
The Practitioner’s Eye: The Ricketts Technique Elements in Non-Extraction Treatment Camouflaging Skeletal Class III with Bite Asymmetry—A Case Series Presentation


Abstract
:1. Introduction
1.1. Aim of the Study
1.2. Ethical Committee
2. A Case Series Presentation
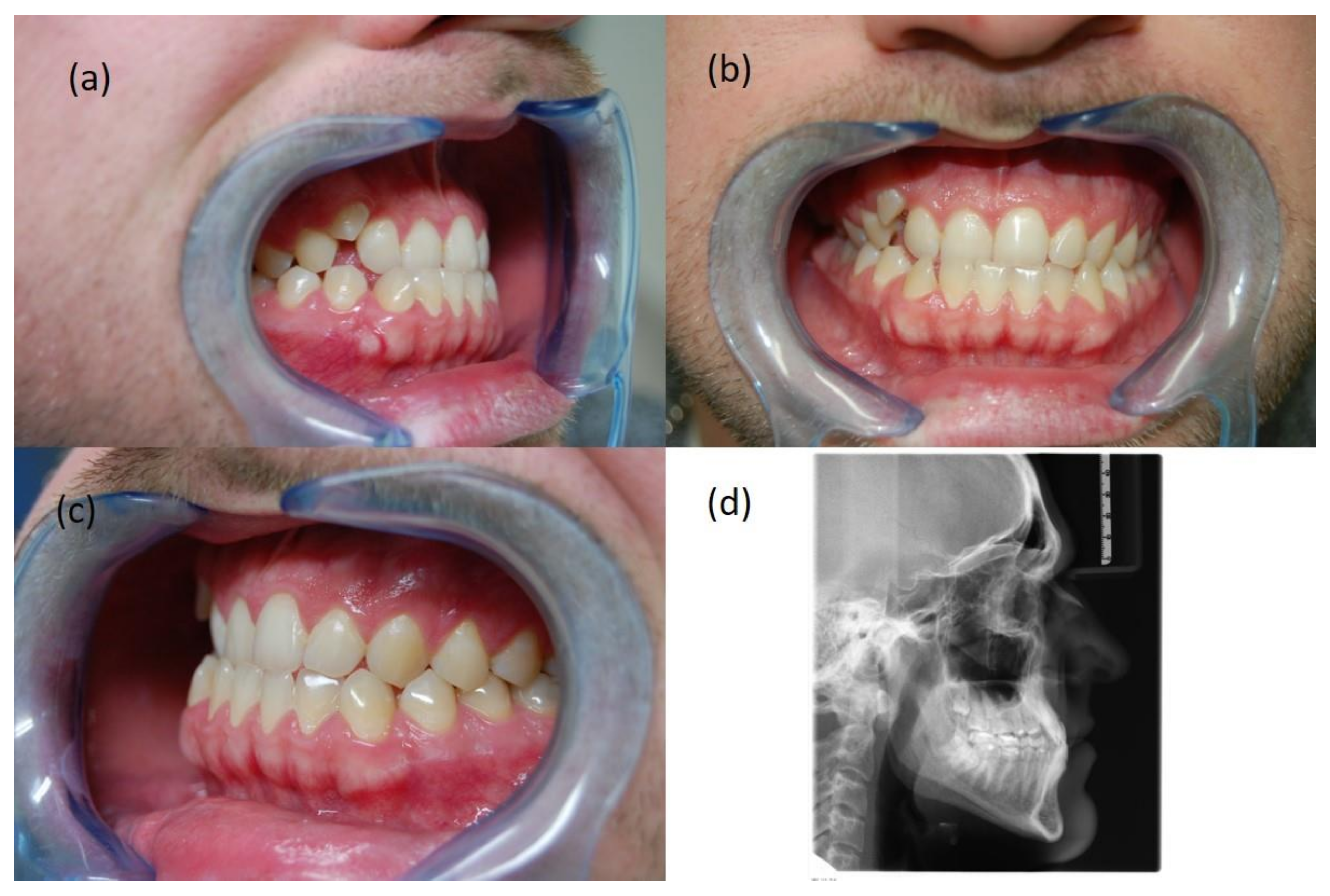
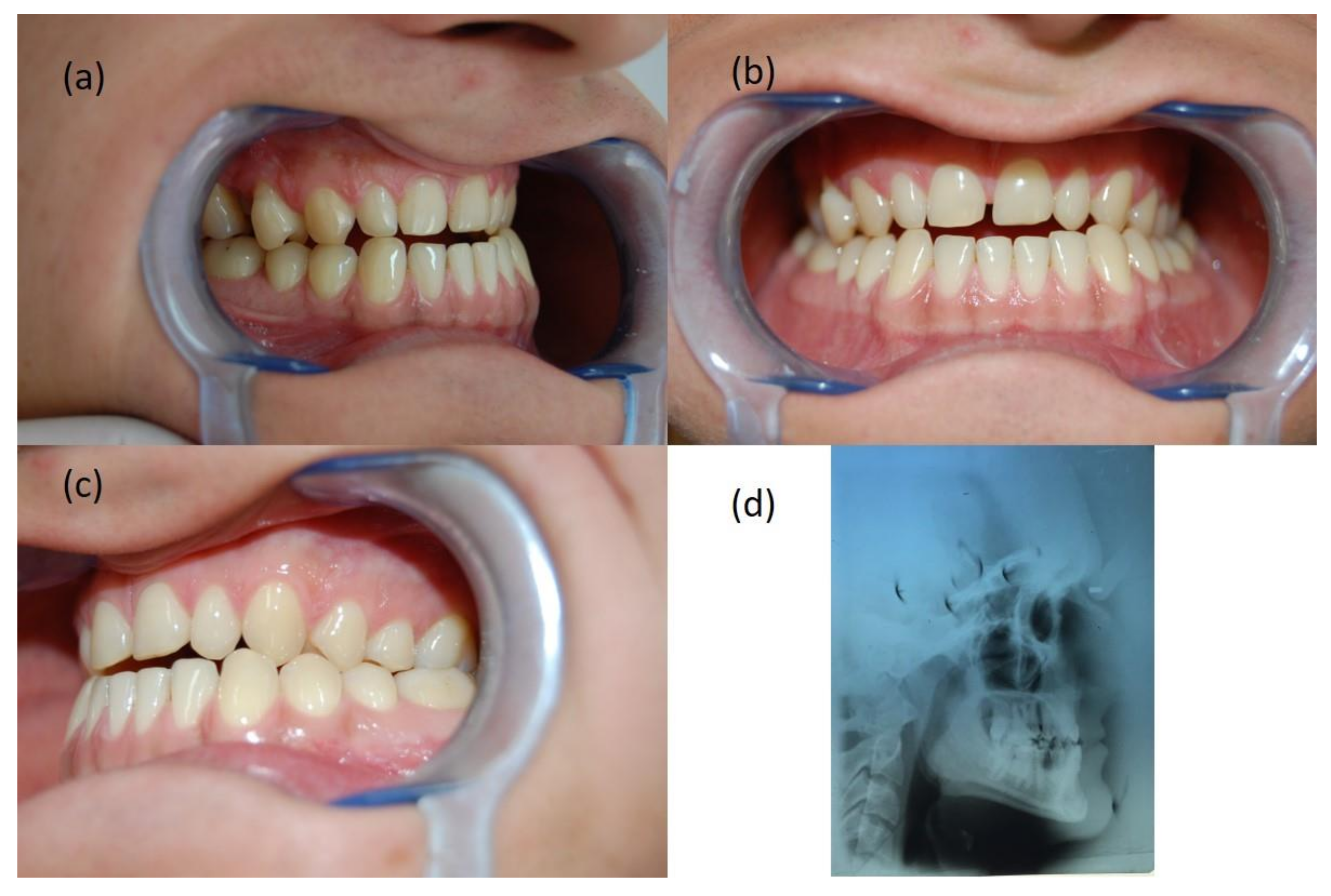
2.1. Patient KK, 26 Years Old
Diagnosis
2.2. Treatment Plan and Process
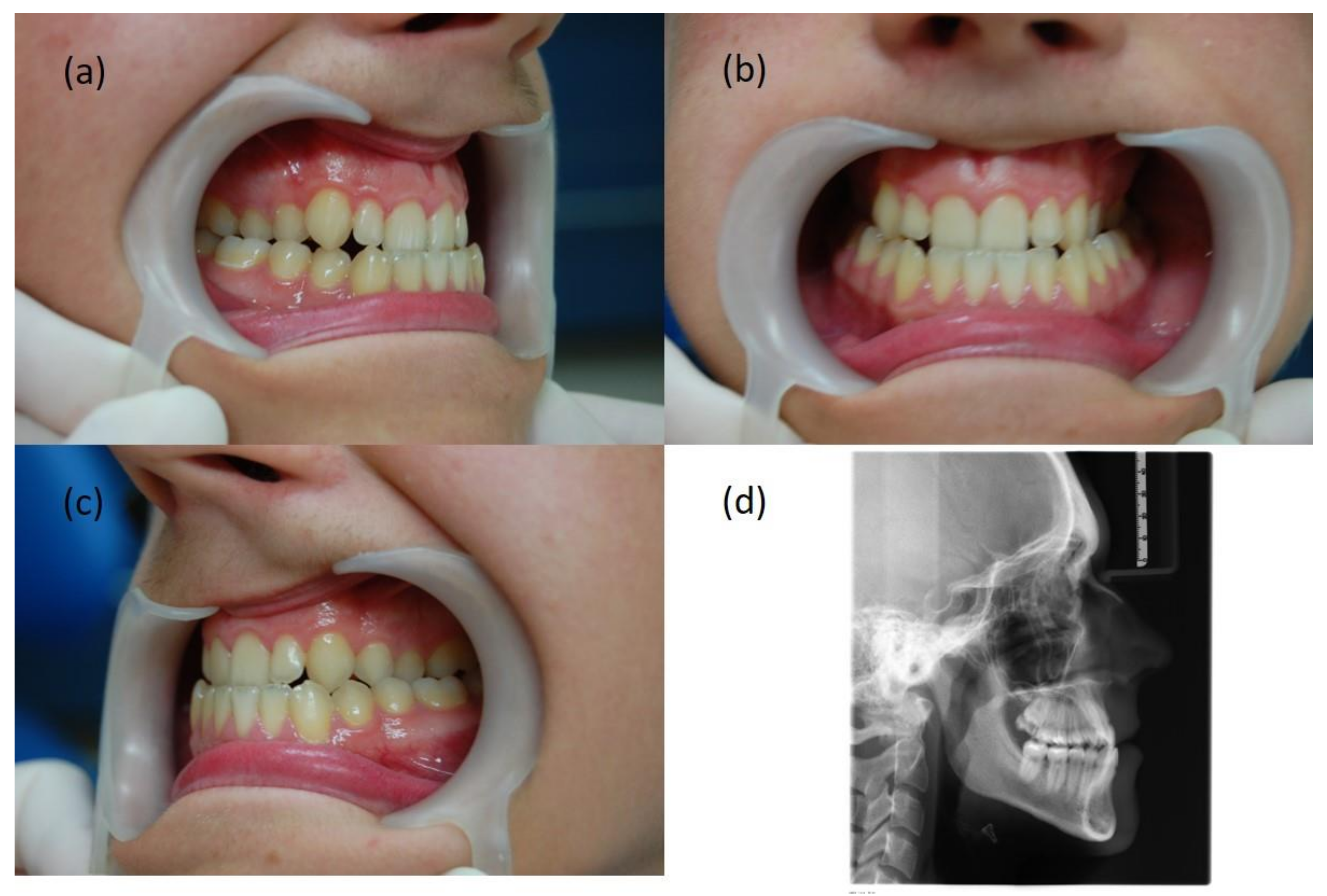
3. Patient IG, 18 Years Old
3.1. Diagnosis
3.2. Treatment Plan and Process
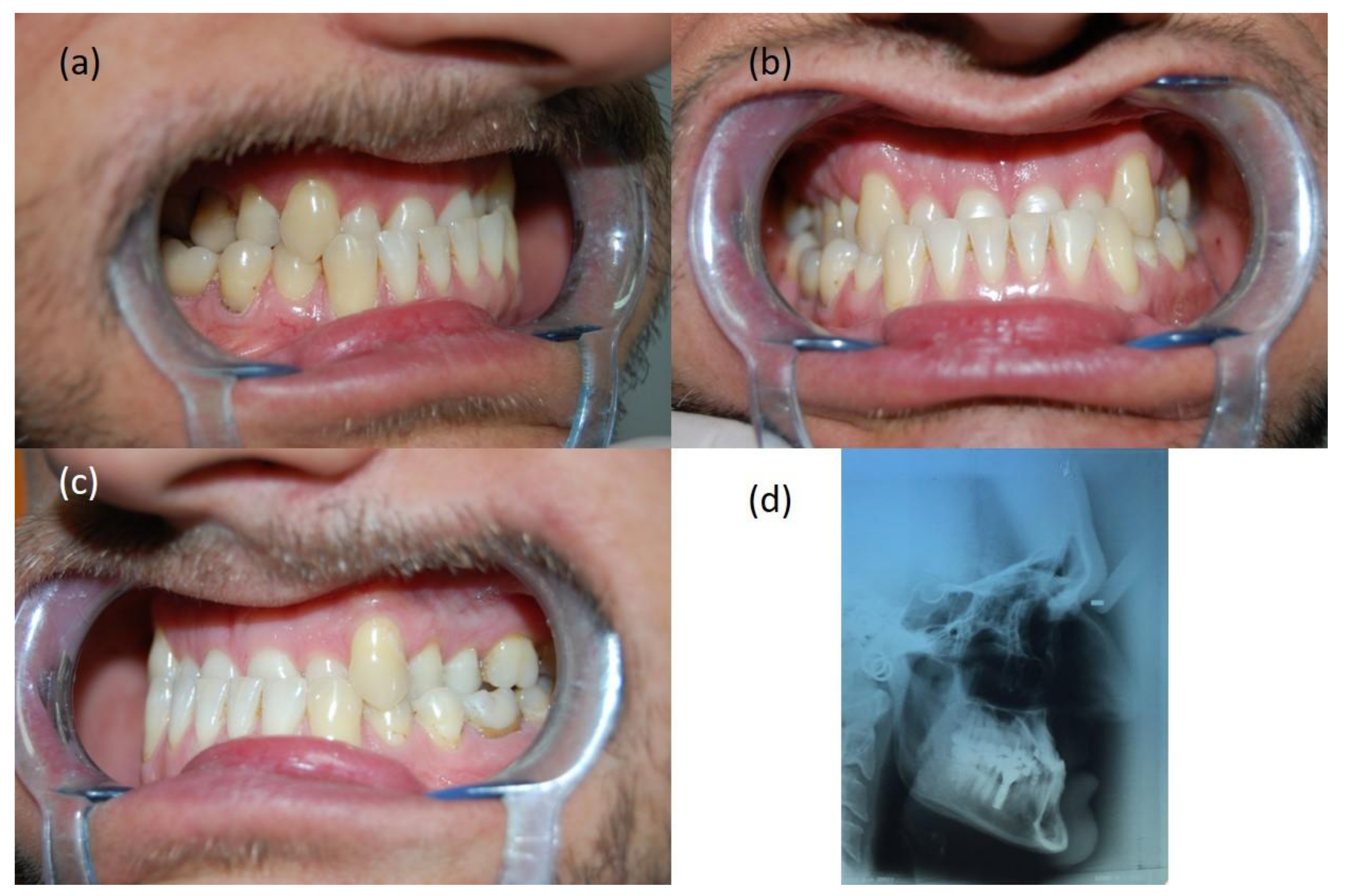
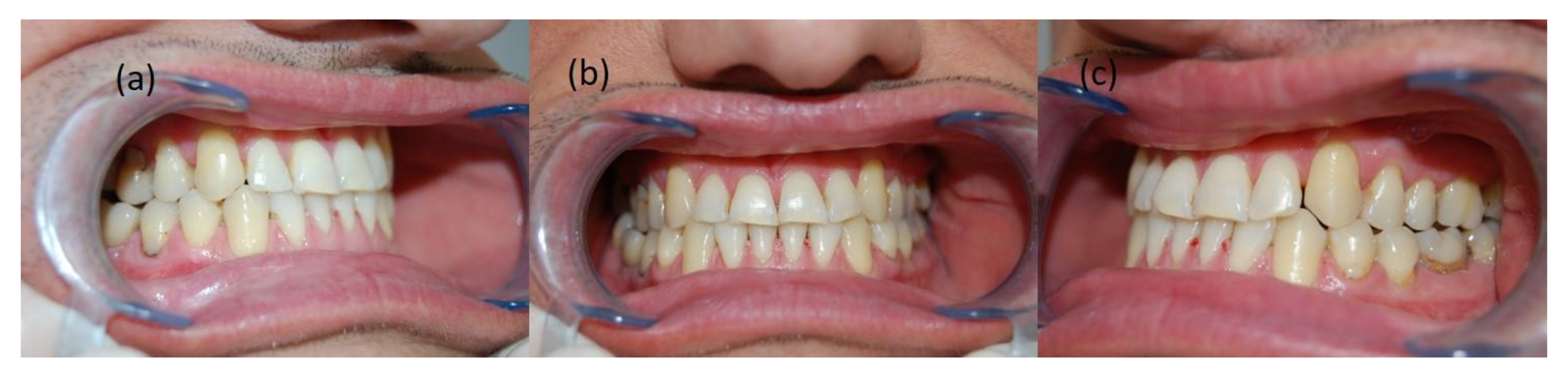
4. Patient PJ, 46 Years Old
4.1. Diagnosis
4.2. Treatment Plan and Process
5. Patient BB, 30 Years Old
5.1. Diagnosis
5.2. Treatment Plan and Process
6. Discussion
7. Conclusions
8. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chan, G.K. Class III malocclusion in Chinese (Cantonese): Etiology and treatment. Am. J. Orthod. 1974, 65, 152–156. [Google Scholar] [CrossRef]
- Baccetti, T.; Reyes, B.C.; McNamara, J.A., Jr. Gender differences in Class III malocclusion. Angle Orthod. 2005, 75, 510–520. [Google Scholar] [CrossRef]
- Yuan, J.T.; Teng, E.; Heller, J.B.; Kawamoto, H.K.; Bradley, J. Asymmetric Class III Malocclusion Association With Cranial Base Deformation and Occult Torticollis. J. Craniofacial Surg. 2012, 23, 1421–1424. [Google Scholar] [CrossRef]
- Langlade, M. Diagnostique Orthodontique; Maloine: Paris, France, 1981; p. 708. [Google Scholar]
