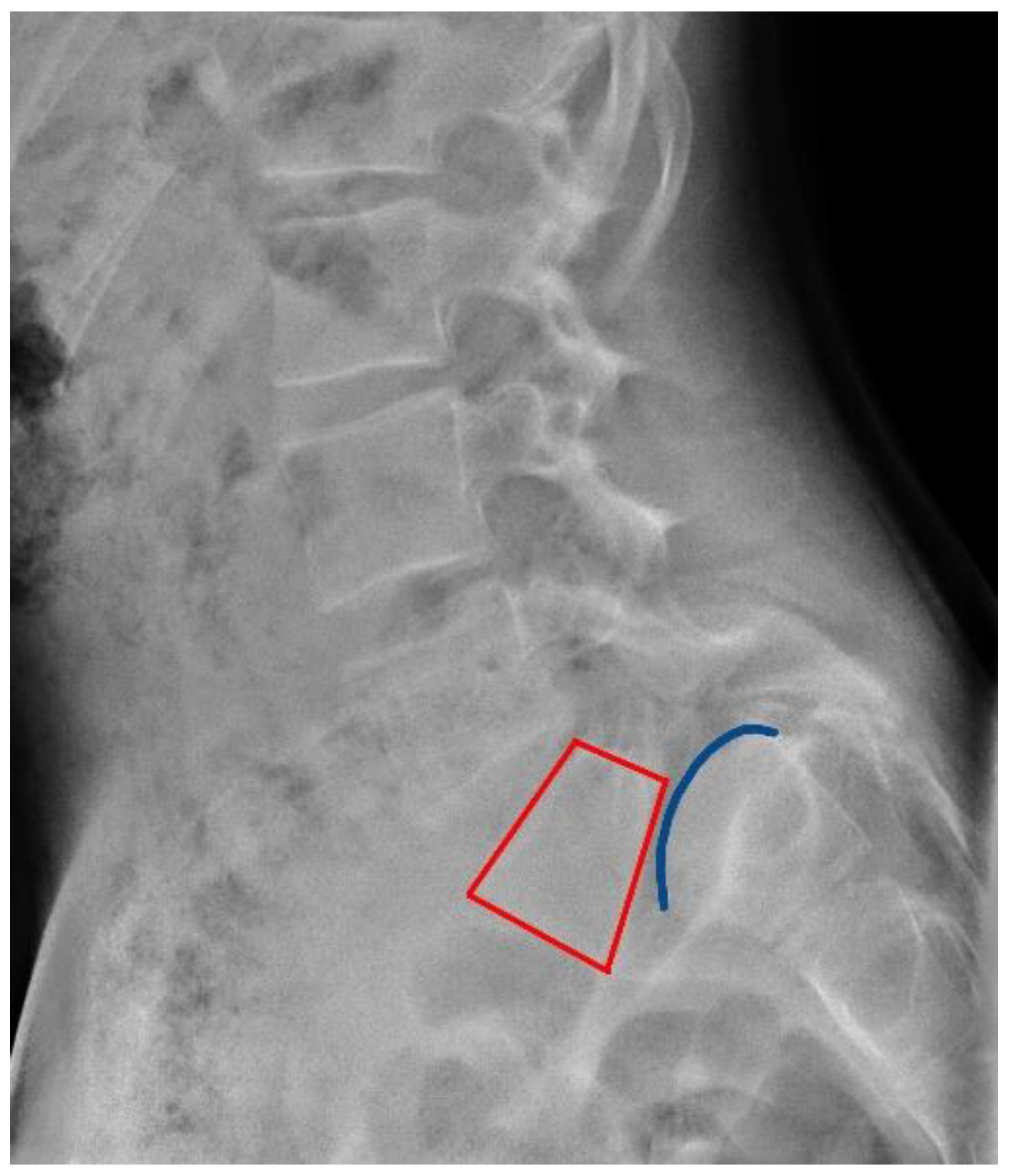
The high dysplastic type (further referred to as HDDS), on the contrary, is characterized by a slip of more than 50% and should be always indicated for surgical treatment. The L5 vertebral body assumes a trapezoidal shape in the sagittal plane with a concave lower endplate. The S1 upper endplate resembles the shape of a dome and the front part of the S1 body is defective, thus contributing to the progression of the slip (
Figure 1). The risk of slip progression in HDDS is high. There is a gradual forward and downward movement of the L5 body, leading to lumbar hyperlordosis, segmental kyphotisation of the LS junction, pelvic retroversion, and ventral