
Philosophical Approach to Neural Autoantibodies in Psychiatric Disease—Multi-Systemic Dynamic Continuum from Protective to Harmful Autoimmunity in Neuronal Systems

Abstract
:1. Introduction—Immunological Conception of Central Nervous System Autoimmunity
2. Methods
3. Results
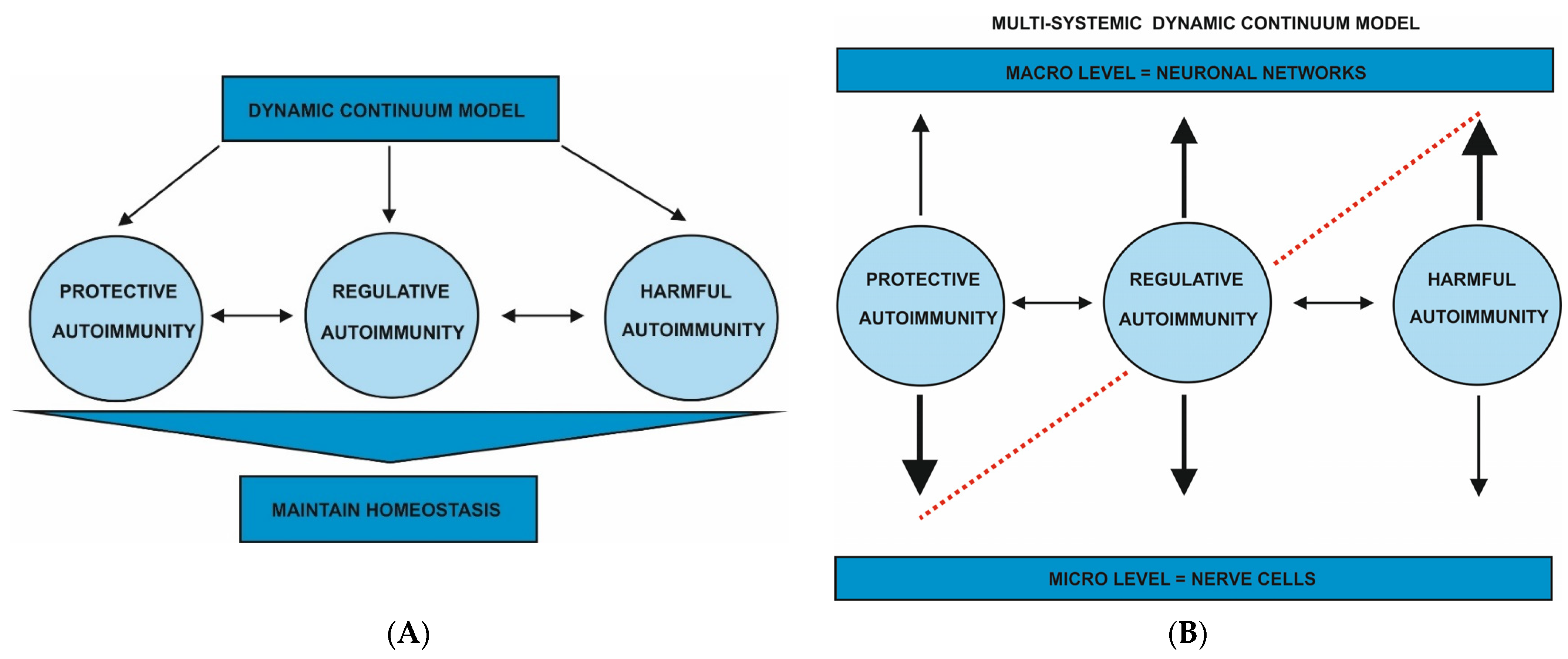
3.1. Philosophical Conception of CNS Autoimmunity
3.2. Autoantibody-Mediated Psychiatric Disease
3.3. Protective Autoimmunity
3.4. Regulatory Autoimmunity
3.5. Harmful Autoimmunity
4. Discussion
Funding
Data Availability Statement
Conflicts of Interest
References
- Bien, C.G.; Vincent, A.; Barnett, M.H.; Becker, A.J.; Blümcke, I.; Graus, F.; Jellinger, K.A.; Reuss, D.E.; Ribalta, T.; Schlegel, J.; et al. Immunopathology of autoantibody-associated encephalitides: Clues for pathogenesis. Brain 2012, 135, 1622–1638. [Google Scholar] [CrossRef] [Green Version]
- Malviya, M.; Barman, S.; Golombeck, K.S.; Planagumà, J.; Mannara, F.; Strutz-Seebohm, N.; Wrzos, C.; Demir, F.; Baksmeier, C.; Steckel, J.; et al. NMDAR encephalitis: Passive transfer from man to mouse by a recombinant antibody. Ann. Clin. Transl. Neurol. 2017, 4, 768–783. [Google Scholar] [CrossRef] [Green Version]
- Blackman, G.; Lim, M.F.; Pollak, T.; Al-Diwani, A.; Symmonds, M.; Mazumder, A.; Carter, B.; Irani, S.; David, A. The clinical relevance of serum versus CSF NMDAR autoantibodies associated exclusively with psychiatric features: A systematic review and meta-analysis of individual patient data. J. Neurol. 2022, 269, 5302–5311. [Google Scholar] [CrossRef]
- Ramirez-Franco, J.; Debreux, K.; Extremet, J.; Maulet, Y.; Belghazi, M.; Villard, C.; Sangiardi, M.; Youssouf, F.; El Far, L.; Lévêque, C.; et al. Patient-derived antibodies reveal the subcellular distribution and heterogeneous interactome of LGI1. Brain 2022, 145, 3843–3858. [Google Scholar] [CrossRef]
- Graus, F.; Titulaer, M.J.; Balu, R.; Benseler, S.; Bien, C.G.; Cellucci, T.; Cortese, I.; Dale, R.C.; Gelfand, J.M.; Geschwind, M.; et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016, 15, 391–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollak, T.A.; Lennox, B.R.; Müller, S.; Benros, M.E.; Prüss, H.; van Elst, L.T.; Klein, H.; Steiner, J.; Frodl, T.; Bogerts, B.; et al. Autoimmune psychosis: An international consensus on an approach to the diagnosis and management of psychosis of suspected autoimmune origin. Lancet Psychiatry 2020, 7, 93–108. [Google Scholar] [CrossRef]