- Proffit, W.R.; Fields, H.W.; Sarver, D.M. Ortodoncja Współczesna Tom 1, 2nd ed.; Komorowska, A., Ed.; Elsevier: Wroclaw, Poland, 2009; p. 297. [Google Scholar]
- Durão, A.R.; Pittayapat, P.; Rockenbach, M.I.B.; Olszewski, R.; Ng, S.; Ferreira, A.P.; Jacobs, R. Validity of 2D lateral cephalometry in orthodontics: A systematic review. Prog. Orthod. 2013, 14, 31. [Google Scholar] [CrossRef] [Green Version]
- Pancherz, H.; Sack, B. Kritische Analyse der Winkel SNA, SNB und ANB bei der Auswertung von kieferorthopädischen Behandlungen. Fortschritte der Kieferorthopädie 1990, 51, 309–317. [Google Scholar] [CrossRef]
- Ricketts, R.M.; Schulhof, R.J.; Bagha, L. Orientation Sella-Nasion or Frankfort horizontal. Am. J. Ortho. 1976, 69, 648. [Google Scholar] [CrossRef]
- Ricketts, R.M.; Langlade, M. Plaidoyer pour une orientation cephalometrique. Rev. D’orthopédie Dento-Faciale 1977, 2, 161–172. [Google Scholar] [CrossRef]
- Schulhof, R.J. When S-N is Abnormal. J. Clin. Orthod. 1977, 11, 343. [Google Scholar]
- Bourriau, J.; Bidange, G.; Foucart, J.-M. Measurement errors in 2D cephalometrics. L’Orthodontie Fr. 2012, 83, 23–36. [Google Scholar] [CrossRef]
- Beltrão, P. Non-Surgical Treatment of Class III with Multiloop Edgewise Arch-Wire (MEAW) Therapy. In Emerging Trends in Oral Health Sciences and Dentistry [Internet]; Virdi, M.S., Ed.; IntechOpen: London, UK, 2015; Available online: https://www.intechopen.com/chapters/47810 (accessed on 11 March 2021). [CrossRef]