movement of the femoral heads. These changes lead to alterations in spinopelvic balance and normal standing and walking [
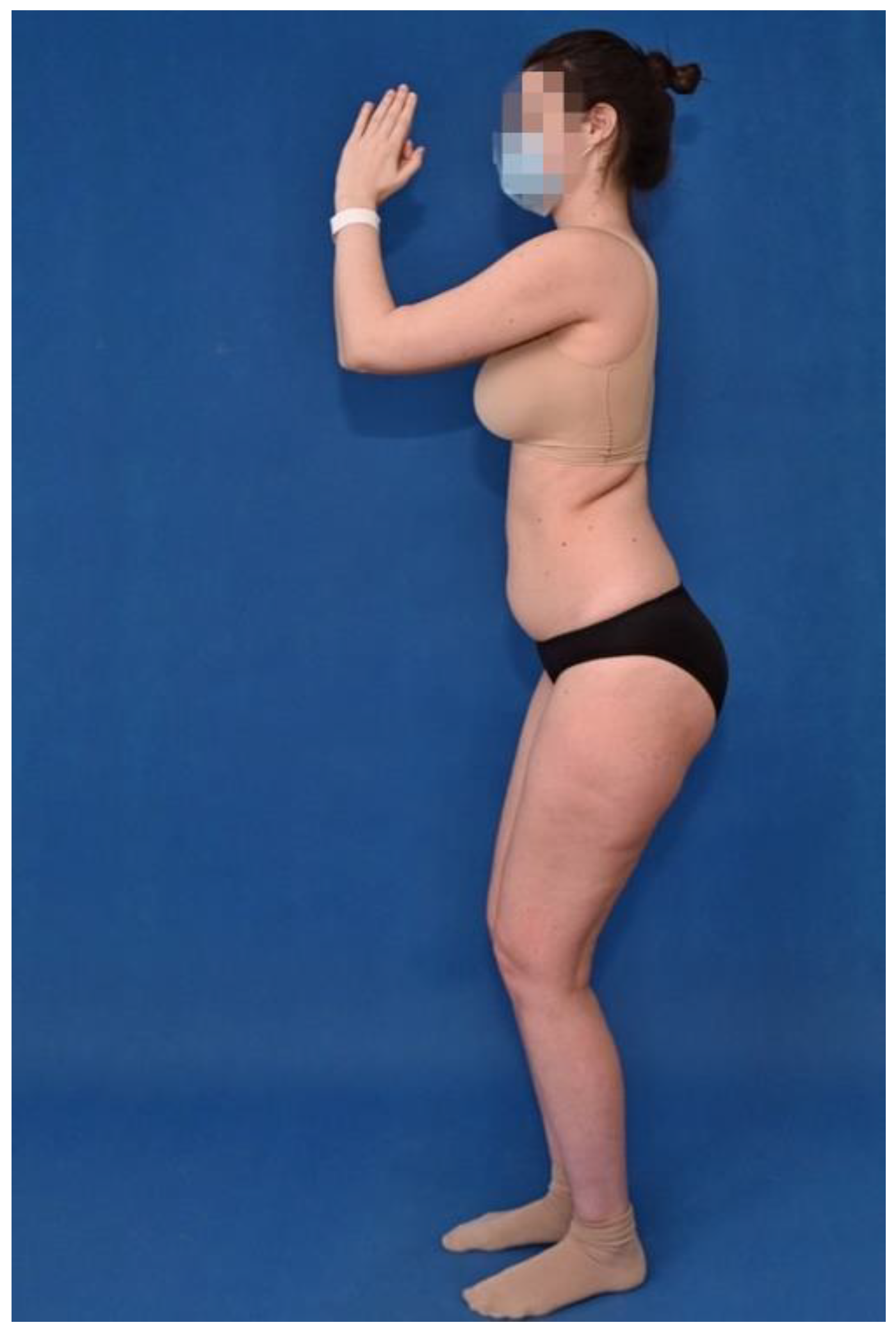
4]. Vertical position of the sacrum with a ventral displacement of the femoral heads and the hamstring contracture leads to semiflexion of the hip and knee joints, leading to a change in the sagittal posture profile, the so-called “monkey’s gait” [
5]. The change in posture is documented in
Figure 2. The incidence of highly dysplastic spondylolisthesis is 11.3% in adults diagnosed with spondylolisthesis [
6]. Subjective difficulties most often include lumbar spine pain with possible neurological complications due to nerve root irritation.