- Hansen, N.; Lipp, M.; Vogelgsang, J.; Vukovich, R.; Zindler, T.; Luedecke, D.; Gingele, S.; Malchow, B.; Frieling, H.; Kühn, S.; et al. Autoantibody-associated psychiatric symptoms and syndromes in adults: A narrative review and proposed diagnostic approach. Brain Behav. Immun. Health 2020, 9, 100154. [Google Scholar] [CrossRef]
- Burnet, F.M.; Fenner, F. The Production of Antibodies, 2nd ed.; Macmillian: Melbourne, Australia, 1949. [Google Scholar]
- Pradeu, T.; Carosella, E.D. The Self Model and the Conception of Biological Identity in Immunology. Biol. Philos. 2006, 21, 235–252. [Google Scholar] [CrossRef]
- Burnet, F.M. Immunological recognition of self. Science 1961, 133, 307–311. [Google Scholar] [CrossRef]
- Pradeu, T.; Jaeger, S.; Vivier, E. The speed of change: Towards a discontinuity theory of immunity? Nat. Rev. Immunol. 2013, 13, 764–769. [Google Scholar] [CrossRef]
- Pradeu, T.; Vivier, E. The discontinuity theory of immunity. Sci. Immunol. 2016, 1, aag0479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, M.; Ziv, Y. Immunity to self and self-maintenance: A unified theory of brain pathologies. Trends Immunol. 2008, 29, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.; Raposo, C. Protective Autoimmunity: A Unifying Model for the Immune Network Involved in CNS Repair. Neuroscientist 2014, 20, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Winters, N.C. Autoimmunity and its expression in the analytic situation: A contemporary reflection on our inherent self-destructiveness. Int. J. Psychoanal. 2022, 103, 558–580. [Google Scholar] [CrossRef]
- Hart, B.A.; Luchicchi, A.; Schenk, G.J.; Stys, P.K.; Geurts, J.J.G. Mechanistic underpinning of an inside–out concept for autoimmunity in multiple sclerosis. Ann. Clin. Transl. Neurol. 2021, 8, 1709–1719. [Google Scholar] [CrossRef]
- Kamimura, D.; Yamada, M.; Harada, M.; Sabharwal, L.; Meng, J.; Bando, H.; Ogura, H.; Atsumi, T.; Arima, Y.; Murakami, M. The gateway theory: Bridging neural and immune interactions in the CNS. Front. Neurosci. 2013, 7, 204. [Google Scholar] [CrossRef] [Green Version]
- Nataf, S. Autoimmunity as a Driving Force of Cognitive Evolution. Front. Neurosci. 2017, 11, 582. [Google Scholar] [CrossRef] [Green Version]
- Hansen, N. Current Nosology of Neural Autoantibody-Associated Dementia. Front. Aging Neurosci. 2021, 13, 711195. [Google Scholar] [CrossRef]
- Banks, S.A.; Sechi, E.; Flanagan, E.P. Autoimmune encephalopathies presenting as dementia of subacute onset and rapid progression. Ther. Adv. Neurol. Disord. 2021, 14, 1756286421998906. [Google Scholar] [CrossRef]