- Gong, G.; Li, J.; Wang, Z.; Li, Y.; Hu, F.; Li, Q.; Miao, D.; Wang, L. Cranial base characteristics in anteroposterior malocclusions: A meta-analysis. Angle Orthod. 2016, 86, 668–680. [Google Scholar] [CrossRef] [Green Version]
- Janson, G.; De Freitas, M.R.; Araki, J.; Franko, E.J.; Barros, S.E.C. Class III subdivision malocclusion corrected with asymmetric intermaxillary elastics. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 221–230. [Google Scholar] [CrossRef]
- Frankel, R. Maxillary retrusion on class III and treatment with the function corrector III. Trans. Eur. Orthod. Soc. 1970, 46, 249–259. [Google Scholar]
- McNamara, J.A., Jr. The functional regulator (FR-3) of Frankel. Am. J. Orthod. Dentofac. Orthop. 1985, 88, 409–424. [Google Scholar] [CrossRef]
- Barrington, E.; Haswell, G.D. The Natural History and Diseases of the Human Teeth, 2nd ed.; Fox, J., Ed.; The Natural History and Diseases of the Human Teeth: London, UK, 1803; p. 331. [Google Scholar]
- Suzuki, N. A cephalometric observation on the effect of the chin cap. J. Jpn. Orthod. Soc. 1972, 31, 64–74. [Google Scholar]
- Graber, L.W. Chin cup therapy for mandibular prognathism. Am. J. Orthod. 1977, 72, 23–41. [Google Scholar] [CrossRef] [Green Version]
- Wendell, P.D.; Nanda, R.; Sakamoto, T.; Nakamura, S. The effects of chin therapy on the mandibule: A longitudinal study. Am. J. Orthod. 1985, 87, 265–274. [Google Scholar] [CrossRef]