The measurement of the extent of the slip is evaluated on X-ray scans using the Meyerding scale [
7]. Meyerding differentiated the sacral endplate into quarters and categorized spondylolisthesis into grades I–IV according to the direction of the slip in a certain quarter. Later, two more grades were added: grade 0, characterized by a normal state without displacement; and grade V, corresponding to spondyloptosis. The percentage expression of the extent of the slip is evaluated by measuring according to Taillard [
8].
Despite significant progress in the diagnosis and development of indication patterns, the question of the appropriate therapeutic algorithm remains controversial. With the development of surgical methods, conservative therapy is declining in favor of surgical therapy. The aim of the surgery should be to prevent the progression of the slip and to correct the asymmetry of lumbosacral parameters, leading to an improvement in the overall sagittal balance of the spine, and the consequent improved standing and walking posture. The clinical effect should be to reduce pain in the LS junction. The cosmetic effect is also significant.
There is significant variability in individual surgical procedures, from fixation in situ, with no reduction in the slipped vertebra, to extensive surgeries with an effort to completely reduce the slipped vertebra; these procedures use different surgical approaches and include more vertebral segments in stabilization [
9].
The aim of this paper is to describe the individual surgical methods used for patients having dysplastic spondylolisthesis with a shift of more than 25%, who were operated on at our institution, and to determine the ideal surgical therapeutic algorithm according to the extent of the vertebral slip.
3. Results
3.1. Slip Reduction and Retention
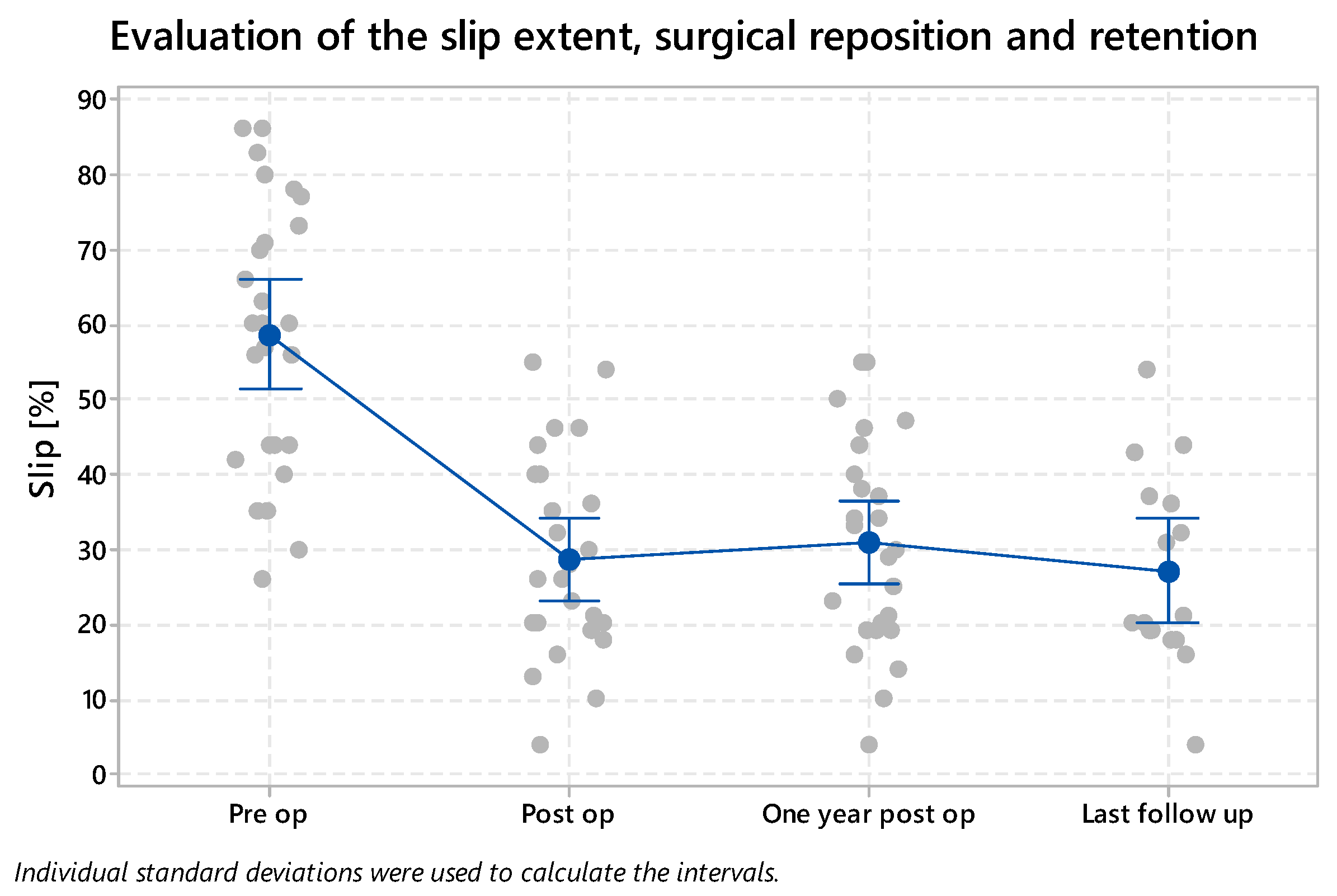
The average preoperative extent of the slip was 60% (27–86%). Postoperatively, the extent of the slip was reduced to 28% (4–55%). The reduction, therefore, reduced the size of the slip by more than 50% (32% statistically significant slip decrease,
p = 0.000). Overall, the extent of the slip was 32% one year after the surgery and 28% during the long-term observation. The given results are summarized in
Figure 5.
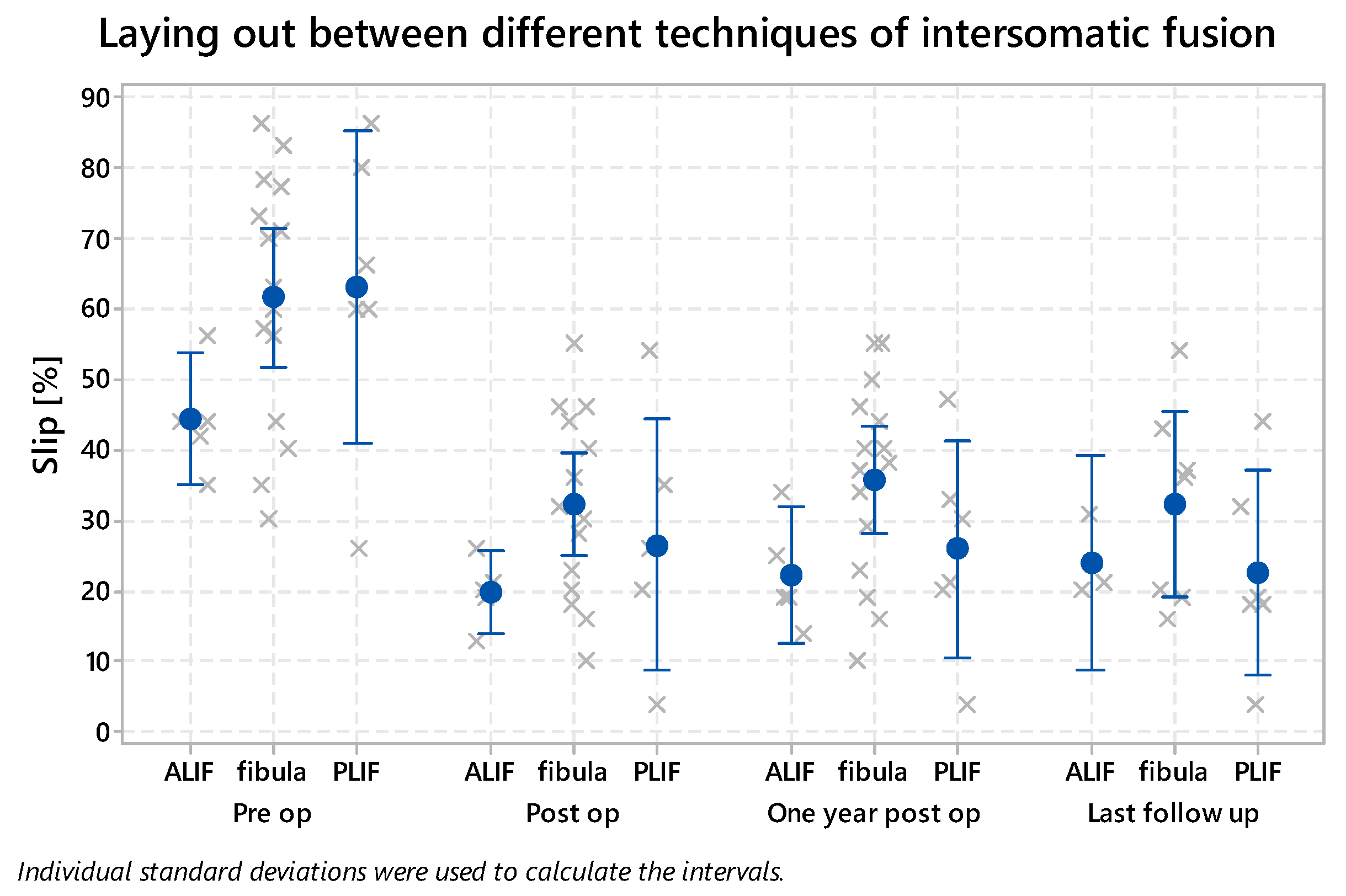
With the PLIF technique, the slip was reduced and decreased from 67% (54–86%) to 26% postoperatively (4–54%) (31% statistically significant slip decrease, p = 0.000). When using fibula, there was a decrease from 62% (27–86%) to 32% (10–55%) (30% statistically significant slip decrease, p = 0.000), and when combining the approaches and using ALIF interbody fusion, the slip decreased from 44% (35–56%) to 20% (13–26%) (24% statistically significant slip decrease, p = 0.001).
Slip retention was evaluated one year after surgery and, on average, 7 years after surgery. The distribution among the individual methods of interbody fusion, i.e., the PLIF technique, the use of a fibular graft, and the ALIF technique is shown in
Figure 6. The only increase in the slip extent—from 32% to 35%—was observed with the use of fibula, between the postoperative period and one year after surgery. However, during the long-term follow-up, the extent of the slip again corresponded to the postoperative value of the slip, i.e., 32%. After repeated evaluation of the X-ray images, we concluded that this was most likely caused by an incorrect measurement of the extent of the slip, given by the rotation of X-ray scans.
All performed surgical methods led to statistically significant improvement in radiological parameters. In repeated postoperative examinations, there were no recurrences of slips, due to the creation of a firm fusion in the affected segment. For large slips, of over 50%, we achieved a better reduction in the slip with the PLIF technique compared to the use of the fibular graft.
3.2. Surgical Time and Complications
The time of the surgery was measured from the skin incision to the end of the surgical procedure. The average surgery time corresponded to 220 min. When employing the PLIF technique, the surgery lasted an average of 227 min; when using the fibula allograft, this was 204 min. With the ALIF technique, i.e., the combination of anterior and posterior approaches, the surgery took 250 min. The combination of approaches, the need to turn the patient from the prone to the supine position, and the need to re-drape the operating field causes a time delay, which is reflected in the total surgery time.