- Endres, D.; Lüngen, E.; Hasan, A.; Kluge, M.; Fröhlich, S.; Lewerenz, J.; Bschor, T.; Haußleiter, I.S.; Juckel, G.; Bergh, F.T.; et al. Clinical manifestations and immunomodulatory treatment experiences in psychiatric patients with suspected autoimmune encephalitis: A case series of 91 patients from Germany. Mol. Psychiatry 2022, 27, 1479–1489. [Google Scholar] [CrossRef]
- Hansen, N.; Juhl, A.L.; Grenzer, I.M.; Hirschel, S.; Teegen, B.; Fitzner, D.; Bartels, C.; Timäus, C.; Wiltfang, J.; Malchow, B. Cerebrospinal Fluid Total Tau Protein Correlates With Longitudinal, Progressing Cognitive Dysfunction in Anti-Neural Autoantibody-Associated Dementia and Alzheimer’s Dementia: A Case–Control Study. Front. Immunol. 2022, 13, 837376. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.F.; Ismail, F.S.; Dornmair, K.; Cerina, M.; Meuth, S.G.; Melzer, N. GABAA Receptor Autoantibodies Decrease GABAergic Synaptic Transmission in the Hippocampal CA3 Network. Int. J. Mol. Sci. 2022, 23, 3707. [Google Scholar] [CrossRef] [PubMed]
- Andrzejak, E.; Rabinovitch, E.; Kreye, J.; Prüss, H.; Rosenmund, C.; Ziv, N.E.; Garner, C.C.; Ackermann, F. Patient-Derived Anti-NMDAR Antibody Disinhibits Cortical Neuronal Networks through Dysfunction of Inhibitory Neuron Output. J. Neurosci. 2022, 42, 3253–3270. [Google Scholar] [CrossRef]
- Kayser, M.S.; Dalmau, J. Anti-NMDA receptor encephalitis, autoimmunity, and psychosis. Schizophr. Res. 2016, 176, 36–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, A. The La Dourarin phenomenon: A shift in the paradigm of developmental self-tolerance. Int. J. Dev. Biol. 2005, 49, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, A. The Network Theory: 21 Years Later. Scand. J. Immunol. 1995, 42, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Notkins, A.L. New Predictors of Disease. Sci. Am. 2007, 296, 72–79. [Google Scholar] [CrossRef]
- Tauber, A.I. Reconceiving autoimmunity: An overview. J. Theor. Biol. 2015, 375, 52–60. [Google Scholar] [CrossRef]
- Savage, P.A.; Klawon, D.E.; Miller, C.H. Regulatory T Cell Development. Annu. Rev. Immunol. 2020, 38, 421–453. [Google Scholar] [CrossRef] [Green Version]
- Liston, A.; Dooley, J.; Yshii, L. Brain-resident regulatory T cells and their role in health and disease. Immunol. Lett. 2022, 248, 26–30. [Google Scholar] [CrossRef]