- Delaire, J. Confection du masque orthopedique. Rev. Stomat. 1971, 72, 579–584. [Google Scholar]
- Haas, A.J. The treatment of Maxillary Deficiency by Opening the Midpalatal Suture. Angle Orthod. 1965, 35, 200. [Google Scholar]
- Westwood, P.V.; McNamara, J.A., Jr.; Baccetti, T.; Franch, L.; Sarver, D.M. Long-term effects of Class III treatment with rapid maxillary expansion and facemask therapy followed by fixed appliances. Am. J. Orthod. Dentofac. Orthop. 2003, 123, 306–320. [Google Scholar] [CrossRef] [Green Version]
- Baccetti, T.; McGill, J.S.; Franchi, L.; McNamara, J.A., Jr.; Tollaro, I. Skeletal effects of early treatment of Class III malocclusion with maxillary expansion and face mask therapy. Am. J. Orthod. Dentofac. Orthop. 1998, 113, 333–343. [Google Scholar] [CrossRef]
- Baccetti, T.; Rey, D.; Angel, D.; Oberti, G.; McNamara, A.J., Jr. Mandibular cervical headgear vs rapid maxillary expander and facemask for orthopedic treatment of Class III malocclusion. Angle Orthod. 2007, 77, 619–624. [Google Scholar] [CrossRef]
- Liou, E.J.; Tsai, W.C. A new protocol for maxillary protraction in cleft patients: Repetitive weekly protocol of alternate rapid maxillary expansions and constrictions. Cleft Palate Craniofac. J. 2005, 42, 21–27. [Google Scholar] [CrossRef]
- Franchi, L.; Baccetti, T.; Masucci, C.; Defraia, E. Early Alt-RAMEC and facial mask protocol in class III malocclusion. J. Clin. Orthod. 2011, 45, 601–609. [Google Scholar]