The extent of blood loss corresponded to an average of 740 mL in all techniques. When employing the dorsal approach only and the PLIF technique, this was 871 mL; when using a fibular graft, it was 709 mL. When combining the posterior and the anterior approaches, the extent of blood loss was 658 mL, i.e., less than in the posterior approach requiring the opening of the spinal canal.
Early complications, occurring up to 3 months after the surgery, were present in 5 patients (5/32; 16%). Of these, neurological complications occurred in 4 patients (4/32; 12.5%). In 3 patients, surgical revision was necessary with the need to reposition screws because of their malposition; subsequent clinical improvement was reported. One patient had transitory buttock hypesthesia with spontaneous regression over time, without the need for surgical revision. One patient required revision of the surgical wound because of secondary healing in the early postoperative period.
We noted that two patients experienced late complications. In the first patient, the screw in the S1 vertebra broke (
Figure 7). Due to negative symptoms and the unchanged position of the instrumentation, surgical revision was not indicated, and the patient has been and still is treated conservatively.
In the other patient, we observed a ventral displacement of the L4 vertebra over the L5/S1 fusion (
Figure 8). The patient was operated on using the PLIF technique. Thus, this was most likely an iatrogenic involvement and overload of the segment above the fusion after the release of the dorsal structures of the L5/S1 segment. At the current time, 6 years after surgery, the patient’s problems are only mild and intermittent. If difficulties progress, we will have to indicate a surgical revision with an extension of the instrumentation to L4 and a 360° fusion of the L4/L5 segment.
3.3. Sagittal Balance
Another part of the evaluation was the radiological measurement of sagittal balance in operated patients. The Slip Angle (SA) was 16° on average (min 0°–max 53°) before surgery; it was reduced to 9° on average (min 0°–max 28°) postoperatively. The Pelvic Incidence (PI) was 70° on average (min 55°–max 84°) preoperatively and 70° on average (min 46°–max 84°) postoperatively. The Pelvic Tilt (PT) was 31° on average (min 5°–max 54°) preoperatively and 24° on average (min 5°–max 48°) postoperatively. The Sacral Slope (SS) was 39° on average (min 20°–max 67°) preoperatively and 43° on average (min 22°–max 75°) postoperatively. The Incidence of L5 (IL5) was 55° on average (min 20°–max 111°) preoperatively and 43° on average (min 21°–max 74°) postoperatively. The lumbar lordosis angle (Lumbar Lordosis, LL) corresponded to a preoperative magnitude of 56° on average (min 20°–max 82°) and postoperatively to 51° on average (min 24°–max 82°). Results of the evaluation of spinopelvic parameters are summarized in
Table 1.
3.4. Satisfaction Questionnaires
Patient-reported outcomes after surgical therapy were evaluated using the Oswestry Disability Index (ODI) during a long-term follow-up [
14]. ODI evaluates lower-back pain according to different physiological situations, such as resting pain, personal care, lifting weights, walking, sitting, standing, sex life, social life, and traveling. The score of the pain is 0–5 in all situations, where 0 corresponds to minimal pain and 5 to maximal pain. The final score is expressed as a percentage. The interpretation of the score corresponds to 0–20%: minimal disability; 21–40%: moderate disability; 41–60%: severe disability; 61–80%: crippled; 81–100%: bed-bound or exaggerating symptoms. Patients who had posterior approach surgery using the PLIF technique rated the outcome on average at 18%, patients with a posterior approach surgery using the fibula at 8%, and patients on the combined approach at 10%. As mentioned above, the range of 0–20% corresponds to minimal disability. Patients can cope with most living activities. None of the surgical methods resulted in a restriction of normal daily activities due to postoperative LS spine pain.