- Schwarz, A.; Schumacher, M.; Pfaff, D.; Schumacher, K.; Jarius, S.; Balint, B.; Wiendl, H.; Haas, J.; Wildemann, B. Fine-Tuning of Regulatory T Cell Function: The Role of Calcium Signals and Naive Regulatory T Cells for Regulatory T Cell Deficiency in Multiple Sclerosis. J. Immunol. 2013, 190, 4965–4970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Figueroa, P.; Roco, J.A.; Papa, I.; Villacís, L.N.; Stanley, M.; Linterman, M.A.; Dent, A.; Canete, P.F.; Vinuesa, C.G. Follicular regulatory T cells produce neuritin to regulate B cells. Cell 2021, 184, 1775–1789. [Google Scholar] [CrossRef] [PubMed]
- Zöphel, D.; Angenendt, A.; Kaschek, L.; Ravichandran, K.; Hof, C.; Janku, S.; Hoth, M.; Lis, A. Faster cytotoxicity with age: Increased perforin and granzyme levels in cytotoxic CD8+ T cells boost cancer cell elimination. Aging Cell 2022, 21, e13668. [Google Scholar] [CrossRef]
- Nissen, M.S.; Ryding, M.; Nilsson, A.C.; Madsen, J.S.; Olsen, D.A.; Halekoh, U.; Lydolph, M.; Illes, Z.; Blaabjerg, M. CSF-Neurofilament Light Chain Levels in NMDAR and LGI1 Encephalitis: A National Cohort Study. Front. Immunol. 2021, 12, 719432. [Google Scholar] [CrossRef] [PubMed]
- Gastaldi, V.D.; Wilke, J.B.; Weidinger, C.A.; Walter, C.; Barnkothe, N.; Teegen, B.; Luessi, F.; Stöcker, W.; Lühder, F.; Begemann, M.; et al. Factors predisposing to humoral autoimmunity against brain-antigens in health and disease: Analysis of 49 autoantibodies in over 7000 subjects. Brain Behav. Immun. 2022, 108, 135–147. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Theory | Advantage | Disadvantage | Reference |
|---|---|---|---|
| Self/non-self model |
|
| [8] |
| Continuity model |
|
| [9] |
| Unified theory of brain pathologies |
|
| [13] |
| Unifying model for immune network for CNS repair functions |
|
| [14] |
| Inherent self-destructiveness |
|
| [15] |
| Inside-out concept of autoimmunity |
|
| [16] |
| Gateway theory |
|
| [17] |
| Force of cognitive evolution |
|
| [18] |
| Multi-systemic dynamic continuum model |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, N. Philosophical Approach to Neural Autoantibodies in Psychiatric Disease—Multi-Systemic Dynamic Continuum from Protective to Harmful Autoimmunity in Neuronal Systems. Antibodies 2023, 12, 1. https://doi.org/10.3390/antib12010001
Hansen N. Philosophical Approach to Neural Autoantibodies in Psychiatric Disease—Multi-Systemic Dynamic Continuum from Protective to Harmful Autoimmunity in Neuronal Systems. Antibodies. 2023; 12(1):1. https://doi.org/10.3390/antib12010001
Chicago/Turabian StyleHansen, Niels. 2023. "Philosophical Approach to Neural Autoantibodies in Psychiatric Disease—Multi-Systemic Dynamic Continuum from Protective to Harmful Autoimmunity in Neuronal Systems" Antibodies 12, no. 1: 1. https://doi.org/10.3390/antib12010001