- Sycinska-Dziarnowska, M.; Janiszewska-Olszowska, J.; Grocholewicz, K. Leczenie przodozgryzu rzekomego z wykorzystaniem protokołu Alt-Ramec. Clin. Orthod. 2018, 1, 41–53. [Google Scholar]
- Vaughn, G.A.; Mason, B.; Moon, H.B.; Turley, P.K. The effects of maxillary protraction therapy with or without rapid palatal expansion: A prospective, randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 299–309. [Google Scholar] [CrossRef]
- Chung, K.R.; Kim, S.H.; Choo, H.; Kook, Y.A.; Cope, J.B. Distalization of the mandibular dentition with mini-implants to correct a Class III malocclusion with a midline deviation. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 135–146. [Google Scholar] [CrossRef]
- De Clerck, H.J.; Cornelis, M.A.; Cevidanes, L.H.; Heymann, G.C.; Tulloch, C.J. Orthopedic traction of the maxilla with miniplates: A new perspective for treatment of midface deficiency. J. Oral. Maxillofac. Surg. 2009, 67, 2123–2129. [Google Scholar] [CrossRef] [Green Version]
- Elnagar, M.H.; Elshourbagy, E.; Ghobashy, S.; Khedr, M.; Evans, C.A. Dentoalveolar and arch dimension changes in patients treated with miniplate-anchored maxillary protraction. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 1092–1106. [Google Scholar] [CrossRef]