The overall satisfaction was evaluated by using the Overall Treatment Evaluation (OTE) questionnaire [
15]. In this questionnaire, the patient is asked about the change in the quality of life following the surgical treatment, and the importance of this change to the patient’s normal daily activities. All patients (100%) reported a change for the better compared to the preoperative condition, and 64% of the respondents reported a much better condition in their evaluation of the treatment. The perception of this change was assessed by 64% of patients as being important, and by 36% of patients as being extremely/very important. As a conclusion, we can state that all patients reported an improvement in their quality of life following the surgical therapy.
4. Discussion
Dysplastic spondylolisthesis is a specific type of involvement of the spinal segment, which affects the L5/S1 segment and occurs twice as often in women [
16]. Clinical symptoms and signs often appear in childhood and adolescence during the growth spurt [
17]. Our group of patients was also dominated by women, who made up almost 70% of the total number of patients. The age distribution also corresponds to the above-mentioned statement, with the majority of patients being mostly adolescents and young adults.
In order to correctly determine the therapeutic algorithm of this pathology, a thorough diagnosis and the correct classification into classification groups are necessary. The long-format X-ray of the spine is necessary to assess the spinopelvic balance, which is pathologically altered in patients with dysplastic spondylolisthesis [
18]. There is an increase in lumbar lordosis. The lumbosacral profile and ventral displacement of the femoral heads also lead to a significant increase in PI and PT [
19]. The values of the given spinopelvic parameters were also significantly increased in our group. The SS value does not have to be significantly changed; it depends on the position of the sacrum. In the case of large slips, where the sacrum is verticalized, i.e., it takes the form of pelvic retroversion, the SS values are lower than those in the physiological state [
20]. The position and angulation of the lumbosacral junction can be measured in various ways. One of these is to form an angle between the L5 upper vertebral endplate and the S1 upper vertebral endplate. This angle corresponds to the lumbosacral angle (LSA). Another possibility is to measure the Slip Angle (SA), as described by Boxall [
21]. There is also variability in the formation of a given angle. This variability is caused by the pathological situation of the lumbosacral junction, the dome shape of the upper endplate of the S1 vertebra, which makes it difficult to form straight lines. In our group, we created SA as the angle between the perpendicular to the posterior edge of the S1 vertebra and the lower endplate of the L5 vertebral body.
Dysplastic changes in vertebral bodies act as a predisposing factor for the progression of vertebral slip. The method of measuring and determining the progress of the slip involves calculating the Severity Index (SI) and defining the unstable zone (UZ). To calculate the SI, it is necessary to make a horizontal line pointing from the center of the S2 vertebra. Next, two vertical lines are created. The first starts from the center of the lower endplate of the L5 vertebra, and the second passes through the center of the femoral heads. In a physiological state, these verticals are identical, as the vertical from the L5 body should pass through the center of the femoral heads. The distance from the center of S2 to the vertical line drawn from the center of the femoral heads is D2. The distance of the vertical line from the L5 body to the vertical line from the center of the femoral heads is D1. The equation for the calculation is SI = D1 × 100/D2. With advanced slip progression and gradual verticalization of the sacrum and ventral displacement of the femoral heads, D1 and, therefore, SI, increases. An SI above 20% is determined as a significant factor corresponding to highly dysplastic spondylolisthesis with a high risk of slip and clinical condition progression. The creation of a square, the side of which is given by the size of the distance D1, corresponds to an unstable zone. If the L4 vertebra extends into this square, it should be part of instrumented stabilization [
22].
Opinions on the treatment of dysplastic spondylolisthesis remain inconsistent and controversial. It is necessary to distinguish between low and high dysplastic spondylolisthesis. HDDS is, in contrast to LDDS, dangerous because of the risk of slip progression, which may possibly progress as far as spondyloptosis [
23]. Prevention of progression is one of the important aspects of treatment; therefore, HDDS should, in our view, always be indicated for surgical treatment.
According to Scaglietti, conservative therapy consists of long-term immobilization in a plaster corset in hyperextension with pressure on the sacrum [
24]. The plaster corset results in significant discomfort for the patient and its reduction ability is only minimal (
Figure 9).