- Tseng, L.; Chang, C.H.; Roberts, W.E. Diagnosis and conservative treatment of skeletal Class III malocclusion with anterior crossbite and asymmetric maxillary crowding. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 555–566. [Google Scholar] [CrossRef] [Green Version]
- Kucukkeles, N.; Yilmaz, H.N. Antoszewska, S., Ed.; Class III malocclusion. In Skeletal Anchorage in Orthodontic Treatment. Class II, III & Transverse malocclusion; Elamed: Katowice, Poland, 2014; pp. 35–52. ISBN 978-83-61190-53-0. [Google Scholar]
- Carriere, L. Nonsurgical correction of severe skeletal class III malocclusion. J. Clin. Orthod. 2016, 50, 216–230. [Google Scholar]
- McNamara, J.A., Jr.; Franchi, L.; McNamara-McClatchey, L.; Kowalski, S.E.; Cheesemane, C.C. Evaluation of adolescent and adult patients treated with the Carriere Motion Class III appliance followed by fixed appliances. Angle Orthod. 2021, 91, 149–156. [Google Scholar] [CrossRef]
- Sato, S. Case Report: Developmental characterization of skeletal Class III malocclusion. Angle Orthod. 1994, 64, 105–111. [Google Scholar] [CrossRef]
- He, S.; Gao, J.; Wamalwa, P.; Wang, Y.; Zou, S.; Chen, S. Camouflage treatment of skeletal Class III malocclusion with multiloop edgewise archwire and modified Class III elastics by maxillary mini-implant Anchorage. Angle Orthod. 2013, 83, 630–640. [Google Scholar] [CrossRef] [Green Version]
- Rubin, R.M. Commentary: Skeletal class III maloccusion. Angle Orthod. 1994, 64, 111. [Google Scholar] [CrossRef]
- Kucukkles, N.; Acar, A.; Demirkaya, A.A.; Evrenol, B.; Enacar, A. Cephalometric evaluation of open bite treatment with NiTi archwires and anterior elastics. Am. J. Dentofac. Orthop. 1999, 116, 555–562. [Google Scholar] [CrossRef]
- Gurgel, J.A.; Pinzan-Vercelino, C.R.M.; Leon-Salazar, V. Maxillary and mandibular dentoalveolar expansion with an auxiliary beta-titanium arch. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Langlade, M. Therapeutique Orthodontique; Maloine: Paris, France, 1986; pp. 135–158. [Google Scholar]
- Pelsue, B.M.; Zinelis, S.; Bradley, T.G.; Berzins, D.W.; Eliades, T.; Eliades, G. Structure, Composition and Mechanical Properties of Australian Orthodontic Wire. Angle Orthod. 2009, 79, 97–101. [Google Scholar] [CrossRef]
- Lin, J.; Gu, Y. Preliminary investigation of nonsurgical treatment of severe skeletal class III malocclusion in the permanent dentition. Angle Orthod. 2003, 73, 401–410. [Google Scholar] [CrossRef]
- Georgalis, K.; Woods, M.G. A study of Class III treatment: Orthodontic camouflage vs. orthognathic surgery. Aust. Orthod. J. 2015, 31, 138–148. [Google Scholar] [CrossRef]
- Eslami, S.; Faber, J.; Fateh, A.; Sheikholaemmeh, F.; Grassia, V.; Jamilian, A. Treatment decision in adult patients with class III malocclusion: Surgery versus orthodontics. Prog. Orthod. 2018, 19, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient KK | Patient IG | Patient PJ | Patient BB | |
|---|---|---|---|---|
| F (°) | 94.4 | 94.1 | 95 | 91 |
| XY (°) | 90.0 | 85.8 | 95 | 91 |