Rehabilitation and physiotherapy act as supportive therapies that strengthen the deep stabilization system of the spine but do not address the pathological merits of the problem. A comparison of surgical and conservative therapies in pediatric patients with highly dysplastic spondylolisthesis was performed by Bourassa-Moreau based on a follow-up of 28 patients, 23 of whom were treated surgically and 5 conservatively. Improved quality of life and a better score in the SRS-22 questionnaire were achieved in the group treated surgically [
25].
However, opinions on the surgery to be performed also differ in the literature, from mere in situ fixation to the effort to fully reduce the affected segment. Proponents of mere in situ fixation argue that neurological complications are minor compared to those resulting from the reduction and overstretching of nerve structures. In addition, more frequent postoperative complications and a higher frequency of reoperations when attempting reduction are reported [
26]. However, results of the in situ fusion are unclear, with a high risk of nonunion development and increased probability of slip deterioration [
27]. On the contrary, the advantage of reduction over in situ fusion is the correction of lumbosacral kyphosis, thereby improving the overall sagittal profile and the symmetry of the lumbosacral junction, leading to correction of gait and standing, and, furthermore, the possibility of direct decompression of nerve structures [
28]. A comparison of both methods, i.e., reduction and in situ fixation, was performed by Longo [
29]. In his study, it was found that there is an improvement in biomechanical conditions and local kyphosis in patients with a reduction in the slipped vertebra. The reduction did not increase the risk of neurological complications associated with in situ fixation.
There is a consensus that, in the case of reduction, it is necessary to perform an interbody fusion of the anterior column; otherwise, there is a risk of failure of the reduction and instrumentation with the formation of a nonunion [
30]. An interbody fusion can be performed by the PLIF technique. Lamartina [
1] presents satisfactory short-term clinical outcomes with the reduction in the deformity using the PLIF technique with cages for interbody fusion. In the case of smaller slips, good results were achieved by a combination of posterior reduction and anterior interbody fusion using the ALIF technique [
31]. A new technique presented in the literature describes a combination of approaches with posterior mono-segmental stabilization and anterior direct reduction in the slip using the anterior cantilever procedure [
32]. The authors achieved a high fusion rate and partial reduction in the slip, and improved the anatomy of the LS junction. Good clinical and radiological results have also been obtained using a trans-sacral strut graft to perform interbody fusion [
9,
33]. According to the authors, there was no significant difference in the use of an allograft or autograft, and remodeling and firm fusion occurred in all patients. An integral part of surgical therapy is the correction of segmental kyphosis and restoration of the symmetry of the lumbosacral junction [
34].
The range of instrumentation and reduction extent have also been discussed. Some authors recommend extending the instrumentation to the L4 vertebra in the case of large slips [
35]. Conversely, prolongation of instrumentation distally using iliac screws into iliac bone reduces the risk of instrumentation failure [
36]. Lombardi [
37] recommends mono-segmental stabilization with the reposition of the slipped vertebra in all cases of dysplastic spondylolisthesis with a slip over 25%. Authors achieved a high rate of spinal fusion and restored proper lumbosacral anatomy while improving the whole sagittal balance. According to the extent of reduction, most authors recommend partial reduction in the slip instead of total reduction, because of the high risk of nerve root irritation [
38]. At our institution, we prefer reduction and mono-segmental stabilization. We agree with Stulik et al. [
39], who, in their group of patients with highly dysplastic spondylolisthesis, achieved very good results in the effort to complete reduction and mono-segmental stabilization of the affected segment.
The frequency of neurological complications resulting from the possible overstretching of nerve roots is one of the arguments of opponents of reduction. Intraoperative neuromonitoring is recommended to reduce the incidence of iatrogenic L5 radiculopathy [
40]. Lamartina [
1] reviewed publications on the treatment of highly dysplastic spondylolisthesis, involving a total of 224 patients. Twenty-eight patients, i.e., 12.5%, suffered from neurological postoperative symptomatology. Of these, 20 patients had solely transient disabilities and 8 patients (3.6%) suffered from verified radiculopathy. In our group, the frequency of neurological complications was 12.5%, as diagnosed in 4 patients of a total of 32.


 ,
, 









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}