| NSBa (°) | 114 | 128 | 125 | 130 |
| A:NPg (mm) | −5.28 | −0.5 | −11 | −8 |
| SNA (°) | 81.8 | 79.4 | 80 | 73 |
| SNB (°) | 85.8 | 80.2 | 87 | 79 |
| ANB (°) | −4 | −0.8 | −7 | −6 |
| Wits (mm) | −7.31 | −3.33 | −13 | −5 |
| Mx/MP (°) | 23.8 | 31.6 | 11 | 18 |
| FMA (°) | 23.5 | 25.3 | 14 | 20 |
| SN/MP (°) | 28.8 | 39.6 | 21 | 30 |
| SN/FH (°) | 6.7 | 15 | 5 | 10 |
| IMPA (°) | 85.5 | 89.8 | 72 | 86 |
| UI/XY (°) | 0 | −8.4 | −13 | −9 |
| OJ (mm) | −1,5 | −2 | −7 | −3 |
| Sn (mm) | −15 | −12 | −32 | −21 |
| UL (mm) | −11 | −9 | −28 | −17 |
| LL (mm) | −6 | −4 | −9 | −12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwanicki, J.; Kawala, B.; Lis, J. The Practitioner’s Eye: The Ricketts Technique Elements in Non-Extraction Treatment Camouflaging Skeletal Class III with Bite Asymmetry—A Case Series Presentation. Symmetry 2022, 14, 316. https://doi.org/10.3390/sym14020316
Iwanicki J, Kawala B, Lis J. The Practitioner’s Eye: The Ricketts Technique Elements in Non-Extraction Treatment Camouflaging Skeletal Class III with Bite Asymmetry—A Case Series Presentation. Symmetry. 2022; 14(2):316. https://doi.org/10.3390/sym14020316
Chicago/Turabian StyleIwanicki, Jaroslaw, Beata Kawala, and Joanna Lis. 2022. "The Practitioner’s Eye: The Ricketts Technique Elements in Non-Extraction Treatment Camouflaging Skeletal Class III with Bite Asymmetry—A Case Series Presentation" Symmetry 14, no. 2: 316. https://doi.org/10.3390/sym14020316